
Abstract
While research evidence has consistently demonstrated the link between social relationships and psychological distress, there is debate over the strength of perceived emotional support compared with perceived negative interaction on psychological distress and whether the relation between social relationships and psychological distress is direct or moderating. In this study, we examined the relation between partner emotional support, partner negative interaction, and trauma on psychological distress. Our sample of married or romantically partnered people was drawn from a nationally representative U.S. data set (N = 5,383). The direct effects of romantic partner emotional support and romantic partner negative interaction on psychological distress were evaluated and compared. Further, we evaluated the moderating effects of partner emotional support and partner negative interaction on the relation between trauma history and psychological distress. Hierarchical regression models revealed that (a) people exposed to trauma experienced greater psychological distress, (b) partner emotional support was linked with reduced distress, (c) partner negative interaction was linked with increased distress, (d) partner negative interaction accounted for more variance in psychological distress compared with partner emotional support, and (e) neither partner emotional support nor partner negative interaction moderated the relation between trauma and distress. These findings indicate that partner negative interaction has a stronger relation with psychological distress than partner emotional support. Further, they support the direct effects of social relationships on psychological distress over the moderating effects.
Despite social relationships having a well-documented relation with psychological distress, explanations for that relation remain contentious (see Cohen, Gottlieb, & Underwood, 2000 for a review). One area of disagreement is the relative relation of perceived emotional support (hereafter referred to as emotional support) compared with perceived negative interaction (hereafter referred to as negative interaction) and psychological distress. In a review of the literature, Lincoln (2000) reported that while the majority of studies indicated negative interaction is a stronger predictor of psychological distress than emotional support, others have found the opposite. Further, meta-analytic evidence indicated that there was no difference in the relation between perceived social support and negative social interaction on psychological distress (Finch, Okun, Pool, & Ruehlman, 1999). Improved understanding of the relative relation of emotional support compared with negative interaction will provide researchers and practitioners with information about where to devote their efforts. The first goal of this study was to help clarify the relative relation of emotional support compared with negative interaction on psychological distress. To do this, we used a large and nationally representative U.S. data set, which allowed for greater statistical power than most studies of these phenomena. We also computed a Pratt index for emotional support and negative interaction, which facilitated a direct comparison between emotional support and negative interaction regarding how much of the variance in psychological distress each accounted for. This method improves on the often—yet inappropriately—used standardized regression coefficient for determining variable importance (for a review, see Thomas, Zhu, & Decady, 2007).
The second goal of this study was to examine whether emotional support and negative interaction had a direct (i.e., main) or moderating (i.e., buffering) relation with psychological distress. While researchers have consistently found direct effects, moderating effects have been inconsistently observed, yet theory assuming moderation continues to dominate the field (Lakey & Orehek, 2011). It has been suggested that researchers have underreported their tests of the moderating effects of social support on psychological distress because of null results (Lakey & Cronin, 2008). As noted above, using a large and nationally representative data set will increase statistical power and bring further understanding of the moderating effects of emotional support.
Direct effects
Emotional support—people’s belief that they are important to or cared for by others—has been identified as one of the strongest correlates with psychological well-being (Ingersoll-Dayton, Morgan, & Antonucci, 1997; Kawachi & Berkman, 2001). Indicators of emotional support include feeling cared for, understood, and listened to (Lincoln, 2000). Emotional support has been linked with reduced psychologically aversive states, such as depression (Sherman, Skrzypek, Bell, Tatum, & Paskett, 2011), panic (Maulik, Eaton, & Bradshaw, 2011), and despair (Thoits, 1995). Additionally, research has indicated that emotional support correlates with increased protective attributes such as effective coping (Cohen, 2004), positive self-view (Cohen & Wills, 1985), and satisfaction with life (Brenner, Norvell, & Limacher, 1989). While the link between emotional support and psychological distress has not been ubiquitously observed (e.g., Rhodes, Ebert, & Meyers, 1994), findings from meta-analyses (e.g., Finch et al., 1999; Ozer, Best, Lipsey, & Weiss, 2003) and systematic review (Lincoln, 2000) have indicated the robustness of their relation.
A destructive component of social relationships—negative interaction—has been linked with psychological distress (Rhodes et al., 1994). Indicators of negative interaction include being criticized, let down, and domineered (Lincoln, 2000). Negative interaction has been associated with increased distress, including depressed mood (Sherman et al., 2011), anxious symptoms (Vinokur & van Ryn, 1993), loneliness (Gant & Ostrow, 1995), and somatic complaints (Cornwell & Waite, 2009; Gant et al., 1993). Additionally, negative interaction, particularly with spouses or friends, has been related to a decreased emotional well-being (Abbey, Abramis, & Caplan, 1985), life satisfaction (Brenner et al., 1989), and positive affectivity (Lakey, Tardiff, & Drew, 1994).
Studies of specific providers of social support have furthered the understanding of the benefits of social support from romantic partners (hereafter referred to as partner support). For example, in a study of pregnant women, those with lower levels of partner support were more likely to experience depressive symptoms (Collins, Dunkel-Schetter, Lobel, & Scrimshaw, 1993). In another study of partner support, providing emotional support was linked with reduced mortality more so than receiving emotional support (S. L. Brown, Nesse, Vinokur, & Smith, 2003). Not surprisingly, studies of the influence of partners’ emotional support have found that partner support was connected with increased relationship satisfaction and was optimized when support was reciprocal (Wright & Aquilino, 1998). The amount of research examining partner emotional support is relatively limited and thus requires further investigation to develop a comprehensive understanding of its functions.
Consistent with studies of negative interaction from other support providers, partner negative interaction has been linked with psychological distress. In a study of couples, partner negative interaction was related to higher levels of psychological distress and divorce (Markman, Rhoades, Stanley, Ragan, & Whitton, 2010). In another study, avoidance of partners’ concerns and feelings was correlated with their partners harboring more negative feelings toward them (Fekete, Stephens, Mickelson, & Druley, 2007). Further, negative interaction in the form of social isolation and feelings of disconnect were related to decreased physical and mental health (Cornwell & Waite, 2009).
In a review of the empirical literature, Lincoln (2000) found that a greater number of studies indicated that negative interaction had a stronger relation than emotional support with psychological distress. In studies comparing the association of emotional support and negative interaction, negative interaction had a stronger relation with depression (Davis, Rhodes, & Hamilton-Leaks, 1997), anxiety (Gant et al., 1993), psychological distress (Rauktis, Koeske, & Tereshko, 1995), and overall psychiatric symptoms (Stephens, Kinney, Norris, & Ritchie, 1987). The absence of negative interaction has also been more related to life satisfaction (Brenner et al., 1989), psychological health (Finch, Okun, Barrera, Zautra, & Reich, 1989), and emotional well-being (Abbey et al., 1985) than the presence of emotional support. Contrarily, some meta-analytic evidence indicated that there were no differences between the relational strength of emotional support and negative interaction with psychological distress (Finch et al., 1999). In a broad review of the psychological literature comparing the impact of good with bad experiences on various emotional and psychological outcomes, Baumeister and colleagues (Baumeister, Bratslavsky, Finkenauer, & Vohs, 2001) concluded that negative experiences—regardless of the domain—have a stronger impact on mental health than positive ones. Further, they suggested that this is evolutionarily adaptive. Specifically, one negative event can more adversely impact survival than one positive event. Thus, strong emotional reactions to negative experiences motivate avoiding these experiences, which increases the likelihood of survival. Applying evolutionary theory to romantic relationships is particularly relevant due to genetic survival—via producing and raising offspring—frequently occurring in this context. While there is evidence of negative experiences relating more strongly to psychological well-being than positive experiences within romantic relationships (Helgeson & Cohen, 1996; Horwitz, McLaughlin, & White, 1997; Rhodes et al., 1994), further study is necessary to extend the understanding of these phenomena.
Trauma and distress
A traumatic event is typically defined as an acute and severe stressful life experience (Wheaton, Young, Montazer, & Stuart-Lahman, 2013). In a population study, over 50% of Americans reported exposure to a traumatic event during their lives (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). While approximately 7% of the U.S. population develops posttraumatic stress disorder (PTSD; Kessler et al., 2005), subclinical levels of distress, resulting from trauma, can have long-lasting detrimental effects (Adshead, 2000). Trauma exposure has been associated with several psychiatric disorders, including mood disorders, anxiety disorders, PTSD, and substance use issues (E. S. Brown, Fulton, Wilkeson, & Petty, 2000; Bryant et al., 2010; Reed, Anthony, & Breslau, 2007). Trauma has also been associated with declines in physical health, socioeconomic stability, and occupational functioning (Carlson et al., 2011).
Moderating effects
The stress-buffering model is the most influential model used to explain the relation between social support and psychological distress (Lakey & Cohen, 2000). Within this model, social support is protective, moderating (i.e., buffering) the relation between stressful life events and distress (Cohen & Hoberman, 1983). Researchers have supported this model via finding that social support buffered the effects of trauma severity and number of traumas on psychological distress in samples of motor vehicle accident victims (Gabert-Quillen et al., 2012), disaster survivors (Arnberg, Hultman, Michel, & Luntin, 2012), postpartum women (Collins et al., 1993), and women survivors of violence (Glass, Perrin, Campbell, & Soeken, 2007). However, other researchers have found that support did not buffer the relation between trauma and psychological distress (e.g., Beeble, Bybee, Sullivan, & Adams, 2009; Burton, Stice, & Seeley, 2004; Stroebe, Zech, Stroebe, & Abakoumkin, 2005; Wade & Kendler, 2000). Additionally, the high number of studies that did not report testing stress buffering has been interpreted as meaning that stress buffering was tested, but findings were not interesting enough to report (Lakey & Cronin, 2008). Thus, it is important that researchers test stress buffering and report findings whether or not they support the stress-buffering model. Further, most studies of stress buffering following trauma have used general measures of social support—summing scales of several types of social support to get a single index of social support. Following the suggestion of Ozer, Best, Lipsey, and Weiss (2003) that emotional support is more protective than other types of social support following trauma, it is important that researchers investigate emotional support specifically. Further, there is a paucity of research evaluating the moderating (i.e., exacerbating) effects of negative interaction following stressful life events.
Present study
In this study, we used a nationally representative sample to examine the direct and moderating effects of partner emotional support, partner negative interaction, and traumatic life events on psychological distress. Specifically, five hypotheses and two nondirectional research questions were evaluated.
Evaluating direct effects
Our first hypothesis was that people with lifetime trauma would report more psychological distress than those without. This would be consistent with previous research (E. S. Brown et al., 2000) and provide validity evidence for conceptualizing trauma as a stressful life event in the present sample. Our second and third hypotheses were that there would be a negative direct effect of partner emotional support on psychological distress (i.e., greater emotional support will be related to less psychological distress) and a positive direct effect of partner negative interaction on psychological distress (i.e., greater negative interaction will be related to greater psychological distress). These types of direct effects have been well documented in the literature (see Lakey & Orehek, 2011 for a review) and provide the basis for hypothesis four. The fourth hypothesis was that there would be a greater direct effect of partner negative interaction, compared with partner emotional support, on distress. If this hypothesis was supported, our first research question would build on previous studies (see Lincoln, 2000) by empirically evaluating how much more—proportionally—negative interaction is related to psychological distress than is emotional support.
Evaluating moderating effects
Consistent with the stress-buffering model (Cohen, 2004), hypothesis five was that partner emotional support would moderate the effect of trauma on psychological distress. Our second research question assessed whether partner negative interaction moderated the effect of trauma on distress. While stress-buffering proponents have not posited that negative interaction exacerbates reactions to stressful life events, we think it is important to examine the inverse of stress buffering.
Method
Sample
Data were drawn from the Collaborative Psychiatric Epidemiological Surveys (CPES), a U.S. nationally representative data set that resulted from the integration of data from three large-scale epidemiological studies of mental health in adults (18 years and older)—the National Comorbidity Survey Replication, the National Study of American Life, and the National Latino and Asian American Study of Mental Health (Heeringa et al., 2004). The total sample for the CPES was 20,013, and all surveys were completed from 2001 to 2003. Participants who indicated being married or in a romantic relationship and who were asked about all variables used in the present analyses were included. This resulted in a sample of 5,383. The unweighted sample consisted of 2,796 women and 2,587 men; the mean age was 43.92 (SD = 14.54); 1,852 identified themselves as White, 1,759 as Latino, 1,506 as Asian, 199 as Black, and 67 as other; 3,635 were employed and 1,748 were not employed; and 1,567 reported having a college degree or more education, 1,354 some college, 1,346 completed high school, and 1,116 reported having less than a high school degree (see Table 1 for weighted demographic information).
Descriptive statistics.

Note. Raw ns are presented. All other values account for the complex sample. Different subscripts within rows indicate significantly different frequencies (p < .01) between the no trauma and trauma groups.
aHigher scores indicate greater distress.
bHigher scores indicate greater partner supportive interaction.
cHigher scores indicate greater partner negative interaction.
*p < .05; **p < .01; ***p < .001 (all two-tailed tests).
Measures
Psychological distress
Psychological distress was measured with the Kessler Psychological Distress Scale (K6), a six-item measure of psychological distress over the past 30 days (Kessler et al., 2003). Respondents indicate from 0 (none of the time) to 4 (all of the time) their distress level for each item. Higher scores indicate greater levels of psychological distress. Several studies supported the K6’s reliability and validity (Kessler et al., 2002, 2003). The Cronbach’s α in this study was .82.
Partner emotional support
Partners’ (i.e., spouses and romantic partners) emotional support was assessed with a 4-item measure of perceived emotional support from their partner (“How much does your partner really care about you?, How much does your partner understand the way you feel about things?, How much can you rely on your partner for help if you have a serious problem?, How much can you open up to your partner if you need to talk about your worries?”). Response options range from 1 (a lot) to 4 (not at all). Responses were scored, so higher scores indicated greater perceived emotional support. Consistent with previous studies (Whisman, Dementyeva, Baucom, & Bulik, 2012), the mean of the 4-item responses was used for the total score. The Cronbach’s α in this study was .80.
Partner negative interaction
Partners’ negative interaction was measured with a 4-item measure of negative interaction with their partner (“How often does your partner criticize you?, How often does your partner make too many demands of you?, How often does your partner get on your nerves?, and How often does your partner let you down when you’re counting on them?”). Response options range from 1 (a lot) to 4 (not at all). Responses were scored, so higher scores indicated greater negative interaction. The mean of the four responses was used for the total score. The Cronbach’s α in this study was .75.
Lifetime trauma
Lifetime trauma was derived from respondents indicating that they had experienced any of 27 specific traumas (e.g., life-threatening automobile accident, beaten up by their parents, and threatened with a weapon) as well as a free response option. Presence of a lifetime trauma was consistent with endorsing criterion A1 of DSM-IV PTSD, “the person experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to physical integrity of self or others” (p. 467) (American Psychiatric Association, 1994).
Demographics
Standard demographic information was collected from each participant via self-report. In this study, we used age, employment status, race/ethnicity, sex, and education.
Analyses
All analyses were conducted in SPSS version 21 using the complex samples procedure that took into account the stratification, clustering, and appropriate weights to provide accurate standard errors. All significance tests employed z-scores for continuous independent variables and the statistic suggested by the Inter-University Consortium for Political and Social Research (ICPSR; Torres, 2008). Each regression model was built sequentially, so that the additional variance in psychological distress accounted for by each step could be evaluated. Step 1 consisted of the demographic variables and the presence or absence of lifetime trauma; Step 2 consisted of the variables in Step 1 as well as the direct effects of partner emotional support and partner negative interaction; and Step 3 consisted of the variables in Step 2 as well as the interactions (i.e., moderating effects) of trauma × emotional support and trauma × negative interaction.
Results
Descriptive statistics are presented in Table 1. Participants were stratified by presence versus absence of trauma history and compared on key variables. For continuous variables, t-tests were used within the CSGLM command. For categorical variables, adjusted F-tests were used within the CSTABULATE command to examine omnibus effects, followed by CSLOGISTIC to evaluate each level of the categorical variables. Of note, psychological distress was greater among those with trauma compared to those without t(1, 111) = 10.64, p < .001. Bivariate correlations are presented in Table 2.
Bivariate correlations between main continuous variables.
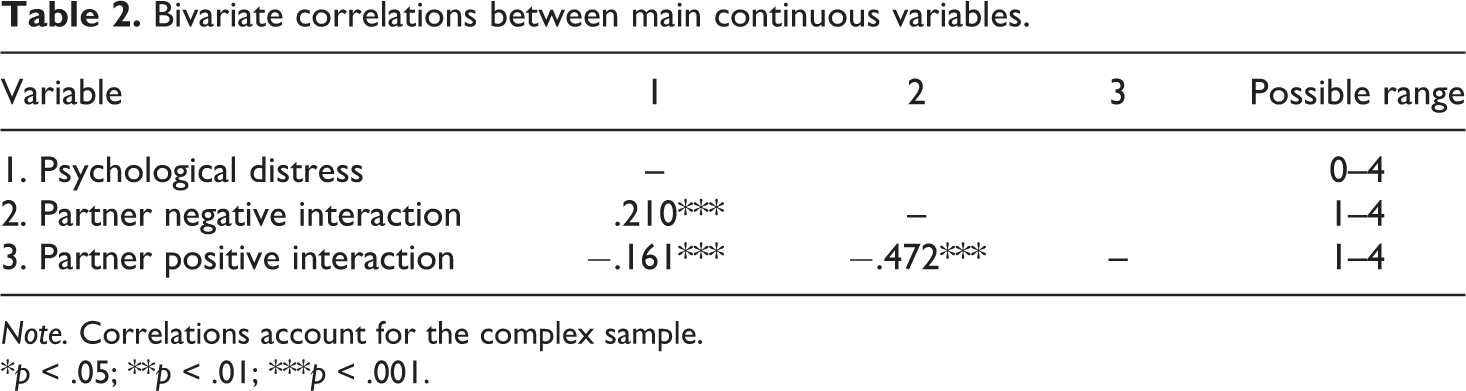
Note. Correlations account for the complex sample.
*p < .05; **p < .01; ***p < .001.
Direct effects
To examine all hypotheses, hierarchical regression analyses were run with psychological distress as the dependent variable (see Table 3). All analyses were run using the CSGLM command. Results in Model 1 supported the hypothesis that those with a traumatic life experience had greater psychological distress than those without a traumatic life experience, Adj. F(1, 111) = 169.69, p < .001. The R 2 of Model 1 was .128, indicating that the demographic variables and the presence of a lifetime trauma accounted for 12.8% of the variance in psychological distress. Model 2 results supported hypotheses two and three – there was a negative direct effect of partner emotional support on distress, Adj. F(1, 111) = 13.59, p < .001, and a positive direct effect of partner negative interaction on distress, Adj. F(1,111) = 90.74, p < .001. Model 2 accounted for 17.3% of the variance in psychological distress, indicating that the addition of emotional support and negative interaction to the variables in Model 1 contributed to explaining an additional 4.5% of the variability in psychological distress. To assess hypothesis four—that the direct effect of partner negative interaction was greater than partner emotional support on distress—we computed a Pratt index (Thomas et al., 2007). The Pratt index is a descriptive index used to partition the R 2 accounted for by the model to each predictor in the model. This is done by multiplying the predictor’s standardized b weight by the bivariate correlation of the predictor and the criterion and then dividing that by the model’s R 2. Predictors’ resulting Pratt indices can then be compared to determine which accounted for more variance (i.e., had a stronger relation with the criterion). In the current model, the Pratt index for partner negative interaction was .189 and for partner emotional support it was .064. Hypothesis four was supported because the Pratt index was greater for partner negative interaction than partner emotional support. Regarding research question one, the Pratt index being approximately three times greater for negative interaction than emotional support indicated that negative interaction accounted for approximately three times greater variance in psychological distress than emotional support.
Results of hierarchical regression analyses predicting psychological distress.
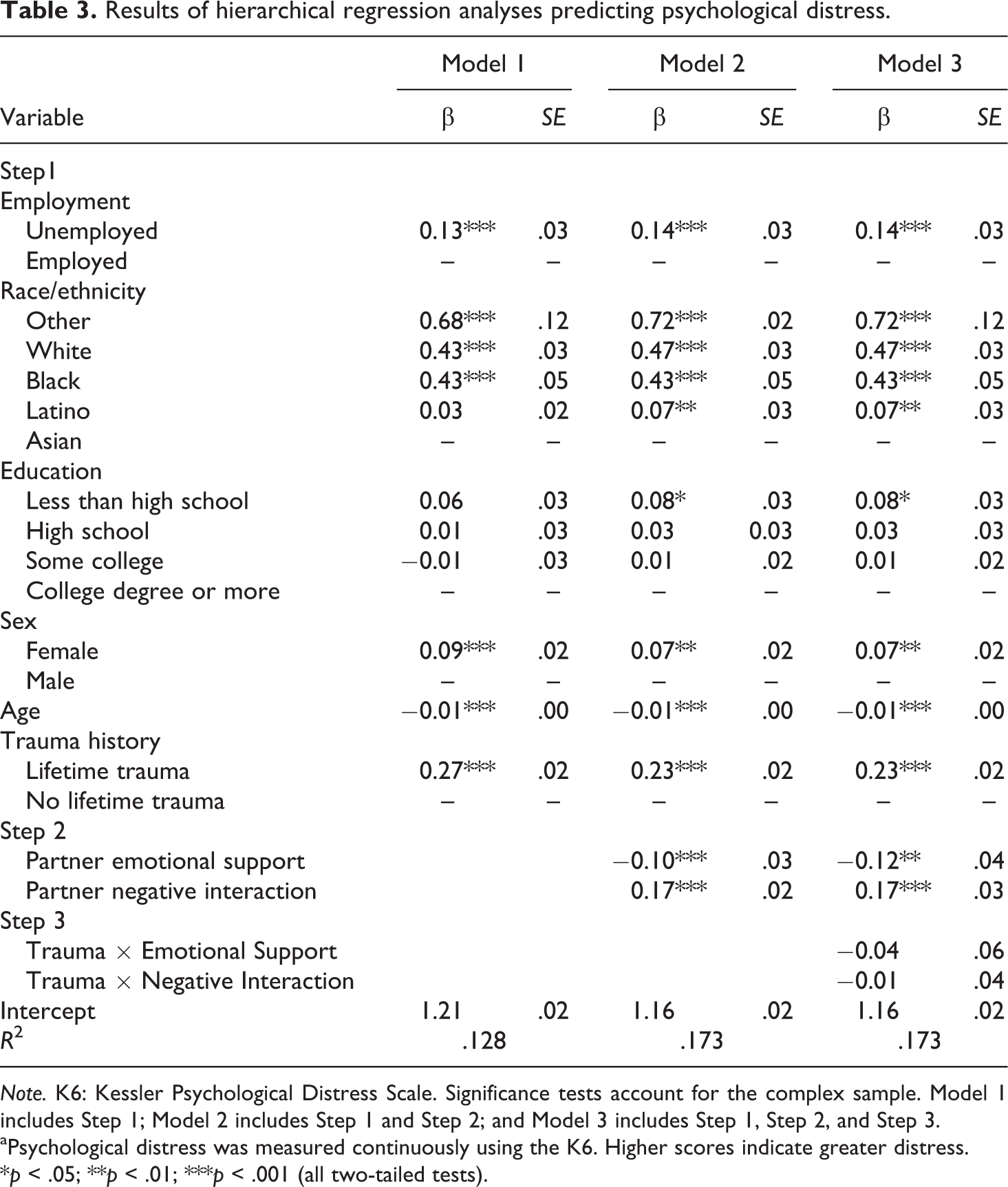
Note. K6: Kessler Psychological Distress Scale. Significance tests account for the complex sample. Model 1 includes Step 1; Model 2 includes Step 1 and Step 2; and Model 3 includes Step 1, Step 2, and Step 3.
aPsychological distress was measured continuously using the K6. Higher scores indicate greater distress.
*p < .05; **p < .01; ***p < .001 (all two-tailed tests).
Moderating effects
In Model 3, the fifth hypothesis and second research question were evaluated. The fifth hypothesis was not supported – partner emotional support did not moderate the effect of trauma on psychological distress, Adj. F(1, 111) = .58, p = .45. Regarding the second research question – partner negative interaction did not moderate the effect of trauma on distress, Adj. F(1,111) = 0.03, p = .86. Model 3 did not account for any additional variance in psychological distress than Model 2.
Discussion
The purpose of this study was to evaluate the relation between trauma, partner emotional support, and partner negative interaction with psychological distress. First, we evaluated the direct effects of partner emotional support and partner negative interaction on psychological distress, followed by proportionally evaluating the strength of negative interaction compared with emotional support. Then, we investigated whether emotional support or negative interaction moderated the relation between traumatic life events and psychological distress.
Direct effects
Our results were consistent with previous findings (Lincoln, 2000), which indicated that negative interaction has a stronger relation with psychological distress than emotional support. In our study, partner negative interaction and partner emotional support both had significant direct effects on psychological distress. Further, partner negative interaction had a stronger relation with psychological distress than partner emotional support. In a follow-up analysis, negative interaction accounted for approximately three times the variance in psychological distress compared with emotional support. Across psychological phenomena, negative interaction having a stronger relation than emotional support is consistent with the finding that bad experiences have a stronger impact on people’s psychological distress than good ones (Baumeister et al., 2001). This general finding has been placed in an evolutionary framework—it is more adaptive for survival (i.e., genetic survival) that bad experiences have a greater impact because that impact will motivate people to leave situations that could hinder their ability to survive. Further, one bad experience can end life, and it is typically the absence of a bad experience that preserves life rather than the presence of a good experience. In the context of romantic relationships, survival applies to self and offspring (or potential offspring). Thus, the psychological distress that results from negative interactions may motivate partners to leave relationships that hinder their ability to survive and thrive.
It is important to note that our findings differ from Finch, Okun, Pool, and Ruehlman’s (1999) meta-analytic findings that indicated that negative interaction and social support did not differ in how much they related to psychological distress. This difference is likely due to the following methodological dissimilarities: (a) their operationalization of psychological distress was heterogeneous, consisting of depression, psychological distress, and inverted well-being indices; (b) they included perceived support and negative interaction from a variety of support providers, where we only included support and negative interaction from romantic partners; and (c) they evaluated the relation of support and negative interaction with psychological distress via bivariate correlations, where we included support, negative interaction, and several other covariates simultaneously in our models. The differences between our findings and Finch and colleagues’ highlight potential moderators (e.g., relationship of support provider) of the relation between negative interaction, social support, and psychological distress that can be used to inform future research.
To increase the understanding of the greater potency of negative interaction compared with emotional support, there are several important directions for future research. First, it is important that researchers continue to use sophisticated analytic techniques to accurately determine the relative strength of negative interaction and emotional support on psychological distress between different support providers (e.g., partners, parents, and friends). From an evolutionary perspective, we would expect the relative strength to be greater from support providers who have a stronger influence on genetic survival. For example, romantic partners would have a greater impact on survival than coworkers. Further, parents’ impact on survival would be greater on children than middle-aged adults; thus, we would expect their negative interactions to be more impactful on those who are more dependent. Also examining the mediating role of psychological distress in the relation between negative interaction and change behaviors (e.g., separation from romantic partners) would further test whether the adaptive function of negative events more strongly influencing psychological distress than positive ones is to motivate change. Building from this, it is important to identify the specific interactions that are perceived as negative compared with positive. Understanding if the potency of the interactions is based on what is communicated, how it is communicated, or when it is communicated would improve our understanding and operationalization of negative interaction and emotional support.
These findings, in concert with previous research, have potential implications for professional practice. First, mental health professionals may serve their clients well by intervening with romantic partners—either individually or in a couples’ or family context—to improve clients’ well-being. Typically, couples-focused treatments are implemented when the presenting problem is interpersonal. Our findings indicate that even when the presenting problem is intrapersonal, there would be value in attending to clients’ relationships. Further, negative interaction having a stronger relation than emotional support with psychological distress indicates that interventions may be most potent if they emphasize reducing negative interactions. While this study focused on romantic relationships, building on previous theoretical work (e.g., Lakey & Orehek, 2011), clinical interventions may serve clients’ best if they focus on whomever clients note as their most important support provider.
Moderating effects
Presently, we did not observe an interaction between lifetime trauma and partner negative interaction or partner emotional support on psychological distress. While stress buffering has been the dominant theory in studies of social support’s relation with distress (Cohen, 2004), buffering effects have been inconsistently observed (see Lakey & Orehek, 2011 for a review). Further, it has been argued that tests of stress buffering that do not find moderating effects often go unreported (Lakey & Cronin, 2008). The lack of stress buffering in this study further supports the argument that buffering does not fully account for the effects of social support on distress. Thus, it is important that continued research investigate both the mediators and moderators that influence the relation between social support and distress. Specifically, there is value in evaluating competing theoretically based social support models, which can be directly compared using contemporary analytic methods (e.g., structural equation modeling). This would facilitate determining which of the models (i.e., theories) best fit the population.
Our study had several limitations that may explain our finding direct but not moderating effects. First, the stressor was a traumatic life event as defined in the DSM-IV. A possibility is that the trauma was too distal to be related to present psychological distress. While this could impact observing stress buffering, meta-analytic evidence suggests that as the time lapse between trauma and assessment increases, social support becomes more protective (Ozer et al., 2003). Another possibility is that trauma type influenced buffering effects, which we could not control for because we did not know the traumas experienced. However, prior studies have found the moderating role of social support across trauma types (Andrews, Brewin, & Rose, 2003; Glass et al., 2007). Finally, our data were cross-sectional and prospective designs are ideal for examining stress buffering (Lakey & Orehek, 2011). While inconsistent observations of stress buffering persist, even in prospective studies, longitudinal designs are preferable for examining stress buffering.
In conclusion, our findings indicate that the direct effects of partner emotional support and partner negative interaction have a stronger relation with psychological distress than their moderating (i.e., buffering) effects post trauma. Further, the greater relation of negative interaction compared with emotional support on psychological distress—when the provider is a romantic partner—is consistent with findings from other studies in which providers were not romantic partners.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.