
Abstract
Perceiving one’s romantic relationship as socially marginalized (i.e., as lacking social approval and acceptance) has been linked to an array of worse relational outcomes, including a greater likelihood of breakup. The present research extended this line of work by examining whether individuals who perceive disapproval specifically because of their current romantic relationship tend to experience worse personal health as well. Using an internet-based sample of romantically involved individuals, this study revealed that perceived marginalization of one’s relationship was associated with reporting more symptoms of poor physical health, as well as lower self-esteem. Each of these associations was mediated by negative affect. Moreover, perceived marginalization was directly associated with engagement in riskier health behaviors, including more cigarette smoking and less frequent condom use. These associations remained, even when controlling for important personal and relationship characteristics. Thus, perceiving that one’s relationship is socially marginalized is associated with worse health outcomes for the partners involved.
Individuals who perceive their romantic relationships as socially marginalized (i.e., as the targets of disapproval by their social networks and/or society at large) tend to experience worse outcomes compared to those who see their relationships as garnering greater social acceptance (Lehmiller & Agnew, 2006, 2007). To date, research has only addressed the potential threats of perceived marginalization to relationship wellbeing, particularly level of romantic commitment and likelihood of relationship dissolution. It remains unclear what implications perceived marginalization might have beyond that, particularly with respect to the personal health of the partners involved.
At least two distinct lines of research might predict that partners who perceive a lack of relationship acceptance would report experiencing worse health. First, perceiving greater social network support for one’s relationship has been linked to better physical and mental wellbeing (Blair & Holmberg, 2008). Thus, it would logically seem to follow that perceiving a lack of acceptance and approval for one’s relationship among family and friends (which is conceptually akin, but not identical to low support) would be linked to poor health. Second, persons who perceive prejudice as a result of possessing a stigmatized social identity, such as racial or sexual minority status, tend to experience worse physical and psychological health outcomes (for a recent meta-analysis, see Pascoe & Smart Richman, 2009). Because our relationships often come to be critical social identities in and of themselves (Brewer, 2008; Brewer & Gardner, 1996; Sedikides & Brewer, 2001), one might expect that when our romantic involvements become the targets of bias, we should suffer negative health effects similar to those experienced by persons who are stigmatized on the basis of other self-defining characteristics. Given this rationale, the goal of the present research was to explore whether perceiving one’s relationship as socially marginalized is potentially detrimental to an individual’s health and wellbeing.
Perceived relationship marginalization
Research indicates that the more disapproval perceived with respect to one’s relationship, the worse one’s romantic outcomes tend to be. Specifically, greater levels of perceived marginalization (a construct that broadly assesses perceptions of social disapproval concerning a given relationship) are associated with less commitment to one’s partnership (Lehmiller & Agnew, 2006). Moreover, longitudinal research has revealed that perceived marginalization predicts a greater likelihood of future breakup and, among partners who actually stay together, it predicts decreases in commitment across time (Lehmiller & Agnew, 2007). Thus, perceiving less approval of one’s romantic involvement seems to undermine relationship quality.
The importance of perceived approval (or a lack thereof) for relationship outcomes has been demonstrated in numerous studies spanning more than two decades of empirical work. Although “approval” has gone by many names and has been operationalized a number of ways in the relationships literature, including social support (Sprecher, 1988), social prescription (Cox, Wexler, Rusbult, & Gaines, 1997), and subjective norms (Etcheverry & Agnew, 2004), one basic conclusion is apparent: when others approve of and accept our relationships, they are more likely to succeed compared to when our romances are socially rejected. It is less clear what perceptions of relationship approval or disapproval might mean beyond couple-level outcome variables because essentially no research has considered this possibility. As a result, one important, but unanswered question concerns whether perceiving one’s relationship as socially marginalized might have negative consequences for one’s personal wellbeing.
Perceived marginalization and health
The social support literature provides one basis for predicting an association between perceived marginalization and health because, generally speaking, perceptions of romantic approval/disapproval tend to overlap with perceived support. In particular, greater approval typically accompanies greater support. Certainly, these concepts are not identical (e.g., it is conceivable that a parent might disapprove of their child’s decision to date a member of another race, yet simultaneously offer support for that union by including their child’s partner in family events), but there would appear to be sufficient similarity among these constructs to at least generate tentative inferences.
Although a substantial amount of research has found that generalized social support predicts enhanced physical and psychological wellbeing (e.g., Ross, Lutz, & Lakey, 1999; Uchino, Cacioppo, & Kiecolt-Glaser, 1996), only one study has considered how perceptions of support specifically for one’s relationship are related to personal health. This study focused on perceived social network support (i.e., support by family and friends) and its association with partners’ physical and psychological wellbeing (Blair & Holmberg, 2008). Results indicated that among both same- and mixed-sex couples, greater support for one’s relationship was linked to better personal health. Such findings would thus imply that when individuals perceive the converse (i.e., when they see their relationships as lacking in network approval and/or support), their health might suffer.
Social network members are not the only ones who provide approval and support for romantic relationships, however. Broader, societal perceptions of disapproval might be just as important to consider in this context. The general literature on prejudice and discrimination advocates for this point and provides further evidence for the notion that perceived marginalization of one’s relationship might translate to worse health outcomes. Again, these concepts are not identical (e.g., one’s relationship might be socially disapproved without necessarily being subject to discrimination), but there would seem to be considerable overlap between being the target of disapproval and being the target of prejudice.
A considerable amount of research has documented adverse health implications associated with perceiving oneself as the target of negative bias (e.g., Pascoe & Smart Richman, 2009). In particular, perceiving that one possesses a marginalized social identity (e.g., perceiving racism or sexism) or that one is being treated unfairly because of it is associated with worse physical and psychological health outcomes, as well as greater engagement in risky health behaviors.
As some evidence of this, research indicates that perceived discrimination is linked to worse mental health among lesbian, gay, and bisexual adults (e.g., Mays & Cochran, 2001), African Americans (e.g., Brown et al., 2000), and women (e.g., Pavalko, Mossakowski, & Hamilton, 2003; Schmitt, Branscombe, & Postmes, 2003). Of importance, the longitudinal nature of some of these studies (Brown et al., 2000; Pavalko et al., 2003) has revealed that while perceived discrimination predicts worse long-term mental health, poor mental health does not predict long-term perceptions of discrimination.
Similar associations have been found with respect to perceived discrimination and physical health. For example, among African Americans, perceived racism is linked to worse self-reported physical health (Borrell, Kiefe, Williams, Diez-Roux, & Gordon-Larsen, 2006), and higher blood pressure (e.g., Din-Dzietham, Nembhard, Collins, & Davis, 2004). Among gay and bisexual men, perceived anti-gay discrimination is linked to greater use of non-prescription medication and more physician visits (Huebner & Davis, 2007).
It has long been theorized that the reason minority group members tend to suffer these worse physical and psychological health outcomes is because the experience of discrimination is stressful (e.g., Allison, 1998; Meyer, 2003; Slavin, Rainer, McCreary, & Gowda, 1991). These “minority stress” theories and models suggest that when an individual perceives that one of their social identities is stigmatized (e.g., their race, gender, or sexual orientation), it creates feelings of distress that can undermine their personal health. Because our romantic relationships also constitute important social identities (Brewer, 2008; Sedikides & Brewer, 2001), perceiving that one’s romance is marginalized is theorized to have stress and health effects similar to those experienced by persons who are rejected on the basis of any other identity they may possess. Although this line of reasoning speaks primarily to the stresses associated with broad, societal perceptions of disapproval and bias, it stands to reason that lacking approval from one’s immediate social network (i.e., family and friends) would be similarly stressful and, thereby, potentially detrimental to one’s health.
In addition to the negative health effects of perceived discrimination that stem from increased stress, there is at least one other mechanism through which such bias may threaten health. Specifically, perceptions of disapproval may harm health indirectly by increasing the likelihood that individuals engage in risky acts such as smoking, alcohol use, and unsafe sex. Individuals who perceive that they are the targets of bias often turn to high-risk behaviors as a means of coping with or “escaping” from stress (Martin, Tuch, & Roman, 2003), or because of a lowered ability to resist such activities due to depleted self-control resources (and experiencing stigma decreases ability to engage in self-control; Inzlicht, McKay, & Aronson, 2006). Risky behaviors linked to perceived discrimination include problem drinking (Martin et al., 2003), cigarette smoking (Landrine & Klonoff, 1996), and reduced condom usage (Diaz, Ayala, & Bien, 2004). Based upon these findings, it seems reasonable to predict more broadly that perceptions of disapproval (from society or from close others) would operate in a similar manner (e.g., they might also increase the need to escape stress or lower self-control) and would thus increase engagement in riskier behaviors as well.
In summary, there are several potential health costs associated with perceiving that one possesses a stigmatized social identity and these costs would likely extend to both the context of romantic relationships and perceptions of social disapproval more generally. Also, it seems reasonable to posit that any potential health costs associated with romantic disapproval would be higher to the extent that the relationship is more important and central to one’s sense of self (i.e., if the self-concept has been “expanded” to include one’s partner; Aron & Aron, 1986), given that increased group identification has sometimes been shown to intensify the association between other forms of perceived discrimination and health (e.g., Pascoe & Smart Richman, 2009).
The present research
The literature review presented above suggests that perceiving a lack of relationship approval, whether it is from our social networks or society at large, should have negative implications for partners’ personal health. The goal of the present study was to examine this possibility. An internet study of relationships was conducted, in which a large and diverse sample of romantically involved individuals was obtained. Efforts were not made to recruit individuals in specific types of partnerships, given that the association between perceived marginalization and outcomes has not previously been moderated by relationship type (Lehmiller & Agnew, 2006, 2007). Thus, the present research sought to focus on the perception of marginalization, not specific types of relationships.
The internet was used to facilitate data collection, given that samples obtained online tend to be more diverse compared to traditional college student samples (Gosling, Vazire, Srivastava, & John, 2004). In carrying out this study, best practices in online research were followed with respect to informed consent, debriefing, confidentiality, and checks for duplicate or fraudulent responding (Barchard & Williams, 2008; Gosling et al., 2004).
Hypotheses
First, perceived relationship marginalization should be associated with worse physical and psychological health outcomes. Specifically, persons who perceive greater levels of romantic disapproval should exhibit lower self-esteem and report more symptoms of poor physical health.
Second, perceived marginalization should be associated with reporting more negative affect stemming from the relationship. Specifically, perceiving that others do not approve of or accept one’s relationship should generate significant feelings of distress and anxiety centering around the relationship itself. For example, perceiving that one’s relationship is socially marginalized might lead one to feel guilty or ashamed of the partner or relationship. Likewise, it might generate feelings of nervousness or fear that something bad will happen because of the romantic involvement.
Third, this negative affect is expected to mediate the marginalization-health associations. Stress, specifically in the form of increased negative affect, has been previously posited as a mediator between perceived discrimination and health in the broader prejudice literature (see Pascoe & Smart Richman, 2009). Thus, it is expected that perceived marginalization will be related to worse health outcomes by virtue of increased levels of negative affect, particularly emotions such as shame, nervousness, and fear.
In addition to being associated with worse physical and psychological health, perceived relationship marginalization should be associated with greater engagement in risky health behaviors, just as perceived discrimination based on the possession of other stigmatized identities has been linked to worse health habits (Inzlicht et al., 2006; Martin et al., 2003). In the present research, these health behaviors are hypothesized to include more smoking and drinking behavior, as well as a reduced likelihood of practicing safe sex. Negative affect will be explored as a potential mediator of the associations between perceived marginalization and these behaviors.
Finally, it was hypothesized that the association between perceived marginalization and stress (i.e., negative affect) would be moderated by both the degree of self-reported closeness between the partners and their relationship duration. Specifically, the expected positive correlation between perceived marginalization and stress should be stronger among individuals who report being closer to their partners and/or who have been in relationships of longer duration, compared to individuals who are not as close or who have not been with their partners as long.
All of the hypotheses advanced above are expected to hold, even when controlling for a number of potentially important personal and relational demographic variables. One might expect personal factors such as age, race, sex, and sexual orientation to be related to health status and behaviors. For example, older persons tend to be in worse health and typically utilize more healthcare than younger persons. Likewise, there are variations in health status among persons of different races and sexual orientations, at least partially as a result of differential experiences with discrimination (e.g., Borrell et al., 2006; Huebner & Davis, 2007). One might also expect relational factors such as cohabitation status and level of relationship secrecy to be consequential for health. For example, persons who are keeping their relationships secret tend to exhibit worse health, at least partially as a function of the inherent stress associated with hiding their involvement (Lehmiller, 2009). Although those who see their relationships as marginalized may be more likely than average to keep their romances secret, the associations between marginalization and health are not expected to be solely a function of engaging in secrecy because the perception of romantic disapproval should generate stress in and of itself. In summary, even when all of these factors are taken into account, it is expected that marginalization will still have unique associations with all of the health outcomes assessed.
Method
Participants
Participants were 834 romantically involved individuals (626 women, 207 men, 1 unspecified gender). The sample was relatively diverse in terms of age (M = 23.78, SD = 8.12; range = 18–59), race/ethnicity (7% Asian, 8% Black, 75% Caucasian, 6% Hispanic, 4% other), and sexual orientation (85% heterosexual, 5% homosexual, 9% bisexual, and 1% other). With respect to relationship characteristics, the average relationship duration was just over two years (M = 24.99 months, SD = 36.23 months; range = less than 1 month to 474 months), and most participants indicated that they were not cohabiting with their partners (81% non-cohabiting, 19% cohabiting). Approximately 10% of the sample indicated that their relationship was same-sex, 22% indicated it was interracial, and 9% indicated it was age-gap (i.e., there was a difference of more than 10 years in age between the partners). When accounting for the fact that there was some overlap in these characteristics across relationships, about one-third (34%) of the sample could be described as being involved in a non-traditional relationship (Lehmiller & Agnew, 2006). All participants were recruited online and were not compensated for their participation.
Following the advice of Gosling et al. (2004), the data were examined for repeat internet protocol (IP) addresses, which were automatically recorded when participants submitted their completed surveys. IP addresses are unique identifying numbers associated with particular computers linked to the internet at particular points in time. A single IP address associated with multiple lines of data may be an indicator that the same individual has completed the questionnaire more than once. To account for this, data were excluded when the same IP address appeared more than once. Approximately 3% of all data submitted were excluded for this reason and are not reflected in the final sample of 834.
Materials
For each multi-item measure described below, a composite score was calculated by averaging responses to all items, after reverse-scoring responses to any necessary questions or statements. Higher scores therefore reflect higher levels of the described construct. In order to enhance participation and completion rates of the survey, many of the measures administered were shortened from their original forms, a common practice in online research (e.g., Lehmiller; 2009; Lehmiller & Agnew 2006, 2007). To ensure that these shortened scales did not negatively impact any measure’s reliability, Cronbach’s Alphas are reported for each scale used in the present research.
Perceived marginalization
To measure perceived relationship marginalization, a four-item inventory developed by Lehmiller and Agnew (2006) was used (α = .80). The items included “My relationship has general societal acceptance” (reverse-scored), “My family and friends approve of my relationship” (reverse-scored), “I believe that most other persons (whom I do not know) would generally disapprove of my relationship”, and “My family and/or friends are not accepting of this relationship”. These items were rated on a nine-point scale ranging from 1 (not true at all) to 9 (very true). Although this measure appears to consist of two subscales assessing different forms of perceived marginalization (i.e., social network vs. society), Lehmiller and Agnew (2006) reported findings of a factor analysis indicating a one-factor solution. Consistent with their results, an exploratory factor analysis with maximum likelihood extraction and promax rotation was conducted with the present data and revealed that all items loaded on a single factor explaining 62% of the item variance. Consequently, it did not appear empirically justifiable to subdivide the measure in order to explore different forms of marginalization.
Please note that although this measure takes into account different sources of social disapproval, it does not necessarily address why a given relationship is subject to reduced acceptance. Thus, some participants who score high on this measure may do so because their relationship is non-traditional (e.g., it is same-sex or interracial), while others may do so for completely different reasons (e.g., one of the partners is perceived as interpersonally unpleasant).
Self-esteem
A shortened version of the Rosenberg Self-Esteem Scale was administered (α = .78) (Rosenberg, 1965), which included the following four items: “On the whole, I am satisfied with myself”, “At times, I think I am no good at all” (reverse-scored), “I feel that I have a number of good qualities”, and “All in all, I am inclined to feel that I am a failure” (reverse-scored). Participants indicated their agreement with these items on a seven-point scale ranging from 1 (do not agree at all) to 7 (agree completely).
Symptoms of poor health
As a proxy for physical and psychological health status, participants completed a widely used symptom checklist. Specifically, a shortened version of the Hopkins Symptom Checklist was administered (α = .88) (Derogatis, Lipman, Rickels, Uhlenhuth, & Covi, 1974). Instructions for this measure read: “Below is a list of symptoms and complaints that people sometimes have. Read each symptom carefully, then select the numbered descriptor that best describes how much discomfort that problem has caused you during the past week including today”. A list of 10 symptoms that were randomly selected from the full scale followed, including “headaches”, “loss of sexual interest or pleasure”, “nausea or upset stomach”, “heart pounding or racing”, “feeling blue”, “nervousness or shakiness inside”, “feeling low in energy or slowed down”, “feeling easily annoyed or irritated”, “feeling lonely”, and “poor appetite”. Participants rated the degree to which they had experienced each symptom on a seven-point scale ranging from 1 (not at all distressed) to 7 (extremely distressed).
Risky health behaviors
Participants completed one-item measures of recent smoking, drinking, and safer sex behaviors. To assess smoking behavior and drinking behavior, participants were given time-line follow-back measures in which they were asked to recall the approximate number of cigarettes smoked and alcoholic drinks consumed in the past week. Such measures are frequently used to assess risky acts of this variety, although they are somewhat limited in that participants will often underreport their behaviors (Shiffman, 2009). First, participants were asked, “This past week, approximately how many cigarettes did you smoke?” Responses to this question were reported on a five-point scale that included zero (coded as 0); one or two (coded as 1); more than two, but less than half a pack (coded as 2); more than half a pack, but less than a whole pack (coded as 3); and more than a whole pack (coded as 4). Second, participants were asked, “This past week, approximately how many alcoholic drinks did you consume?” Responses to this question were reported on a five-point scale including zero (coded as 0); one (coded as 1); more than one, but less than five (coded as 2); more than five, but less than ten (coded as 3); and more than ten (coded as 4). Lastly, to assess safer sex behavior, participants were asked, “Did you and your partner use a condom the last time you had sexual intercourse?” Participants could indicate yes, no, or my partner and I have never had sexual intercourse. Participants who have never had sexual intercourse with their current partner (23% of the sample) were excluded from the analyses considering condom use. Recent condom use was therefore treated simply as a dichotomous variable coded as 0 for yes or 1 for no. This item was based on past research assessing risky sexual behaviors, in which recent condom use has been assessed with a binary variable in relation to last intercourse (e.g., Senf & Price, 1994). Also, although lack of condom use in the context of a long-term romantic relationship might not necessarily be perceived as “risky” to the couple members themselves, it does carry some degree of risk, given the high prevalence of infidelity (for example, some studies have reported the prevalence of infidelity to be as high as 85.5%, although prevalence rates certainly vary based upon how infidelity is defined and the samples obtained; for a review, see Luo, Cartun, & Snider, 2010).
Negative affect
To assess the degree of negative affect generated by the relationship itself, participants completed a modified version of the Positive and Negative Affect Scale (PANAS) (Watson, Clark, & Tellegen, 1988). The instructions were revised to focus on affect stemming specifically from one’s romantic relationship, and participants were only presented with a subset of eight negative affect items (α = .89). The instructions were: “The following scale consists of a number of words that describe different feelings and emotions. Read each item and then select the appropriate answer next to that word. Indicate to what extent you have felt this way because of your partner or relationship during the past week”. Participants rated the extent to which they had felt the following emotions on a scale ranging from 1 (very slightly or not at all) to 7 (extremely): distressed, upset, guilty, scared, jittery, ashamed, nervous, and afraid.
Potential moderators and covariates
Several other measures were administered because they were theorized to have potential value as either covariates or moderator variables. First, participants completed the Inclusion of Other in the Self (IOS) Scale (Aron, Aron, & Smollan, 1992), which measures the degree of emotional and behavioral closeness to one’s partner. The IOS measure instructs participants to “look at the image below and indicate which pair of circles best describes your relationship with your partner by selecting the appropriate number”. Afterwards, participants were presented with seven Venn diagrams that represent different degrees of self–partner overlap. Response options for this measure ranged from two completely separate circles (1) to two circles that almost completely overlap (7).
Next, participants completed a measure of relationship secrecy. This measure was created specifically for the present research and consisted of five items designed to assess the degree to which participants were hiding their relationship from social network members and from society at large (α = .92). The items included “I am trying to keep my relationship secret from people I care about”, “I am trying to keep my relationship secret from people I frequently interact with”, “I am trying to keep my relationship secret from certain family members”, “I am trying to keep my relationship secret from some of my friends”, and “I try to keep my relationship secret when out in public”.
Finally, participants answered several demographic questions about themselves and their current relationship, including questions about age, gender, sexual orientation, race/ethnicity, relationship duration (assessed in number of months), and cohabitation status (coded as either 0 for not cohabiting, or 1 for cohabiting).
Procedure
The internet survey was accessible via links posted on various websites, with the majority of participants coming from Facebook (www.facebook.com) and the Social Psychology Network (www.socialpsychology.org). Advertisements identified this as a study of relationships and indicated that persons involved in any type of romantic relationship were welcome to participate. Aside from involvement in a current relationship, the only other requirement for participation was being 18 years of age or older.
When participants arrived at the questionnaire website, they were first prompted with a consent button. Upon providing consent, participants were presented with the measures described above. Before completing these measures, participants were told that if they were currently involved in more than one romantic relationship that they should complete the survey with only their most significant partner in mind. This was to ensure that participants answered all questions in terms of the same relationship. After completing the survey, they were directed to another page thanking them for their participation.
Results
The primary analyses reported below do not include any covariates; analyses with control variables are addressed in the Ancillary Analyses section. Table 1 presents intercorrelations among the key study variables, along with their means and standard deviations.
Intercorrelations among key study variables
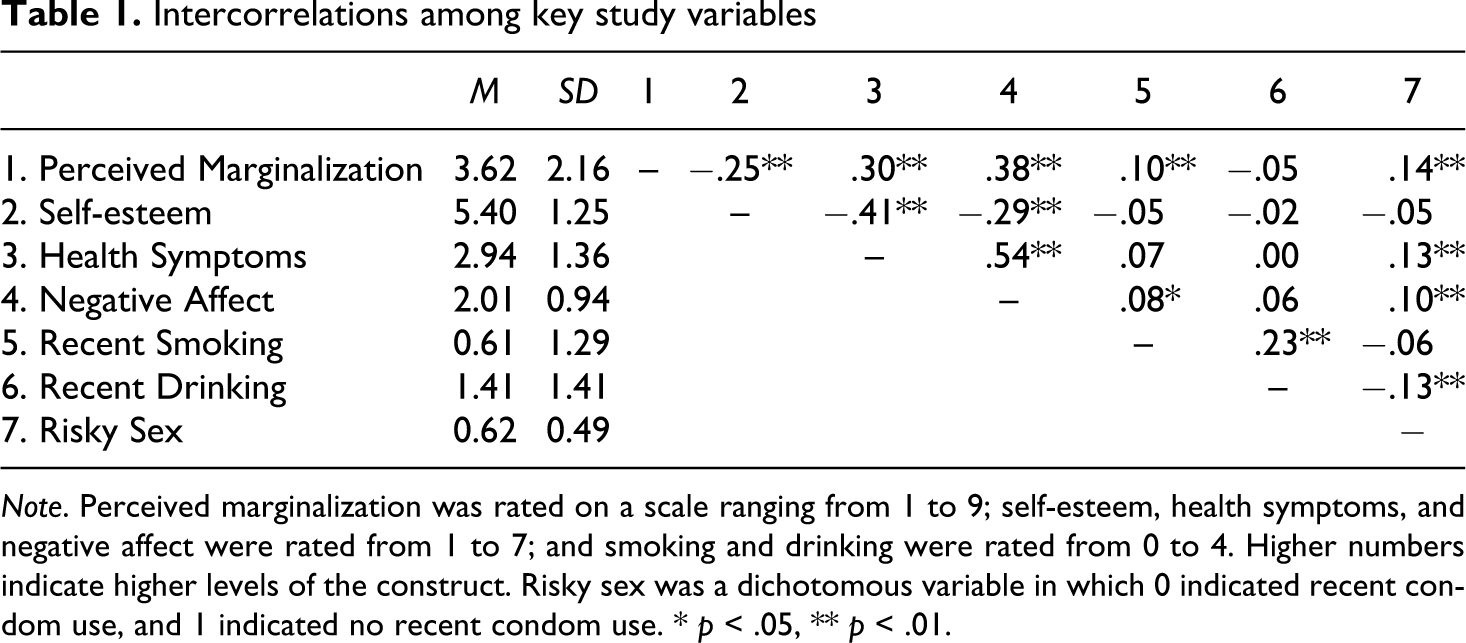
Note. Perceived marginalization was rated on a scale ranging from 1 to 9; self-esteem, health symptoms, and negative affect were rated from 1 to 7; and smoking and drinking were rated from 0 to 4. Higher numbers indicate higher levels of the construct. Risky sex was a dichotomous variable in which 0 indicated recent condom use, and 1 indicated no recent condom use.
* p < .05,
** p < .01.
Marginalization and self-reported health
Consistent with hypotheses, multiple regression analyses revealed that perceived relationship marginalization was associated with lower self-esteem (β = −.25, t (814) = −7.47, p < .001; Cohen’s f 2 = .07), poorer health symptom reports (β = .30, t (814) = 8.89, p < .001; Cohen’s f 2 = .10), and higher levels of negative affect (β = .38, t (818) = 11.91, p < .001; Cohen’s f 2 = .17). 1
Next, tests for mediation were conducted using procedures outlined by Baron and Kenny (1986). Specifically, these multiple regression analyses considered whether negative affect mediated the link between marginalization and the health outcomes assessed. The first set of analyses considers self-esteem as the outcome variable. Consistent with mediation criteria, marginalization was significantly associated with both self-esteem and negative affect (see above). Also, negative affect was significantly associated with self-esteem when marginalization was included simultaneously in the model (β = −.23, t (813) = −6.48, p < .001), such that greater negative affect was associated with lower self-esteem. Finally, the association between marginalization and self-esteem declined in magnitude when controlling for negative affect (β = −.16, t (813) = −4.53, p < .001), suggesting partial mediation. Results of a Sobel test corroborated these findings (z = −5.67, p < .001).
The second set of analyses considered symptom reports as the outcome variable. As noted above, marginalization was significantly associated with both symptom reports and negative affect. In addition, negative affect was significantly associated with symptom reports when marginalization was included simultaneously in the model (β = .50, t (813) = 15.84, p < .001), such that greater negative affect was associated with more reported health symptoms. Lastly, the association between marginalization and symptom reports decreased when controlling for negative affect (β = .10, t (813) = 3.20, p = .001), indicating partial mediation. Results of a Sobel test corroborated these findings (z = 9.52, p < .001). The pattern of results across both sets of mediation analyses suggests that marginalization may potentially harm one’s physical and psychological wellbeing by means of generating negative emotions.
Marginalization and self-reported risky health behaviors
With respect to health behaviors, results of multiple regression analyses indicated that greater perceived marginalization was associated with more cigarette smoking in the past week (β= .10, t (817) = 2.77, p = .006; Cohen’s f 2 = .01), but was unrelated to recent alcohol use (β= −.05, t (817) = −1.31, ns). Additionally, results of a logistic regression analysis revealed that perceived marginalization was associated with reduced condom usage among those participants who were sexually active with their partners (unstandardized B = .12, odds ratio = 1.12, Wald χ 2= 8.19, p = .004). Thus, greater perceived marginalization was associated with engaging in at least some riskier health behaviors.
Mediation analyses were conducted to determine whether negative affect mediated marginalization’s links with smoking behavior and condom usage. Results indicated that negative affect was not associated with any of the health risk behaviors when marginalization was statistically controlled. Mediation criteria were therefore not met in either case. Thus, there was indeed an association between marginalization and these risky health behaviors, but negative affect failed to account for this.
Moderation by relationship closeness
Next, both relationship closeness (as assessed by IOS scores) and duration were examined as potential moderators of the association between marginalization and negative affect following procedures suggested by Aiken and West (1991). After centering all variables, the appropriate interaction terms involving marginalization and each of the potential moderating variables were created. Next, all of the relevant terms (i.e., marginalization, the moderating variables, and their interactions) were added simultaneously in separate regression models predicting negative affect. When interactions emerged as significant, they were probed by calculating simple slopes at one standard deviation above and below the mean of the moderating variable.
Results indicated that marginalization and perceived relationship closeness significantly interacted in a regression model (β = .27, t (3, 796) = 2.58, p = .01). In interpreting this interaction, it should be noted that there was a significant positive association between marginalization and negative affect regardless of level of perceived closeness to one’s partner. Nonetheless, this association was stronger at higher levels of closeness (simple slope = .19, t (809) = 9.60, p < .001) than it was at lower levels of closeness (simple slope = .12, t (809) = 6.23, p < .001).
Contrary to expectations, the interaction between marginalization and relationship duration did not achieve significance (β = −.02, t (3, 815) = −0.23, ns). Although the closeness and duration results appear to be inconsistent with one another, it is important to note that these variables were only slightly related to each other (r = .09, p < .01). Thus, having a longer-term relationship does not necessarily mean that the partners are exceptionally close.
Ancillary analyses
All of the above analyses were repeated using a variety of demographic and relationship variables as covariates. These included participant age, race (a binary variable categorized as White vs. non-White), sex, sexual orientation (a binary variable categorized as heterosexual vs. non-heterosexual), cohabitation status (a binary variable categorized as cohabiting vs. non-cohabiting), and level of relationship secrecy. Prior to conducting these analyses, all six potential covariates were tested as moderators of the association between marginalization and each outcome variable in order to determine whether the assumption of equal slopes was met. Only participant age failed to meet this assumption, given that it significantly interacted with perceived marginalization in predicting the binary condom use variable (unstandardized B = −.02, Wald χ 2 = 7.12, p = .008) 2 . Simultaneous inclusion of the remaining five control variables did not substantially modify the results of any of the analyses presented above, including tests for mediation (i.e., all significant results remained significant; non-significant results remained non-significant).
Discussion
Consistent with predictions based upon the social support and prejudice literatures, results indicated that individuals who perceived greater levels of marginalization specific to their current relationship tended to express lower levels of self-esteem and more symptoms of poor health. These associations were at least partially mediated by negative affect, suggesting that one possible reason marginalization may contribute to worse health is because it is stressful. These findings remained significant even when controlling for several important personal and relational characteristics. In particular, it is notable that all associations held even when controlling for level of relationship secrecy, which has been shown to relate to health outcomes in past research (Lehmiller, 2009). Thus, it does not appear to be the case that marginalization is related to health simply because marginalized partners are keeping their relationships secret.
It appears that any potential implications of perceived marginalization for health may be compounded by increased engagement in risky health behaviors. The present study revealed that greater perceived marginalization was associated with increased cigarette smoking, as well as a reduced likelihood of condom use. Contrary to expectations, no association was found between perceived marginalization and recent alcohol use. Potential explanations for this null result are addressed below (see Strengths and Limitations section).
Unexpectedly, neither of the marginalization–risk behavior associations was mediated by negative affect. There are several possible post hoc explanations for this. First, it could be that the appropriate mediating variable was not assessed. In the case of relationship marginalization, perhaps depleted self-control resources (which have been documented among persons experiencing other types of stigma; Inzlicht et al., 2006) could explain this result. Alternatively, it could be that the negative affect measure administered in the present research was not broad enough (e.g., perhaps emotions such as anger or sadness are the driving factor behind engagement in unhealthy behaviors). Second, a recent meta-analysis of perceived discrimination and health (Pascoe & Smart Richman, 2009) speculated that, although perceived discrimination has an indirect effect on overall health status via stress, its effect on health behaviors may be direct, or at least mediated by something other than stress responses. Viewed in this light, the lack of mediation in the present research is perhaps unsurprising. Nonetheless, it is an issue worthy of study in future research.
It is also noteworthy that the association between perceived marginalization and negative affect was moderated by perceived closeness to one’s partner. This finding suggests that any association between marginalization and stress may become more pronounced as the partner becomes a more integral part of the self. A corresponding finding was not found for relationship duration; however, relationships of longer duration are not necessarily characterized by enhanced closeness. Indeed, as noted in the Results section, these variables were only very weakly correlated. Instead of duration, perhaps it would have been more informative to consider relationship status (e.g., dating vs. partnered) or seriousness of the involvement as potential moderating variables. Nonetheless, the closeness results are consistent with the notion that as perceived closeness to one’s partner increases, perceived marginalization of one’s relationship may become all the more harmful.
In general, the effect size estimates for the associations between perceived marginalization and health tended to fall in the small to medium range when compared to conventional standards. This is generally consistent with the size of the meta-analytic correlations observed between other forms of discrimination and health (Pascoe & Smart Richman, 2009). However, bigger effects were observed for the general health indices (self-esteem, symptoms, and negative affect), and smaller effects were observed for the behaviors. This makes sense, given the limitations of the health behavior measures, which are discussed below (see the Strengths and Limitations section).
These findings have several important implications. First, perceiving that one’s relationship is socially marginalized is not an uncommon experience, and there are any number of reasons why others might disapprove of a given relationship. Despite this, however, many of these relationships survive. Future research would therefore be well served by exploring both individual- and relational-level factors that might potentially buffer the stress of perceived marginalization, thereby alleviating any negative outcomes.
As a starting point, it might be useful to study individuals who have managed long-term marginalized relationships in order to determine what factors may have protected the health of the couple members and their relationship from the strain of social rejection. It is possible that, at least for some couples, the shared experience of marginalization might actually increase relationship closeness, thus reducing stress. The rejection-identification model (Branscombe, Schmitt, & Harvey, 1999), although traditionally applied to intergroup contexts, suggests that when minority group members are willing to make attributions to prejudice, it tends to increase group identification, thereby buffering psychological wellbeing. Applying such a model to the study of marginalized relationships might prove to be of great value in explaining why some of these relationships persist.
In addition, it might be useful to explore individual difference factors that are generally associated with a greater ability to recover from stress, such as psychological resilience (e.g., Ong, Bergeman, Bisconti, & Wallace, 2006), as well as more specific factors that have been shown to be effective at reducing the detrimental effects of other forms of perceived discrimination (e.g., racism, sexism) on health, including having a larger social support network and/or taking an active or problem-focused approach to coping (Pascoe & Smart Richman, 2009).
Given the negative associations between perceived marginalization and partners’ health, combined with results suggesting that these associations tend to increase in strength as partners become closer, another implication of these data is that ending a marginalized relationship could potentially bring health benefits to the partners involved by virtue of removing a chronic source of stress. Longitudinal research would be useful for exploring this intriguing possibility. Such research could also be used to address the question of why some people stay in marginalized relationships over time, despite all of the potential costs. Perhaps marginalized relationships have to be especially high-functioning in order to survive and buffer individuals from the stress of social disapproval. Alternatively, persistence in a marginalized relationship might have more to do with individual differences in stress resiliency. By taking a longitudinal approach, we can gain a better understanding of the circumstances under which a marginalized relationship is likely to stand the test of time.
Strengths and limitations
There are multiple strengths of the present research. First, the sample size was quite large and contained reasonable diversity. In particular, there was significant variability in terms of participant age, sexual orientation, and relationship characteristics, which allowed for the examination of several potentially important moderator variables. Certainly, the sample was not as diverse as it could have been, especially given that participants were predominately White, relatively young, and most were not cohabiting with their partners. Whether the results of this research will generalize to older adults and more established relationships is thus an important question for future research. Nonetheless, the present sample’s diversity was still significantly enhanced compared to a typical college student sample. Another important strength of this work lies in the fact that health outcomes were assessed via multiple indicator variables, including psychological wellbeing, health symptoms reports, as well as recent health-relevant behaviors. Of importance, there was a consistent pattern of results across each of these measures (with the exception of alcohol use), which bolsters the theoretical case that perceived marginalization may be consequential for partners’ health. Finally, this research bridges several different research literatures, including close relationships, social support, prejudice and discrimination, and health. As such, it has broad implications and serves to further demonstrate the utility of building connections across research areas that are often separate.
This work is not without its limitations, however. First, only one-item measures were used to assess each of the risky health behaviors. This could potentially explain the lack of an association between perceived marginalization and alcohol use, given that one-item measures tend to be less reliable. In addition, the scale intervals were not consistent, which may have obscured some of the variability. Perhaps most important, because the alcohol use measure did not specify exactly what constitutes an “alcoholic drink”, it is possible that there may have been inconsistencies in how participants responded to the question based upon what they define as one drink. The other risky behavior measures administered (i.e., smoking and condom use) are not subject to this same criticism because there is less ambiguity in terms of what constitutes smoking a cigarette or using a condom. Also, across all risky behavior measures, there was likely to be some degree of socially desirable responding, given that participants tend to underreport engagement in unhealthy behavior (e.g., Shiffman, 2009). In short, the lack of association between perceived marginalization and alcohol consumption could quite plausibly be due to measurement error and thus should not be taken as definitive.
Second, the correlational nature of the data prevents us from making any causal inferences. We cannot conclusively say whether perceived marginalization actually causes worse health outcomes for the partners involved. In fact, one could argue for the reverse causal direction (e.g., lower psychological wellbeing might predict perceptions of marginalization). For example, people who are already feeling badly about their relationship might be more prone to think that others disapprove of it, or they may be biased to attend more to negative rather than positive social information regarding their romance. Alternatively, perhaps persons lower in self-esteem are more rejection-sensitive, which leads them to anticipate more disapproval of their relationship (whether it is real or not).
The general literature concerning discrimination and health would argue against alternative causal processes. For example, at least some experimental research has demonstrated causal effects of perceiving discrimination on psychological wellbeing (Schmitt et al., 2003). Moreover, longitudinal research has found that although perceived discrimination predicts long-term mental health, the reverse is not true (Brown et al., 2000; Pavalko et al., 2003). Thus, the reverse causal direction would not seem to make as much sense from a theoretical standpoint. Nonetheless, future research in this area might consider studying perceived marginalization and health via experimental or longitudinal methods in order to obtain a better sense of the temporal ordering of events.
A related limitation of this research lies in the fact that it does not point to a definitive process by which perceived marginalization might generate stress (i.e., negative affect), given the nature of the stress measure used. It could be the case that perceived marginalization creates generalized negative affect that either (1) spills over to one’s feelings about the relationship, or (2) is mistakenly attributed to one’s partner. Another possibility is that perceived marginalization might generate stress by virtue of negatively impacting the relationship itself. For example, research has shown that perceptions of marginalization longitudinally predict decreases in commitment over time (Lehmiller & Agnew, 2007). To the extent that commitment is reduced, increases in conflict and stress would seem to be a likely outcome. It should also be noted that other processes aside from stress could be contributing to the marginalization–health associations (e.g., depleted self-control resources; Inzlicht et al., 2006). Future research would thus benefit by exploring the specific pathway(s) through which perceived marginalization might contribute to worse health outcomes.
Lastly, this work is limited in that it examined perceived relationship marginalization without taking into account perceived disapproval or stigmatization of other social identities. For some relationship types (e.g., interracial, same-sex), the partners involved may perceive others’ disapproval as stemming from the relationship itself, but they may also perceive significant disapproval or bias as a function of possessing certain personal traits or characteristics (e.g., racial or sexual minority status). As discussed at the outset of this paper, there is a significant amount of research linking identity discrimination to personal health outcomes (e.g., Pascoe & Smart Richman, 2009). Whether perceived relationship marginalization is uniquely associated with health above and beyond perceiving bias due to the possession of other social identities is unclear. In an attempt to address this idea, all analyses in the present research were repeated, controlling for racial and sexual minority status, as well as gender and age. Addition of these covariates did not alter the results of any analyses, suggesting that perceived relationship marginalization does uniquely contribute to health outcomes. In order to more fully address this idea, future research should consider explicitly assessing perceived marginalization with respect to both the relationship itself as well as other pertinent social identities.
Conclusions
The present research indicates that a lack of perceived approval for one’s relationship is linked with a variety of poor physical and mental health outcomes, as well as greater engagement in certain high-risk health behaviors. Thus, perceiving that one’s relationship is socially marginalized appears to have negative implications not only for the romance itself (Lehmiller & Agnew, 2006, 2007), but also for the health of the partners involved. These findings contribute to a growing body of literature indicating that, across diverse contexts, perceptions of marginalization may be consequential for personal wellbeing.
Footnotes
Notes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.