
Abstract
Longitudinal associations between postseparation relationship stressors (coparenting conflict and harassment) and health outcomes (depressive, posttraumatic stress disorder [PTSD], and physical health symptoms) as moderated by contextual factors (i.e., marital intimate partner violence [IPV], negative life events, and social support) were examined in a sample of divorcing mothers. Respondents were 135 mothers recruited within 4 months of a divorce filing who participated in five interviews at 3-month intervals over a 1-year period. Multilevel modeling procedures used to account for the repeated assessments over time revealed direct associations between postseparation stressors and health outcomes differing based on IPV and negative life events. For example, coparenting conflict after separation was associated with higher levels of depressive, PTSD, and physical health symptoms among mothers who experienced no violence, whereas the opposite pattern was observed among mothers whose marriages were characterized by coercive controlling violence. Negative life events magnified that negative impact of coparenting conflict on mental and physical health. Contrary to expectation, social support did not diminish the negative health effects of postseparation stressors. Findings support the value of examining how distinct postseparation factors are associated with divorcing mothers’ health within the broader context against which the divorce process plays out.
Keywords
Divorce is often associated with health problems among divorcing women (e.g., Symoens, Colman, & Bracke, 2014). This connection is typically attributed to multiple stressors that are linked (directly or indirectly) to the separation process. Experiencing multiple or chronic stressors is associated with increased mental health problems and psychological distress, especially depression (Lorenz et al., 1997; Thoits, 2010) and physical health symptoms (Cohen et al., 1998). Negative interactions after separation, such as coparenting conflict or harassment by former partners, represent one potential source of stress that may affect divorcing women, particularly when children are involved (Hardesty et al., 2017). However, postseparation dynamics play out within a larger context that may exacerbate or ameliorate links between stressors and health outcomes. Contextual factors that may exacerbate the negative effects of postseparation conflict and harassment include features of the prior marital relationship (Symoens et al., 2014). Intimate partner violence (IPV) is a marital characteristic that has been linked to both postseparation stress factors and health outcomes among mothers (Woods, Hall, Campbell, & Angott, 2008; Wuest, Ford-Gilboe, Merritt-Gray, & Berman, 2003). Different types of marital IPV (i.e., coercive controlling violence [CCV] vs. situational couple violence [SCV]) appear to relate to diverse postseparation experiences and presumably different health outcomes (Hardesty et al., 2012, 2017), but these associations remain unexplored. Experiencing negative life events because of separation (e.g., changes in residence or finances; Logan & Walker, 2004) might also exacerbate negative outcomes, whereas social support may ameliorate the negative effects of stress resulting from the divorce process (DeGarmo, Patras, & Eap, 2008). To date, the effects of coparenting conflict and harassment have been examined in distinct bodies of work with general samples of divorcing parents (for conflict) versus samples of women who experienced IPV (for harassment). To disentangle these pathways of influence, the current longitudinal study examines how postseparation relationship stressors (i.e., coparenting conflict, harassment) influence mothers’ mental and physical health, and how these associations vary as a function of contextual factors (i.e., marital IPV, negative life events, and social support).
Postseparation stressors and mothers’ mental and physical health
Divorce is associated with negative mental and physical health outcomes for women (Amato, 2000; Braver, Shapiro, & Goodman, 2006), especially in the first year after separation (Lorenz et al., 1997). According to the divorce–stress–adjustment perspective, associations between divorce and adjustment vary by stress resulting from the separation process (Amato, 2000). In the initial period following separation, divorcing parents, for example, must disentangle their relationships as former partners while continuing their relationships as coparents. Thus, factors contributing to stress during the divorce process include postseparation coparenting conflict and harassment from former partners. Coparenting conflict refers to disagreements that focus on parenting children together, such as caregiving arrangements, parenting practices, and decision-making. Coparenting conflict is common early in the divorce process (Braver et al., 2006) and tends to decrease over time (Ahrons, 1981; Cookston, Braver, Griffin, De Luse, & Miles, 2007; Maccoby & Mnkookin, 1992). For women, postseparation conflict with former partners has been linked to depression (Whiteside & Becker, 2000). It is unknown whether coparenting conflict has similar associations with broader health outcomes (Hardesty et al., 2012).
In contrast to coparenting conflict, which relates to joint roles as parents, harassment refers to intrusive actions aimed at the former partner. Behaviors tend to be repetitive nuisance or threatening actions, such as showing up without warning, bothering at work, or leaving threatening messages. Harassment is associated with separation and divorce (Davis, Coker, & Sanderson, 2002) and is especially likely to occur in the early separation period when former partners have continued contact due to shared children (Hardesty, Khaw, Chung, & Martin, 2008; Sheridan, Blaauw, & Davies, 2003). Similar to coparenting conflict, postseparation harassment tends to decrease over time (Hardesty et al., 2017). Postseparation harassment is associated with women’s reports of depression (Broughton & Ford-Gilboe, 2016; Davis et al., 2002; Mechanic, Weaver, & Resick, 2008), symptoms of posttraumatic stress disorder (PTSD; Kamphuis & Emmelkamp, 2001; Mechanic et al., 2008), and physical health symptoms (Pathe & Mullen, 1997), although these findings are cross-sectional. Coparenting conflict and harassment have typically been studied in different samples, including divorcing parents in general and abused women. In this article, we examine how postseparation coparenting conflict and harassment distinctly influence depressive, posttraumatic stress, and physical health symptoms over time in a sample of mothers early in the divorce process with and without a history of IPV. Finally, past studies have tended to focus on average levels of adjustment comparing divorced and married samples (Amato, 2010); we use prospective methods to explore variability among divorcing women due to moderating contextual factors.
Contextualizing postseparation stress
Relationship dynamics following separation play out within a larger context. Yet, to date, differences in adjustment within samples of divorcing individuals have not been extensively studied (Symoens et al., 2014). The current study considers the role of three contextual factors: IPV, negative life events, and social support.
Intimate partner violence
IPV in marriage is associated with increased likelihood of divorce (Amato & Rogers, 1997), but the prior marital relationship is an often-overlooked contextual factor in the divorce process (Symoens et al., 2014). The direct effects of IPV on the mental and physical health of women are well-documented. The most common mental health effects include depressive and PTSD symptoms, with rates much higher than the general population (Mechanic et al., 2008; Zlotnick, Johnson, & Kohn, 2006). Abused women also report poorer physical health than nonabused women do (Dillon, Hussain, Loxton, & Rahman, 2013). Less understood is how IPV, especially different types of IPV, influences the postseparation context (Hardesty et al., 2012; Logan & Walker, 2004). There is evidence from a handful of longitudinal studies that temporal pathways between IPV and depressive, PTSD, and physical health symptomology are both direct and indirect (via stress factors; Dillon et al., 2013). IPV in the marital relationship may set the stage for more negative relationship dynamics after separation. For example, postseparation conflict and harassment are higher after separation for those with marital IPV (Hardesty et al., 2017).
There is also some evidence that coparenting conflict and harassment differ across different types of IPV. CCV refers to physical violence that occurs within a larger, pervasive context of coercive control. SCV is not tied to coercive control but instead is violence that occurs when arguments escalate or partners lash out in anger (Johnson, 2008). Both coparenting conflict and harassment are more likely for women who experienced CCV than SCV or no violence (NV) in marriage (Hardesty, Crossman, Khaw, & Raffaelli, 2016; Ornstein & Rickne, 2013). Finally, the course of conflict and harassment differs over time depending on the type of IPV; for example, divorcing mothers who experienced CCV show the most volatility in conflict and harassment across the first year (Hardesty et al., 2017). Understanding how IPV, including different types, affects associations between postseparation stress and health would inform interventions to support postseparation adjustment.
Negative life events
There is abundant evidence that divorce is typically accompanied by a range of stressful life events. Compared to married women, divorcing women report significantly more negative life events (e.g., job change, residential move) in the 1–2 years after separation (Lorenz et al., 1997). Studies have documented the direct effects of negative life events on depression for divorcing women (e.g., Lorenz et al., 1997), but negative life events may also operate in combination with postseparation conflict and harassment. Negative life events experienced after separation may amplify the negative effects of coparenting conflict and harassment because they place additional demands on women’s physical and emotional attention, resources, and coping mechanisms. Thus, women who experience high levels of negative life events in combination with conflict and harassment are likely to experience more negative health effects. To our knowledge, the role of negative life events in postseparation adjustment has not been examined as it relates to conflict and harassment.
Social support
Social support is a contextual factor that has been found to moderate the effects of postseparation stress on adjustment (DeGarmo et al., 2008). This is consistent with the stress-buffering hypothesis (Cohen & Wills, 1985), which posits that close and supportive relationships can help individuals cope with potentially distressing events (Sarason, Sarason, & Gurung, 1997). Using cross-sectional data, Broughton and Ford-Gilboe (2016) reported that perceived social support and postseparation harassment were negatively associated but did not find that social support moderated the negative impact of harassment on family health. They posited that social support may offer comfort and assistance but may not directly alter the intrusiveness of harassment and thus its impact on functioning. Whether social support served as a protective factor for women’s individual health was not examined. Given high levels of stress experienced by divorcing mothers early in the separation process, it is useful to understand how social support may buffer effects of those stressors on their health (Broughton & Ford-Gilboe, 2016).
Purpose
Taken as a whole, the extant literature indicates that postseparation relationship stressors are linked to mothers’ mental and physical health. However, several limitations remain. First, with the exception of Hardesty et al. (2016, 2017), coparenting conflict and harassment are typically studied in different types of samples (general divorcing samples vs. abused women, respectively), making it impossible to disentangle their pathways of influence. Second, measures of coparenting conflict and harassment have not been conceptually distinct and/or have conflated conflict and/or harassment with violence (e.g., Broughton & Ford-Gilboe, 2016; Kamphuis & Emmelkamp, 2001). Relationship status and time since separation also vary across studies on both conflict and harassment. Furthermore, most studies have been cross-sectional with data collected years after separation, increasing the potential for recall bias (Symoens et al., 2014). Finally, despite evidence that different IPV types are associated with different postseparation dynamics, the unique effects of these differences on health outcomes are unexplored. Understanding the unique trajectories of coparenting relationships after separation from a violent partner as well as the potential role of different IPV types is important for developing individualized interventions and policies.
The current study addresses limitations of past work using a longitudinal sample of recently separated women who reported different IPV types, including NV. We also used distinct measures of postseparation coparenting conflict and harassment to understand their unique effects on women’s health. We address the following hypotheses:
Method
Procedure
All women named in a divorce filing within the past 12 weeks were identified using public court records in a large county in the Midwestern U.S. The target sample size was 120 (based on a priori power analysis), and recruitment efforts continued until this number was exceeded. Recruitment letters were sent via U.S. mail or the attorney of record; if phone numbers were available, follow-up calls were made. Potential participants who responded to recruitment efforts were screened for eligibility. Inclusion criteria were that divorcing women (a) had at least one child under age 18 with their former partner (to ensure the relevance of parenting a minor child); (b) had custody of their child(ren) at least 25% of the time (to ensure the relevance of coparenting); (c) had been physically separated for less than 3 years (to limit recall bias); and (d) could understand and speak English (due to budget constraints preventing the use of translators). Letters were sent to all 577 women named in a divorce filing between August 2010 and November 2012. Nearly one quarter (23.4%, N = 135) agreed to participate and completed a baseline interview. Of the 442 nonparticipants, 39 were eligible and interested but did not show for interviews or respond to follow-up efforts; 20 declined to participate; 15 did not meet the criteria; and 368 never responded. It was not possible for us to determine whether the latter group received the recruitment letter or met the inclusion criteria.
Five in-person interviews consisting of structured and open-ended measures and lasting 60–90 min were conducted at 3-month intervals. Interviews were administered orally by graduate students trained to be attentive to the emotional and psychological responses of participants. IRB approval and a Federal Certificate of Confidentiality were obtained. Numerous precautions were taken to ensure women’s safety and privacy (e.g., recruitment letters did not mention IPV, framing the study as an investigation of mothers’ experiences with divorce). Participants’ rights and potential risks were discussed in the informed consent process, including limits of confidentiality (e.g., mandatory child abuse reporting laws). Most interviews took place in public locations (e.g., private room in library) but some were conducted at women’s homes. Mothers received US$35 for completing the first interview, US$40 at Times 2 and 3, and US$45 at Times 4 and 5. Those who completed all five interviews were entered into a drawing for an additional US$100. This incentive structure resulted in high retention rates. Baseline (T1) interviews were conducted with 135 mothers; retention rates ranged from 84% to 90% at T2–T5 (119, 119, 114, and 121 mothers completed follow-up interviews after 3, 6, 9, and 12 months, respectively).
Sample
At T1, mothers were 20.83–53.92 years old (M = 35.22, SD = 7.02). The sample was predominantly White (n = 103, 76.3%); 18 mothers (13.3%) identified as Black/African American, 6 (4.4%) as Asian/Asian American, 5 (3.7%) as biracial, and 3 (2.2%) as Latino/Hispanic. Mothers had between one and four (M = 1.79, SD = 0.80) biological or adopted children with their former partner. On average, mothers had been married to their former partner nearly 10 years (SD = 6.01; range = 0.42–27.92 years) and had been physically separated for 8 months (SD = 6.37; range < 1–27 months). At T1, 20% (n = 27) reported that their divorce was finalized and 45% had formal custody agreements (23.6% joint physical, 73.6% mother sole physical). Most mothers (84.5%) had formal custody agreements 1 year later (23.4% joint physical, 73.8% mother sole physical). When mothers had sole physical custody, 85.7% and 80.0% of fathers had formal visitation agreements at baseline and 1 year later, respectively. The majority (59.3%) of mothers were employed full time; the rest were employed part time (20.7%), unemployed by choice (10.4%) or not by choice (4.4%), or in another employment status (5.2%). About half were college graduates (31.9% bachelor’s degree and 17.8% some graduate education); the remainder reported some college (38.5%) or a high school education or less (11.1%). At the time the data were collected, our sample was demographically similar to the county population (U.S. Census Bureau, 2011).
Measures
Postseparation stressors
Two postseparation stressors were assessed at each time point using existing measures with established psychometric properties. At T1, mothers reported on experiences since separation; at later time points, they reported on the period since the previous interview (approximately 3 months). Mothers rated frequency of coparenting conflict on 4 items from the Quality of Coparental Communication scale (Ahrons, 1981; e.g., “How often is the conversation stressful or tense?”) using a scale from 1 (never) to 5 (always). Responses were averaged, with higher scores indicating higher levels of conflict (T1–T5 α = .80–.86). The Harassment in Abusive Relationships: A Self-Report Scale (Sheridan, 2001) was used to measure harassment. Mothers indicated how often their former partner engaged in each of 23 behaviors (e.g., “sits in his car outside my home”) on a scale of 1 (never) to 5 (very frequently). Responses were summed for a maximum possible score of 92; higher scores indicated more frequent harassment (α = .71–.81).
Health outcomes
Three indicators of psychological and physical health were evaluated at all 5 time points using established measures designed for use in general populations. Overall scores were computed by summing, with a higher score indicating greater symptom severity. Physical health symptoms were assessed using the 13-item “somatic module” from the Patient Health Questionnaire-15 (PHQ-15; Kroenke, Spitzer, & Williams, 2002). The 2-item “depression module” was excluded due to overlap with the measure of depressive symptoms. Respondents indicated whether they had been bothered by 13 somatic symptoms (e.g., headaches) in the past month on a scale from 1 (not bothered at all) to 2 (bothered a lot). In our sample, Cronbach’s αs for the PHQ-13 ranged from .61 to .74 at each time point, somewhat lower than the internal reliability reported for the PHQ-15 by Kroenke and colleagues in a large sample recruited from medical settings (.80). Depressive symptoms were measured with the 12-item version (Anderson, Malmgren, Carter, & Patrick, 1994) of the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977). Participants indicated the number of days in the last 7 that they experienced each symptom (e.g., restless sleep). Alphas in the current study were .82–.90, slightly lower than reported by Zlotnick, Johnson, and Kohn (2006) in a national sample of women with and without IPV (α = .93). PTSD symptoms were assessed using the 6-item version (Lang & Stein, 2005) of the PTSD checklist (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996), which corresponds directly to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria for PTSD. Respondents indicated how much they have been bothered by each problem (e.g., intrusive memories) in the last month on a scale from 1 (not at all) to 5 (extremely). The 6-item version correlates highly with the original 17-item measure (r = .97) and has high specificity and sensitivity (Lang & Stein, 2005); alphas in our sample were .80–.85.
Moderators
Three potential moderators were assessed: IPV, negative life events, and social support. Mothers were classified into three mutually exclusive marital IPV groups based on their reports of physical violence using the revised conflict tactics scales (CTS2; Straus, Hamby, Boney-McCoy, & Sugarman, 1996) and coercive control using the Dominance-Isolation subscale of the Psychological Maltreatment of Women Inventory (PMWI; Tolman, 1992) during marriage (assessed at T1). Using Hardesty and colleagues’ (2015) approach, mothers were classified as experiencing NV, SCV (violence and little to no coercive control), and CCV (violence and high coercive control). At T5, mothers reported on negative life events during the past year (corresponding to the time of separation) using items from the Life Events Questionnaire (Norbeck, 1984). For the current study, 29 items were selected based on their relevance to the divorce process (e.g., changes in work, residence, or relationships); we excluded events that were overly specific (e.g., major dental work), that all participants experienced (e.g., separation from spouse), or that overlapped with other measures (e.g., spousal conflict). Mothers indicated whether each event occurred and, if so, whether it had a “good,” “bad,” or “neutral” effect on them. An aggregated negative life events score was computed by summing the “bad” events. At each time point, mothers completed the 12-item Social Support Network (SSN) scale (Block, 2000), which considers three aspects of informal social support (acceptance and support, emergency help, and access to resources). Women rated each item (e.g., “Someone I care about stands by me through good times and bad times”) on a scale from 1 (disagree strongly) to 6 (strongly agree). The SSN has demonstrated validity and reliability (Block, 2000). An overall score was computed by averaging, with higher scores indicating a higher level of perceived social support (α = .82).
Covariates (T1)
Covariates were identified based on past research (Hardesty et al., 2012). Mothers reported their age (in years), length of marriage (in years), time since separation (in months), and whether their divorce was finalized (0 = not finalized; 1 = finalized). Mothers also reported whether they had a custody agreement (0 = no custody agreement; 1 = custody agreement) and their level of education (1 = less than high school; 9 = doctoral degree). Each of the continuous covariates was mean centered prior to analysis.
Plan of analysis
Preliminary analyses
Most participants completed five (n = 100; 74.1%) or four (n = 22; 16.3%) interviews. Most attrition occurred between T1 and T2. Comparisons of participants who dropped out after T1 (n = 7) versus remained in the study (n = 128) on the study variables revealed no demographic differences or differences by IPV type, social support, or any of the health outcomes. Mothers who dropped out reported lower levels of coparenting conflict, M = 1.71, SD = 0.49 vs. M = 2.65, SD = 1.08, t(132) = 4.51, p < .001; and less harassment (M = 22.43, SD = 0.98 vs. M = 26.18, SD = 6.27) than mothers who remained in the study, t(133) = 5.64, p < .001. About 11% of the data were missing. Little’s Missing Completely at Random (MCAR) test showed that data were not missing completely at random, χ2(10) = 25.76, p = .004. However, only one significant difference between participants with and without missing data was found. Specifically, those with missing data at T5 had lower levels of education than those without missing data. For all analyses, missing data were handled using the restricted maximum likelihood algorithm, which provides unbiased estimates of complete data, given the incomplete data (Bryk & Raudenbush, 1992).
Analysis
To account for the correlated error inherent in longitudinal data, we conducted growth curve analyses with the hierarchical linear modeling software (HLM 7; Raudenbush, Bryk, Cheong, Congdon, & Du Toit, 2011). Multilevel modeling procedures were used to account for the repeated assessments over time. In the first step, we ran a series of unconditional models to calculate the intraclass correlations for each of the outcome variables. To test the primary hypotheses, we entered linear time (0 = Time 1), coparenting conflict, harassment, social support, and interactions for each of the coparenting variables with time and with social support into the within person (Level 1) equation. Negative life events and IPV group (with NV as the reference group) were entered into each of the between persons (Level 2) equations. Each model controlled for mother’s age and education, months since separation, presence of a custody agreement, marital length, and whether the divorce was finalized. We tested this model for each of the study outcomes (i.e., depressive, PTSD, and physical health symptoms). Significant interactions were probed using standard procedures (Aiken & West, 1991); due to space limitations, only one figure per interaction is presented when the patterns were similar across models.
Results
Table 1 presents means and standard deviations for study variables. Intraclass correlations showed that about half of the variance in depressive (49%) and PTSD symptoms (49%) and the majority of the variance in physical health symptoms (64%) was at the between-persons level. Because results differ by outcome, we organized the following sections by outcome (see Table 2). Due to space limitations, we discuss only the findings that reached statistical significance. All nonsignificant findings are reported in Table 2.
Means and standard deviations for all study variables at each time.

Note. M = mean; SD = standard deviation; PTSD = posttraumatic stress disorder.
Postseparation stressors, intimate partner violence, negative life events, and demographic controls predicting depressive, PTSD, and physical health symptoms over time.
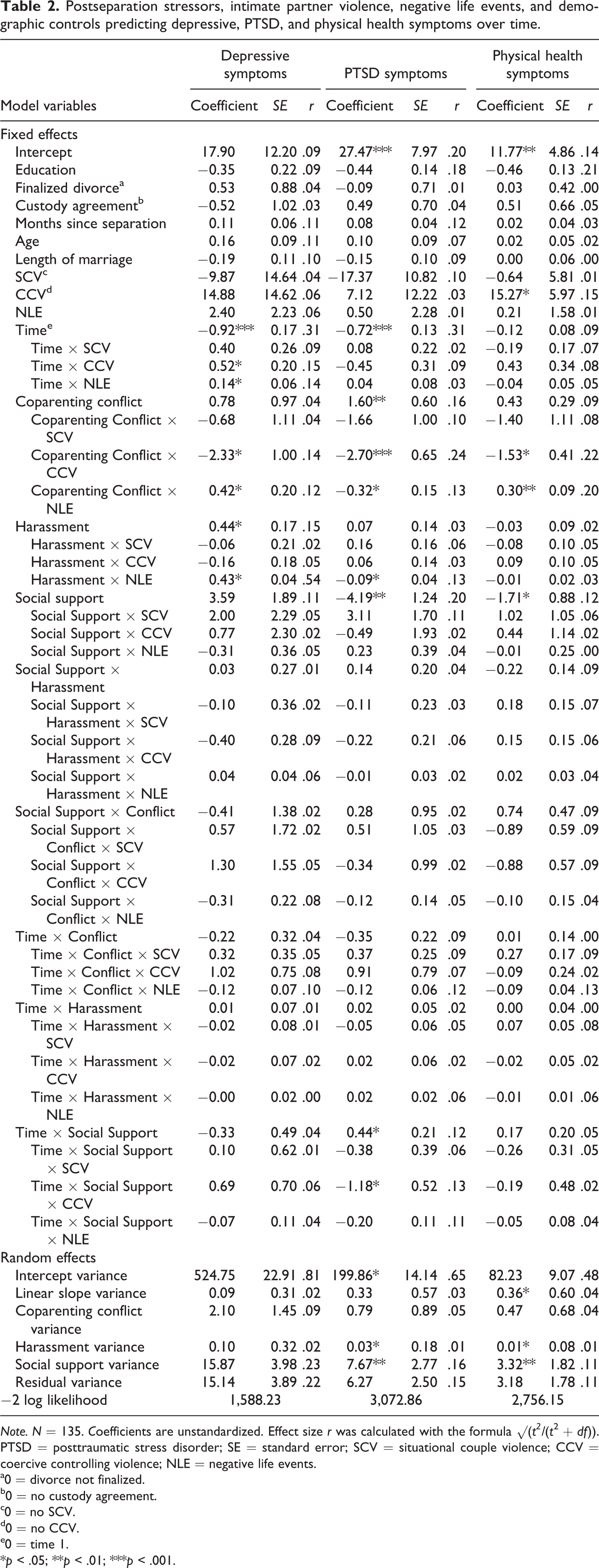
Note. N = 135. Coefficients are unstandardized. Effect size r was calculated with the formula √(t2/(t 2 + df)). PTSD = posttraumatic stress disorder; SE = standard error; SCV = situational couple violence; CCV = coercive controlling violence; NLE = negative life events.
a0 = divorce not finalized.
b0 = no custody agreement.
c0 = no SCV.
d0 = no CCV.
e0 = time 1.
*p < .05; **p < .01; ***p < .001.
Depressive symptoms
The model examining depressive symptoms indicated that levels of depressive symptoms decreased over the course of the study (B = −.92, p < .001). The linear decline of depressive symptoms was qualified by two significant interactions, one with IPV type (B = .52, p < .05) and one with negative life events (B = .14, p < .05). Figure 1(a) and (b) shows the decomposition of these interactions. Regarding IPV type, women who experienced NV (b = −.98, p < .001) had a steeper decrease in depressive symptoms over the course of the study than those who experienced CCV (b = −.33, p < .001). There were no significant differences between women who experienced SCV and NV. Women who experienced lower levels of negative life events (b = −1.20, p < .001) experienced a steeper decline in depressive symptoms than those who experienced higher levels of negative life events (b = −.80, p < .001).
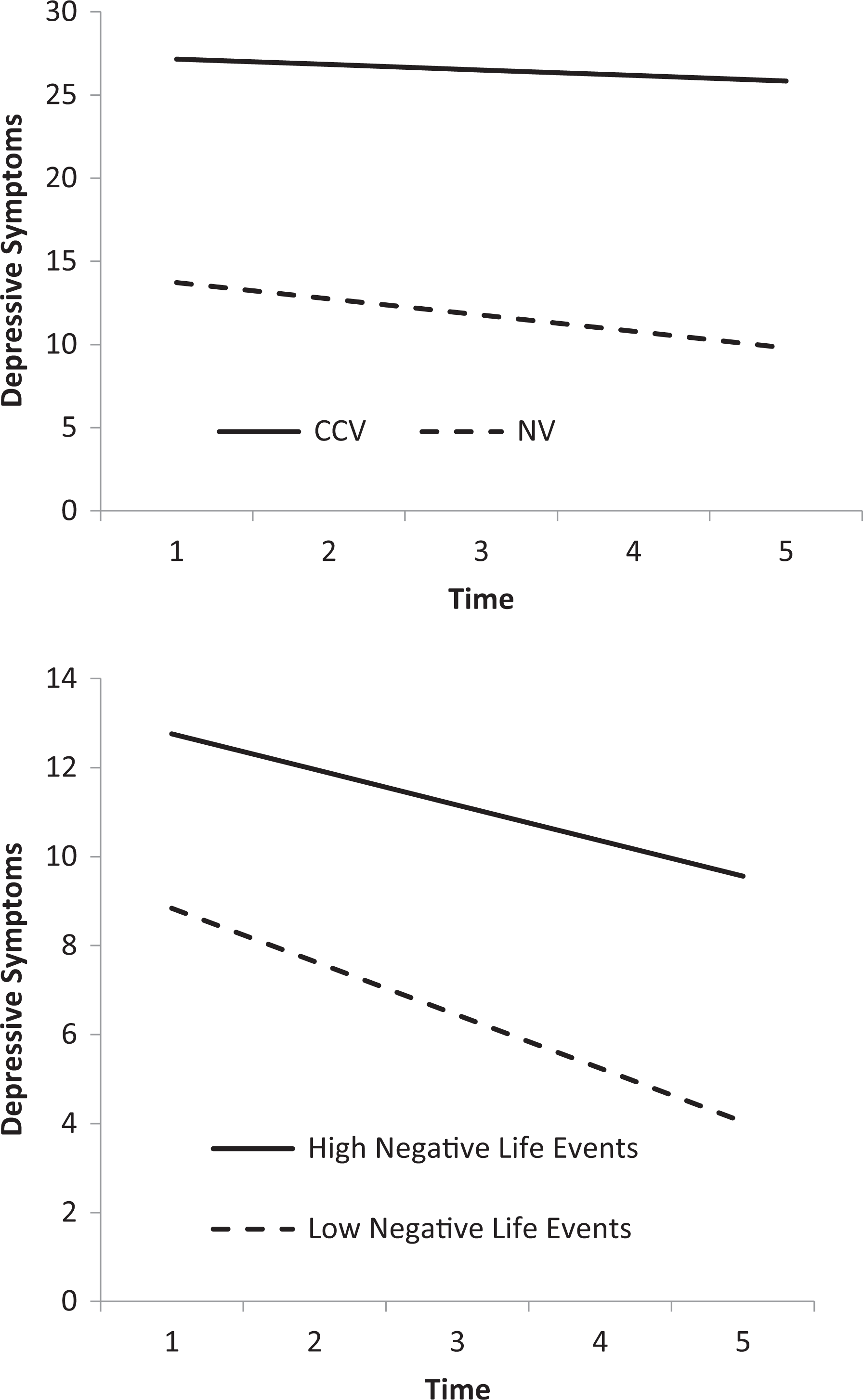
The interaction between time and IPV type (a) and time and negative life events (b) on depressive symptoms. IPV = intimate partner violence.
There was also a main effect of harassment on depressive symptoms (B = .44, p < .05), but this effect was moderated by negative life events (B = .43, p < .05). The association was stronger for those who reported higher (b = .66, p < .001) versus lower (b = .23, p < .001) levels of negative life events (see Figure 2). The association between coparenting conflict and depressive symptoms was moderated by IPV type (B = −2.33, p < .05) and negative life events (B = .43, p < .05) in that the association was positive for those who experienced NV (b = .88, p < .001) and negative for those who experienced CCV, b = −1.45, p < .001; see Figure 3(a) for an illustration. There were no significant differences between women who experience SCV and NV. The association was also stronger for women who reported higher (b = 1.15, p < .001) versus lower (b = .72, p < .001) levels of negative life events, see Figure 3(b) for an illustration.

The interaction between harassment and negative life events on depressive symptoms.
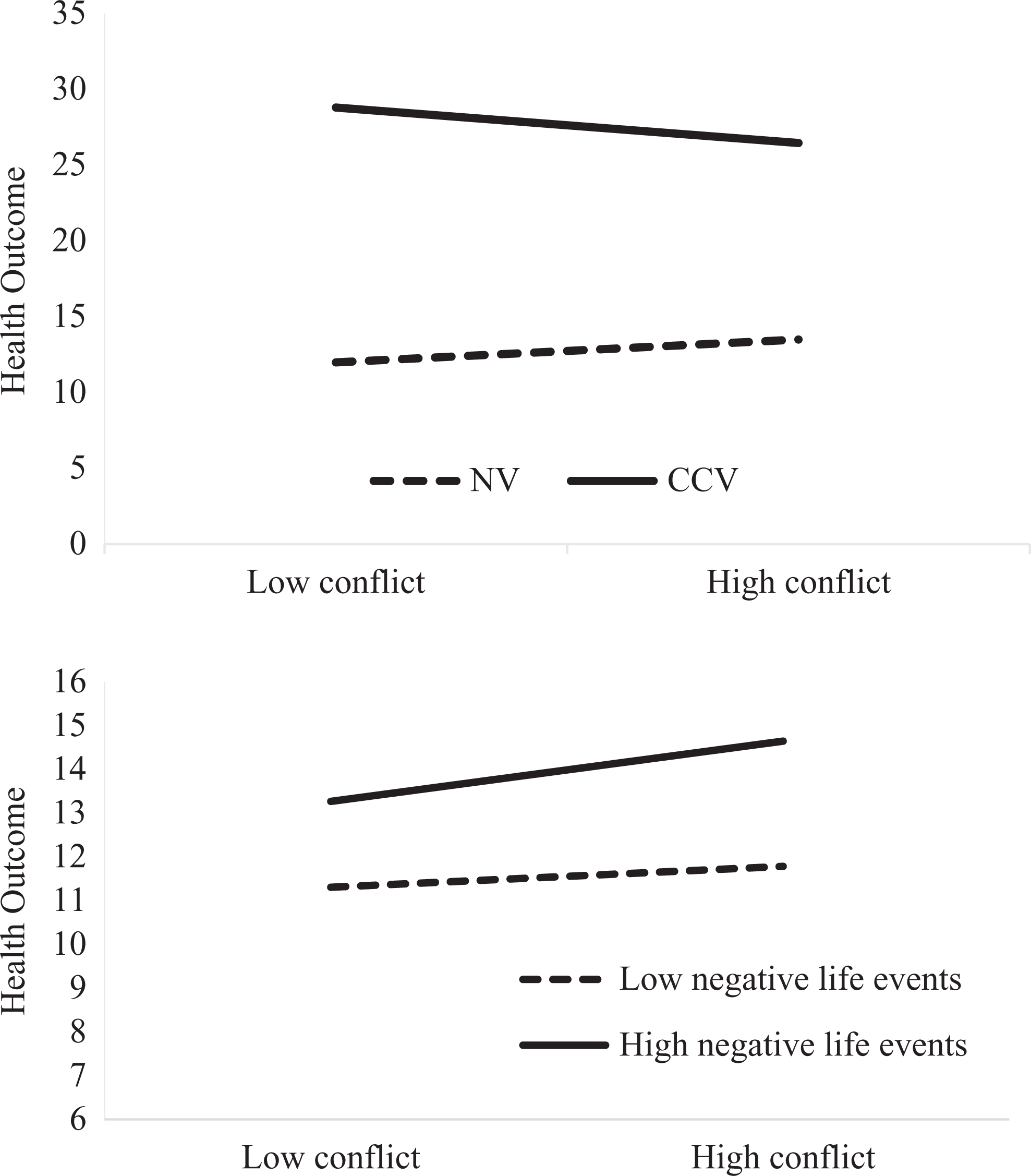
Illustration of interaction between coparenting conflict and IPV type (a) and negative life events (b) on health outcomes (i.e., depression, PTSD, and physical health symptoms). IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
PTSD symptoms
The second model showed that PTSD symptoms decreased over the course of the study (B = −.72, p < .001). There were main effects for both conflict (B = 1.60, p < .05) and social support (B = −4.19, p < .01). The association between conflict and PTSD symptoms was moderated by IPV type (B = −2.70, p < .001) such that the association was positive for women who experienced NV (b = 1.60, p < .001) and negative for women who reported CCV, b = −1.09, p < .001; see Figure 3(a) for an illustration of this interaction. There were no significant differences between women who experienced SCV and NV. Moreover, the association was moderated by negative life events (B = −.32, p < .05) such that the association was stronger for those who experienced higher (b = 1.76, p < .001) versus lower (b = 1.43, p < .001) levels of negative life events, see Figure 3(b) for an illustration of this interaction.
The association between harassment and PTSD symptoms was also moderated by negative life events (B = −.09, p < .05; see Figure 4): it was significant and positive for those who reported higher (b = .14, p < .001) levels of negative life events but not significant for those who reported lower levels of negative life events (b = −.01, p = .80). The association between social support and PTSD symptoms was qualified by a three-way interaction with time and IPV type (B = −1.18, p < .05; see Figure 5). Among women who experienced CCV, PTSD symptoms decreased over time for both those with higher (b = −1.35, p < .001) and lower (b = −.97, p < .001) levels of social support. Among women who experienced NV, PTSD decreased at both higher (b = −.64, p < .001) and lower (b = −.84, p < .001) levels of social support.

The interaction between harassment and negative life events on PTSD symptoms. PTSD = posttraumatic stress disorder.

Three-way interaction between social support, time, and IPV group on PTSD symptoms. IPV = intimate partner violence; PTSD = posttraumatic stress disorder.
Physical health symptoms
In the model predicting physical health symptoms, there was a significant main effect of IPV group (B = 15.27, p < .001) such that women who experienced CCV reported more physical health symptoms than those who experienced NV. There was also a main effect of social support (B = −1.71, p < .05). Similar to the previous models, there was a significant cross-level interaction between coparenting conflict and IPV group (B = −1.53, p < .05) such that the association was positive for those who experienced NV (b = .43, p < .001) and negative for those who experienced CCV, b = −1.10, p < .001; see Figure 3(a) for an illustration. There were no significant differences between women who experienced SCV and NV. There was also a significant interaction between coparenting conflict and negative life events (B = .30, p < .01) in that this association was stronger for those who reported higher (b = .59, p < .001) versus lower levels of negative life events, b = .23, p < .001; see Figure 3(b).
Discussion
The overarching goal of this longitudinal study was to examine associations between postseparation stressors and health outcomes, including the possible moderating role of contextual factors. Overall, mothers’ depressive and PTSD symptoms were greatest soon after separation and decreased over the year. Others have also found a rapid onset of depression soon after a serious life event (Kendler et al., 1995). Consistent with the divorce–stress–adjustment model (Amato, 2000), this pattern likely reflects the heightened disruption in the immediate aftermath of separation, and the time parents need to regain some stability and structure. In the current sample, decreases in depression were most dramatic when mothers did not have a history of IPV and had fewer negative life events after separation. These mothers may have had less cumulative stress burden (Thoits, 2010), allowing them the emotional resources needed to recover at a faster pace (Kessler, 1997). Physical health symptoms, on the other hand, did not change significantly over time. This finding supports Lorenz, Wickrama, Conger, and Elder’s (2006) claim that psychological distress may be more reactive to acute stressors whereas physical health symptoms result from an accumulation of chronic stress over longer periods. The 1-year period of our study may not have been enough time to identify physical health effects.
Coparenting conflict is a postseparation stressor that has been linked to mothers’ depression in past studies (see Whiteside & Becker, 2000). Our findings reveal the broader impact of coparenting conflict on PTSD and physical health symptoms. As hypothesized, mothers with more coparenting conflict after separation had more depressive, PTSD, and physical health symptoms when coupled with higher levels of negative life events. In other words, in the context of high levels of negative life events, the effects of conflict on mothers’ health were magnified. The chronic nature and pileup of stress may make these mothers particularly vulnerable to health problems after separation.
For mothers who experienced CCV in marriage, however, coparenting conflict after separation was associated with less depression and PTSD and fewer physical health symptoms. This was contrary to what we hypothesized and the opposite of what mothers with no IPV experienced. In the context of CCV, reports of coparenting conflict after separation could reflect mothers’ efforts to reclaim control. Abused mothers have a strong need to protect their children after separation and may draw on their anger or fear as personal resources to shift the balance of power with their former partners (Kirkwood, 1993). Higher coparenting conflict, at least in the short term, could emanate in part from mothers’ growing sense of personal empowerment (e.g., assertiveness, expressions of anger). In cross-sectional studies, personal empowerment has been linked to decreased PTSD symptoms among abused women (e.g., Perez, Johnson, & Wright, 2012; Wright, Perez, & Johnson, 2010). For mothers leaving marriages with CCV, feelings of greater control over their situations could have psychological and physical health-enhancing effects (Wallerstein, 1992). In the long term, however, persistent coparenting conflict, especially if an expression of mothers’ assertiveness, could put some mothers at risk. Perez, Johnson, and Wright (2012) found that empowerment was protective for abused women, except in situations of severe violence where abusers may become more violent. Future studies should measure personal empowerment and investigate its possible role in coparenting conflict and health outcomes over time.
Although coparenting conflict after separation has been studied extensively, this is the first study, to our knowledge, to examine harassment distinct from conflict and its longitudinal impact on divorcing mothers’ health. As expected, postseparation harassment negatively affected both depressive and PTSD symptoms. Similar to coparenting conflict, the effects of harassment were magnified in the context of more negative life events, lending further support to the divorce–stress–adjustment model (Amato, 2000). In contrast to conflict, harassment negatively affected mothers’ mental health regardless of prior IPV experiences. For mothers who experienced CCV, the intrusive nature of postseparation harassment may resemble the controlling tactics they experienced during marriage in ways that coparenting conflict does not and interfere with their recovery from abuse (Wuest et al., 2003). Studies are needed to understand how the dynamics of harassment vary by IPV type, as Nielsen, Hardesty, and Raffaelli (2016) found that harassment in the context of CCV included a wider variety of tactics and more threatening or controlling behaviors than SCV. Contrary to our hypothesis, harassment was not associated with physical health symptoms; however, marital IPV, specifically CCV, was directly related to more physical health symptoms. If changes in physical health take longer to surface, this could explain why marital, but not postseparation, control dynamics were related to worse physical health (Lorenz, Wickrama, Conger, & Elder, 2006). Future studies should follow mothers for longer periods to determine the effects of sustained harassment on their physical health.
Contrary to our expectations, social support did not protect divorcing mothers from the negative effects of conflict and harassment. The measure of social support used in this study asked about perceived informal support, not received or formal support, and did not differentiate among emotional, instrumental, and informational support. In the context of early separation, certain types of support (e.g., practical/instrumental vs. emotional) may be considered more helpful and perhaps may be more effective in buffering negative effects on health (Bowker, 1984; Gielen, McDonnell, Wu, O’Campo, & Faden, 2001). The measure also did not assess the quality of interactions with support members, which is important because past research has shown that support can often come with unsolicited advice and/or criticism (Zoellner, Foa, & Bridigi, 1999). Social conflict can diminish the influence of positive support (Guruge et al., 2012). Finally, there is some evidence that when support members share similar experiences (e.g., also going through divorce and/or IPV), they may unintentionally normalize experiences of conflict and harassment (Levendosky et al., 2004). Instead of moderating the effects of postseparation stress, social support was directly related to fewer physical health symptoms. Moreover, in the context of CCV as well as NV, social support at all levels reduced PTSD over time. These findings concur with an overall or direct benefit of social support for positive health rather than a stress buffering process (Cohen & Willis, 1985; Levendosky et al., 2004).
Our findings should be considered in the context of study limitations. Data were collected in a single U.S. county from mothers who were responsive to our recruitment letter so they cannot be generalized to broader populations. The study relied on data from a single reporter, so concerns regarding shared method variance should be considered. Negative life events were measured retrospectively over the prior year so these reports may be subject to recall bias. The study took place over a 1-year period, during which many of the women did not finalize their divorces. It is crucial that future research assess these dynamics over a longer period, especially given that physical health impacts take longer to manifest. Finally, our sample size was too small to allow us to examine (rather than control for) the effects of sociodemographic characteristics that may alter associations between postseparation stressors and health outcomes. Despite these limitations, our study was strengthened by the longitudinal design, in-person data collection method, and use of valid measures. Our findings highlight the need to examine the effects of coparenting conflict and harassment separately. Negative events are best understood as a contextual factor that complicates and magnifies the detrimental effects of postseparation stressors. Finally, our research continues to demonstrate the importance of differentiating between types of IPV in relationships.
Footnotes
Authors’ note
An earlier version of this paper was presented at the annual conference of the National Council on Family Relations in 2017.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Child Health and Human Development (NICHD, R21HD061559A), the Department of Human Development and Family Studies and Office of Research in the College of Agricultural, Consumer and Environmental Sciences at the University of Illinois at Urbana-Champaign, and Hatch Grant 793-348 from the USDA National Institute of Food and Agriculture.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. Requests for data or materials used in the research should be emailed to the first author at