
Abstract
We examined whether romantic relationship involvement, a well-established protective factor against mental health problems among heterosexual adults, is also protective for sexual and gender minority emerging adults assigned female at birth (SGM-AFAB), a group at high risk for mental health issues. Using cross-sectional data from a community sample of 222 SGM-AFAB ages 18–20 years, we assessed associations between current relationship involvement and five mental health variables: depressive symptoms, anxiety symptoms, alcohol use problems, cannabis use problems, and illicit drug use. There were no differences by romantic involvement in problematic cannabis use or other illicit drug use. Overall, participants in a relationship reported fewer depressive symptoms, fewer anxiety symptoms, and less problematic alcohol use than participants who were single. Some associations differed, however, by participant gender identity, sexual orientation identity, and partner gender. Specifically, relationship involvement was associated with fewer depressive and anxiety symptoms for cisgender female participants (n = 154) but not for gender minority participants (n = 68) and for lesbian participants (n = 38) but not for bisexual/pansexual participants (n = 134) or those with other sexual orientation identities (n = 50). Participants romantically involved with a cisgender female partner (n = 43) had fewer depressive and anxiety symptoms than single participants (n = 100), those with a cisgender male partner (n = 56), and those with a gender minority partner (n = 23). Together, these findings suggest that romantic involvement may promote mental health for many, but not all, SGM young adults, highlighting the importance of attending to differences among SGM subgroups in research and efforts to reduce mental health and substance use disparities.
Keywords
Likely driven by societal stigma against nonheterosexual and transgender identities (Meyer, 2003), sexual and gender minority (SGM) individuals experience disproportionately high rates of mental health problems, including depression, anxiety, and substance use disorders (Institute of Medicine, 2011). Although these disparities are present across the life span, they are particularly striking during emerging adulthood (Austin & Bozick, 2012; Schuler et al., 2018), a developmental era roughly corresponding to ages 18–25 years (Arnett, 2005) when depression, anxiety, and substance use are highly prevalent (SAMHSA, 2012). Compared to their heterosexual counterparts, SGM emerging adults have higher rates of depression and anxiety (Lytle et al., 2014; Marshal et al., 2013; Needham, 2012; Oswalt & Lederer, 2017) and more problematic use of alcohol, marijuana, and other illegal drugs (Austin & Bozick, 2012; Needham, 2012; Talley et al., 2010). Disparities in depression and substance use are largest for SGM young adults assigned female at birth (AFAB; Marshal et al., 2008, 2013; Schuler et al., 2018), who appear to be at particular risk for poor mental health outcomes, even compared to SGM assigned male at birth (AMAB; Meyer, 2003).
To address these mental health disparities, it is important to identify factors that may protect SGM-AFAB emerging adults from anxiety, depression, and substance use. Involvement in a committed romantic partnership is one well-established protective factor for mental health and substance use among heterosexual adults (e.g., Kamp Dush & Amato, 2005; Vanassche et al., 2013). However, it is not clear whether SGM-AFAB, particularly those who are emerging adults, also experience mental health benefits from their romantic relationships. In the current study, we assessed whether current romantic involvement was associated with depressive symptoms, anxiety symptoms, problematic alcohol and cannabis use, and use of other illicit drugs among 18- to 20-year-old SGM-AFAB emerging adults. Further, we assessed whether these associations differed by gender identity (cisgender female vs. gender minority), sexual orientation identity (lesbian vs. bisexual/pansexual vs. others), race, or partner gender.
Romantic involvement and mental health in adults
Involvement in a committed relationship is theorized to benefit mental health in several ways. According to social control theories, spouses and serious romantic partners monitor one another’s behavior, encouraging healthy behaviors that promote emotional well-being (e.g., sleep, exercise) and discouraging risky behaviors such as heavy drinking and drug use (Umberson, 1987). Romantic involvement may also promote mental health by providing an intimate, emotionally fulfilling, and supportive relationship that satisfies individuals’ needs for social connection (House et al., 1988). Marriage also provides tangible legal and financial benefits, including access to partner income and health insurance benefits, which promote general health and well-being (e.g., Waite & Gallagher, 2000). Consistent with these theories, research on heterosexual adults has long documented the mental health benefits of marriage and other committed relationships. Compared to single adults, those who are married or committed to a romantic partner report better psychological well-being (e.g., Kamp Dush & Amato, 2005; Vanassche et al., 2013). Further, longitudinal studies show that entry into marriage or a committed relationship is followed by reduced depression (Lamb et al., 2003) and alcohol and drug use (Duncan et al., 2006; Staff et al., 2010), suggesting a causal effect of romantic involvement on mental health.
Relationship involvement and mental health among emerging adults
Although historically most theory and research has focused on the benefits of marriage for adult mental health (e.g., Waite & Gallagher, 2000), there is a growing literature exploring potential mental health benefits of involvement in a wider range of romantic relationship types during emerging and young adulthood. Compared to single young women, those in committed dating relationships have reported fewer depressive symptoms (Whitton et al., 2013) and less alcohol consumption (Braithwaite et al., 2010; Whitton et al., 2013) but not less use of illicit drugs (Braithwaite et al., 2010; Simon & Barrett, 2010). Longitudinal research has yielded mixed findings. In some studies, young adult substance use declined upon entry into a dating (Fleming et al., 2010; Furman & Collibee, 2014) or nonmarital cohabiting relationship (Duncan et al., 2006; Staff et al., 2010). However, in other studies, entry into a relationship between ages 18 and 20 was not associated with reduced heavy drinking or marijuana use (Fleming et al., 2010) and romantic involvement predicted subsequent increases in depression in first-year college students (Davila et al., 2004).
These inconsistent findings raise the possibility that romantic involvement does not confer the same mental health benefits during emerging adulthood that it does later in life. There are several theoretical reasons why this might be the case. In contrast to adult spouses, young romantic partners may not monitor or exert social control over each other’s behavior, and the social pressure against engaging in risky behaviors when married may not be present. Young romantic relationships also do not typically provide legal or financial benefits that might ease stress and promote health. Further, during emerging adulthood, when many people pursue academic and occupational goals before settling down (Arnett, 2005), relationships often lack long-term commitment. Because highly committed relationships (e.g., marriage, cohabitation) most strongly promote subjective well-being and discourage risky substance use (Kamp Dush & Amato, 2005), the less committed relationships of emerging adults may not confer strong mental health benefits.
On the other hand, there are reasons to think emerging adults should benefit psychologically from romantic involvement. Developing romantic competence represents a central developmental task of young adulthood (Roisman et al., 2004) and romance may provide an intimate, emotional connection not offered by other social partners. Romantic involvement may also discourage substance use among emerging adults by limiting engagement in the single “hook-up” culture where heavy drinking and drug use are prevalent (e.g., Owen et al., 2010). More research is needed to clarify how romantic involvement is associated with mental health among emerging adults.
Relationship involvement and mental health among sexual and gender minorities
Little is known about the effects of romantic involvement on the mental health and substance use of SGM, particularly emerging adults. The same-sex romantic relationships of adults, overall, are remarkably similar to adult different-sex relationships across multiple dimensions of relationship quality (e.g., Kurdek, 2005) and show similar associations between relationship quality and partners’ depressive symptoms (Whitton & Kuryluk, 2014). Further, sexual minority and heterosexual adults report similar efforts to promote healthy behaviors and discourage heavy substance use in their romantic partners (Reczek & Umberson, 2012). It seems likely, then, that the benefits of romantic involvement to mental health and substance use would generalize to SGM, at least during adulthood. During emerging adulthood, it is possible that SGM may benefit even more than heterosexuals from romantic involvement because a dating partner can provide emotional support that is commonly missing from parents and peers (Ryan et al., 2009; Katz-Wise & Hyde, 2012). Further, affiliation with members of the SGM community can buffer the effects of minority stress on young sexual minority women (Johns et al., 2013). On the other hand, dating a same-sex partner may activate internalized stigma, raise risk for family rejection by revealing same-sex attractions, and lead to experiences of relationship stigma (stigma targeting a couple based on their gender composition), all of which may increase risk for mental health and substance use problems (Newcomb & Mustanski, 2010; Rosenthal et al., 2019; Ryan et al., 2009).
Research on the associations between romantic involvement and mental health among SGM is sparse. In a handful of cross-sectional studies, adult lesbians in a committed relationship reported fewer depressive symptoms (Ayala & Coleman, 2000; Kornblith et al., 2016; Oetjen & Rothblum, 2000) and better psychological well-being (Wayment & Peplau, 1995) than those who were single. Among sexual minority men, romantic involvement has been linked with lower depressive symptoms and less use of some illicit drugs (Parsons et al., 2013; Starks et al., 2019). However, romantically involved sexual minority men did not use less marijuana or alcohol than single men (Starks et al., 2019). Further, another study found that romantic involvement was not associated with rates of anxiety or depressive disorders among gay and lesbian adults and was associated with higher odds of anxiety disorders among bisexual adults (Feinstein et al., 2016).
Studies on younger SGM are even more rare and have yielded inconsistent findings. Two found no consistent differences in psychological well-being between single and romantically partnered male and female SGM youth ages 16–24 years (Baams et al., 2014) and ages 15–19 years (Bauermeister et al., 2010). Another found that involvement in a dating or cohabiting relationship was not associated with lower rates of marijuana or hard drug use in lesbian and gay 18–26 year olds (Austin & Bozick, 2012). In contrast, a longitudinal study of SGM-AFAB and SGM-AMAB youth (spanning ages 16–26) indicated that SGM youth reported less psychological distress, alcohol consumption, and use of illicit drugs other than marijuana when they were romantically partnered than when they were single (Whitton et al., 2018a, 2018b). However, the effects of romantic involvement were more positive for Black versus White youth, and bisexual youth reported more psychological distress and marijuana use when in a relationship than when single. Clearly, more research is needed, with consideration of potential differences between subgroups of sexual minority emerging adults.
Moderators of associations between relationship involvement and mental health
Although often treated as a homogenous group, SGM young people are diverse along many dimensions, including gender identity, sexual identity (i.e., self-identified sexual orientation), and race. Further, they form romantic relationships with a variety of partners, including cisgender men and women (whose gender identity and sex assigned at birth match; e.g., James et al., 2016) and gender minority individuals (i.e., those who identify as transgender, genderqueer, nonbinary, etc.). Understanding how relationship involvement may affect mental health among young SGM requires attention to potential differences along these demographic lines.
First, we must consider the increasing number of young people who identify as transgender (e.g., are AFAB and identify as men; Flores et al., 2016) or nonbinary (e.g., gender nonconforming, genderqueer; Richards et al., 2016). These individuals, collectively labeled gender minorities, experience troublingly high rates of discrimination and violence (e.g., James et al., 2016). Romantic involvement may particularly benefit gender minority young adults by buffering them from the negative mental health effects of these experiences. Alternately, many partnered gender minorities encounter stigma against their romantic relationships, which is associated with depression (e.g., Gamarel et al., 2014) and substance use (Reisner et al., 2014), suggesting potential negative effects of involvement on mental health.
Specific sexual orientation identities may also influence how romantic involvement affects mental health and substance use. Whereas gay and lesbian people generally appear to benefit from relationships, romantic involvement has been associated with greater risk for anxiety disorders (Feinstein et al., 2016), more psychological distress (Whitton et al., 2018b), and more use of marijuana and other illicit drugs (Whitton et al., 2018a) among bisexuals. These differences may be attributable to unique stressors bisexuals face when involved in romantic relationships, including invalidation of their bisexual identity by others who assume they are lesbian/gay or heterosexual based on their current partner’s gender (Dyar et al., 2014) and pressure from non-bisexual partners to change their sexual identity (Bostwick & Hequembourg, 2014).
Exploring racial differences in how romantic involvement is associated with SGM mental health is needed as part of broader efforts to understand how co-occurring social identities may intersect to impact health (Institute of Medicine, 2011). Because SGM people of color experience discrimination, microaggressions, and harassment based on both their sexual and racial minority identities (Balsam et al., 2011), they may particularly benefit from the social support of a romantic relationship. Indeed, romantic involvement was associated with less psychological distress for Black and Latinx SGM youth, but not White SGM youth, in one study (Whitton et al., 2018b). However, because most studies have used samples lacking in racial and ethnic diversity, more research is needed.
Finally, though it is often assumed that sexual minorities only have same-sex partners, around one-fourth of sexual minority adolescents and one-fourth of lesbian adults report relationships with different-sex partners (Bauermeister et al., 2010; Diamond & Savin-Williams, 2000). There is some evidence that, for sexual minority adolescents, involvement in same-sex relationships is positively associated with psychological well-being, including lower anxiety and internalized heterosexism and higher self-esteem, but different-sex relationship involvement is not (Bauermeister et al., 2010; Russell & Consolacion, 2003). These initial findings support further investigation of potential differences by partner gender in the effects of relationships on SGM mental health beyond adolescence. Further, we are aware of no studies that have explored the mental health effects of relationships with gender minority partners, though many sexual minority women report sexual or romantic partnerships with them (Mereish et al., 2017).
The current study
The current study aimed to advance our understanding of how relationship involvement is associated with the mental health of SGM-AFAB emerging adults. Using cross-sectional data provided by a community sample of 222 SGM-AFAB aged 18–20 years, we assessed associations between current relationship involvement and five mental health variables: depressive symptoms, anxiety symptoms, alcohol use problems, cannabis use problems, and illicit drug use. Further, we evaluated potential differences in these associations by participant gender identity, sexual orientation identity, race, and gender identity of the romantic partner.
Method
Participants and procedure
Data were drawn from the late adolescent/emerging adult cohort of FAB400 (N = 400; 16–20 years old at baseline), an ongoing longitudinal merged-cohort study of young SGM-AFAB, focused on their health, development, and intimate relationships (Whitton et al., 2019). Inclusion criteria required participants to be AFAB, speak English, and either identify with a sexual or gender minority label, report same-gender attractions, or report same-gender sexual behavior. Consequently, the sample is comprised of sexual minority women, transgender men, and nonbinary AFAB youth. Participants were recruited using various methods including venue-based, online, and peer-incentivized recruitment. Because design effects for each dependent variable, which quantify the extent to which the sampling error deviates from what would be expected if individuals were randomly assigned to clusters, were below the recommended cutoff of 2.0 (Muthén & Satorra, 1995), we did not account for clustering within recruitment chains in the analyses.
The present study uses data from the FAB400 baseline assessment, collected from 2016 to 2017. Participants were paid US$50 for completing a battery of self-report measures using computer-assisted self-interview. The study protocol was approved by the Institutional Review Board at Northwestern University with a waiver of parental permission for participants under 18 years of age under 45 CFR 46, 408(c). We selected participants (N = 242; 60.5%) in the age range of 18–20, given our focus on relationship involvement during emerging adulthood. We then excluded six participants who reported current involvement in more than one romantic relationship and one randomly selected partner from each of the 14 couples who reported on the same relationship to retain independence of data. This yielded an analytic sample of 222 emerging adult SGM-AFAB; demographic characteristics are presented in Table 1.
Demographic characteristics of analytic sample (N = 222).

Note. Proportions with different superscripts differ from each other at p < .05.
Measures
Relationship involvement
Participants were asked to report on up to three sexual and/or romantic partnerships occurring in the last 6 months. If the participant reported any type of romantic partnership that was ongoing at the time of the interview (from casually dating to married), they were coded as romantically involved; otherwise, they were coded as single.
Depressive and anxiety symptoms
The Patient-Reported Outcomes Measurement Information System Depression Short Form 8b and Anxiety Short Form 8a (Pilkonis et al., 2011) were used to assess depressive and anxious symptoms in the past 7 days. Participants rated how frequently they experienced each of eight depressed feelings (e.g., unhappiness, helplessness) and eight anxious feelings (e.g., unease) on a 5-point scale (1 = never to 5 = always). Scores were calculated by summing the 8 items (α = .93 for depression, α = .93 for anxiety).
Problematic alcohol use
The Alcohol Use Disorders Identification Test (Babor et al., 2001) measures the frequency and quantity of alcohol consumption and problems associated with alcohol use (e.g., How often during the past 6 months have you had a feeling of guilt or remorse after drinking?) in the previous 6 months. Scores represent the sum of all 10 items (possible range = 0–40; α = .83); higher scores indicate more alcohol use problems.
Problematic cannabis use
The Cannabis Use Disorders Identification Test–Revised (Adamson et al., 2010) measures marijuana use and problems associated with use in the past 6 months. Scores represent the sum of the 8 items (possible range = 0–32; α = .80); higher scores indicate more cannabis use problems.
Other illicit drug use
To assess other illicit drug use, all participants were asked whether they had used any of the following nonprescription drugs in the past 6 months: cocaine or crack, heroin, methamphetamines, GHB, ketamine, poppers, inhalants, hallucinogens, or ecstasy. Due to low counts of individual illicit drug use, a dichotomous variable was created indicating the presence or absence of illicit drug use.
Potential moderators
Gender identity
Participants responded to the question, What is your current gender identity? with the following options: male, female, transgender, gender nonconforming, genderqueer, nonbinary, and not listed (please specify). Responses were used to assign participants to one of two groups: cisgender women (self-identified as female) and gender minorities (participants who identified with any other gender identity).
Sexual identity
Participants were asked, Which of the following commonly used terms best describes your sexual orientation? with the options: gay, lesbian, bisexual, queer, unsure/questioning, straight/heterosexual, pansexual, asexual, and not listed (please specify). To provide adequate power for moderation analyses, sexual identity was recoded into three categories: monosexual (gay or lesbian), non-monosexual (bisexual/pansexual), and others.
Race/ethnicity
Participants were asked to select the option(s) that best described their race from the following: American Indian or Alaskan Native, Asian, Black or African American, Native Hawaiian or other Pacific Islander, White, or others (please specify). Participants also indicated whether they identified as Hispanic or Latino/Latina/Latinx, regardless of race. As recommended by the National Institutes of Health (2001), all those who selected a Latinx ethnicity were classified as Latinx regardless of race. All others were classified based on the race they selected: Black, White, or others (including all other racial identities, due to low numbers).
Partner gender
Participants were asked to indicate their partner’s gender identity, with the following options: cisman, ciswoman, transman, transwoman, gender nonconforming, genderqueer, nonbinary, and not listed (please specify). Responses were used to categorize partners’ gender as cisgender male, cisgender female, or gender minority.
Data analytic plan
We first tested for differences in each continuous mental health variable (depressive and anxiety symptoms, problematic alcohol, and marijuana use) by relationship involvement using one-way analyses of covariance (ANCOVAs). For each ANCOVA, we entered a two-level factor for romantic involvement (single vs. involved) and included gender, sexual identity, and race as covariates, given previous evidence that these demographic variables are associated with likelihood of romantic involvement, psychological symptoms, and substance use (Whitton et al., 2018a, 2018b). Because the illicit drug use variable was dichotomous, we entered relationship involvement and the control variables (gender, sexual identity, and race) into a logistic regression model predicting illicit drug use.
We then evaluated potential differences in these associations (i.e., moderating effects) by participant gender identity, sexual identity, and race using a single multivariate regression predicting each mental health variable. Each dependent variable was regressed onto relationship involvement, gender identity (cisgender female vs. gender minority), two dummy-coded variables representing sexual identity (bisexual/pansexual and other sexual identity) with lesbian as the reference group, three dummy-coded variables representing race (Black, Latinx, and other race) with White as the reference group, and six interaction terms multiplying relationship involvement and each of the moderator variables. This strategy allowed us to assess the unique moderating effects of gender identity, sexual identity, and race, controlling for the moderating effects of the others. Models were calculated using PROCESS for SPSS version 23 (Hayes, 2013), which not only provides regression coefficients for each predictor variable but also tests of the highest order unconditional interaction (i.e., tests of whether a categorical variable with more than two levels has a significant moderating effect), simple slopes between relationship involvement and the dependent variable at each level of the categorical moderator, and adjusted means on the dependent variable for single and romantically involved participants at each level of the categorical moderator. We present both simple slopes and these adjusted means to facilitate interpretation of differences in the outcome variables by romantic involvement within each demographic subgroup.
Tests of whether partner gender moderated the association between romantic involvement and psychological functioning required a different approach. Because partner gender was only available for participants who were romantically involved (and missing for the 100 single participants), it could not be included as a predictor for all participants and we could not create a multiplicative interaction term. Therefore, we created a four-level variable to represent both relationship involvement and partner gender (single vs. cisgender female partner vs. cisgender male partner vs. gender minority partner). We ran separate one-way ANCOVAs for each dependent variable using this variable as a four-level factor, controlling for participant gender, sexual identity, and race, to test for differences in the continuous dependent variables between participants who were single, partnered with a male, partnered with a female, or partnered with a gender minority individual. To test for effects of involvement/partner gender on illicit drug use (a categorical outcome), we ran a logistic regression with three dummy-coded predictors (cisgender female partner, cisgender male partner, and gender minority partner) with single as the reference group, controlling for gender, sexual identity, and race.
To interpret the magnitude of observed group differences, effect sizes were estimated using Cohen’s d (
Results
Preliminary analyses
Descriptive analyses indicated that 26 participants (11.7%) were “casually dating” their partner. Because these relationships might function differently from more committed relationships with respect to mental health, we first evaluated whether it was appropriate to include casual daters in the romantically involved group. Differences between casual daters and participants in more committed relationships (“serious dating relationships,” engaged, cohabiting, married, or lifelong committed relationships; n = 96) on all of the continuous dependent variables were assessed using t-tests and differences on the dichotomous illicit drug use variable were assessed using χ2 analysis. None of the dependent variables differed by relationship type (all ps > .05) and effect sizes were quite small (ds ranging from .09 to .28 and ϕ = .15). Therefore, casual daters were included in the romantically involved group.
Next, we assessed for demographic differences between romantically involved and single participants. Age and race did not differ by relationship involvement (ps > .05). There were differences in gender by relationship involvement, χ2(1, N = 222) = 4.65, p = .03; the proportion of cisgender females was higher among romantically involved than single participants (75.4% vs. 62.0%). There were also differences by sexual identity, χ2(2, N = 222) = 19.41, p < .01; the proportion of lesbian participants was equivalent among romantically involved and single participants (18.0% vs. 16.0%), the proportion of bisexual/pansexual participants was higher among those romantically involved than single (70.5% vs. 48.0%), and the proportion with other sexual identities was lower in the romantically involved than the single group (11.5% vs. 36.0%).
Main effects
Table 2 presents the means/proportions for each mental health variable by romantic involvement, adjusted for participant gender, sexual identity, and race, as well as test statistics and effect sizes from the ANCOVAs and logistic regression. These results show that relationship involvement was not associated with problematic marijuana use or illicit drug use. However, participants in a relationship reported fewer depressive symptoms, fewer anxiety symptoms, and less problematic alcohol use than participants who were single (small effects).
Means and proportions of mental health and substance use problems by relationship status.
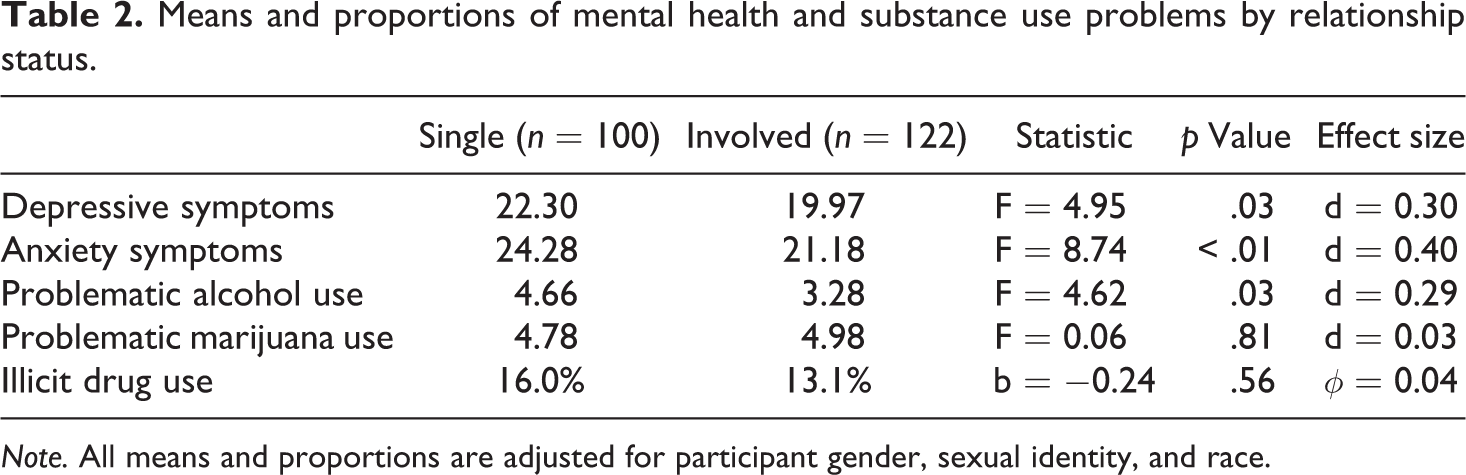
Note. All means and proportions are adjusted for participant gender, sexual identity, and race.
Moderation analyses
Participant gender identity
The interaction between relationship involvement and gender identity was significant only in the prediction of depressive symptoms, F(1,213) = 4.06, p = .045, and anxiety symptoms, F(1,213) = 6.51, p = .01. Simple slopes analysis indicated that cisgender females who were in a relationship reported fewer depressive symptoms (M = 18.42) than cisgender females who were single (M = 22.18), b = −9.43, t = −3.08, p < .01, d = 0.52. Among gender minorities, however, depressive symptoms did not significantly differ between those in a relationship (M = 22.88) and those who were single (M = 21.92), b = −4.84, t = −1.49, p = .14, d = 0.13. Similarly, cisgender females who were in a relationship reported fewer anxiety symptoms (M = 18.50) than single cisgender females (M = 23.51), b = −9.64, t = −3.46, p < .01, d = 0.69. In contrast, anxiety symptoms did not significantly differ between gender minorities who were in a relationship (M = 26.01) versus single (M = 24.68), b = −3.89, t = −1.28, p = .20, d = 0.18. These associations are presented in Figure 1(a) and (b).

Associations between relationship involvement and (a) depressive symptoms and (b) anxiety symptoms by participant gender identity (cisgender female vs. gender minority). Note. **p < .01. All means are adjusted for main and moderating effects of sexual identity and race.
Sexual identity
The interaction between sexual identity and relationship involvement was significant in predicting depressive symptoms, F(2,212) = 3.67, p = .03, and anxiety symptoms, F(2,212) = 3.49, p = .03, but not other outcomes. Simple slopes analysis (shown in Figure 2(a) and (b)) indicated that, among lesbian participants, those in a relationship reported fewer depressive symptoms (M = 16.27) than those who were single (M = 24.66), b = −9.43, t = −3.08, p < .01, d = 1.15. In contrast, depressive symptoms did not differ by romantic involvement among bisexual/pansexual participants (M involved = 19.85; M single = 20.58, b = −1.96, t = −0.90, p = .37, d = 0.10) or among those with other sexual identities (M involved = 21.62; M single = 23.29, b = −4.07, t = −1.29, p = .20, d = 0.23).

Associations between relationship involvement and (a) depressive symptoms and (b) anxiety symptoms by sexual identity (lesbian vs. bisexual/pansexual vs. other sexual identity). Note. **p < .01. All means are adjusted for main and moderating effects of participant gender identity and race.
Results were fairly similar to anxiety symptoms. Among lesbian participants, those in a relationship reported significantly fewer anxiety symptoms (M = 18.55) than those who were single (M = 27.55), b = −10.35, t = −3.40, p < .01, d = 1.24. Among bisexual/pansexual participants, those in a relationship (M = 21.26) reported marginally fewer anxiety symptoms than those who were single (M = 23.67), b = −3.79, t = −1.76, p = .08, d = 0.33. Anxiety symptoms did not differ by romantic involvement for participants with other sexual identities (M involved = 21.43; M single = 21.20), b = −2.32, t = −0.75, p = .46, d = 0.03.
Race
The interaction between relationship involvement and race was not significant in any analysis (all ps > .05), indicating that race did not moderate the association between relationship involvement and any dependent variable.
Partner gender
There were no differences in problematic alcohol use, marijuana use, or illicit drug use by involvement/partner gender (all ps > .05). Depressive symptoms, however, differed by involvement/partner gender, F(3, 212) = 6.11, p < .01 (see Figure 3). Pairwise comparisons using Fisher’s least significant difference test demonstrated that participants with a cisgender female partner (M = 16.96) had fewer depressive symptoms than those with a cisgender male partner (M = 20.85; p = .01; d = 0.51), those with a gender minority partner (M = 23.50; p < .01; d = 0.65), and those who were single (M = 22.36; p < .01; d = 0.45). There were no other group differences in depressive symptoms. Anxiety symptoms also differed by involvement/partner gender, F(3, 212) = 5.67, p < .01. Pairwise comparisons showed that participants with a cisgender female partner (M = 18.73) had fewer anxiety symptoms than those with a cisgender male partner (M = 22.11; p = .02; d = 0.49), a gender minority partner (M = 23.69; p < .01; d = 0.63), and single participants (M = 24.35; p < .01; d = 0.44). In addition, participants with a cisgender male partner had fewer anxiety symptoms than participants who were single (p = .03; d = 0.40). There were no other group differences in anxiety symptoms.

Depressive and anxiety symptoms by involvement with partners of different genders. Note. All means are adjusted for participant gender, sexual identity, and race. Participants with cisgender female partners had fewer depressive and anxiety symptoms than all other groups. Those with cisgender male partners had fewer anxiety symptoms than single participants.
Discussion
In this sample, SGM-AFAB emerging adults currently involved in a romantic relationship reported fewer depressive symptoms, fewer anxiety symptoms, and less problematic alcohol use than those who were single. Together with similar findings for heterosexual emerging adults (e.g., Kamp Dush & Amato, 2005; Simon & Barrett, 2010; Whitton et al., 2013) and SGM late adolescents and young adults (Whitton et al., 2018a, 2018b), these findings suggest that romantic relationships may be a broad protective factor for mental health among young people, whether their identity is heterosexual or nonheterosexual.
Findings were most robust for alcohol consumption; romantic involvement was associated with less problematic drinking for SGM-AFAB participants of all races, gender identities, and sexual identities. Further, the association was consistent across SGM-AFAB’s relationships with cisgender female, cisgender male, and gender minority partners. These results echo previous evidence that SGM adolescents and young adults drink less alcohol at times when they are romantically partnered than at times when they are single and that this is equally true across gay/lesbian and bisexual identities and across cisgender and gender minority identities (Whitton et al., 2018a). It appears that the reductions in heavy drinking associated with marriage in adults do extend to the romantic relationships of SGM emerging adults. Although the mechanisms of effect are unclear, it may be that romantically partnered young SGM-AFAB disengage from the heavy-drinking party scene populated by single adults who are uninterested in relationships or attempting to meet new partners (e.g., Claxton et al., 2015; Owen et al., 2010).
In contrast, the associations of romantic involvement with depressive and anxiety symptoms differed based on gender identity, sexual orientation identity, and partner gender. This suggests that the psychologically protective effects of relationship involvement may only be present for some, but not all, SGM-AFAB emerging adults. Most strikingly, whereas romantic involvement was associated with fewer depressive and anxiety symptoms for cisgender female participants, it was not for gender minority participants. The reduced symptom levels associated with romantic involvement among cisgender women in relationships are consistent with a prior longitudinal study of predominantly cisgender SGM late adolescents and young adults (Whitton et al., 2018b); however, it is unclear why romantic involvement was not similarly associated with less internalizing symptoms among gender minority participants. One possibility is that the stigma against gender minority romantic relationships (e.g., Gamarel et al., 2014) cancels out any positive psychological effects of romantic involvement. If the present findings are replicated, it will be important to explore factors that may interfere with gender minorities benefiting from romantic involvement in the way that heterosexuals (e.g., Kamp Dush & Amato, 2005) and cisgender sexual minorities (e.g., Whitton et al., 2018b) generally do.
Sexual orientation identity also moderated the associations between romantic involvement and psychological symptoms. Specifically, involvement was associated with depressive and anxiety symptoms for lesbian participants only, and not for those with non-monosexual (i.e., bisexual, pansexual) or other sexual orientation identities (including queer, unsure/questioning, and asexual). This finding adds to a growing body of research suggesting that romantic involvement does not have psychological benefits for bisexual individuals (Feinstein et al., 2016; Whitton et al., 2018b), although we did not observe involvement in a relationship to increase bisexual’s anxiety and psychological distress as those studies did. It may be that, for non-monosexuals, any mental health benefits of having a romantic partner are outweighed by stressors inherent in the relationship. Many bisexual women report that when they are romantically involved, their sexual identity is erased by outsiders assuming that they are lesbian or heterosexual based on the gender of their partner (Dyar et al., 2014) and by pressure from their partners to change their sexual identity to match their current relationship (Bostwick & Hequembourg, 2014). Future research is needed to test whether such experiences explain why romantic involvement may not psychologically benefit non-monosexual people and to identify strategies to improve the supportiveness of their relationships.
A novel finding from the present study is that, for SGM-AFAB emerging adults, relationships with cisgender female partners may be particularly beneficial to psychological health. Participants involved with a female partner reported fewer anxiety and depressive symptoms than any other groups, including not only single participants but also those with male or gender minority partners. These results echo findings from studies of sexual minority adolescents indicating that involvement in same-sex relationships, but not different-sex relationships, is positively associated with psychological well-being (Bauermeister et al., 2010; Russell & Consolacion, 2003). Perhaps some young SGM-AFAB date cisgender men in part due to fear of deviating from compulsive heterosexuality norms or a lack of available female partners interested in a same-sex relationship; such relationships may not confer the psychological benefits that a relationship based in sexual attraction and emotional connections would. However, this explanation is not likely for participants who identified as bisexual or pansexual and are likely attracted to men. It is also possible that involvement with a woman tends to be met with social approval within SGM-AFAB communities, whereas involvement with a man can elicit disapproval and criticism from lesbian peers (Hayfield et al., 2014). It is not clear why partnering with a gender minority individual was not associated with fewer depressive and anxiety symptoms, though stigma against gender minority romantic relationships (e.g., Gamarel et al., 2014) may play a role. More research is needed, particularly to explore whether the effects of romantic involvement on psychological health differ by partner gender within individuals over time, and what mechanisms may explain those differences.
Unexpectedly, we found no racial differences in the associations between romantic involvement and any mental health variable. This is contrast to findings from a study using a within-person design (Whitton et al., 2018b), which found that these associations were stronger among Black, and to some extent Latinx, SGM youth than White SGM youth. It is possible that the current study had more power to detect effects in White participants due to a larger sample size. Alternately, the discrepant findings may be due to differences in the age range of the samples: We focused just on 18- to 20-year-old emerging adults, while they captured adolescence through young adulthood (16–26 years). Future research should explore potential differences in the association between romantic involvement and mental health across varying ages.
There were also no differences in use of marijuana or other illicit drugs between single and romantically involved participants in this sample. These findings add to a growing literature suggesting that the “marriage benefit” to marijuana use does not extend to the nonmarital different-sex relationships of young adults (Duncan et al., 2006; Fleming et al., 2010) or to the relationships of lesbian and cisgender female SGM youth (Whitton et al., 2018a). Especially in the light of the increasing decriminalization and availability of marijuana, it will be important to identify factors other than romantic involvement that may protect SGM-AFAB against problematic cannabis and other illicit drug use.
Several study limitations should be noted. First, the cross-sectional data cannot speak to direction of effects; the observed associations may reflect that good mental health promotes entry into a relationship rather than relationship involvement promoting mental health. Once multiwave longitudinal data are available from this sample, we will be better able to explore directionality by testing whether romantic involvement prospectively predicts psychological functioning within individuals. We also did not explore whether the quality of participants’ relationships was associated with their mental health; future research is needed to identify specific relationship characteristics (e.g., satisfaction, communication, commitment) that may promote psychological health among SGM-AFAB emerging adults. It is possible that differences in relationship quality may help to explain observed differences between demographic subgroups. The nonprobability sample limits the extent to which findings can be viewed as representative of the general population of SGM-AFAB emerging adults. Because many participants were recruited via SGM-focused events or social media connections, they may be more embedded in the LGBT (lesbian, gay, bisexual, and transgender) community and more likely to be “out” than the average SGM-AFAB emerging adult. This might reduce potential negative effects of involvement in a romantic relationship, particularly with a cisgender female or gender minority partner. Because all participants were recruited from Chicago, findings may not reflect the experiences of SGM-AFAB living in other regions, especially those less accepting of nonheterosexuality.
Conclusions
Despite these limitations, this study provides new and valuable information about the association between romantic involvement and mental health among SGM-AFAB emerging adults. The current findings extend a small literature suggesting positive mental health effects of romantic relationship involvement for heterosexual emerging adults by demonstrating that it is associated with fewer depressive symptoms, fewer anxiety symptoms, and less problematic alcohol use among SGM-AFAB emerging adults as well. Interestingly, the results suggest that SGM-AFAB who are romantically involved with another woman experience fewer depressive symptoms than not only single SGM-AFAB but also than those who are romantically involved with a cisgender man. This is contrary to concerns that dating a same-sex partner may raise vulnerability to psychological difficulties by activating internalized stigma or revealing a nonheterosexual orientation to unaccepting others. As such, these results suggest the potential utility of efforts to encourage and support romantic relationships—including same-sex relationships—among SGM emerging adults, which may help to address the mental health disparities experienced by this population. Such efforts might include programs to encourage dating among SGM (e.g., through planned LGBT-focused social events) and to teach healthy relationship skills (Mustanski et al., 2015). However, the potential benefits of romantic involvement may not extend to all SGM-AFAB, particularly those who identify as a gender minority or whose sexual identity is not lesbian, highlighting the importance of attending to differences among SGM subgroups in research, theory, and efforts to reduce mental health and substance use disparities.
Footnotes
Acknowledgments
We gratefully acknowledge the FAB400 research team, including Kitty Beuhler, Christina Dyar, Parks Dunlap, Jazz Stephens, Greg Swann, Arielle Zimmerman, and Brian Mustanski. We also thank the FAB400 participants for their invaluable contributions toward understanding the health of the SGM community. These findings were presented at the 2019 meeting of the Association for Behavioral and Cognitive Therapies, Atlanta, GA.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute of Child Health and Human Development (R01 HD086170; PI: Whitton). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing the first author at