
Abstract
It is common for romantic partners to influence one another’s health maintenance behaviors. Previous research has examined positively and negatively framed social control messages to understand health behavior outcomes and relational affect; however, this study confirms and extends previous research by studying the associations between health transformations (from interdependence theory, health behaviors enacted for the partner) and relationship satisfaction. Data from a cross-sectional dyadic survey of heterosexual couples were analyzed using actor–partner independence models. As expected, dyadic results showed that positive social control was associated with greater healthy and fewer unhealthy partner transformations, whereas negative social control was associated with lower relationship satisfaction and more unhealthy transformations. Further, the breadth of partner health behaviors that individuals attempt to influence moderated the associations between social control and relationship satisfaction and health transformations. We discuss how the results from this study underscore the health implications associated with the nature and breadth of social control communication in romantic relationships.
Keywords
Decades of research confirms that social relationships play an important role in understanding personal well-being and health (Holt-Lunstad, 2018). Communication likely serves as one mechanism through which these health outcomes are realized, as individuals directly (Tucker, Elliot, & Klein, 2006) or indirectly (Tucker, 2002) enact social control to encourage others’ adoption of health-enhancing behaviors and discourage their engagement in unhealthy behaviors (Umberson, 1987). In a seminal study, Lewis and Rook (1999) reported that spouses were the most likely—and most effective—source of health-enhancing social control messages. Yet, health-related social control messages are not uniformly effective in eliciting partners to change their behavior.
The dual effects model of social control (Lewis & Rook, 1999) provides insight into the way in which personal relationships influence health. The model hypothesizes that health social control messages will contribute to negative affect (i.e., psychological distress) and health behavior change. Related, the domain specific model of social control predicts an alignment in the outcomes of positive and negative social control messages: that positive social control is independently associated with positive affect and negative social control with negative affect (e.g., Okun, Huff, August, & Rook, 2007). Using elements of the dual effects and domain specific models, the current study examines positive and negative social control strategies in a dyadic design of interdependent partners. Within the context of romantic relationships, individuals’ receptivity to influence may also be explained by interdependence theory (Kelley & Thibaut, 1978), which outlines the circumstances in which people make behavior changes for their partner or relationship. Given that health-related influence (Burke & Segrin, 2016) and interdependence (Kelley & Thibaut, 1978) are both associated with relationship satisfaction, this study examined behavior change and relationship satisfaction as outcomes of receiving positive and negative social control. This study builds on and extends previous research by fusing social control and interdependence theories to better understand how relationship satisfaction is associated with receiving positive and negative health-related social control communication from one’s romantic partner.
Health-related social control
People in romantic relationships use social control to persuade a partner to reduce or stop health-compromising behaviors or to encourage healthy behaviors (Butterfield & Lewis, 2002). A recent meta-analysis affirmed the effectiveness of interpersonal social control. Across 35 studies of health-related social control, spanning decades of research and a variety of health behaviors, Craddock, vanDellen, Novak, and Ranby (2015) reported an association between receipt of social control messages and health behavior outcomes. Health influence messages vary in tone, however, leading some scholars to evaluate the independent effects of positive and negative social control messages.
Positive social control messages often include praise, positive emotion (Butterfield & Lewis, 2002), encouragement, reminders, and suggestions (Fekete, Geaghan, & Druley, 2009) with the intent of influencing a partner’s healthy behavior adoption. Alternatively, negative social control messages often communicate guilt, anger, withdrawal, or negative emotions (Fekete et al., 2009). Positive social control is more commonly reported in romantic relationships (Burke & Segrin, 2017) and is considered more desirable (Tucker & Mueller, 2000). Positive social control is often more effective in inciting partner behavior change and is positively associated with relationship satisfaction (Craddock, vanDellen, Novak, & Ranby, 2015). In comparison, negative influence messages often have deleterious relationship effects (Dillard & Fitzpatrick, 1985), as they may elicit an indirect sense of obligation or compliance (Lewis & Rook, 1999; Tucker, 2002; Umberson, 1987). Moreover, these negative messages can be counterproductive or ineffective in influencing partner health behavior change (Butterfield & Lewis, 2002), even resulting in “backfiring” (Craddock et al., 2015), health-compromising behaviors (Helgeson, Novak, Lepore, & Eton, 2004; Tucker & Anders, 2001), or less healthy diet and more negative emotional outcomes (Dailey, in press).
According to Dailey (in press), integrating different, but related, theories on health-enhancing communication helps to explain greater variance in people’s diet and exercise outcomes. When it comes to healthy behavior changes in relationships, dyadic theories, such as interdependence theory, provide insight into the outcomes that partners experience as a function of the interdependence and mutual influence inherent within their interactions (Lewis et al., 2006). As such, the relational dynamics associated with social control and partner outcomes may be further elucidated through the application of interdependence theory and relational transformations.
Social control and health behavior transformations
Interdependent relationships provide a context for studying health-related influence; in one study, an overwhelming majority of married couples (95%) reported trying to influence or regulate their partner to engage in health maintenance behaviors (Lewis & Butterfield, 2007). One factor affecting individuals’ health behavior change is their orientation toward accepting influence from a relational partner (Sullivan, Pasch, Schreier, & Healy, 2018), which can be understood through interdependence theory (Kelley & Thibaut, 1978), this theory suggests that individuals in relationships consider their own and their partner’s needs and outcomes as they make decisions. Perhaps, a partner’s health influence message presents an opportunity to transform, or change, a personal health behavior.
Kelley’s (1979) work on interdependent relationships builds upon the premise that relational partners experience noncorrespondence (i.e., wanting a partner to stop doing something or do more of something), which becomes evident through the expression of interpersonal influence. When faced with a conflict of interest, individuals may decide to converge their behavior to align with the partner, termed a transformation of motivation (Kelley, 1979). In the context of health-related communication, individuals’ expression of social control might highlight a conflict of interest; partners can choose to respond by transforming their health behaviors to meet these individuals’ wishes. Transformations of motivations are important to study from the perspective of both partners because they represent an appraisal of and response to interpersonal processes. According to Lewis et al. (2006), transformations of motivation stimulate joint consideration and coordination of health behavior change, transforming “from a primarily self-centered orientation or motivation to one that is more pro-relationship and health enhancing” (p. 1373).
Whereas research on health behavior convergence suggests that partners often align eating behaviors, exercise, and weight gain or loss with one another (Burke, Beilin, Dunbar, & Kevan, 2004; Craig & Truswell, 1990; Treiber et al., 1991), and decrease smoking to align with partner preference (Rook, Thuras, & Lewis, 1990), these studies primarily focus on health behavior engagement rather than health behavior transformations. In the current study, health behavior transformations are instead conceptualized as individuals’ attribution of changes in their health behaviors to their partner. Given the range of behaviors on which couples converge, this study examines a variety of health transformation contexts, including diet, exercise, sleep, substance use, and routine exams and advice from health professionals, as these behaviors have proved to lower risk for disease (McGinnis & Foege, 1993; Vincent et al., 2017).
Focusing solely on healthy behavior transformations would be shortsighted, as health transformations may include unhealthy behaviors as well. Indeed, Homish and Leonard (2008) noted that both healthy and unhealthy behaviors of one individual could be an influential source of behavior change for one’s partner within a romantic relationship. As examples, sometimes individuals reported engaging in unhealthy behaviors because their partners also engage in this behavior (e.g., drug use, Powers & Anglin, 1996), or because social control attempts by one’s social network were too frequent (Lewis & Rook, 1999). In addition to examining healthy behavior transformations, this study examines the extent to which partners engage in unhealthy transformations of the aforementioned behaviors and also aims to understand these transformations in light of the frequency and breadth of influence communicated in these relationships.
Social control frequency and breadth of influence
In the context of health behavior change, partners report wanting their spouse to change two behaviors, most commonly diet and exercise (Tucker & Anders, 2001). Beyond diet- and exercise-related changes, however, other researchers have found that partners influence each other with regard to seeking medical help (Markey, Markey, & Gray, 2007), substance use, sleep (e.g., Okun et al., 2007), tobacco or smoking (e.g., Westmaas, Wild, & Ferrence, 2002), condition-specific medical adherence (Fekete et al., 2009), and general health (Tucker, 2002). Given this range of possible health influence topics, it follows that positive or negative influence may function differently when it is isolated to one or two behaviors compared to spanning many different health contexts. As such, building on previous research that examines social control frequency (Burke & Segrin, 2017; Butterfield & Lewis, 2002), the current study examines the frequency of social control messages in combination with the breadth of influence attempts. According to the dual effects model of social control (Lewis & Rook, 1999), which suggests that ineffective health influencers might arouse negative partner affect and to Lewis et al. (2006), who suggest that dyadic theories allow for a better understanding of couple functioning, it is important to examine relationship satisfaction as an additional outcome of health-enhancing communication in romantic relationships.
Social control and relationship satisfaction
The quality of the relationship may be central in understanding how health messages from a romantic partner are interpreted (Sarason & Sarason, 2001) and how a person reacts to health influence messages (Tucker, 2002). Indeed, Dailey (in press) found that positive social control was associated with greater positive emotions, and negative social control was associated with greater negative emotions. Similar to the dual effects and domain specific models of social control, these findings highlight the relationship between social control and affect, but provide limited insight into the potential relationship satisfaction outcomes associated with these health-related social control messages from a partner. Given the mutual influence that occurs within these interactions, it is likely that relationship functioning—more specifically, relationship satisfaction—is salient within the context of health-enhancing social control (Lewis et al., 2006). The existing research in this area suggests that a halo effect exists: that more positive influence is often associated with better relationship quality outcomes (Markey et al., 2007), and that people often attribute more positive motives to a partner’s social control behaviors if they are satisfied in their relationship (Knoll, Burkert, Scholz, Roigas, & Gralla, 2012). Although few studies examine positive and negative health-related messages from a dyadic perspective, evidence suggests that receiving positive social control messages is related to greater partner relationship satisfaction (Burke & Segrin, 2016).
Using social control theory and interdependence theory, we pose the following hypotheses and research questions. As mentioned previously, because health-related social control can take a variety of forms (Lewis, Butterfield, Darbes, & Johnston-Brooks, 2004) and is associated with a range of outcomes, we include both healthy and unhealthy behavior outcomes in this study. Similarly, the interdependence inherent within these strategic relational exchanges (Lewis et al., 2004) underscores the value of examining dyadic reports of these positive and negative influence messages. Therefore, specific to the hypotheses, we predict interpersonal outcomes (i.e., partner effects), and we report actor effects for each hypothesis. Specific to the research questions, we explore both individual and interpersonal associations among variables.
Method
Procedures and participants
The study procedure received Institutional Review Board approval. Participants were recruited using study announcements posted on Craigslist.com, and college students at two of the authors’ institutions were invited to participate or refer eligible couples (i.e., over 18 and in a romantic relationship, have their own e-mail address). Each partner was e-mailed a link to an online questionnaire, instructed to complete it separately, and provided with a unique code to enter into the questionnaire for data matching purposes. Participants were encouraged to take the survey without their partner present. The online survey, which took approximately 30 min for individuals to complete, began with informed consent and outlined compensation: Craigslist individuals were paid US$10 and college-student recruited individuals received an option for course credit for referral.
Of the 336 couples invited to participate with a secure survey link and unique e-mail code, the final sample included 243 male/female matched couples (72% response rate). Of those matched individuals, 442 had complete data on the primary study variables. All individuals with complete or partial data were retained for analyses and only individuals with complete actor and partner data on each variable in the model are reported; therefore, the final Ns range from 362 to 416. Participants in the sample ranged in age from 18 years to 71 years (M = 32.08, SD = 13.49) and were in their relationships for nearly 9 years (M = 8.98 years, SD = 11.11, ranging from 4 months to 44.5 years). Over half (62.66%) lived with their partner full time, and 41.88% had one or more children with their partner.
Most participants were employed full time (47.30%), part time (17.01%) or were enrolled as full or part-time college students (24.48%). Education attainment varied from high school diploma (10.35%), college coursework (41.41%), college degree (25.47%) and post-graduate (17.39%). Household income ranged from less than US$50,000 annually (44.4%), US$50,000–100,000 (24.74%), to over US$100,000 (30.87%). Most identified as European American (77.45%), Hispanic or Latino (11.90%), African American (4.18%), more than one race or ethnicity (3.76%), and Asian, Pacific Islander, or American Indian (<3%).
Measures
Health-related social control
Positive and negative health-related social control questions were adapted from the health-related social control scale (Butterfield & Lewis, 2002; Lewis et al., 2004). The prompt began, “How often, in the past 6 months, have you used these tactics to get your partner to engage in healthy activities or behaviors?” and included 13 separate items, ordered randomly, with brief descriptions for clarity. Response options included a Likert-type scale, where 1 = never and 7 = frequently. A principal component factor analysis with direct oblimin rotation (which assumes factors are correlated) was used to examine the factor structure of social control. The scree plot revealed two factors with eigenvalues above 1, accounting for 73.54% of the variance. Six items loaded to component 1 with factor loadings from .63 to .90. Positive strategies included: asked partner to do something to improve their health, expressed positive emotion (displayed happiness, pleasure, kindness to partner when engaging in healthy activities), stated importance (tried to help partner understand why healthy activities are important), made suggestions (offered alternative ideas to help improve partner’s healthy lifestyle), persistence (reminded or reinforced previous requests to be healthy), and reasoned (introduced evidence, examples, or facts to partner about health), M = 19.29, SD = 10.29, range 6–42 (women M = 21.28, SD = 10.41, men M = 17.38, SD = 9.79, α = .92 women, α = .93 men). Factor loadings for component 2 ranged from .54 to .96 and included six negatively valenced items: bargained (offered partner an exchange or trade-off to engage in healthy behaviors), expressed negative emotions (displayed anger, frustration, resentment for not engaging in healthy activities), guilt (made your partner feel bad for being unhealthy), invoked obligation (made partner feel like he/she has to engage in healthy activities out of obligation to you, work, children, etc.), told (made a demand that partner be healthier), and used withdrawal (avoided interacting with partner to get them to engage in healthier activities), M = 11.33, SD = 7.94, range 6–42 (women M = 11.82, SD = 7.97, men M = 10.86, SD = 7.81, α = .91 women, α = .93 men). One item, persuade (used influence to get partner to engage in healthy behaviors), loaded onto both factors and was dropped. The majority of the positive and negative social control items in this study align with previous research (Burke & Segrin, 2016).
Breadth of health influence
To gauge participants’ breadth of influence attempts, a count variable began with the probe, “What types of health behaviors do you attempt to influence your partner to change?” The 10 topics included types of food eaten (54.9% of respondents responded that they attempt to influence partner in this area), amount of food eaten (32.9%), types of exercise or physical activity (33.7%), amount of exercise or physical activity (39.7%), how often partner gets checkups (25.9%), how partner interprets or follows advice from medical professionals (24.1%), the types of substances (alcohol, tobacco, or drugs) partner uses (21.6%), how often partner uses substances (24.1%), how much time partner sleeps (26.7%), and partner’s sleep patterns (24.3%). Responses were summed across 10 topics, such that higher scores represent a greater breadth of influence, M = 3.08, SD = 2.30, range 0–10 (women M = 3.56, SD = 2.30, men M = 2.61, SD = 2.19), with 13.6% reporting they attempt to influence 0 partner behaviors, 13.6% 1 behavior, 18.9% 2 behaviors, 17.5% 3 behaviors, 10.3% 4 behaviors, 9.3% 5 behaviors, 8.8% 6 behaviors, 4.1% 7 behaviors, 1.9% 8 behaviors, 0.6% 9 behaviors, and 1.4% attempt to influence all 10 behaviors.
Healthy and unhealthy transformations
To assess how often individuals made health-related transformations for their partners, participants were given the instructions: Some people do healthy things for their partners. Respond to the following about how often, in general, you do this for your partner. How often do you: 1) eat healthier, 2) get more physical activity, 3) monitor health (get checkups, tests), 4) avoid alcohol, tobacco, or drugs, and 5) get more restful sleep because of your partner?
An exploratory factor analysis was conducted and revealed that healthy and unhealthy transformations loaded on to separate factors. Scree plots for the separate groups revealed distinct factors with eigenvalues greater than one. For healthy transformation items, n = 463, factor loadings ranged from .62 to .71, with 45% of the variance explained. The items assessing transformations were intended to be formative versus reflexive (Edwards & Bagozzi, 2000), representing the health-related transformations that each person attributed to their partner. In other words, we did not expect that responses to transformation frequency across different items would necessarily be correlated, but we did think that each item contributed to a broad picture of health transformations. Therefore, responses were summed across healthy transformations to create a variable representing the total frequency of health behaviors done for the partner, M = 6.76, SD = 5.10, range 0–20 (women M = 6.37, SD = 5.10, men M = 7.14, SD = 5.06). For unhealthy transformations, n = 466, factor loadings ranged from .52 to .74, with 40% of variance explained. Similarly, responses were summed to create a frequency of unhealthy behavior transformations for the partner, M = 2.70, SD = 3.44, range 0–18 (women M = 2.85, SD = 3.34, men M = 2.55, SD = 3.54).
Relationship satisfaction
Relationship satisfaction was assessed using 8 items from Rusbult, Martz, and Agnew’s (1998) satisfaction scale of the Investment Model, such as “My relationship is close to ideal,” rated on a 1 = strongly disagree to 7 = strongly agree scale, M = 5.94, SD = 1.26 (women M = 5.89, SD = 1.31, men M = 6.04, SD = 1.14, α = .96 women, α = .95 men).
Data analysis
Data from individuals nested in couples were examined in multilevel models using SAS PROC mixed to account for interdependence among participants. Consistent with Kenny, Kashy, and Cook’s (2006) Actor Partner Interdependence Model, the models for each hypothesis and the research questions included actor (individual) and partner (interpersonal) independent variables. Accordingly, the model testing the first hypothesis tested an association between actor and partner reports of positive (H1a) and negative (H1b) social control and included healthy behavior transformations as the outcome. Parallel models were run to examine relationship satisfaction as the outcome (H2a and H2b) and unhealthy behavior transformations as the outcome (RQ1).
Three additional models were run to test the interactions being explored in RQ2 and RQ3. These models were parallel to the preceding three models, with the following independent variables: actor and partner positive and negative social control, actor and partner reports of breadth of influence, and the interaction terms between the social control and breadth of influence variables. RQ2 specified two separate dependent variables, healthy and unhealthy transformations, separately. RQ3 specified relationship satisfaction as the dependent variable. Significant interaction term results were decomposed by graphing regression slopes 1 standard deviation above and below the sample mean (Aiken & West, 1991).
Potential covariates were selected based on previous research on interpersonal health influence and health outcomes research (e.g., Markey et al., 2007; Tucker & Mueller, 2000; Umberson, 1987). Models were first estimated using main effects for predictor variables, then control variables were estimated. The following variables were dummy-coded and tested in all analyses: race (22.5% non-White), education (42.9% college-education or higher), one or more children (41.9%), and marital status (43.8% married); age was a continuous control. Additionally, we tested models including the recruiting method (either college student recruit, 91%, or Craigslist ad), and directional effects of influence by participant sex. There were no sex differences in any of the models. Only significant control variables were retained in the results for parsimony.
Results
Correlations among study variables are in Table 1. All intraclass correlations for the hypotheses and research questions were significant at the p < .001 level, with coefficients between .46 and .66.
Correlations among study variables.
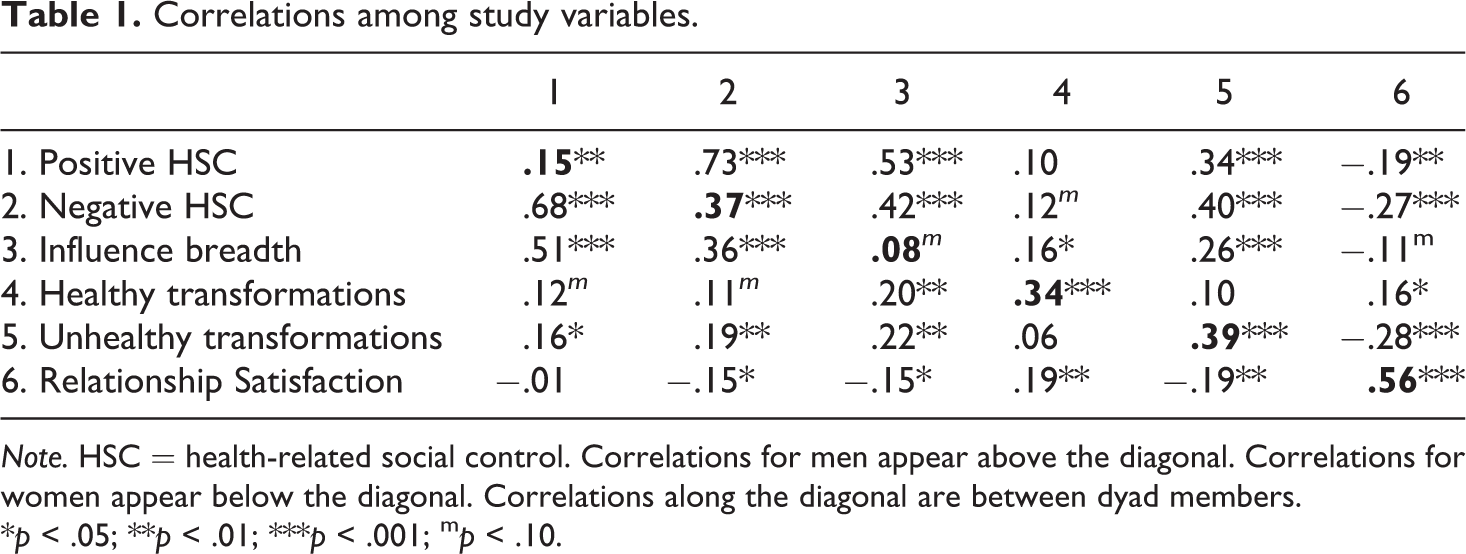
Note. HSC = health-related social control. Correlations for men appear above the diagonal. Correlations for women appear below the diagonal. Correlations along the diagonal are between dyad members.
*p < .05; **p < .01; ***p < .001; m p < .10.
The first hypothesis predicted that positive social control would be associated with more partner healthy behavior transformations (H1a), and negative social control would be associated with fewer partner healthy behavior transformations (H1b). The results revealed one significant partner effect in the model, n = 416: Individuals’ positive health social control was positively associated with their partner’s reported healthy behavior transformations, b = .11, SE = .03, t (407) = 3.23, p = .001, B = 1.13. For every 1 unit change in individuals’ positive social control, their partner’s reported healthy transformations increased by 1.13 or 5.66%. Individuals’ negative social control was not significantly associated with their partner’s reported healthy behavior transformations. Similarly, neither of the actor effects were significant for positive or negative social control. Thus, the first hypothesis was supported for positive social control only.
The first research question (RQ1) probed whether positive or negative social influence was associated with unhealthy behavior transformations. Two significant partner effects emerged, controlling for recruitment method. Individuals’ more frequent positive social control was significantly associated with their partner’s reports of fewer unhealthy transformations, b = −.06, SE = .02, t (395) = −2.87, p = .004, B = −0.62, indicating that a 1 unit change in individuals’ positive social control was associated with a decrease of −.62 in their partner’s reports of unhealthy transformations (or −3.43%). In contrast, individuals’ more frequent negative social control was significantly associated with their partner’s reports of more unhealthy transformations, b = .10, SE = .03, t (417) = 3.46, p = .0006, B = 0.79, indicating that a 1 unit change in individuals’ negative social control was associated with an increase of .79 in their partner’s reports of unhealthy transformations (or 4.41%). In terms of actor effects, individuals’ more frequent negative social control was significantly associated with their own reports of more unhealthy transformations, b = .07, SE = .03, t (417) = 2.62, p = .009, B = 0.56, indicating that a 1 unit change in individuals’ negative social control was associated with an increase of .56 in their own reports of unhealthy transformations (or 3.8%). There was no significant actor effect of positive social control on unhealthy transformations.
The second research question (RQ2) probed the interaction of use of frequent positive and negative social control and breadth of influence across different health domains in associations with healthy and unhealthy behavior transformations. One significant interaction effect emerged for healthy behavior transformations, such that individuals’ breadth of influence moderated the association between their use of negative social control and their healthy behavior transformations, n = 416, b = .04, SE = .02, t (403) = 2.14, p = .03. The results indicated that the relationship between individuals’ negative social control use and their healthy transformations was strongest with greater breadth of influence across different health domains, b = .11, SE = .05, p = .03, B = 0.79. For a 1 SD change in negative social control, healthy transformations increase by 0.79 (3.96%) when individuals engage in a greater breadth of health influence (see Figure 1). The slope for lower breadth of influence was not significant. No significant results emerged for positive social control or for unhealthy behavior transformations in these models, and no significant partner interaction effects emerged for RQ2.
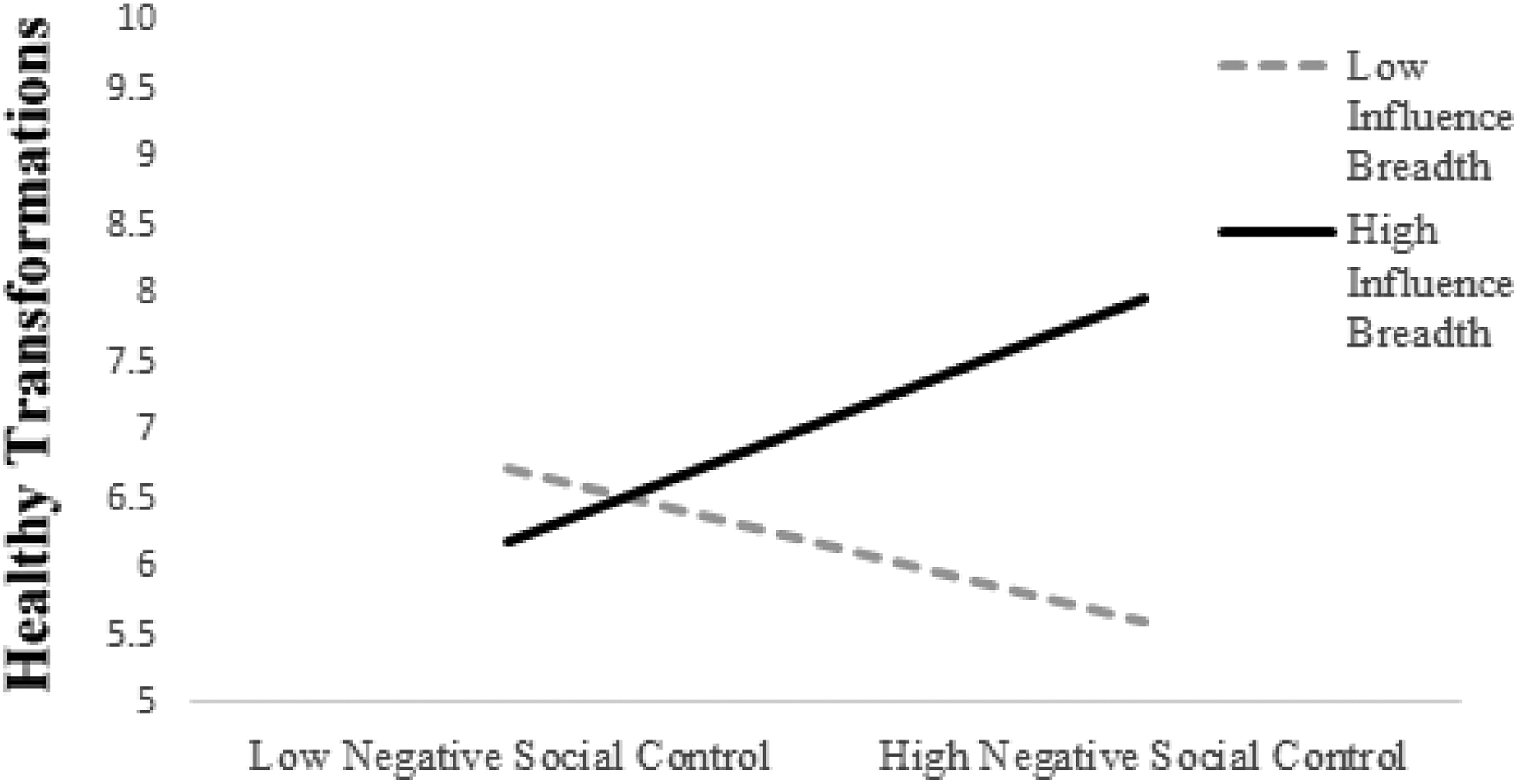
Health influence breadth moderates the association between negative social control and healthy transformations (actor effect).
The second hypothesis predicted that positive social control would be associated with greater partner relationship satisfaction (H2a) and that negative social control would be associated with lower partner satisfaction (H2b). Again, the results illustrated one significant partner effect in the final model, which included age as a significant control variable (age was negatively associated with relationship satisfaction; n = 362 due to missing data on age variable): Individuals’ negative social control was associated with lower partner-reported relationship satisfaction, b = −.03, SE = .01, t (362) = −2.63, p = .009, B = −0.24. For every 1 unit change in individuals’ negative social control, their partner’s relationship satisfaction decreased by −0.24 or −3.40%. Individuals’ positive health social control was marginally positively associated with partner-reported relationship satisfaction, however, b = .02, SE = .01, t (342) = 1.87, p = .06, B = 0.21. There was no significant actor effect for positive social control, but a significant actor effect emerged for negative social control, b = −.03, SE = .01, t (362) = −2.68, p = .008, B = −0.24, indicating that a 1 unit change in individual’s negative social control was associated with a decrease of −0.24 in their own relationship satisfaction (or −3.40%). The second hypothesis was supported for negative social control only.
The third research question (RQ3) probed the interaction of the use of frequent positive and negative social control and breadth of influence across different health domains in associations with relationship satisfaction. Two significant actor interaction effects emerged for relationship satisfaction, controlling for age. The results indicated that individuals’ breadth of influence moderated the association between their use of positive social control and relationship satisfaction, n = 362, b = −.01, SE = .00, t (325) = −3.19, p = .002, and also between their negative social control and their relationship satisfaction, b = .02, SE = .01, t (349) = 3.22, p = .001. Specifically, the relationship between positive social control and relationship satisfaction was strongest for people with a low breadth of influence topics discussed, b = .05, SE = .01, t (326) = 3.62, p = .0003, B = 0.51. For a 1 SD change in positive social control, relationship satisfaction increases by 0.51 (7.35%) when individuals engage in less breadth of health influence (see Figure 2). The slope for greater breadth of influence was not significant. Results for negative social control revealed that greater use of negative social control was associated with lower relationship satisfaction with lower health influence topic breadth, b = −.08, SE = .02, t (353) = −4.14, p < .001, B = −0.64. For a 1 SD change in negative social control, relationship satisfaction decreases by 0.64 (−9.07%) when individuals engage in less breadth of influence (see Figure 3). The slope for greater breadth of influence was not significant. Taken together, these two intrapersonal interaction effects confirm the importance of examining social influence in terms of the frequency of positive and negative messages, as well as the number of health maintenance behaviors a person influences their partner to change. No significant partner interaction effects emerged for RQ3.
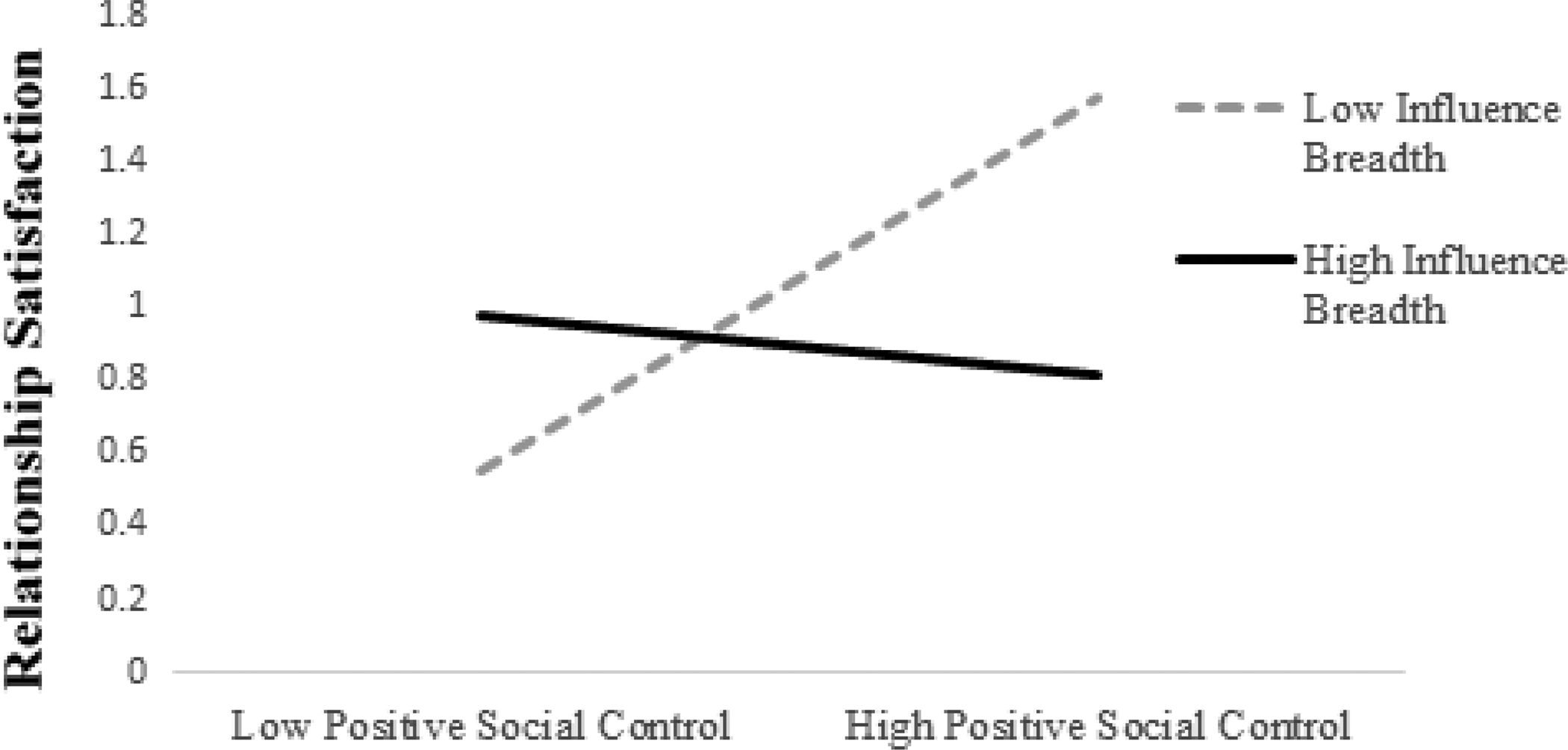
Health influence breadth moderates the association between positive social control and relationship satisfaction (actor effect).
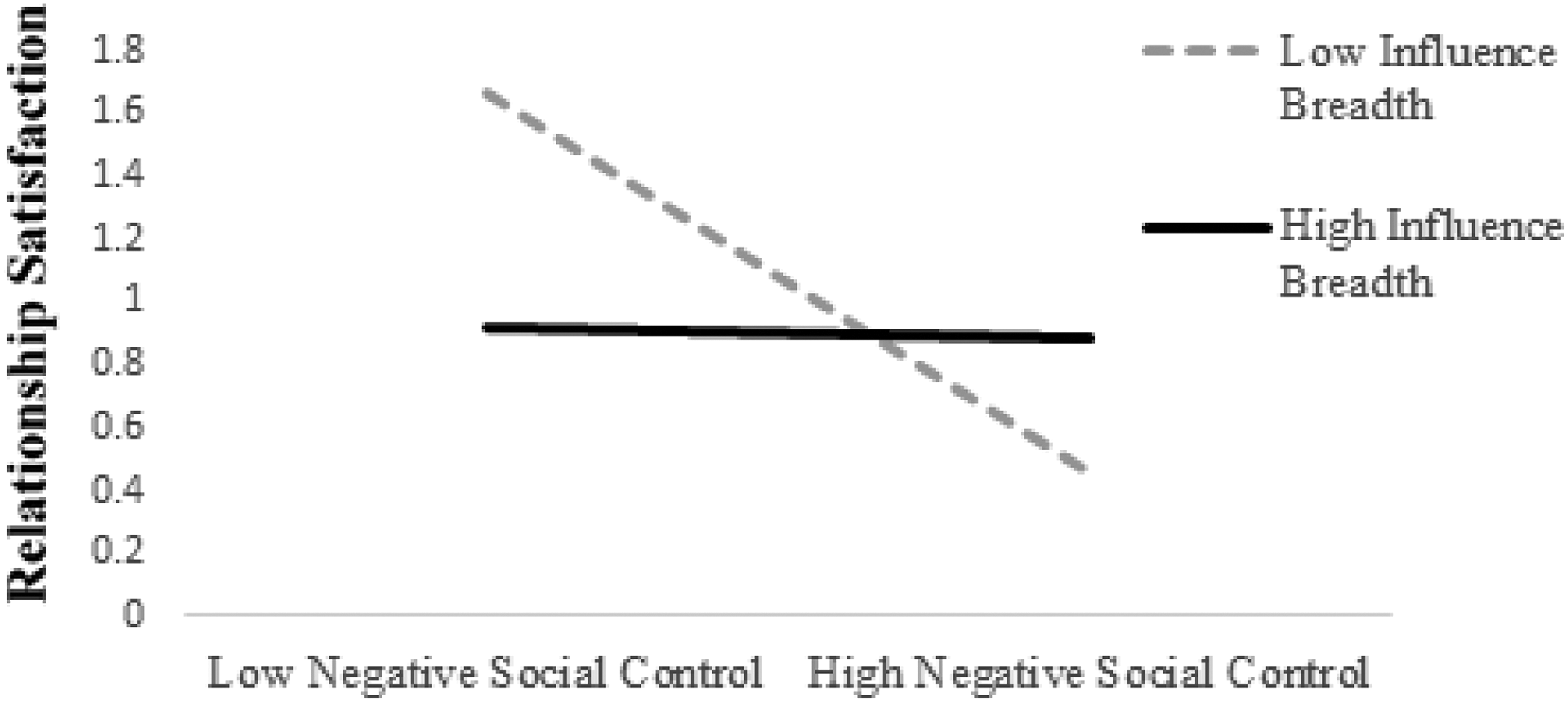
Health influence breadth moderates the association between negative social control and relationship satisfaction (actor effect).
Discussion
This study built upon and extends the dual effects and domain specific models of social control (Lewis & Rook, 1999; Okun et al., 2007) by incorporating interdependence theory (Kelley, 1979) to frame the investigation of health behavior change and relationship quality associated with social control communication in romantic relationships. First, in line with previous research, positive and negative social control attempts functioned in tandem in associations with health behavior transformations and relationship satisfaction. Second, and importantly, the study extends previous research regarding the nuanced effects of positive and negative social control by examining unhealthy behavior transformations, as well as the range of health influence across different health domains.
The effects of negative social control were straightforward: Using more negative social control was not associated with the partner’s healthy transformations (H1b), but was associated with own and partner reports of more unhealthy transformations (RQ1), and own and partner lower relationship satisfaction (H2b). In regard to unhealthy transformations, the present findings offer an empirical extension of the nature of dyadic social control in to the realm of unhealthy behavior. Previous dyadic, cross-sectional health influence research revealed a consistent pattern for negative social control and health-compromising behavior outcomes (Tucker & Anders, 2001). Even specific forms of negative health influence have been linked with deleterious outcomes in other work. For example, restricting or monitoring a partner’s eating is associated with higher partner body mass index and lower body satisfaction (Markey, Gomel, & Markey, 2008), and negatively framed warnings about food are associated with lower patient adherence to a diabetic diet (Stephens, Rook, Franks, Khan, & Iida, 2010). Consistent with these studies, we also found evidence of “backfiring behaviors” (Craddock et al., 2015) for negative social control. In our study, not only was greater negative social control associated with lower relationship satisfaction (H2b), but partners also reported increased frequency of unhealthy transformations (RQ1). The evidence suggests that a pattern of negativity may be present in influence and unhealthy behaviors. Findings echo the intrapersonal and relational impacts of social control in the dual effects model (Lewis & Rook, 1999; Okun et al., 2007).
Congruent with the existing research (Craddock et al., 2015), using positively framed influence messages to get a partner to engage in healthy behaviors was associated with partner-reported health behavior change. Whereas studies in this area have focused on health behaviors in general (Burke & Segrin, 2017), this study drew from interdependence theory to examine health behavior transformations specifically, shedding light on the relationship between one partner’s perception of their health-related influence and the other partner’s perceptions of their healthy behavior changes. That is, one person’s reports of using more frequent positive social control messages to influence their partner to be healthy were associated with their partner’s reports of making more healthy (H1a) and fewer unhealthy (RQ1) transformations for them.
From an interdependence theory standpoint, these partner effects exemplify the process of a transformation of motivation. That is, a partner perceives making a health behavior change in response to, or because of their partner, which in turn should shape their behavior toward their partner (Rusbult & Arriaga, 1997; Rusbult & Van Lange, 2003). In the present study, the interdependent nature of relationship influence was visible across the healthy and unhealthy transformations. This transformative process tends to bode well for relationship satisfaction in previous research (Van Lange et al., 1997); however, reports of using positive social control were not significantly associated with one’s own relationship satisfaction in the current study (H2a). These patterns underscore the earlier points by both Dailey (in press) and Lewis et al. (2006) that multiple theories are useful in trying to understand the associations between forms of positive and negative social influence and partner healthy and unhealthy transformations.
Providing additional context for the dyadic effects between social control and partner transformations, the breadth of influence attempts across different health domains was consequential to consider. The interactions in Figures 2 and 3 (specific to RQ3) depict an intrapersonal influence process in which a person reports about their own relationship satisfaction differently, depending on how many health behaviors they are trying to influence in their partners. When individuals reported less health influence breadth, whether they used positive social control or negative social control mattered; as the targeted, positive influence was associated with their own greater relationship satisfaction (Figure 2) and the targeted, negative influence was associated with lower relationship satisfaction (Figure 3). In other words, spreading out influence across different health behavior domains (in our sample, attempts to influence more than five of a partner’s health behaviors) did not seem to change the association between social control and relationship satisfaction. It was the more targeted influence—when a person reported trying to change only one or two partner behaviors—in which we found that relationship satisfaction reports vary. The evidence indicates that individuals who are trying to influence a partner consistently about the same few topics may find that their satisfaction varies with the tone of their influence attempts. Perhaps individuals who are satisfied widen the scope of influence in order not to come across as “nagging” on a partner to be healthier (Lewis & Rook, 1999) or that for dissatisfied individuals, their negative affect toward a partner is related to the way they communicate about health topics (e.g., using guilt or withdrawal to get a partner to be healthier).
The interaction effects presented in Figure 1 (specific to RQ2) provide additional support for our argument that the breadth of influence matters, especially when combined with negative social control messages. Our participants reported greater healthy transformations with increased breadth and negative social control. Practitioners might offer advice for individuals to construct interpersonal health influence messages carefully, either by narrowing or expanding the health behaviors they are trying to get a partner to change or by reducing negatively toned influence messages and increasing the frequency of positive influence messages. Here, evidence suggests that these strategies may work in tandem.
Lewis and Rook’s (1999) work offers support for understanding how interpersonal influence occurs for people in romantic relationships. Using frequent negative social control strategies and targeting just a single unhealthy behavior of a partner could signal relationship turmoil. Take, for example, the most frequently cited topic for health influence in this study: type of foods eaten. If an individual reports using frequent negative social control strategies such as guilt or expressing negativity, but is only targeting their partner’s food intake, the individual may report lower relationship satisfaction because their social control triggers conflict or because their expectations for how a partner should be responding to their influence are not met. Future research should continue to examine the range of topics for influence, as well how people use multiple forms of influence to persuade a partner to be healthier, and these associations over time.
Although this study provided valuable insight into health-related social influence in the context of romantic relationships, there are some limitations that should be addressed. While the healthy and unhealthy transformations variables represent a novel operationalization of the transformations of motivation context relative to interpersonal health behaviors, we only captured changes that people were making, which might not be inclusive of transformations that are not changes, but have been enacted previously, or even routinely. The health transformations measure would benefit from future investigation and application. For example, for the item “I consume alcohol, tobacco, or drugs because of my partner,” we would separate these items from each other (one question about alcohol, one question about tobacco, one question about drugs) to see the unique contributions posed by each of these questions and also to add additional questions to these scales, given that at five items each, the scales were fairly brief. We would also clarify the directions to the participants (e.g., “sometimes people do unhealthy things for their partner” could be changed to “given your partner’s influence on you, how often do you participate in each of the following activities”). An additional idea for future research could be taking a more nuanced approach to the transformation measures; for example, asking the benefits to the self, the romantic partner, and to the romantic relationship (Visserman, Righetti, Impett, Keltner, & Van Lange, 2018) when engaged in healthy and unhealthy transformations.
Another idea for future research is specific to understanding health-related social control. In addition to assessing health social control frequency tactics and breadth of influence attempts across various domains, future work in this area could attempt to discern influence focused on encouraging health enhancing behaviors versus avoiding health compromising behaviors. For example, the most frequently reported influence was over “types of foods eaten” (55% of our sample reported attempting influence in this domain), yet we did not ask a more specific question such as “How often do you attempt to get your partner to eat more nutritious or healthful foods?” or “How often do you attempt to get your partner to avoid unhealthy foods?”
Additionally, the cross-sectional design limits the findings to correlation and not causation and limits our ability to understand the directionality of the associations presented in this study (e.g., it is also possible that people in less satisfying relationships are more willing to enact negative social control). Other designs (e.g., daily diary designs; Young, Curran, & Totenhagen, 2012) may also help us further untangle the day-to-day experiences of positive and negative influence, partner health transformations, and relationship quality. Despite the varied sampling methodology, the sample is relatively homogeneous; thus, future work would benefit from studying couples in different socioeconomic and relational contexts.
By fusing elements of social control models with transformations of motivation from interdependence theory, this study was able to both confirm and extend research regarding positive and negative health-related influence in relationships. Beyond the theoretical advances made by this study, the findings also highlight several opportunities for application within a therapeutic or counseling setting, offering individuals and couples information about how to navigate health-related communication with a partner in a way that might result in healthy behavior change while also preserving relationship quality. Specific to couples, the data are quite clear that one person’s negatively-framed influence messages toward a partner can backfire. Not only do these negative communication strategies reflect lower satisfaction (for both the individual and the partner), but they actually may have the opposite effect than intended (in that a partner may enact more unhealthy behaviors). For applications to individuals, giving a partner frequent positive and specific praises may be especially rewarding. For a person who is using negative control strategies to try to get a partner to change their health behavior, spreading out the negative influence over many different behaviors may be personally beneficial (corroborated by Figures 1 and 3; one’s own relationship satisfaction and own reports of healthy transformations).
In conclusion, the findings emphasize interpersonal and intrapersonal processes in the dual effects model of social control. Findings build upon previous theory and research, confirming the importance of studying positive and negative social control messages as separate, as advocated in the domain specific model of social control, but also as dual contributors to health behavior change and relationship quality outcomes. Both the dual effects model and interdependence theory acknowledge that the interactive and interdependent nature of close relationships enhances—and complicates—our understanding of interpersonal influence in romantic relationships, which is reflected in the findings in this study.
Footnotes
Authors’ note
A version of this manuscript was presented at the November 2018 National Communication Association Conference, Salt Lake City, UT, USA.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by Hanover College faculty development grant to VJY.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are not available. The data can be obtained by emailing: