
Abstract
During August–September 2013, this research was conducted in two sites of World Vision India’s GRACE Project that specialize in providing care and support to children/adolescents (ages 11–19) impacted by HIV/AIDS in Chennai.1 This qualitative report presents the findings alongside a literature review that focuses on building resiliency upon the “innate capacities” of children/adolescents impacted by HIV/AIDS towards psychosocial, vocational, and spiritual flourishing. In order to better understand the ways in which programs can respond to the true needs of this demographic, the interviews and focus groups were framed with a participatory grassroots approach to discover unique challenges, future dreams, and existing capabilities.2 This study addresses the nature of resiliency in transformational development by exploring its engagement with the interlocking dimensions of well-being in four sections: 1) framing immediate needs and integrated programming, 2) social support and the role of kinship in transformational development, 3) enhancing vocational resiliency through participatory development, and 4) identity reformation and redeemed relationships within the Kingdom of God.
Keywords
Introduction
Out of an understanding that each vulnerable child has dignity and uniqueness within, there is a need for not only risk focused strategies that “reduce exposure to hazardous experiences,” but also asset focused strategies that sufficiently “provide resources needed for the development of competence” (Joy-Wright, 2010: 22). This trend has come out of the recent changes within the humanitarian sector, shifting from a general modernistic focus on improving deficiencies in “the physiology of survival” (physical dimension) to the Universal Declaration of Human Rights now having an evolving framework on well-being to cultivate “life with dignity” (now including psycho-social and spiritual dimensions) (Barnett and Stein, 2012: 116–120). Resiliency research shows that instead of a narrow external focus on “risk, deficit, and pathology” that perpetuates low expectations of children, programs that focus primarily on innate resilience “provide a major protective factor in positive expectations … when internalized by youth motivate and enable them to overcome risks and adversity” (Benard et al., 2007: 5). Pargament and Cummings have provided empirical evidence to support these immaterial domains enhancing resilience during humanitarian contexts as they uniquely engage: 1) “the search for meaning,” 2) “the quest for emotional comfort and anxiety reduction,” 3) “promotion of a sense of social interconnectedness,” and 4) “communion with the sacred” (Pargament and Cummings, 2010: 193–211).
The Kingdom of God brings healing and redemption to the poor, through Christ, insofar as it holistically deals with the “underlying marring of identity” that is rooted in the perpetuation of disempowerment and injustice (Christian, 1999: 216). As we are all made in the image of God, intrinsic resiliency is our God-given capacity to preserve and sustain our humanity despite circumstances of adversity that threaten our hope and/or pursuit of human flourishing. This participatory research report, centered on responses from interviews and focus groups, will explore the nature of resiliency as it relates to the human pursuit of identity, socialization, and vocation. The rationale for using this grassroots approach to research was to empower the voices of those living with HIV/AIDS to not only shed light on various theoretical approaches to psychosocial care and resiliency, but also enable them to become dignified participants for program feedback and evaluation. As we explore the mission of God within this context, listening to perspectives on spirituality and hope enable us to both learn from and empower those in their pursuit of human flourishing, as illustrated by this interviewee:
AIDS is like a slipper, if you are wearing it in your mind it will be everywhere with you. You shouldn’t stick to it all the time. If you remove it, you can walk a normal life. (17-year-old male)
Provision of “Basic Needs” and the Foundation for Resiliency
A. Learning from the Felt Immediate Needs Related to HIV/AIDS
The concept of resilience can be used in a re-active way (after harm has been done to the child) or in a proactive and preventative way, focusing on how the existing “continuum of defensive, adaptive, and perseverant elements” can be stimulated in order to teach them how to deal with life’s difficulties (Rak, 2002: 258). This participatory research study on resiliency centers on the conviction that these perseverant children/adolescents themselves are best suited to inform and guide our understanding of the felt immediate needs related to HIV/AIDS.
3
Therefore, the experiences, struggles, aspirations, and priorities of this demographic are all used to develop a framework that not only deals with the realities of struggle, but also points to participatory methods of development. We began by having the focus groups shed light on the particular barriers to resiliency with this first question:
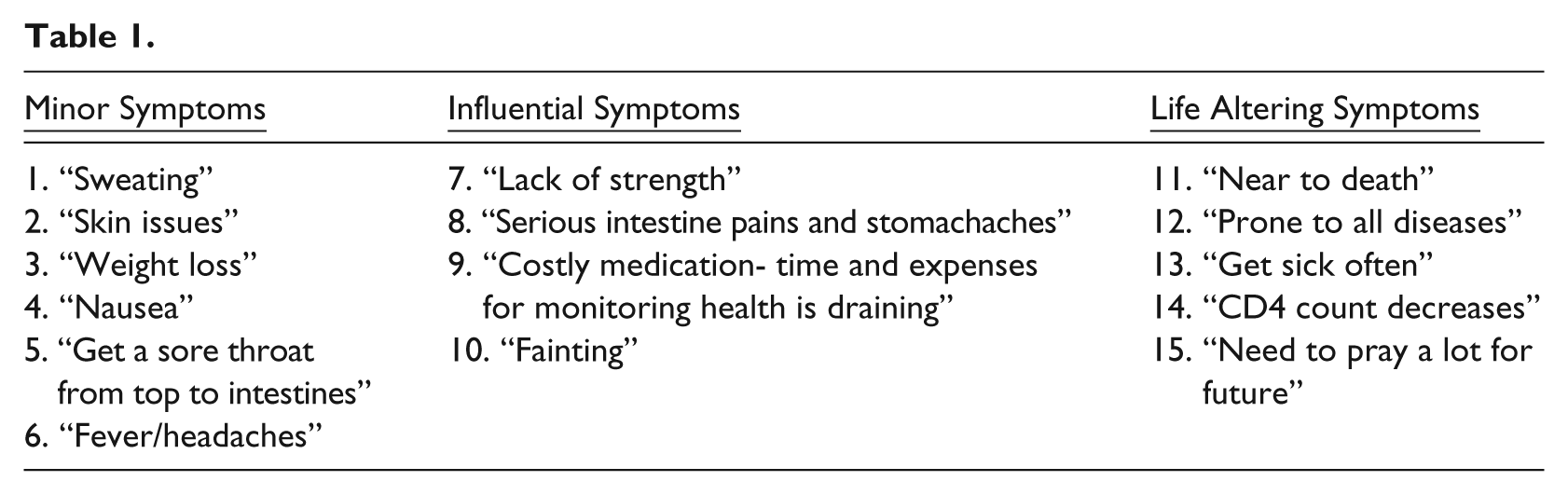
While it is difficult to measure the weights of the physical impacts of HIV/AIDS, we must first recognize that this frames an interlocking burden that has many life-altering forms. In Table 1, the collective group responses are framed in three general categories that highlight the various levels of impact that physical stressors have on normal daily living.
4
As these help us frame their context of adversity, especially as it relates to socialization and vocation, we can begin to develop a helpful response of understanding and compassion. The economic weight of HIV/AIDS infection is massive on the household’s overall mortality, income, productivity, and health expenditures. This threat to household security (school/job discrimination, hospital costs, or physical weakness) increases the vulnerability of the entire household as poverty, especially for the “excluded,” further compounds the stressors related to HIV/AIDS, as one group spokesperson in Adambakkam stated:
If your father is infected, income will be very low [due to physical weakness] and there will be employment discrimination. Food will be limited. There is no facility to study well and it is hard to focus. If neighbors find out about his status, they will discriminate your family and they will keep you alone. They will see you as different people. These can lead to bad habits, threats to the family, and even possibilities of death.
B. Addressing Needs of “Existence” While Fostering Participation
As the child develops into an adolescent, there becomes an “identity crisis” where having a life threatening illness is “a threat to autonomy and a potential threat to self-determination” (Erikson, 1963: 36). These immediate threats to household security, along with this internalized loss of self-determination, reinforce the “nearsighted psychology” of the marginalized as it develops a “perception of time inconsistency” that often leads to child labor, improper adherence to treatment, isolation, and absence from school (Banerjee and Duflo, 2011: 154). An illustration of this in relation to prioritization conflicts or psychosocial issues related to vocation is expressed in the following expressions of fear from the one-on-one interviews:
5
My fear of dying is always with me. It is hard to focus in school. I see other kids doing well; I always ask why do I have to be like this? Why did I have to get infected? (14-year-old male) I am very afraid something will happen with my mother since she is vulnerable. This always makes me stressed. (16-year-old male)
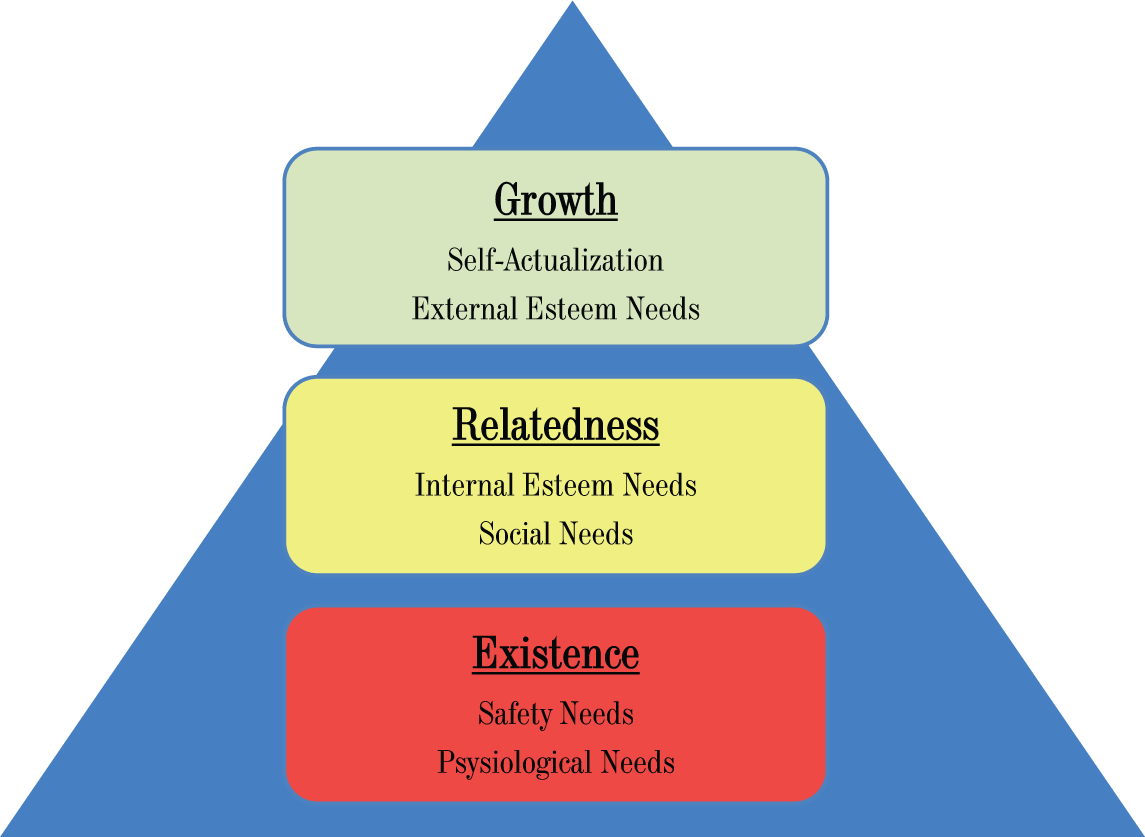
When addressing the foundation of resilience building, Psychologist Clayton P Alderfer connects these basic or “Existence” needs to propel the interrelated motivations of “Relatedness” and “Growth” (see Figure 1) (Alderfer, 1969: 142–175).
ERG Theory of Motivation: An Empirical Test of a New Theory of Human Needs; Organizational Behavior and Human Performance.
Much of the individual interviews centered on making sense of present circumstances in order to progress in vocation due to this new “identity crisis.” Figure 1 demonstrates how the satisfaction of “basic needs” specific to this study’s demographic leads to progression, whereas frustration can lead to regression. Masten affirms this relationship by stating, “when adversity is relieved and basic human needs are restored, then resilience has a chance to emerge” (Masten, 1994: 5). This has emerged out of Abraham Maslow’s original “Hierarchy of Needs” theory, which has psychological health predicated on fulfilling innate human needs of “deficiency” in priority (physiological, safety, love/belonging, esteem), culminating in self-actualization (Maslow, 1954: 63–79). By understanding motivation in the school and educational context on the basis of this theory, one may well argue that full attention to school work can only occur when more basic needs (physical, security, and social) are satisfied. However, development practitioners, largely operating from the Mental Health Professionals Stress Scale (MHPSS) framework, have promoted a broader framing of the psychosocial well-being of communities by including mental health as a key sector of humanitarian response (Ager et al., 2013). Rather than isolating psychosocial and spiritual needs from material provision, Williamson and Robinson state that the “Seven Domains of Well-being” (biological, material, social, spiritual, cultural, mental, emotional) are interrelated and cannot be addressed effectively if they are not addressed in an integrated way (through safety, development, and participation)” (Robinson and Williamson, 2006: 8). In approaching stability from inward stability, programs must avoid reinforcing dependency by creating integrative opportunities in which these innate capabilities can grow. While this holistic framework needs to be held together for programming, the following sections have been dissected to examine the literature review and empirical research for each innate capability separately.
Psychosocial Support and Care: Recovery, Coping, and Kinship
A. Psychosocial Recovery: Grief, Loss, and Isolation
As we previously explored the “needs of existence” and their respective stressors, this section will look at the role of psychosocial support and care, especially in how these promote positive behaviors in recovery, coping, and socialization. As Figure 2 prioritizes social support and care as the third highest need for programming, it is clear that the participants deem this as critical in addressing the psychosocial recovery of a child that has been newly diagnosed with HIV/AIDS. The next focus group question expands on this as they describe the common influence(s) of social stigma on a child/adolescent. The focus group at Adambakkam responded to this question below:
Group 1: “The main difficulty [with stigma] is not having friends and being alone from people. I would help them with finding friends that understand.”
Group 2: “I feel alone in class because I can’t disclose my status. In games and group studying we are excluded so we feel alone. I would help you to find ways to be included.”
Group 3: “It is because of your fear that you will remain isolated. Someone will misunderstand what you have. Have trusted friends or family to help you overcome this fear.”
Group 4: “If your neighbors find out, they will discriminate your family and they will keep you alone.”
Group 5: “People that find out will keep you alone. They see you as a different person. Some will tease you.”
Group 6: “It can lead to bad habits, threats to family, and possibilities of death.”
Vocational Selection.
The themes of isolation and fear are the common threads found in the previous groups’ responses. Although these are generally transferable to all populations influenced by any form of stigma or discrimination, specific articulations of hindrances were limited due to the developing levels of self-awareness and/or transparency in this particular life stage. When grief or traumatic experiences are internalized, especially when losing a family member to the disease, the complications and stigma associated with HIV can further perpetuate isolation from the support that is needed. Psychologist Phyllis Kilbourn states,
When children have experienced trauma, either in the family or from outside forces: they automatically begin to put up walls to protect themselves and often turn inward to create as much safety for themselves as possible. They have learned through their experiences that the world is not a safe place. (Kilbourn, 2002: 65)
For the 37% that expressed a preference or restriction to coping in isolation, these responses demonstrate the isolated approaches to obtain a sense of safety:
When I am really stressed I go to the beach by myself and walk for a while. I sit alone for a while and think. (17-year-old male) When I am stressed, I don’t talk with my mom and sister. I usually fight with them. I cope by keeping things to myself and focusing on other positive things. (16-year-old female (father expired)) I don’t want to talk to my family about my problems. Sometimes I sit in bed and cry by myself to feel better. Even though I don’t want to be sad by myself, I am scared to tell others. (14-year-old female (both parents expired)) I keep my problems to myself and am not comfortable sharing with others yet. I won’t open up my problems to anyone and as time goes by, I hope it will pass and I will forget it. (14-year-old male)
B. The Role of Kinship and Belonging
Moving from Alderfer’s stage of existence (disclosure, guidance, and healthy decisions) to relatedness, social support, and care serves to deepen capacities to resiliency within the context of kinship. As this program created a space where HIV/AIDS specific struggles were used to unify a group, kinship has been formed and used collectively as a powerful resource by individuals. This was most notable in the focus groups, where teams were visibly excited, affectionate, and empathetic with one another. This developed sense of belonging provides a feeling of physical comfort and trust with a minimal amount of fear and apprehension about the future. Developmental psychologist Erik Erikson elaborates on this phenomenon:
Trust in intimacy sets the stage for a lifelong expectation that the world will be a good and pleasant place to live … when a development stage is not completed and its tasks accomplished, one can go through life unattached. Rather than feeling like an outsider, belonging is an awareness of being wanted and accepted, of being cared for and enjoyed. (Erikson, 1969: 34, 52, 74).
More than material provision, the relational nature of the program needs to give opportunity for healthy socialization towards a new sense of belonging. As programs develop space in which kinship can be mutually fostered within the social sphere of individuals impacted by HIV/AIDS, the social stigma pressures of intrusive thoughts and avoidant behaviors are diminished and replaced. Peer affiliation fosters resiliency by empowering one “in the midst of adversity and failure” to “overcome risks” in a child’s overall development course” (Balswick et al., 2005: 157). During the individual interviews, those that expressed a sense of belonging found strength through sharing in their unique struggles:
My school friends don’t know my status but my friends here know. When I first shared my status with them, it built trust and they immediately accepted me. They reassure me and say ‘I love you’. They used to kiss and hug me and at first I felt surprised, but they said ‘it’s ok we are friends’. I am happy here because they help build my confidence. (13-year-old female) I have become very close to people here and have realized that you need to be really close to people with HIV to really help them and provide care for their condition. (17-year-old male) My favorite part is that I can see many friends and play with them. I have many close friends here and can talk about anything. I used to share many things with them, and my problems. I feel closer to my friends here than my friends at school. (13-year-old female) Before WVI’s schooling provisions and activities, I didn’t talk much. I had difficulty speaking words. They have given me chances to speak up in public and interact, which has helped give me confidence socially. (17-year-old male (expressed fears of communicating due to stigma))
This particular framework of kinship establishes a relational stability that will build capabilities to persevere in relationships and vocation. More than one-on-one relationships with mentors or extended kin structures, programs must also lead to family stability as psychosocial interventions should “support rather than usurp the parental role … maintaining the family structure will enhance [children living with HIV] in developing healthy independence, mobility, and self-care, which enhances their sense of self” (Pequegnat, 2006: 136).
C. Utilizing Affinity Towards Social Responsibility and Healing
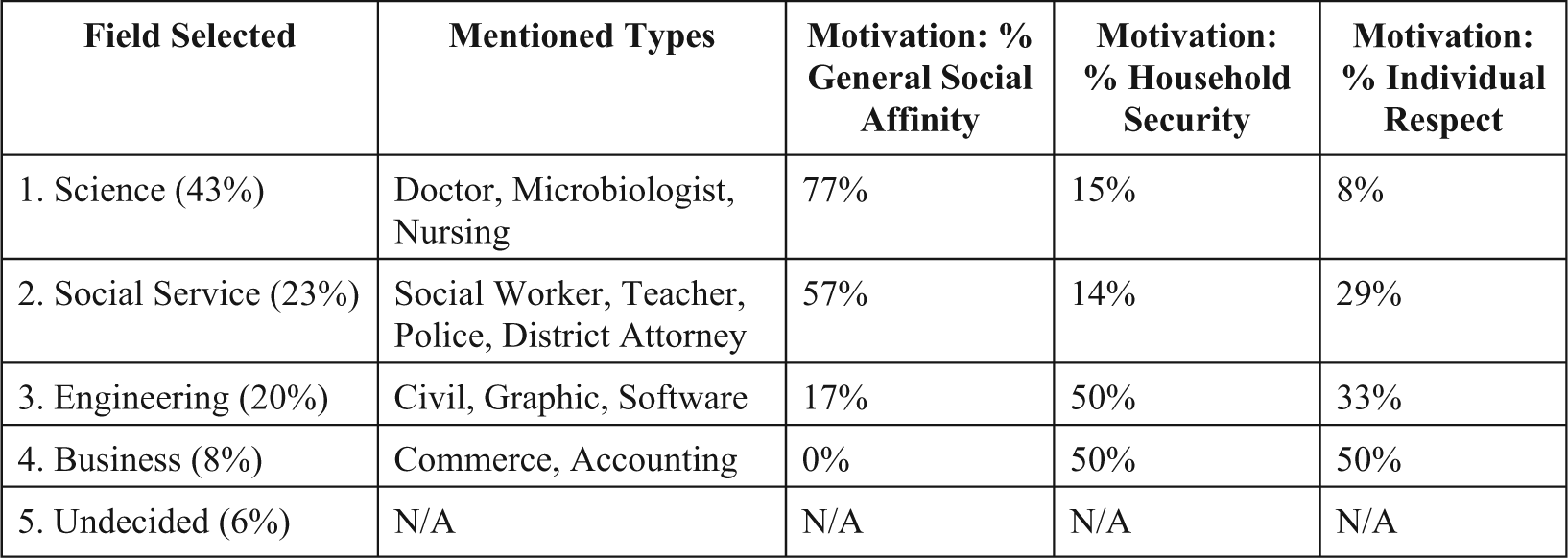
Benard’s study on the role of meaningful contribution in resiliency found that “paradoxically, one of the best way to bounce back from personal problems is help someone else with theirs … in a new healing role, they are now resources rather than problems” (Benard et al., 2007: 11). Perhaps more than receiving from others, by discovering meaningful ways to contribute to the needs of others, a higher level of social responsibility can build one’s innate capacity for altruism. As the individual interviews addressed future ambitions and the motivations behind vocational selection, 63% mentioned social affinity. Secular researchers have found “altruism to be one of the important factors in young people joining and staying in a long term program” related to HIV treatment and programming (Rogers, 2003: 192–203). During the individual interviews, we asked each participant: It’s not [my friends’] mistake that they are infected by HIV. I like people that are infected with HIV more than those that aren’t. I want to be friendly with them and spend time with them. (16-year-old female) Counseling allows everyone to manage their problems and allows you to open up to people more with struggles. (15-year-old female (after the passing of her father and receiving help/counseling from a World Vision staff, Jayaraj, she asked him if he could “be like a new father” to her)). I have two close friends in this program and feel more comfortable sharing my struggles with them. We are all the same and it is like family for me. (14-year-old male) [This program] boosts my confidence to face society. After coming here I learned about awareness of this struggle and I am motivated to help people with this. (19-year-old female)
This peer-to-peer approach to counseling not only can facilitate deeper mutual healing through solidarity, but it also expands the capacity for altruism. During the focus group discussions in Tiruvallur, one group shared that the best counseling advice would be: “Don’t discriminate them, and keep them with you. The best thing you can do is to be with them.” While two-thirds emphasized utilizing relationships in their advice, the other third instead focused on practical actions: “Take tablets regularly and put duty and focus on studying. Don’t think of anything else.” While H Norman Wright elaborates on how altruism promotes resiliency as it internalizes into positive introspection by stating, “the image a person has of himself is determined mostly through his interpersonal relationships … a person’s self-estimate is the result of the interpretations he makes of his involvements with others” (Wright, 1974: 135). It is this relationship that not only enhances the dignity within the child, but also increases their capacity to uniquely improve the social welfare of others facing the same difficulties.
Participating in Vocation Towards a Sense of Hope
A. Finding Hope through Vocation
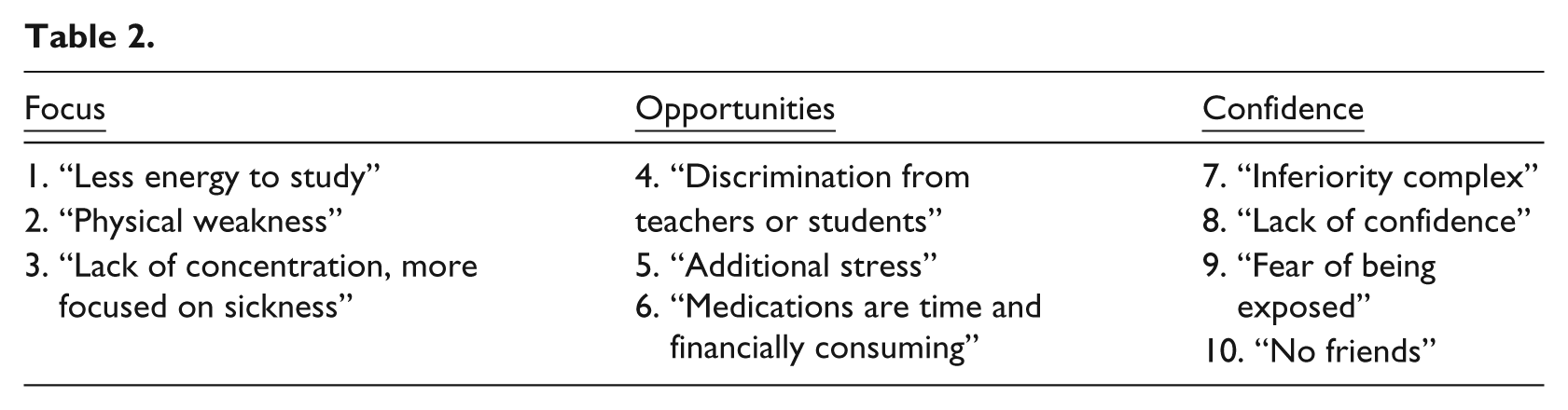
The role of vocation is central to the Christian belief that God has created all people with gifts and talents oriented toward specific purposes and a way of life. A holistic approach to vocational development enables the child to participate, with adequate support, in recovering dignity, discovering gifts/abilities/passions, and pursuing their God-given vocation. A 14-year-old boy aspiring to become a doctor summed up the various hindrances to education for those infected with HIV/AIDS by stating, “The fear of death makes you lose focus on school. You think that you are a sick person, how can I compete against a non-sick person?” As we had the focus groups elaborate on their experienced barriers to education, they responded to this question:
With all of these responses (refer Table 2) reinforcing the “inferiority complex,” these responses consist of physical, social, and psychological stressors that make it challenging to succeed in school. As some have lost a parent or felt isolated in these particular struggles, additional relational support and resources are needed to have confidence to “compete against a non-sick person.” These focus groups unanimously recognized the Life Skills Program as it has helped them to shift their focus away from these hindrances or deficiencies and instead build a confident a sense of ownership over their futures.
B. Discovering Resiliency in Vocational Selection
While this group expressed numerous barriers to vocation, results found that they not only aimed for higher-level aspirations, but also believed that their respective goals were achievable. As each interview asked the child/adolescent what their future goals were, 93% planned on graduating college and only 7% expressed doubts that they could achieve their true vocational ambition due to either low grades/marks or financial constraints. Despite the existing exterior restrictions of this particular group, we must support and nurture inward resiliency, rooted in the hope to flourish, as a source that galvanizes positive change. By looking at Figure 2 below, these white-collar occupation selections, while still not fully estimated or developed, demonstrate a confidence in their capabilities that make these projections realistically attainable to them.
Key motivations behind vocational pursuit as a driver for resiliency centered on affinity (helping others with HIV/AIDS specific issues and creating a better society), helping parents gain household security, and overcoming/redeeming status. Sociologist JA Clausen argues that adolescent “planful competence,” or the “thoughtful, assertive, and self controlled processes that underlie choices and the pursuit of life goals,” represent a critical resource that facilitates vocational choices that “establish relationships and institutional commitments that endure into adulthood and provide the context for achievement and satisfaction” (Clausen, 1991: 805, 842). As vocation is deeply integrated with identity formation, especially in relation to this target group’s unique barriers and stage of life, we must learn to instill confidence as they move towards their hopes and dreams. Erikson explains that this self-perception in relation to the future is largely solidified during the developmental stage of “Industry vs. Inferiority” in early adolescence (Erikson, 1963: 36). With adults providing support and guidance with high expectations during this stage, participatory development fosters “industry” for their understanding of the future, which can be further solidified as they discover confidence in their ability to achieve vocational goals. Rhodes and Lowe’s longitudinal study on Youth Mentoring and Resilience: Implications for Practice looked at the role of mentorship, characterized by “longevity, closeness, clear expectations, support and follow-up with goals,” in producing consistent and positive outcomes (Rhodes and Lowe, 2008: 11).
Spirituality and the Process of Transforming Identity
A. The Internalized Outcome of a “Spoiled” Identity
With this demographic experiencing HIV/AIDS during a critical stage of identity formation, social stigma often becomes internalized leading to feelings of isolation, depression, and hopelessness. Erving Goffman, an expert on the psychological impacts of social stigma, famously described it as “a process by which the reaction of others spoils normal identity” (Goffman, 1963: 18). The various exclusions due to this world’s marred sexuality, exploitation, and covenantal relationships have radically drifted from God’s original design for humanity. Below are a few responses that illustrate how social isolation, suffering, and physical restrictions have been internalized in such a way that it disrupts their self-perception:
When I see a healthy child, I always think why am I not like them. They aren’t infected, why did I have to be born infected? (16-year-old male) I have faced endless problems with HIV. I used to ask my parents if there is a real god in the world. Why did I have to go through all of this suffering as a kid? I used to cry and ask, why did I deserve to get this disease? My mother never gave me a good answer. (13-year-old female) I feel a lot of abuse from the stigma in society. My family is often treated poorly. I remember when food was served to them in a plastic dog plate because of their status. This really changed me. (22-year-old female) My grandma didn’t talk to me much when she found out I was infected. She discriminated me and I felt like an outcast. (13-year-old female) I am most happy when I am home. The hardest struggle for me is my condition and how people view me because of it. (12-year-old male)
While having children as recipients can provide short-term material provision, work with children and adolescents needs to be holistically nuanced in order to reverse the entanglements of disempowerment. Tollestrup highlights the consequences of this perpetuation by stating, “where empowerment is absent, the sense of worthlessness can become internalized … one of the most tragic, debilitating, and anti-developmental byproducts of poverty” (McConnell et al., 2007: 190). As we have previously discussed the role of vocation, how is it to be nuanced in order to reverse this “spoiling” of self-understanding? Benard proposes that true resilience, as it centers on identity, is to learn how to properly view and use one’s innate capacities, in the context of relationships and vocation, toward developing long-term “personal lifelines to overcoming adversity” (Benard et al., 2007: 184). Bryant Myers expands on this to describe the goal of transformational development by stating, “no transformation can be sustainable unless this distorted and disempowering sense of identity is replaced by the truth. Healing the marred identity of the poor is the beginning of transformation” (Myers, 2011: 178). The next section will further explore how this transformation is realized through shifts in worldview and becoming participants in the Kingdom of God.
B. Nuancing “Religious Coping” Towards Resiliency
As children/youth infected with HIV/AIDS are often isolated in suffering, having a personalized individual faith is perhaps the most tangible form of immediate comfort and encouragement. As spirituality was discussed only during the individual interviews due to confidentiality, 76% of participants mentioned spirituality as a form of coping, which was even higher than interpersonal coping with family or friends. Furthermore, spirituality has also been found to be critical in understanding both how and why to persevere through long-term adversity. According to the Commission of Children at Risk secular research study in 2003, “children are hardwired for enduring attachments to other people and for moral and spiritual meaning … as they are psychologically seeking ultimate answers” (Benard et al., 2007: 79–80). Here are examples of how spirituality is a method for the human desire for comfort and peace:
I’m only comfortable sharing my problems with God. I have good trust with Him. I treat God like my own friend. I can talk to Him about anything. (17-year-old female) Prayer exercises in the sessions help me a lot and gives me peace when I think about Jesus hearing my requests. (15-year-old female) Even though I come to World Vision and go to a Christian school, my views are still the same. I am still Hindu. Although I do talk to Jayaraj (WVI staff) when my struggles get bad, I usually keep it in. Because of my family’s status I cry for them. If I feel sad or guilty, I like to meditate and it makes me feel better. (17-year-old female) I think and pray to Jesus when life gets hard. (12-year-old male)
Community psychologists searching for effective empowerment strategies affirm this by recognizing that empowerment is essentially worldview-related (Rappaport, 1987: 139–142). Rather than avoiding the harsh realities of living with HIV/AIDS, how do programs successfully empower children/adolescents in their worldviews towards overcoming these realities? Charles Kraft highlights the significance of worldview, as it is the “framework to explain, evaluate, validate, prioritize commitments, interpret, integrate and adapt to various realities and pressures of life” (Kraft, 1989: 183). As the previous responses demonstrate a resolve to rethink circumstance, there is an implied need for an integrated approach that uniquely expands worldviews towards resiliency by addressing the restrictors and enhancers of religion. Pargament’s study highlights the many religious framings that can possibly negatively shape one’s experience of distress (depression, trauma) and response to suffering (disclosure, coping styles, socialization): judgment or punishment for my wrongdoing, Satanic/supernatural attacks, any perception of God’s absence or abandonment, disconnected or contradictory to worldview, or an inevitable fate to be embraced (Pargament, 1997: 224–231). As redemption is central to the Christian understanding of identity, and thus resilience, how are we to confront and negotiate worldview inadequacies that may perpetuate an irredeemable or worthless self-perception? Developing tools for coping that are contextualized to both the reason and response to suffering can promote a healthy view of self that can respond with resiliency to negative life events.
C. Discovering the Imago Dei as Participants in the Kingdom of God
By defining resilience as a pattern of “stable longitudinal functioning following adversity” rather than an “absence of dysfunction,” psychologists Mancini and Bonanno focus on positively managing “personality variables, coping strategies, self-views, implicit beliefs, and attachment dynamics” that influence long-term pathways (Bonanno and Mancini, 2004: 84). As we have previously addressed the nature of “self-views” and “coping strategies,” these all directly influence healthy relational attachments, especially as it relates to God. Every child is made in the image of God with the right to dignity (instead of stigma/isolation), security (instead of no healthcare or shelter), and purpose (instead of displaced vocation). The end goal of development is more than self-esteem or even a successful career. More than helpful secular approaches to development, God’s kingdom involves discovering our true identity as children of God in restored relationships. The process of discovering and continually rediscovering God’s intention of our humanity through material or spiritual wellbeing creates windows for us to see ourselves within God’s story. Myers adds that “the key to moving toward this better future of shalom and abundant life is the discovery that the community’s story, and our story, can in fact become part of this larger story, the story of God’s redemptive and restorative work in the world” (Myers, 2011: 176). Here are a few examples of how children/adolescents have experienced this intersection of stories as they participated in World Vision’s GRACE project:
This World Vision program is a key time for my friends to search for God. While raising awareness, you must also have moral teachings and learn about God since He is our true need. They need God at this point to get through this. Without God, my life would be miserable. (22 year-old-female) Getting all of this help from World Vision and seeing my friends care for me here has been evidence that a God is there. I have seen other people like me go to Him for help. (13-year-old female) I have learned that Jesus is good through World Vision, but I still want to follow the Hindu tradition of my family. (17-year-old male)
Conclusion
As each child interviewed displayed a search for healing, meaning, and purpose in their present circumstance, we must conclude by not only affirming the need for each holistic component, as previously discussed, but also recognizing the critical role of transformational development. Spirituality isn’t an instrumentalized domain of well-being, but instead deeply embedded in all components of one’s life. Theologian Jürgen Moltmann expands on this transformation by pronouncing the ultimate redefining redemption of God:
This source of power, that is God active in history, including the history of the poor, enables the poor to ‘imagine the future anew,’ bringing a new sense of dignity where the poor are no longer the passive objects of oppression and humiliation; they are now their own conscious subjects … [with] the assurance of their indestructible dignity in God’s sight. (Moltmann, 1993: 101)
Our work is not only to deal with people’s physical needs, but also to heal their marred identity as they engage in society and vocation. Resiliency is ultimately developed through living in light of discovering one’s self as the Imago Dei or “image of God,” which is inextricably linked to one’s participation within the Kingdom of God. As Jesus is the true reflection of our true humanity, a restored relationship with the Creator (through Christ) enables us to reinterpret our powerlessness towards unchanging dignity as children of God.
Footnotes
Acknowledgements
Special acknowledgments to the World Vision India National Office for allowing this study to take place and to all of the staff and community members who have supported and participated in all levels of this research. In particular, thank you to Jayakumar Christian, Ashis Swalsingh, Vijay Edward, Anjana Purkayastha, Jovitta Xavier, and Karen Gonzalez for their leadership in coordinating this study and/or providing valuable feedback to this report. Additionally, Francina Smith and the GRACE Project field staff offered training, organization, and critical technical guidance for the entire research process. Jayaraj Veeraraghavan and Sam Martin Manokaran were instrumental in orchestrating the logistics and translation for the focus groups and interviews conducted at their respective sites in Adambakkam and Tiruvallur. Rita Dhanabalan provided assistance throughout the process of transcribing recorded interviews and preserving linguistic accuracy for the responses used in this study. Lastly, the 48 children/adolescents from Adambakkam and Tiruvallur were central to this study’s outcome as they were not only transparent with their personal experiences, but also innovative in offering concrete feedback on how GRACE Project can enhance intrinsic resiliency. This document has not been endorsed by those listed in these acknowledgments, both with Fuller Seminary and World Vision, and therefore does not necessarily reflect consensus by all members on its consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.