
Abstract
Guided by the communicative ecology model of successful aging (CEMSA), this study examined how older adults’ and their romantic partners’ age-related communication indirectly predicts older adults’ perceptions of aging well, depressive symptoms, and alcohol use disorder (AUD) symptoms, via aging efficacy. Older adults were profiled as engaged, bantering, and disengaged agers. Romantic partners were profiled as engaged, bantering–high health, disengaged, and gloomy agers. Bantering older adults, disengaged older adults, and older adults with disengaged partners reported lower perceptions of aging well and more depressive symptoms, via lower aging efficacy (relative to engaged older adults and older adults with engaged partners). Also relative to engaged older adults, disengaged older adults reported more AUD symptoms, via lower aging efficacy. The indirect association involving AUD symptoms suggests that the CEMSA’s boundary conditions might be expanded to include more objective variants of successful aging. Results also suggest the merit of future family studies on how age-related communication might predict successful aging.
Keywords
Global populations are comprised of an unprecedented number of older adults, and these numbers continue to grow. In the U.S., for example, the number of adults aged 65 and older is expected to more than double from 46 million in 2016 (15% of the population) to 98 million in 2060 (24% of the population; Mather, 2016). In the light of this, it is important to study successful aging.
This study considers global assessments of aging well, depressive symptoms, and alcohol use disorder (AUD) symptoms as three variants of successful aging. By examining these three facets of successful aging, this approach allows for older adults who are experiencing some type of physical disability (e.g., difficulty walking) to still be classified as aging successfully, provided that they have cultivated strong mental well-being and health behaviors over time in the same way that some of their counterparts who are not experiencing physical disability have cultivated. More specifically, the study examines whether or not older adults’ perceptions of their own and their romantic partners’ age-related communication are indirectly associated with these variants of successful aging, via aging efficacy. In what follows, we synthesize scholarship on how successful aging has been conceptualized and operationalized. We then draw on the communicative ecology model of successful aging (CEMSA; Fowler, Gasiorek, & Giles, 2015; Gasiorek, Fowler, & Giles, 2016) to explain how the age-related communication of older adults and their romantic partners may be indirectly associated with the variants of successful aging.
An overview of successful aging
Successful aging definitions can be broken down into two major lines of work: scholarship that treats successful aging more objectively (e.g., avoiding physical disease, being able to complete certain physical activities) and scholarship that treats successful aging more subjectively (e.g., having a strong sense of happiness or life satisfaction; Gasiorek et al., 2016). Researchers using the CEMSA, the framework guiding this study, have traditionally defined successful aging as the subjective assessment that one’s life is going well (Fowler et al., 2015). However, in more recent CEMSA research, Bernhold, Gasiorek, and Giles (2018) proposed that researchers include other more objective variants of successful aging alongside this, including depressive symptoms and unhealthy alcohol consumption. Depression is a diagnosable medical illness that involves strong feelings of sadness, loss of energy, and a lack of interest in activities once considered enjoyable (American Psychiatric Association, 2018). Unhealthy alcohol consumption can be considered in several ways, one of which is the presence of AUD. AUD refers to a diagnosable and chronic disease characterized by “compulsive alcohol use, loss of control over alcohol intake, and a negative emotional state when not using” (National Institute on Alcohol Abuse and Alcoholism, 2014). Scholars have recently included self-reported depressive symptoms (e.g., Hsu & Jones, 2012) and alcohol use (e.g., Bernhold et al., 2018) as indicators of successful aging.
Additionally, scholars have recommended that researchers incorporate lay adults’ definitions of successful aging into empirical investigations of this construct (Reichstadt, Sengupta, Depp, Palinkas, & Jeste, 2010). Lay adults have repeatedly mentioned low levels of depressive symptoms and healthy alcohol consumption as two components of successful aging. For example, asking older adults to define what successful aging means to them, Ferri, James, and Pruchno (2009) found that 33% of participants mentioned strong mental health (e.g., low levels of depressive symptoms) and 15% of participants mentioned healthy lifestyles (e.g., making healthy food and drink choices). Tate, Swift, and Bayomi (2013), likewise, found that lay participants mentioned cognitive health (e.g., not having mental illness, retaining one’s memory) and lifestyle behaviors (e.g., abstaining from cigarettes and alcohol, consuming alcohol in moderation) as key aspects of successful aging. More recently, Jopp et al. (2015) found that 43.8% of lay participants mentioned health behaviors (e.g., refraining from smoking, not consuming too much alcohol, consuming healthy diets) as part of their open-ended definitions of successful aging. Bowling (2006) reported that 46% of adults between ages 50 and 64, as well as 48% of adults between ages 65 and 74, defined successful aging as having strong mental well-being. Bowling used these findings to argue that the many definitions of successful aging should inspire researchers to consider multiple facets of successful aging. Following this recommendation, we consider general assessments of aging well, low levels of depressive symptoms, and low levels of AUD symptoms to be three variants of successful aging.
One unresolved issue for the CEMSA as a theoretical framework is whether or not the model is better suited to explaining subjective aspects of successful aging than it is to explaining more objective aspects of successful aging. Bernhold et al. (2018) found that older adults’ age-related communication was associated with subjective perceptions that life is going well and depressive symptoms, but not associated with the number of standard alcoholic drinks consumed during a typical drinking occasion (a more objective indicator of successful aging). Similarly, Gasiorek and Barile (2018) found that age-related communication was associated with the number of mentally unhealthy days, but not the number of physically unhealthy days, that people experienced during the past month. Thus, one primary aim of the present study is to further probe the CEMSA’s boundary conditions by examining whether or not the age-related communication of older adults and their romantic partners is associated with more objective aspects of successful aging (in this study, treated as the number of AUD symptoms).
The CEMSA
Fowler and colleagues’ (2015) introduced the original CEMSA to explain how people can shape their experiences of aging through communication, and it was predicated on the assumption that people have some control over the degree to which they age successfully (Schulz & Heckhausen, 1996). In the model, illustrated in Figure 1, uncertainty about the aging process is proposed to influence one’s own age-related communication. In turn, one’s own age-related communication predicts positive affect about aging, negative affect about aging, and aging efficacy. Aging efficacy refers to the extent to which people believe they are capable of aging successfully (Fowler et al., 2015; Welch & West, 1995); in the model, it is posited as the proximate predictor of successful aging.
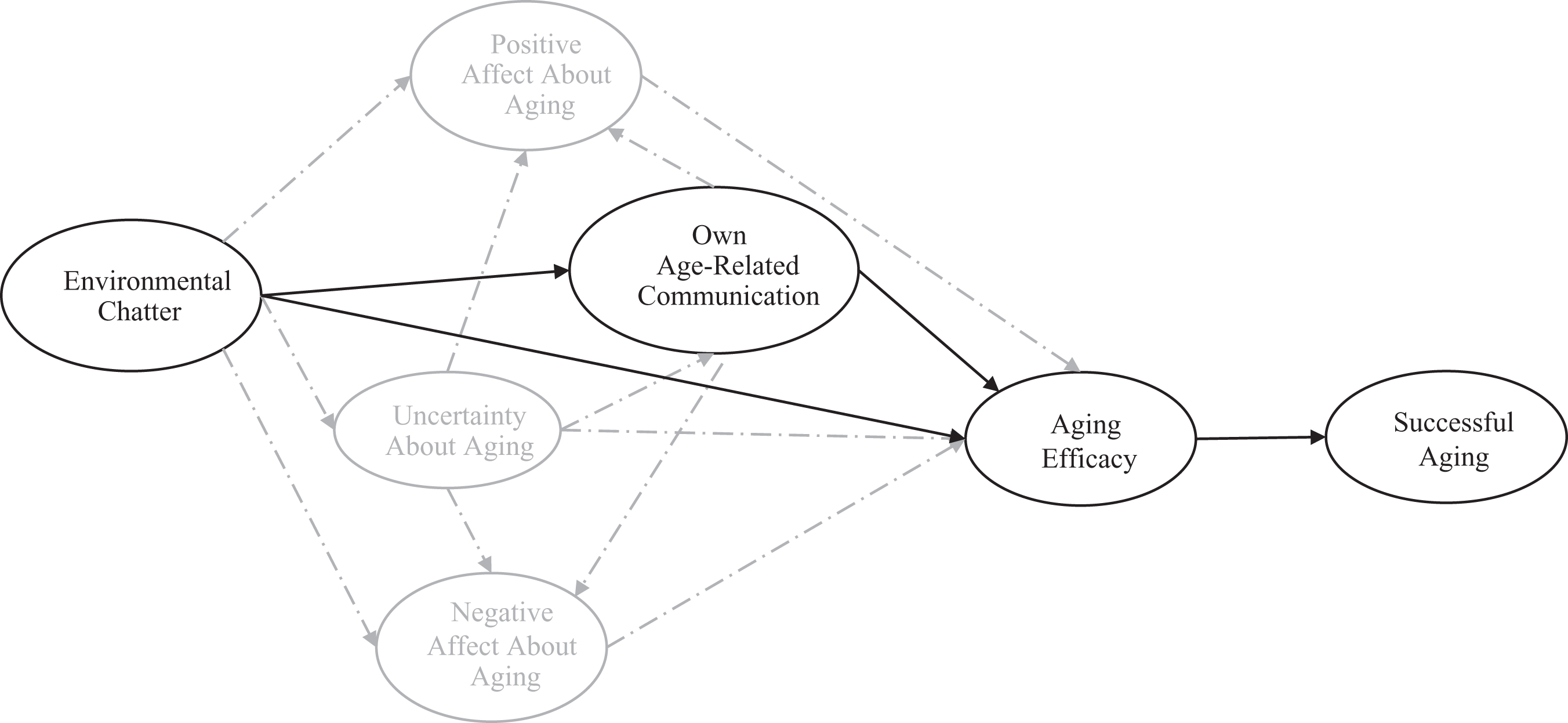
The CEMSA. Note. In this study, we treat environmental chatter as older adults’ perceptions of their romantic partners’ age-related communication. We treat successful aging as global assessments of aging well, depressive symptoms, and AUD symptoms. Model components and interrelationships outlined in solid black lines constitute the main focus of this study. Model components and interrelationships outlined in light gray and dashed lines are not the focus of this study. CEMSA = communicative ecology model of successful aging; AUD = alcohol use disorder.
Together, seven behaviors form the CEMSA’s own age-related communication component (for a more detailed description of each behavior, see Fowler et al., 2015). The first behavior involves invoking one’s age as an excuse for shortcomings, which is thought to be relatively harmful. The second behavior involves expressing optimism about aging, which is thought to be relatively adaptive. The third behavior concerns collusion in teasing others about their age. Over time, the negative stereotypes in age-related jokes (e.g., impotent older men, infirm older people) may be harmful as people assimilate them into their own self-definitions (Levy, 2009). The fourth behavior involves how people manage being the recipient of ageism. Humor may be one particularly effective strategy to combat ageist speech, as can be used to indicate that ageist behavior is problematic while also allowing the older adult to appear good-natured (Ryan, Kennaley, Pratt, & Shumovich, 2000). The fifth behavior involves resisting antiaging messages in the media. Many television commercials and other advertisements promote “antiaging” products by depicting signs of aging as undesirable (Coupland, 2009). If accepted, these messages may be detrimental to people’s ability to age successfully. The sixth behavior is discussing future caregiving preferences with relational partners, which may provide older adults with a sense of control. The seventh behavior concerns engaging with new communication technologies. Older adults have reported new technologies (e.g., social media) as empowering when they use them to connect with loved ones (Hill, Betts, & Gardner, 2015).
Across studies, these seven behaviors have formed distinct profiles, or subgroups defined by how adults communicate about aging (e.g., Gasiorek, Fowler, & Giles, 2015). Engaged agers are characterized by relatively low levels of age-related excuses, teasing others about age, and playing along when others tease them about their age, as well as relatively high levels of expressed optimism about the aging process, skepticism of antiaging messages in the media, discussion of future caregiving preferences, and use of new communication technologies. Bantering agers are relatively high on almost all behaviors (i.e., self-categorizing as old, expressing optimism, teasing others about age, playing along with age-related teasing, resisting antiaging messages in the media, and embracing new communication technologies). However, they discuss their caregiving preferences somewhat less frequently than engaged agers. Finally, disengaged agers score relatively low on almost all behaviors (i.e., self-categorizing as old, expressing optimism, teasing others about age, playing along with age-related teasing, resisting antiaging media messages, and discussing caregiving preferences), but their use of new communication technologies parallels that of the other two subgroups. Given the consistency with which these subgroups have emerged in past research, we predicted the following:
This study also investigated whether or not participants’ reports of their romantic partners’ age-related communication make an independent contribution to explaining participants’ successful aging, above and beyond participants’ reports of their own age-related communication. Given their consistency in past research, it seems likely that the three profiles could be replicated when considering older adults’ perceptions of their romantic partners’ age-related communication:
Although these three types of agers have consistently emerged in past research, Bernhold et al. (2018) also identified a fourth subgroup, which they labeled gloomy agers. Gloomy agers reported relatively high levels of age-related excuses, but relatively low levels of all the other communication behaviors (especially with respect to expressing optimism about the aging process and keeping up with new communication technologies). The researchers argued that gloomy agers resembled a “worst-of-all-worlds” approach to aging in almost all respects. Because gloomy agers have only surfaced in one previous study, we asked the following:
As noted in Figure 1, the CEMSA also theorizes that messages about aging in one’s social environment (i.e., “environmental chatter”)—such as communication from relational partners—will predict older adults’ own age-related communication. Several perspectives suggest that people are likely to develop communication patterns that resemble those of their relational partners. Communication accommodation theory (CAT; e.g., Giles, 2016), for example, proposes that speakers converge, or become more communicatively similar, to their interaction partners, the more that speakers want to decrease social distance (Dragojevic, Gasiorek, & Giles, 2016). Across studies, convergence and other types of accommodation have been positively associated with relational solidarity and favorable evaluations of the interaction partner (Soliz & Bergquist, 2016). As such, older adults seem likely to develop communication patterns about aging that are similar to their romantic partners’, especially if older adults enjoy high-solidarity romantic relationships and think highly of their romantic partners.
Work on communicative mimicry would also suggest that people are likely to unconsciously mirror their relational partners’ communication patterns (Chartrand & Bargh, 1999). Unlike CAT, however, the mimicry tradition suggests that the imitating of relational partners is a natural human tendency that does not necessarily rely on interactional goals such as decreasing social distance. From this perspective, people are likely to imitate relational partners regardless of liking, suggesting that older adults’ age-related communication may resemble their romantic partners’ even if older adults are not in especially close and satisfying relationships. In short, research on convergence and mimicry would both suggest that older adults’ age-related communication may be patterned in such a way that it resembles the age-related communication of their romantic partners:
According to the CEMSA (see Figure 1), older adults’ own age-related communication should be indirectly associated with their own successful aging, via their aging efficacy. In previous studies, engaged agers have reported greater aging efficacy and successful aging (operationalized as global assessments that one is aging well) compared to bantering and disengaged agers (Gasiorek et al., 2015). Bantering agers have reported greater aging efficacy and satisfaction with life than disengaged agers (Gasiorek & Barile, 2018; Gasiorek & Fowler, 2016). Recent CEMSA research also found that, relative to an engaged profile, a disengaged profile was associated with lower levels of aging efficacy, which in turn predicted more self-reported depressive symptoms and less agreement that one is aging well (Bernhold et al., 2018).
Older adults’ aging efficacy may, in part, be cultivated through their own patterns of communication. Gilleard and Higgs (2010) argued that people do not understand old age through an objective list of changes that accompany this phase of the life span, but rather through the discourses about aging that they communicatively construct and toward which they orient themselves. Put differently, the idea of aging takes on systems of meaning based on the ways in which people talk about growing older (Gilleard & Higgs, 2000). Maladaptive patterns of own age-related discourse have been proposed to exacerbate any preexisting fears that one is experiencing age-related declines (e.g., fears of losing one’s memory). These maladaptive patterns of talk and the accompanying fears they foster have been proposed to then erode aging efficacy (Welch & West, 1995).
In turn, lower aging efficacy may predict lower global assessments of aging well, more depressive symptoms, and more AUD symptoms. Previous research has shown a lack of efficacy to be one mediating variable that translates various burdens (e.g., financial strain) into maladaptive outcomes, such as depressive symptoms (Chou & Chi, 2001). Feeling in control of one’s own aging is thought to be an empowering experience (Giles, Davis, Gasiorek, & Giles, 2013). When people feel unable to control their aging process, they may feel disempowered and, hence, dissatisfied with life and depressed; they may also turn to alcohol to help them cope with their feelings of disempowerment and perceived inability to handle life (Grembowski et al., 1993; Vahia et al., 2010). We posit the three variants of successful aging to be parallel outcomes with one another, as opposed to certain variants of successful aging predicting other variants of successful aging. Consistent with this positioning, Jeste, Depp, and Vahia (2010, p. 82) argued that there is “remarkable convergence” in the factors and pathways predicting various subjective and objective indicators of successful aging. They also noted that depression often co-occurs with a negative subjective outlook on one’s life and poor dietary habits (see also Briggs, Magnus, Lassiter, Patterson, & Smith, 2011; Moore et al., 2013). Taken in its entirety, it thus seems reasonable that one’s own age-related communication would predict aging efficacy, and aging efficacy would then predict the three variants of successful aging:
The indirect associations in H4 speak to Fowler and colleagues’ (2015) assertion that people can have considerable agency over their own successful aging. Another relevant consideration is the degree to which people’s successful aging may partly be the product of their social environments. Hendricks and Hatch (2009), for example, noted that social arrangements structure the life course in such a way that some people are placed on a trajectory toward more (or less) favorable experiences during older adulthood. From this perspective, successful aging must also be considered as the product of factors beyond personal choice (Katz & Calasanti, 2015). Although Gilleard and Higgs (2000) argued that people’s own discourses shape their meanings about aging, they also acknowledged that discourses from relational partners partly shape how confident people feel in their ability to age well. Relational partners might construct maladaptive discourses by relying on stereotypes about what it means to age (e.g., aging involves cognitive decline and senility), and these discourses from relational partners have been proposed to erode older adults’ agency and sense of control about their own aging process (Welch & West, 1995). More broadly, Holtzman et al. (2004) proposed that older adults’ engagements with social network members present opportunities to strengthen or erode older adults’ efficacy in various life domains, such as their efficacy to lead a fulfilling life.
In Figure 1, social circumstances in the CEMSA are represented by “environmental chatter” (Gasiorek et al., 2016). Environmental chatter refers to the direct and indirect messages about aging people observe in their surroundings that may also shape how successfully they age. Gasiorek et al. (2016, p. 39) referred to this chatter as the “background noise” about aging that may not be always processed thoughtfully or critically, but can contribute to people’s notions of what it means to grow older. Numerous forms of communication may qualify as environmental chatter, including memorable messages people hear about aging, how role models (e.g., parents, grandparents) communicate about aging, and the extent to which relational partners do or do not accommodate. In this study, we focus on one form environmental chatter may take: the way that older adults’ romantic partners communicate about age-related issues.
Several lines of theory and research suggest that the age-related communication of older adults’ romantic partners should contribute to older adults’ successful aging. Family systems theory holds that family members are interdependent, such that the actions of each family member affect other family members (Yoshimura & Galvin, 2018). From this perspective, people who are disengaged or gloomy in their age-related communication may also “drag down” their romantic partners. Relatedly, work on stress contagion in families has found that people’s ill feelings and unmanaged stress can spill over into the well-being of other family members (Nelson, O’Brien, Blankson, Calkins, & Keane, 2009; Waters, West, & Mendes, 2014). When their romantic partners communicate about aging in relatively maladaptive ways (e.g., teasing, sounding gloomy about the aging process), older adults may feel less confident in their own ability to age well. This lowered aging efficacy may than predict older adults’ weaker agreement with the notion that they are aging well, more depressive symptoms, and more AUD symptoms. In their entirety, these perspectives imply that the age-related communication of romantic partners is likely to predict older adults’ aging efficacy and, in turn, successful aging:
Method
Participants and procedures
A total of 233 adults aged 55 and older were recruited on Amazon’s MTurk to complete a survey about how they and their romantic partner communicate about age-related issues. We paid an additional fee on MTurk to stipulate a qualification that our study only be visible to potential participants who were at least 55 years old, rather than being visible to the entire pool of MTurk workers. To be eligible for this study, participants had to currently have a romantic partner (i.e., spouse, fiancé[e], or dating partner). The recruitment description potential participants read on MTurk before enrolling in the study noted this eligibility requirement. Participants were male (42.5%) and female (56.7%), with 0.9% of participants not specifying their sex. On average, participants were 63.27 years old (SD = 4.73 years). The majority of participants were European American (84.5%). Participants rated their socioeconomic status (SES) as lower class (20.6%), middle class (76.8%), and upper class (2.1%), with 0.4% of participants not providing this information. The annual income of participants’ households was measured in US$10,000 increments, with a median income between US$40,000 and US$49,999. All participants were compensated US$1.00 for taking the survey. This is the first study from this data set.
As romantic partners, participants predominantly reported on spouses currently living in the same household as the participants (73.0%). However, some participants reported on their fiancé(e)s (1.3%), dating partners (19.7%), separated spouses living in different households (2.6%), and other types of romantic partners (3.0%), with 0.4% of participants not specifying relationship type. There was also an option at the end of the survey for participants to report that they were not currently in a romantic relationship, but no participant selected that option. Romantic partners were men (54.9%) and women (44.2%), with 0.9% of participants not reporting this. On average, romantic partners were 61.66 years old (SD = 7.87 years). Ethnicities of romantic partners were similar to those of participants, with the majority of romantic partners being European American (79.4%).
Measures
Online Supplemental Table S1 reports bivariate correlations between all study variables. The Online Appendix also provides a full list of items for the scales described below.
Age-related communication
Twenty-one items from Fowler et al. (2015) operationalized participants’ own age-related communication. All items were answered on a Likert-type format ranging from 1 (strongly disagree) to 7 (strongly agree). The items pertained to age-related excuses to account for one’s shortcomings (e.g., “When I forget something or have trouble with a task, I often say it is because of my age”), expressed optimism about the aging process (e.g., “I frequently express the fact that I am optimistic about aging”), collusion in the teasing of others about their age (e.g., “When I send birthday cards or messages, I often poke fun at the person’s age”), management of ageism (e.g., “When others make jokes about my age, I usually play along”), resistance to antiaging messages in the media (e.g., “I resent the ads that claim I should work at looking younger”), discussion of future caregiving preferences (e.g., “I have tried to make sure my family is informed of my preferences if they ever need to make health decisions for me”), and use of new communication technologies (e.g., “I enjoy keeping up with new communication technologies such as social media or smart phone apps”). Consistent with past CEMSA research (e.g., Bernhold et al., 2018; Gasiorek et al., 2015), we did not compute reliability coefficients for these items because latent profile analysis treats each individual age-related communication item as an independent contributor to profile membership.
The same 21 items also assessed participants’ perceptions of their romantic partner’s age-related communication. Slight adjustments were made to the item wording when assessing the romantic partner’s communication (e.g., “When my spouse or dating partner forgets something or has trouble with a task, he/she often says it is because of his/her age”). Participants were instructed to answer these 21 items while thinking about their general observations of how their romantic partner communicates. These items were also answered on a Likert-type format ranging from 1 (strongly disagree) to 7 (strongly agree).
Aging efficacy
Six items from Gasiorek et al. (2015) measured aging efficacy (e.g., “I feel able to cope with things that might happen to me as I age”). All items were answered on a Likert-type format ranging from 1 (strongly disagree) to 7 (strongly agree). Responses to the items were averaged, with higher scores indicating greater efficacy (M = 4.93, SD = 1.10, α = .87).
Global assessments of aging well
Six items from Gasiorek et al. (2015) gauged the extent to which participants felt they were aging well (e.g., “How well are you aging?” and “I am happy with the age I am right now”). Three items used semantic-differential formats (e.g., 1 = not at all well, 7 = extremely well); the remaining 3 items used Likert-type formats (i.e., 1 = strongly disagree, 7 = strongly agree). Responses on the 6 items were averaged, with higher scores indicating stronger perceptions of aging well (M = 5.18, SD = 1.23, α = .90).
Depressive symptoms
Six items from the Center for Epidemiologic Studies Depression Scale (Radloff, 1977) measured self-reported depressive symptoms (e.g., “I felt like I could not stop feeling sad even with help from family or friends”). The items contained four response options ranging from rarely or none of the time (less than 1 day in the past week) to most or all of the time (5–7 days in the past week). Responses on the items were averaged, with higher scores indicating more depressive symptoms (M = 1.48, SD = 0.55, α = .82).
AUD symptoms
The Diagnostic and Statistical Manual of Mental Disorders (see National Institute on Alcohol Abuse and Alcoholism, 2016) assessed the extent to which participants reported symptoms of AUD. The scale consists of 11 items asking participants to reflect on their alcohol-related thoughts and behaviors over the past year (e.g., “In the past year, have you had times when you ended up drinking more, or longer, than you intended?”). Responses to the 11 items were summed, with higher scores indicating a greater number of AUD symptoms. After excluding participants who reported that they never consumed alcohol (n = 63), the remaining 170 participants reported an average of 0.48 symptoms of AUD (SD = 1.34).
Results
Profiles of communication about aging
Latent profile analysis (LPA) with Mplus 7.2 (Muthén & Muthén, 1998–2014) was used to identify profiles of communication about aging by participants (H1 and RQ1) and their romantic partners (H2 and RQ1). In this study, the indicator variables were the 21 items measuring different forms of communication about aging. We conducted two sets of LPAs: one for participants’ own communication and one for their romantic partners’ communication (as reported by participants). A series of models was run for each analysis; each model had one more latent profile than the previous model, until models became unstable or resultant profiles were small or nonsensical. To select the best model for each set of indicators, we used the Bayesian information criterion (BIC) and sample size-adjusted BIC in conjunction with substantive interpretations of the resulting profiles (Morgan, 2015). Fit statistics for these models, for each set of indicators, are available in Online Supplemental Table S2.
For participants’ own communication (H1), a three-profile solution was determined to be the most appropriate. The structure of the three profiles closely resembled those found in previous research, supporting H1. A disengaged profile (30.5%) was characterized by relatively low levels of talking about age; an engaged profile (42.5%) was characterized by relatively low self-categorization and teasing about age, but higher levels of optimism and talk about future care wishes; and a bantering profile (27.0%) was characterized by high levels of self-categorization, optimism, and teasing, but only moderate levels of talk about future care wishes. A profile plot for the own age-related communication profiles is presented in Figure 2.
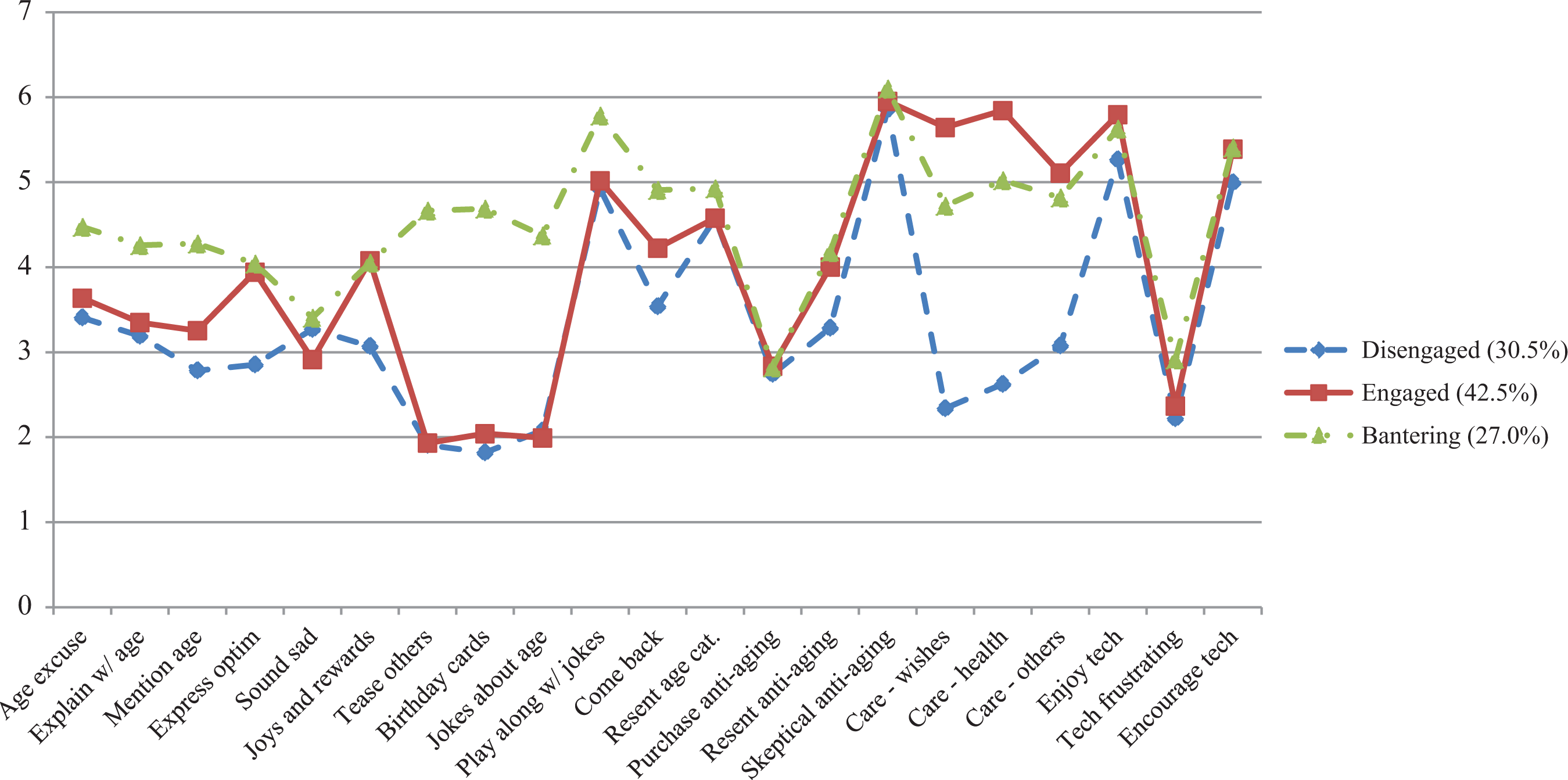
Profiles of participants’ own communication about aging.
For romantic partners’ communication (H2), a four-profile solution was determined to be the most appropriate. Partially supporting H2, two of the four profiles resembled those found in past research (and in participants’ own self-reported communication): an engaged profile (38.3%) and a disengaged profile (22.2%). A third profile, which was characterized by high levels of self-categorization, optimism, teasing, and talk about future care wishes, generally resembled the bantering profile found in participants’ own communication, although endorsement of care-related talk was markedly higher. We labeled this profile bantering–high health (23.0%). The fourth profile was similar to the gloomy profile identified by Bernhold et al. (2018): it was characterized by high levels of self-categorization, low levels of expressed optimism, teasing, and talk about future care, and moderate-to-low levels of engagement with technology. Accordingly, we also labeled this profile gloomy (16.5%; RQ1). A profile plot for these communication profiles is presented in Figure 3.
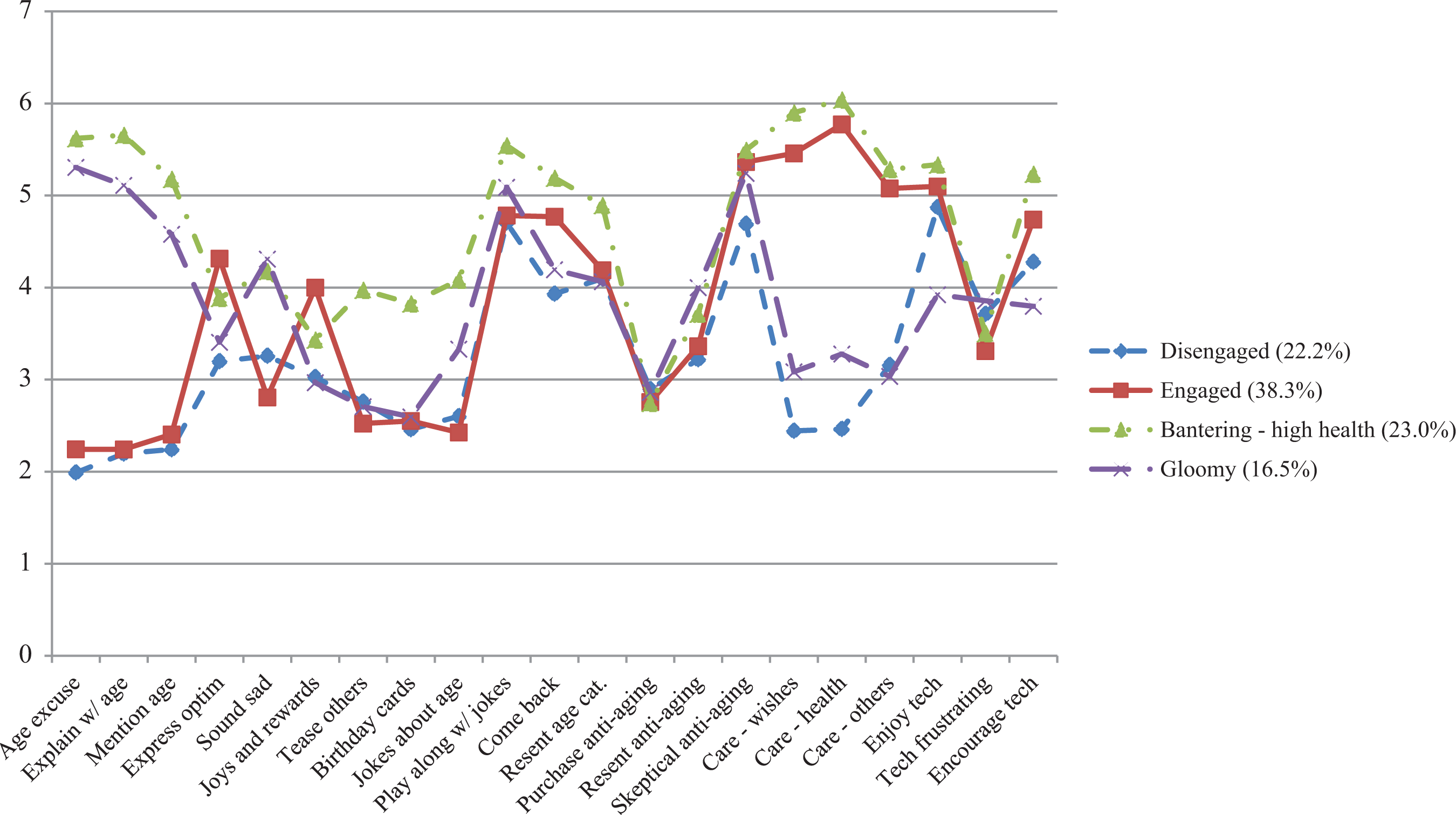
Profiles of romantic partners’ communication about aging.
Combinations of profiles in couples
To determine how people’s own communication profile related to their romantic partners’ profile (H3), we conducted a latent transition analysis (LTA). An LTA model provides estimates of the probability of experiencing different combinations of profiles across two or more sets of profiles in a data set. Although this analytic technique is typically used to examine stability and change in individuals’ profile membership across time, it can also be used to examine the relationships between sets of profiles associated with individuals in cross-sectional data (e.g., the probability of a participant being engaged, and also having an engaged partner; or of a participant being engaged, and having a disengaged partner, etc.). These probabilities of different profile combinations are displayed in a matrix in which the sum of the probabilities for each row is always 1.00. The resulting matrix for our analyses is presented in Table 1.
Latent transition matrix for the romantic partner’s communication profile predicting the participant’s own communication profile.

Our results suggest that people are most likely to have a romantic partner who shares their communicative profile (or a similar profile), supporting H3: of those with disengaged romantic partners, 75.3% were also members of the disengaged profile themselves. Of those with engaged romantic partners, 56.4% were also classified as engaged (while 26.2% were classified as disengaged, and 17.4% as bantering). Of those with bantering–high health partners, 56.7% were (also) classified as bantering, while 33.6% were classified as engaged. Finally, of those with gloomy romantic partners, 50.3% were classified as disengaged (the profile that most closely resembles a gloomy profile, of the three identified for people’s own communication), 28.8% were classified as bantering, and 20.9% were classified as engaged.
Communication as a predictor of successful aging
H4 and H5 predicted that older adults’ own communication and their romantic partners’ communication (respectively) would indirectly predict the extent to which older adults were aging successfully, via aging efficacy. To test these predictions, path modeling was employed. Participants’ own communication and their romantic partners’ communication were operationalized as their most likely profile membership (MLPM) for each set of profiles. MLPM for own and romantic partners’ communication was positioned as predictors of efficacy about aging, which in turn predicted the three variants of successful aging. Engaged agers served as the reference profile for both participants’ and romantic partners’ age-related communication. Romantic partners’ sex, age, marital status, relationship length, and relational closeness (all variables as reported by participants) were positioned as covariates of romantic partners’ communication profiles. Participants’ sex, age, SES, and household income, as well as marital status, relationship length, and relational closeness with their romantic partner, were positioned as covariates of participants’ own communication profiles, efficacy, and the three variants of successful aging. Additionally, the error terms for all communication profiles (romantic partners’ and participants’ own) were intercorrelated.
Because not all participants consumed alcohol, two separate models were run: one with all participants (n = 233), with global assessments of aging well and depressive symptoms as outcomes; and one with only participants who reported drinking alcohol (n = 170), with AUD symptoms as the outcome. The decision to run two separate models was consistent with analytical procedures in Bernhold et al. (2018). Moreover, including only the subset of participants who reported consuming alcohol in the model predicting AUD symptoms allowed for a closer examination of how age-related communication indirectly predicts AUD symptoms among people for whom alcohol consumption is relevant to their lives. An independent samples t-test was conducted to check whether or not participants who reported consuming alcohol differed from those who reported consuming no alcohol on non-AUD outcomes of interest (i.e., efficacy, global assessments of aging well, and depressive symptoms). No significant differences were found; all | t |’s < 1.85, p’s > .07. The distribution of the AUD symptoms was highly skewed, with most participants reporting no (n = 135) or one (n = 16) symptom(s). Thus, a negative binomial regression was used to model the relationship between efficacy and AUD symptoms.
To test H4 and H5, we examined the indirect effects (calculated by Mplus) from romantic partners’ and participants’ own MLPM to successful aging outcomes for each set of profiles. These indirect effects are presented in Table 2. Coefficients for paths between covariates and other study variables are available in Online Supplemental Table S3.
Indirect effects of communication profiles on perceptions of aging well, depressive symptoms, and AUD symptoms.
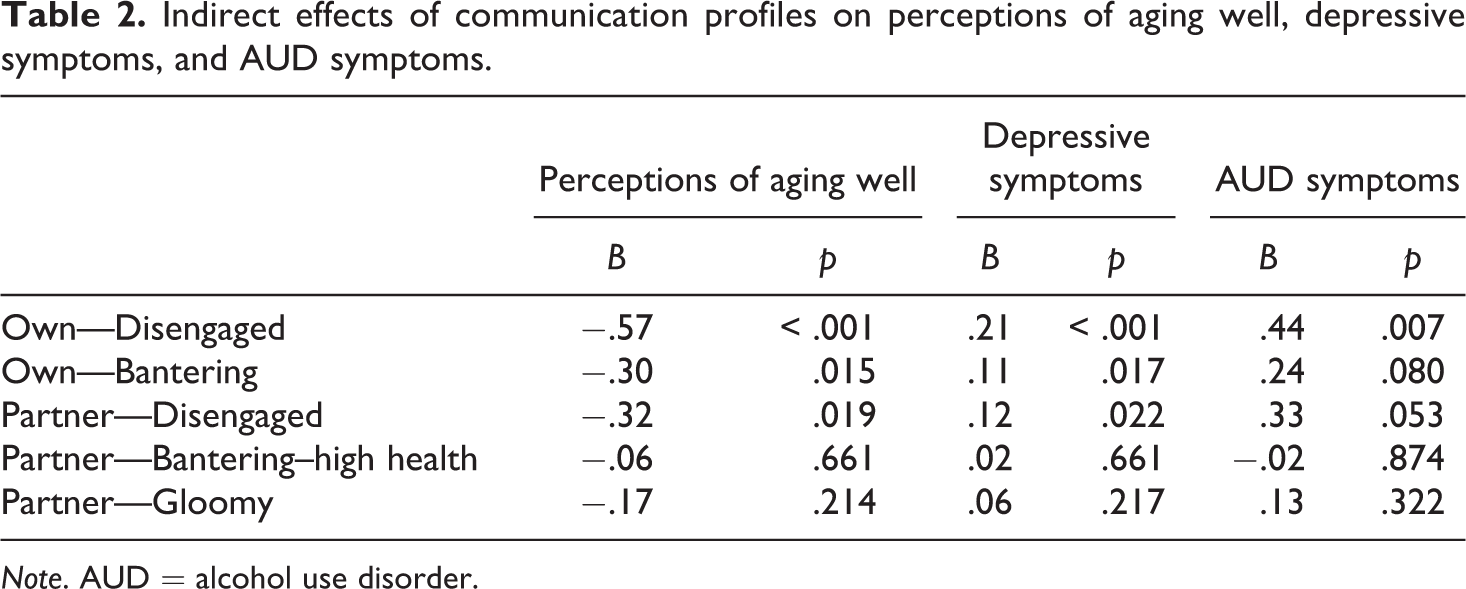
Note. AUD = alcohol use disorder.
Consistent with predictions, older adults’ own age-related communication profile membership was indirectly associated with their experiences of successful aging, via efficacy. Relative to being a member of an engaged profile, being a member of a disengaged profile indirectly predicted lower global assessments of aging well (B = −.57, p < .001), higher reports of depressive symptoms (B = .21, p < .001), and more AUD symptoms (B = .44, p = .007). Additionally, being a member of the bantering profile (relative to an engaged profile) indirectly predicted lower global assessments of aging well (B = −.30, p = .015) and higher reports of depressive symptoms (B = .11, p = .017). Having a romantic partner exhibiting a disengaged profile (relative to an engaged profile) also indirectly predicted lower assessments of aging well (B = −.32, p = .019) and higher reports of depressive symptoms (B = .12, p = .022). No other profiles exhibited indirect associations with successful aging outcomes.
Discussion
This study examined how older adults’ and their romantic partners’ age-related communication indirectly predicts older adults’ global assessments that they are aging well, depressive symptoms, and AUD symptoms, via aging efficacy. Consistent with previous research, participants were classified into engaged, bantering, and disengaged profiles based on their own patterns of age-related communication. The replication of these profiles when examining older adults’ own age-related communication adds additional evidence for their stability across studies.
A novel contribution of this study is its insight into older adults’ observations of their romantic partners’ age-related communication. Older adults’ romantic partners were classified into four profiles: engaged, disengaged, bantering–high health, and gloomy agers. Although the engaged and disengaged romantic partner profiles resembled profiles in previous research, the bantering–high health profile was somewhat new. This profile involved relatively high levels of discussing caregiving preferences, accompanied by higher tendencies to self-categorize as old and tease others about age (as classically characterize a bantering profile). An inspection of covariate paths revealed that romantic partners were more likely to be in the bantering–high health profile when they were (1) older in chronological age and (2) in closer relationships with participants. This profile may be more likely to manifest with increasing age as romantic partners begin to experience new health challenges or begin to more seriously consider their own mortality. It may also be more likely to manifest in closer romantic relationships because they may confer the security and comfort conducive to using humor and discussing caregiving preferences. Future researchers should more fully explore the reasons why romantic partners fall into the bantering–high health profile. Given that preparing for future caregiving needs has been found to be an empowering process (Pinquart & Sorensen, 2002), a bantering–high health profile might not be especially harmful for older adults to observe in their romantic partners.
Somewhat more surprisingly (and in contrast to predictions), the gloomy romantic partner profile was not associated with participants’ perceptions of aging well, depressive symptoms, or AUD symptoms (relative to the engaged romantic partner profile). In previous research (Bernhold et al., 2018), one’s own membership in the gloomy profile was indirectly associated with lower perceptions of aging well, more depressive symptoms, and greater loneliness (relative to one’s own membership in the engaged profile). This suggests that the gloomy profile may operate differently depending on whether or not older adults themselves are gloomy agers, versus whether or not older adults’ romantic partners are gloomy agers. Older adults may be better equipped to ward off any adverse implications of the gloomy profile when they observe relational partners communicating in gloomy ways rather than when they themselves communicate in these ways. Consistent with this speculation, covariate paths showed that participants were more likely to have gloomy partners when they were in more emotionally distant romantic relationships. This suggests that participants in this study might have cultivated resilience to the gloomy communication tendencies of their romantic partners by emotionally distancing themselves from these partners. Participants might also be careful to not let their daily lives become overly intertwined with the lives of their gloomy partners (e.g., by trying to arrange their daily schedules so that they are not constantly around their partners with gloomy communication tendencies). More research is needed to explore why the gloomy profile might not be especially harmful for older adults to observe in romantic partners. Open-ended interviews with older adults who have romantic partners with gloomy age-related communication tendencies might be especially helpful in documenting their experiences cultivating resilience.
Another contribution of this study was its examination how communication profiles of older adults and their romantic partners relate. Consistent with predictions that people would exhibit similar communication patterns to their romantic partner, 56.4% of older adults with engaged romantic partners were engaged agers themselves, 56.7% of older adults with bantering–high health romantic partners were bantering agers themselves, 75.3% of older adults with disengaged romantic partners were disengaged agers themselves, and 50.3% of older adults with gloomy romantic partners were disengaged agers (the disengaged profile is arguably the most similar own aged-related communication profile to the gloomy romantic partner profile). However, the overlap between older adults’ and their romantic partners’ age-related communication was far from perfect. Given that mimicry and convergence have predicted greater perceptions of affection, higher communication quality, and other prosocial outcomes (e.g., Floyd & Ray, 2003), one potentially profitable avenue for future researchers would be to investigate how different combinations of adults’ and their romantic partners’ age-related communication tendencies might be associated with relational outcomes such as (dis)satisfaction or destructive or productive conflict tendencies.
Consistent with predictions, we found older adults’ own age-related communication was indirectly associated with successful aging, via aging efficacy: relative to being an engaged ager, being a disengaged ager indirectly predicted lower global perceptions of aging well, more depressive symptoms, and more AUD symptoms, via lower aging efficacy. Similarly, relative to being an engaged ager, being a bantering ager indirectly predicted lower global perceptions of aging well and more depressive symptoms, via lower aging efficacy. These results suggest that people seem to have some agency over the extent to which they are able to age well, and this agency can be realized through their communication (Fowler et al., 2015).
It was also notable that being a disengaged ager (relative to being an engaged ager) was indirectly associated with more AUD symptoms, via lower aging efficacy. A primary goal of this study was to test the CEMSA’s boundary conditions by examining whether or not age-related communication is associated with more objective aspects of successful aging such as AUD symptoms. The indirect association between being a disengaged ager and AUD symptoms suggests that the CEMSA may indeed be able to explain some objective aspects of successful aging. Given that healthy dieting and exercise are frequently mentioned in lay older adults’ definitions of successful aging (e.g., Jopp et al., 2015), our results suggest the need for future longitudinal research examining how patterns of age-related communication may be related to behaviors such as healthy eating, consuming alcohol in moderation, and exercising regularly.
Finally, we also found that romantic partners’ communication predicted variants of successful aging (over and above the influence of older adults’ own communication). When participants had romantic partners who resembled disengaged agers (relative to having romantic partners who resembled engaged agers), participants reported lower perceptions of aging well and more depressive symptoms, via lowered aging efficacy. This supports the contention that successful aging is also the product of one’s social circumstances (e.g., Hendricks & Hatch, 2009). Moreover, although romantic partners’ age-related communication did not indirectly predict participants’ AUD symptoms, the indirect association for disengaged romantic partners (relative to engaged romantic partners as the reference profile) to AUD symptoms, via lower aging efficacy, approached significance (p = .053). This marginal finding suggests that future researchers should continue exploring how family members’ age-related communication may be associated with older adults’ alcohol-related thoughts and behaviors.
Limitations and additional opportunities for future research
This study contains limitations that also raise opportunities for future research. First, the data were cross-sectional, and, as such, causality cannot be established. The placement of variables in this study aligns with previous CEMSA scholarship (e.g., Bernhold et al., 2018; Fowler et al., 2015); yet bidirectional associations among constructs are possible. Future longitudinal projects will be better equipped to address the temporal order of variable relationships and other criteria related to causality. A second limitation involved the fact that reports of romantic partners’ age-related communication came from the participants rather than from the romantic partners themselves. While this captures participants’ perceptions of their social environment (which are important to understanding their experiences of that environment), it may or may not accurately capture romantic partners’ actual communication patterns. Future researchers are encouraged to study both parties in the romantic relationship, asking both parties to report on their own and their romantic partners’ age-related communication. Additionally, although romantic relationships are an important type of family relationship, much opportunity exists to examine how the CESMA applies to other types of family relationships. This could be done, for example, by studying how grandparents, parents, and grandchildren mutually influence one another’s successful aging through their patterns of communication about age-related issues.
Relatedly, because all the data for this study were self-reported, common method bias cannot be ruled out, and correlations between some constructs may have been larger than what would have been observed in studies with multiple sources of data. However, Conway and Lance (2010) reviewed previous research finding that same-method observed score correlations are fairly accurate representations of true-score correlations. Following their recommendations, we did not impose any statistical corrections on our data to account for common method bias, but future researchers should strive to triangulate self-report measures with other types of data, such as trained coders’ observations of interactions.
Conclusions
This study examined the extent to which older adults’ and their romantic partners’ age-related communication indirectly predicts older adults’ perceptions of aging well, depressive symptoms, and AUD symptoms. The ability of participants’ own age-related communication to indirectly predict AUD symptoms suggests the merit of continued attention to how the CEMSA may be used to explain both subjective and objective aspects of successful aging. The influence of romantic partners’ communication on perceptions of successful aging and depressive symptoms also highlights the importance of accounting for people’s social environments to their experiences of aging well. Future researchers might use the results of this study as a basis for dyadic- and family-level studies on how multiple family members jointly influence each other’s aging trajectories through their patterns of communication.
Supplemental Material
Online_Appendix_supplementary_material - Older adults’ perceptions of their own and their romantic partners’ age-related communication and their associations with aging well, depressive symptoms, and alcohol use disorder symptoms
Online_Appendix_supplementary_material for Older adults’ perceptions of their own and their romantic partners’ age-related communication and their associations with aging well, depressive symptoms, and alcohol use disorder symptoms by Quinten S. Bernhold and Jessica Gasiorek in Journal of Social and Personal Relationships
Supplemental Material
Supplemental Material, Table_S1 - Older adults’ perceptions of their own and their romantic partners’ age-related communication and their associations with aging well, depressive symptoms, and alcohol use disorder symptoms
Supplemental Material, Table_S1 for Older adults’ perceptions of their own and their romantic partners’ age-related communication and their associations with aging well, depressive symptoms, and alcohol use disorder symptoms by Quinten S. Bernhold and Jessica Gasiorek in Journal of Social and Personal Relationships
Footnotes
Authors’ note
A version of this article was presented at the 105 Annual Convention of the National Communication Association in Baltimore, MD, USA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing:
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.