
Abstract
Eye–hand coordination is a visuomotor task that enables one to look, localize, and touch objects. Eye–hand coordination is known to be poor in children with developmental delay. In this study, we assessed the feasibility of measuring eye–hand coordination task in children with developmental delay using Sanet Vision Integrator (SVI), a commercially available device. Children (age: 3–16 years) with developmental delay and their age-similar typically developing peers were enrolled. White circles (5.5°) on a black background were presented on the SVI touch screen monitor. Participants popped these circles by touching it. Reaction time, accuracy, and an overall performance score were computed. Participants could perform the task from 4 years of age and with visual acuity 20/400 (6/120) or better. This resulted in 85% (17/20) of children with developmental delay and 95% (19/20) of typically developing children completing the task. Children with developmental delay were significantly (p < .001) less accurate (56%) and took longer (2.63 s) to complete the task when compared with their peers (accuracy = 93%, reaction time = 1.46 s). The overall performance score of children with developmental delay was also lower than their peers by a factor of 3.3. Eye–hand coordination performance can be measured and quantified with SVI. The quantification of speed and accuracy is possible and a unitary measure combining speed-accuracy can be computed. The task can be performed both by typically developing children and by children with developmental delay. Thus, it is feasible to measure eye–hand coordination using SVI. Such quantification will be useful for children undergoing interdisciplinary therapies for their medical conditions.
Introduction
Eye–hand coordination is a visuomotor skill that requires the ability of the visual system and musculoskeletal system to process and combine the information between the eyes and the hands (Rizzo et al., 2017). Optimal coordination between the eyes and hands is mediated by complex feedforward–feedback mediation between visuo-perceptual and visuomotor systems (Rizzo et al., 2019). Eye–hand coordination development starts from 5 months of age and gets refined over the years to reach adult-like timing and accuracy by the age of 9 years (Favilla, 2006; Hurlock, 1978; von Hofsten, 2007). However, in children with developmental delay this eye–hand coordination development can be delayed. The term “developmental delay” describes a broad phenotype when a child is unable to meet the developmental milestones when compared with their peers from the same demographics (Centers for Disease Control and Prevention, 2022; Choo et al., 2019). The etiology of developmental delay can be idiopathic, genetic, environmental, or psychosocial, and it can result in impairment in one or more domains of gross and fine motor development, speech and language skills, cognitive performance, and so on (Abo El Elella et al., 2017; Choo et al., 2019; Khan & Leventhal, 2022). Such a developmental delay can impact the daily living skills and activities of the child.
To accomplish a task like grasping a toy, good coordination between the eyes and hands is necessary, beyond good visual acuity or contrast sensitivity. Parents of children with developmental delay sometimes present to our eye clinic with complaints of functional vision difficulties, for example, child is having difficulty to pick a ball from the floor. While evaluations of visual functions (e.g., visual acuity) are regularly performed in the eye clinics, alongside with this, measurements of functional vision (i.e., ability to use vision for daily activities) can also aid in quantification of these functional difficulties. This in turn will provide better care and management plan for this cohort of children. This will be particularly helpful when working with an interdisciplinary team comprising physiotherapists, optometrists, occupational therapists, and so on who provide early intervention for children with developmental delay.
Tests involving eye–hand coordination reveal the sensory-motor integration and can also be indicative of functional vision abilities particularly for tasks involving spatial localization (Grant et al., 2014). However, such functional vision parameters may get tested by qualitative observations for specific tasks such as past-pointing (Leigh & Zee, 2015) or activity-based observations such as placing objects in a slot (O’Connor et al., 2010). Quantification of these performance measures in an ophthalmology or optometry clinical setting is very rare or none. Lab-based studies have quantified eye–hand coordination and demonstrated that children with autism and cerebral palsy are slower than their typically developing peers (Crippa et al., 2013; Saavedra et al., 2009). Patients with visual impairment such as amblyopia take longer time to plan and reach a target in an eye–hand coordination task (Niechwiej-Szwedo et al., 2011). Recently, quantitative analysis for eye–hand coordination has been made available in a commercial app (applications) (Lee et al., 2014; Lee & Ryan, n.d.). As this app requires cognitive and fine motor skills to perform the trace task, it may be challenging for some children with developmental delay. There is now an increasing trend towards using apps or interactive games to measure visual functions, for example, in Peekaboo Vision (Livingstone et al., 2019) (see “Methods” section), eye–hand coordination would be needed for some of these apps. Eye–hand coordination is also important, especially in timed tests or games that are given for amblyopia therapies. Thus, it will be helpful to explore a technology that can test and quantify eye–hand coordination performance as well, especially in those patients for whom this sensory-motor integration may be affected.
Sanet Vision Integrator (SVI) (HTS Inc., Gold Canyon, AZ, USA) is a commercially available device (Figure 1(a)) with several software features that permit to train and quantify eye–hand coordination, eye movements, visual memory, balance, and so on. The device is primarily used in vision therapy (Bhombal et al., 2020; Gallaway et al., 2017) and in sports vision (Appelbaum & Erickson, 2018). Literature on the use of SVI has been sparse (searched with keywords “Sanet vision integrator” in PubMed, Google Scholar, and ScienceDirect). SVI measure is shown to be repeatable for eye–hand coordination tasks in adults (Panchal et al., 2016). SVI use in children has not been reported in the literature to the best of our knowledge, be it for typically developing children or for children with developmental delay. Therefore, we undertook a study to determine if children with and without developmental delay are able to do the eye–hand coordination task using the SVI. In this study, the term developmental delay is used in its broad sense. It includes children with delayed milestones and having visual impairment. The study additionally aimed to quantify and compare the eye–hand coordination using SVI between children with developmental delay and their peers having normal visual acuity, without any delayed milestones, termed as “typically developing” children in this study. Given that no normative data are known for SVI, the data from the typically developing children through this study can be considered as pilot data for obtaining the same. Such a data would help in comparing the performance of children with visual impairment with and without multiple disabilities.

(a) The SVI (Sanet Vision Integrator) screen setup used in our study. (b) A participant performing the proactive eye–hand coordination task in SVI.
Methods
A cross-sectional prospective study was conducted. The institutional review board of our institute approved the study protocol. The protocol followed the tenets of Declaration of Helsinki. Written informed consent was obtained from parents/legal guardians of all the participants after explaining the study procedure and verbal assent was obtained from the child.
Participants
Participants were children in the age group of 3–16 years. Children with developmental delay, with or without cerebral visual impairment (CVI), were recruited from those visiting the Special Needs Vision Clinic and Institute of Vision Rehabilitation of our institute. These participants were referred to this clinic after having a comprehensive eye examination with the pediatric neuro-ophthalmologist. Participants with any visual field defects were excluded. Participants with developmental delay due to syndromic associations (e.g., Down syndrome) or spectrum disorders (e.g., autism) were also excluded. The pediatric neuro-ophthalmologist made the diagnosis for CVI and/or any ocular abnormalities. The treating pediatric neurologist elsewhere made the diagnosis of developmental delay and/or other systemic conditions.
Rehabilitation specialists evaluated the participants in the Special Needs Vision Clinic and those who required physiotherapy, special education, vision stimulation therapy, and low vision examination were appropriately referred to those services within this clinic. A physiotherapist evaluated and graded the referred participants as per the Gross Motor Function Classification System (GMFCS). While GMFCS is recommended to be used only for children with cerebral palsy, it is still acceptable to use it to distinguish participants as ambulatory and non-ambulatory (Towns et al., 2018). Children with upper limb disability were excluded. No other scales or tests were used to specifically quantify hand motor control, fine motor skills, cognitive ability, or intelligence quotient (IQ) in the clinic. Only qualitative observations for how children managed their activities of daily living were documented by the rehabilitation specialists. Children of employees in the institute and those children visiting the pediatric ophthalmology clinic for regular eye checkup were recruited for the typically developing cohort (controls). Children in the control group had presenting visual acuity of 20/25 or better in each eye and with no known ocular pathologies. All the participants performed the test with their habitual correction.
Peekaboo visual acuity measurement
Grating acuity was tested for all the participants on the Peekaboo Vision app (Livingstone et al., 2019). This interactive application is used to measure grating acuity on an iPad pro (12.9-inch diagonal LED-backlit Multi-Touch display, 2732 × 2048 resolution) for young children. The app has also been shown as a feasible test for children with Down syndrome (Sumalini et al., 2022). The participant could touch the side where a grating stimulus was presented on the iPad. Upon a correct touch, an animated face is shown with a “yippee” sound, encouraging the child’s participation. The visual acuity range of Peekaboo Vision is from 1.90 logMAR to –0.12 logMAR. The test was done binocularly at the recommended 50 cm viewing distance. The examiner ensured the distance was maintained by checking the distance with a measuring tape if the participant moves forward or backward. The visual angle of the circular stimulus in Peekaboo Vision at 50 cm is 5.5°. This size of the circle was used as the stimulus size in the eye–hand coordination task in SVI (see details below).
Eye–hand coordination task
Eye–hand coordination was measured with the SVI (HTS Inc., Gold Canyon, AZ, USA, version 3.6) installed in a Dell computer system (Intel i3-8100 CPU@ 3.60 GHz). The device comes with an LCD television (SONY, 55″, 1920 × 1080 with 29 Hz refresh rate) and a touch screen frame attached to it. The SVI software has different modules to test and train functions such as visual cognition, visual memory, and visuomotor functions, including eye–hand coordination. For the purpose of this study, the “Proactive” test in the eye–hand coordination module was used. All the testing was done under room illumination.
In the proactive eye–hand coordination module, a stimulus would appear at random locations on the computer screen and will remain until touched (Figure 1(b)). The stimulus was a white circle (5.5°) on a black background, with 100% contrast. Upon touching, the stimulus disappears with a popping sound and the next stimulus appears elsewhere on the screen. A central fixation stimulus (an alphabet of comparable size with the circle) was always present. The participant begins the task first by standing comfortably in front of the SVI computer screen and fixating at the center stimulus. Once the test starts, participants were encouraged to disengage from the central target and to freely gaze and search for the stimulus that could appear anywhere on the computer screen. Due to variable arm lengths, participants were allowed to choose their own comfortable viewing distance; however, the visual angle size of the stimulus was maintained at 5.5° for every participant. To achieve this, different stimuli sizes were measured with a ruler and visual angles were calculated for different viewing distances. The stimulus size in SVI can range from 1 (smallest) to 100 (largest) in arbitrary units. A linear regression was plotted to calculate the arbitrary units that has to be set in SVI, for the participant’s preferred viewing distance to obtain a 5.5° stimulus size.
Each participant was given one demo trial to get oriented to the task. If not understood, another two demo trials were given encouraging the participant to touch the stimulus quickly and correctly, when it appears (Figure 1(b)). Use of both their hands to touch the stimuli was encouraged. If the participant was unable to perform the task after three demo trials, then the participant was excluded from the study. After the demo trials, the main study was initiated. Every participant was given three test sets with a total of 45 stimuli (each test set consisted of 15 stimuli). Overall, it took about 15–20 min to complete the study.
Data analysis
Two outcome variables were obtained from SVI: reaction time (in seconds) and accuracy (in percentage). The device measures the average time taken to pop or touch the stimulus and generates the reaction time as one of the outcome variables. Also, a trial was considered accurate only if the very first touch was on the stimulus. For both these outcome variables, average was computed from three consecutive test sets. In addition, an overall performance score was calculated by taking the ratio of accuracy to reaction time. Hence, higher the overall performance score, better was the participant’s performance. Correlations were computed between age, reaction time, accuracy, and overall performance score. Visual acuity measured with Peekaboo Vision was correlated with the clinically measured visual acuity values as well. As the data were non-normally distributed, non-parametric tests (Mann–Whitney U test, Spearman correlation) were performed. SPSS version 20 (IBM SPSS Statistics, New York, NY, USA) was used for statistical analysis of all the data.
Results
A total of 40 participants were enrolled in this study. Of this, 20 children had developmental delay (CVI = 6) and 20 were their age-similar typically developing peers. The median age of both cohorts was comparable, t(38) = 1, p = .32. Among the 20 children with developmental delay, 17 children were able to complete the task and were included in the study. Of the three participants who could not complete the task, three of them had 1.91 logMAR visual acuity, which was below threshold for the SVI stimulus (5.5° or 1.81 logMAR). Among the 20 typically developing children, one participant (age 3 years) was not able to complete the task and was excluded. The demographic details of the participants who were included in the study, along with other clinical information for the two groups, are shown in Table 1.
Demographic details of the participants along with visual acuity, ocular conditions, & additional information (for children with developmental delay).

MRI: magnetic resonance imaging.
Performance measures
As expected, typically developing children had a significantly (Mann–Whitney U, p < .001) better performance (Figure 2) characterized by less reaction time (median [interquartile range] = 1.46 s [1.10–1.63]), more accuracy (93% [88.89–95.56]), and higher overall performance score (64.07 arbitrary units [52.93–89.16]), when compared with children with developmental delay (reaction time = 2.63 s [1.98–3.61], accuracy = 56% [21.10%–73.30%], and overall performance = 19.5 arbitrary units [6.16–34.12]). Children with developmental delay showed greater variability in all the performance measures.
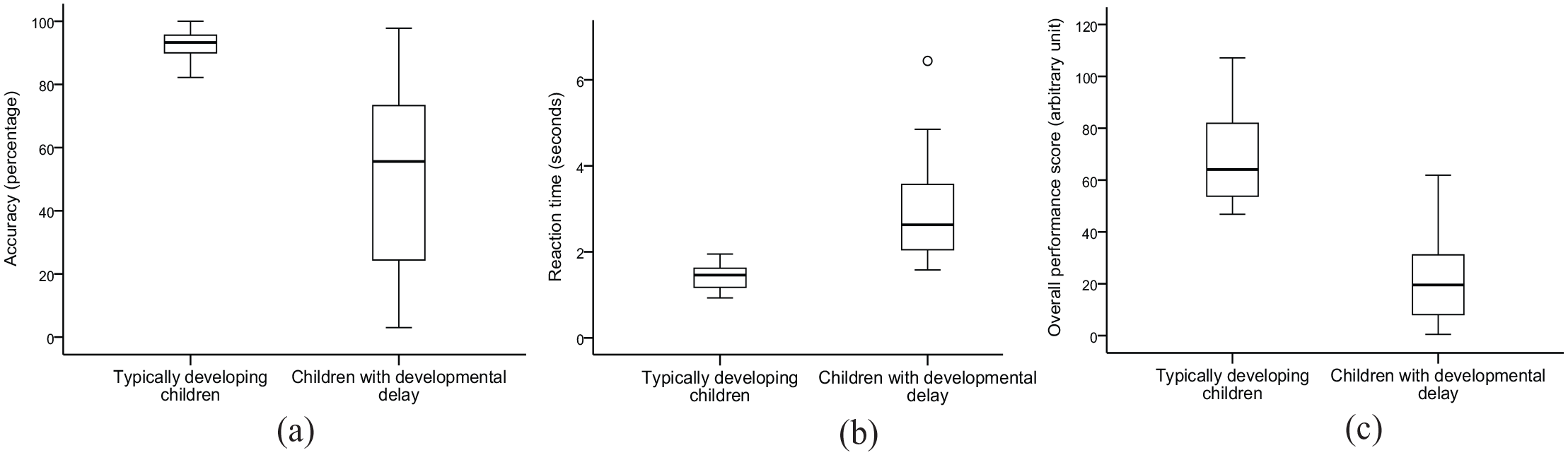
Boxplots for (a) accuracy, (b) reaction time, and (c) overall performance scores of typically developing children and children with developmental delay.
Typically developing children showed a moderate positive correlation (Figure 3) between age and the overall performance score (Spearman’s ρ = .52, p = .02). However, such a trend was not found in children with developmental delay (Spearman’s ρ = .25, p = .31). In addition, no correlation was found between visual acuity and overall performance score (Spearman’s ρ = –.26, p = .30) for children with developmental delay.
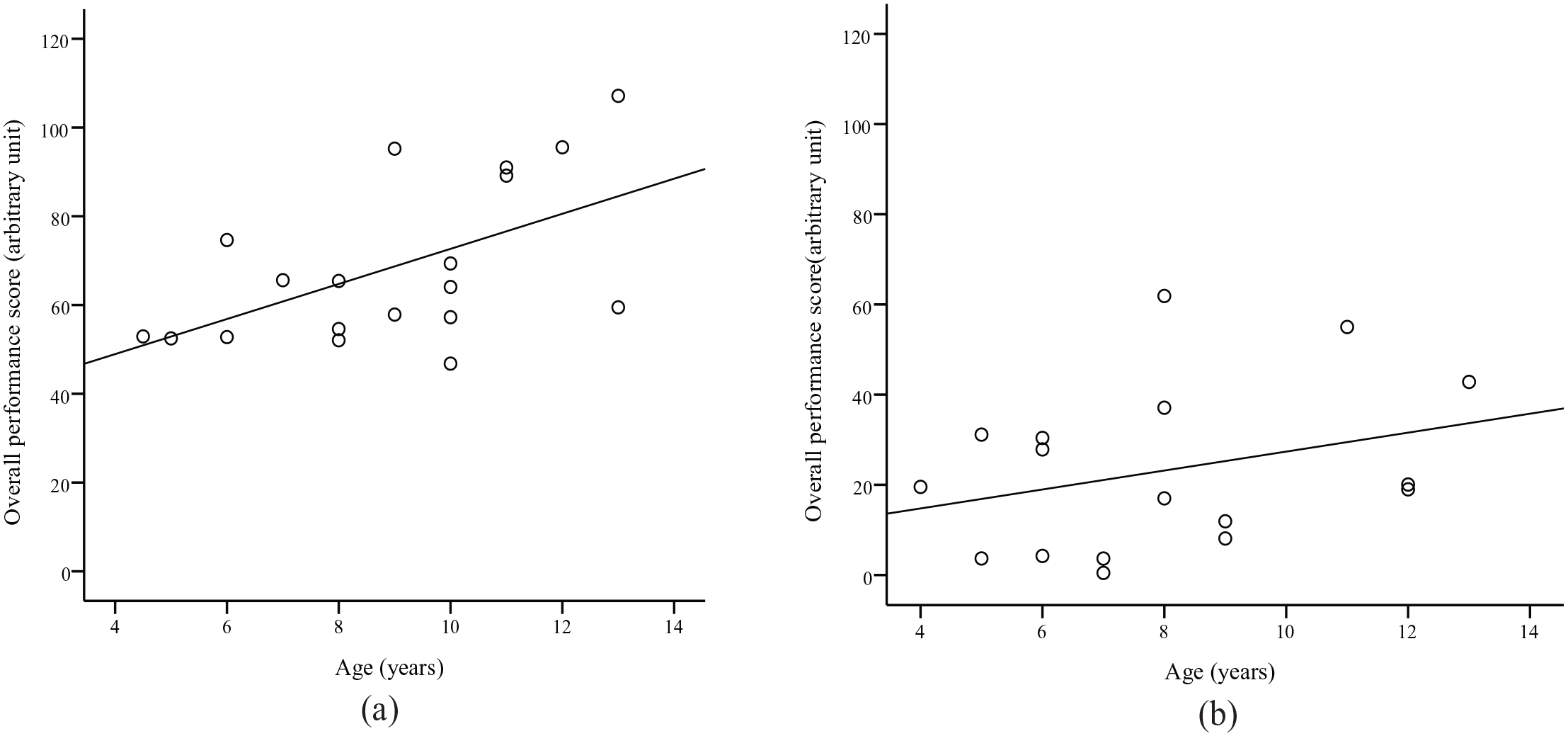
Scatter plot with linear regression line fit between overall performance score and age of the participants in (a) typically developing children and (b) children with developmental delay.
All participants (n = 40) were able to perform the Peekaboo Vision visual acuity task on their own, by the touch response. The binocular acuity measures from the Peekaboo Vision and that recorded in the clinic taken from the medical records for children with developmental delay showed a moderate (Spearman’s ρ = .61, p = .005) but significant correlation. For one participant, visual acuity was mentioned as fixating and following light in their clinical records and measured as 1.9 logMAR with Peekaboo Vision. This patient was excluded from the correlation calculation.
Of the 17 children with developmental delay, seven children required a referral to the physiotherapist. These referred participants were graded to be within GMFCS Level 1 and 2 with no upper limb limitations. The accuracy and overall performance scores were comparable (Mann–Whitney U test, p > .4) between these subgroups of participants who were graded (n = 7) and others who were not (n = 10), whereas the reaction time was significantly lesser (Mann–Whitney U, p < .04) for those who were not graded.
Discussion
We aimed to study if SVI can be used to measure eye–hand coordination in children with developmental delay and how that would compare with their typically developing peers. We found 85% (17/20) of children with developmental delay and 95% (19/20) of typically developing children were able to complete the task. Participants from 4 years of age and children with visual acuity of 1.3 logMAR (20/400) or better were able to perform this task. Also, participants with GMFCS level up to 2, without any upper limb dysfunction, were also able to perform the eye–hand coordination task in SVI.
The performance measures of time taken to complete the task and number of accurate trials can be documented using SVI. A unitary overall performance score that can account for time-accuracy trade off can also be computed and compared. As expected, the typically developing children were faster (by a factor of 1.8) and more accurate (by a factor of 1.6) in this eye–hand coordination task and hence exhibited a compounded higher overall performance score (by a factor of 3.3) when compared with children with developmental delay. The reaction time results in this study are comparable with a previous study that found the eye–hand reaction time to be slower by a factor of 1.1 in children with autism and Asperger’s syndrome when compared with their peers (Crippa et al., 2013). Children in autism spectrum disorder can also have developmental delay in the fine and gross motor domain (Provost et al., 2007). The participants in this study did not have a gross motor defect, but their fine motor skills were not assessed. In children with developmental coordination disorder, it has been found that their eye–hand coordination is deficient and they take twice longer to dwell on their fixation with sequential gaze, when compared with the typically developing peers (Wilmut et al., 2006).
A trend of improved performance with age (Figure 3(a)) was observed for the typically developing children. This is in agreement with the developmental growth curve that has been observed in other visual performance tasks (Niechwiej-Szwedo et al., 2021; Satgunam & Luo, 2018). However, such a trend was not observed in children with developmental delay. Several reasons could explain this finding. Poor visual acuity may result in poor performance in an eye–hand coordination task. Such a trend has been observed in patients with amblyopia and not in participants with induced optical blur (Niechwiej-Szwedo et al., 2012). Also, eye–hand coordination is found to be poor in children with CVI who also had poor visual acuity (Chokron & Dutton, 2016). However, our study results showed no correlation (Spearman’s ρ = –.26, p = .30) in performance with visual acuity, in children with developmental delay. This lack of correlation could be due to the suprathreshold target that was presented, at which level the visual impairment did not affect the eye–hand coordination performance in the SVI task, except for those whose visual acuity is worse than 1.8 logMAR. Other factors that can be attributable to the lack of correlation could be the cohort’s different ocular conditions, which also includes nystagmus (Liebrand-Schurink et al., 2014) and strabismus (O’Connor et al., 2010), both of which are known to have poor eye–hand coordination. A subgroup analysis for the different ocular conditions was not performed in this study due to the smaller sample size in each of those conditions. Other factors such as cognition (Martzog et al., 2019) and fine motor skills (Gaul & Issartel, 2016) are believed to impact eye–hand coordination. These factors were not investigated in this study. It was observed that the participants (n = 10) who did not require the GMFCS grading by the physiotherapist had significantly lesser reaction time (Mann–Whitney U, p < .04) compared with those participants (n = 7) who were graded. The latter cohort’s delayed reaction time could have been due to the motor deficits. Future studies can be undertaken with representative ocular conditions and graded levels of fine motor abilities, to investigate their role in the eye–hand coordination task.
Performance measures of children with developmental delay showed greater variability (Figure 2). More variability in tasks involving manual movements has been reported in individuals with developmental delay due to autism and Down syndrome (Glazebrook et al., 2006; Noghondar et al., 2021). While we took the average of three measures on the same test session to consider repeatability factor, further studies can be conducted to understand the repeatability of the outcome parameters measured over different days or weeks. Developmental age of the child instead of the chronological age can also be considered to explain the variability. In this study, developmental age was not computed. Intelligence quotient discrepancy (IQD) was also not checked for these children with developmental delay. IQD has been shown to have an association with motor competence (Yu et al., 2016).
Another outcome from this study showed that Peekaboo Vision can be used even in those children who were documented as fixating and following light in their clinical records. This could be due to the engaging nature of this app (Livingstone et al., 2019). Peekaboo Vision permits a larger area around the stimulus to be considered as an accurate touch response. This indicates that even if the child is not very accurate in their eye–hand coordination, as found using the SVI eye–hand coordination task, they can still perform the task in the Peekaboo Vision on their own. However, it must also be noted that in Peekaboo Vision the examiner can also give the touch response, based on the looking behavior of the patient, in case they are unable to touch and respond.
In conclusion, it is feasible to use SVI device to estimate the eye–hand coordination for both typically developing children and those with developmental delay. The device quantifies the time taken to complete the task and the accuracy of the performance. With such performance measures, clinicians and therapists managing children with developmental delay can monitor the progress (or not) in a longitudinal fashion. They can also evaluate the effectiveness of any intervention therapies given to these children to improve their eye–hand coordination using SVI.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank RenewSys India Private Limited and Mission for Vision, India, for their financial support in procuring the clinical equipment (Sanet Vision Integrator) used in this study. They also thank Hyderabad Eye Research Foundation and DBT grant (BT/PR32404/MED/30/2136/2019) for supporting the time of P.N.S. Authors have no financial interest in the device described here.