
Abstract
This study examined the effects of parents’ posttraumatic stress symptoms (PTSS) and parenting behaviors, children’s feelings of safety, and children’s self-disclosure on children’s PTSS, to elucidate the mechanisms underlying intergenerational effect of PTSS. Three months after the Super Typhoon Lekima occurred in China, August 2019, self-report questionnaires were used to investigate 866 Chinese parent–child dyads (children’s mean age was 10.55 years, 52.2% were boys; parents’ mean age was 37.99 years, 23.2% were fathers) in the area most affected by the typhoon. The results found that parents’ PTSS may have disrupted the provision of emotionally warm parenting, in turn reducing children’s feelings of safety and limiting their self-disclosure, ultimately increasing the severity of children’s PTSS. This suggested that the mechanisms underlying the intergenerational effect of PTSS between parents and children involve the combined role of parents’ emotionally warm parenting, children’s feelings of safety, and children’s self-disclosure.
Keywords
Individuals exposed to natural disasters have been found to be more likely to report a range of psychopathologies, commonly including posttraumatic stress symptoms (PTSS; e.g., Cenat et al., 2020). Moreover, natural disasters have also been found to exert negative effects on families (e.g., McDermott & Cobham, 2012), leading family members (e.g., parents and children) to develop PTSS (e.g., Jones et al., 2002). PTSS can be transmitted between parents and their children in a family environment (e.g., Gil-Rivas et al., 2010) because children take cues from their parents about danger and safety, and respond to parental distress (e.g., Pfefferbaum & North, 2008). Many studies have found that children of parents with PTSS report more PTSS than those with non-PTSS parents (e.g., Yehuda et al., 2008; 2001), and some studies have suggested that parents’ PTSS has a detrimental effect on children’s PTSS (e.g., Lambert et al., 2014; Zhou et al., 2017).
To elucidate the underlying mechanisms by which parents’ PTSS affects children’s PTSS, several mechanisms have been proposed in previous studies. One proposed mechanism lies with the parenting behaviors emphasized by cognitive-behavioral interpersonal theory of PTSD (Creechi & Misca, 2017). This theory suggested that PTSS has negative effects on parent–child relationship function via several processes. For example, behavioral avoidance symptoms may interfere with participation in parent–child activities and symptoms of emotional numbing may interfere with parents’ affective engagement and expression because they are less sensitive to their child’s behavior and emotions (Creechi & Misca, 2017; Sherman et al., 2016). Furthermore, parents’ hyperarousal due to anger and hostility may result in dysfunctional parenting behavior (Bryant et al., 2018; Chemtob et al., 2013; Davies et al., 2008). These can cause internalizing or externalizing problems among children (e.g., Bryant et al., 2018; Schwerdtfeger et al., 2013), further aggravating children’s psychological distress. In light of these previous findings, in the current study, we proposed that parenting behaviors may play a mediating role between parents’ PTSS and children’s PTSS.
In addition to parenting behaviors, children’s feelings of safety may also be an important mechanism. Parents’ PTSS precipitate parental behaviors experienced as frightening by their child (e.g., sudden retreat from child; Schuengel et al., 1999), and threatening children’s feeling of safety. Importantly, family approaches maintain that problems in the functioning of the family unit among PTSS victims are a source of problems experienced by their offspring (e.g., Rosenheck & Fontana, 1998). Families with parents with PTSS may experience difficulties in intimacy and communication (e.g., Fredman et al., 2017; Sherman et al., 2015), and outbursts of aggression (e.g., Byrne & Riggs, 1996; Taft et al., 2007). These behaviors can lead to marital conflict (e.g., Brown et al., 2012; Miller et al., 2013). Living in this type of atmosphere can adversely affect children’s feelings of safety, and this can potentially lead to heightened sensitivity to threats, including minor threats. In turn, this may trigger a sequence of physical, emotional, and cognitive emergency responses, also known as chronic hyperarousal, activating intrusive thoughts, avoidant behaviors/thoughts (e.g., Doron-LaMarca et al., 2015), and finally PTSS. Thus, parents’ PTSS can exert negative effects on children’s PTSS by decreasing children’s feelings of safety.
Another potentially important mechanism involves children’s self-disclosure. Self-disclosure refers to the tendency to share feelings and thoughts with others. By talking with others, individuals can clarify their psychological state and come to terms with events, resulting in gradual habituation to both stimuli and responses from stressful events (Zhen et al., 2018) and reframing of the meaning of trauma (e.g., Calhoun & Tedeschi, 2006), ultimately extinguishing negative emotional associations (e.g., Shim et al., 2011), including PTSS. However, in families with parents exhibiting PTSS, children may not disclose their thoughts and emotions because of the effects of parents’ PTSS. On the one hand, parents’ negative psychological reactions may reduce the child’s willingness to disclose traumatic experiences or distress, out of a desire to avoid increasing others’ distress (e.g., Cummings, 2011). On the other hand, parents’ PTSS can lead to more aggression toward children (e.g., Bryant et al., 2018; Chemtob et al., 2013; Davies et al., 2008), which, in turn, can engender problematic or non-open communication between parents and their children, limiting children’s ability to disclose their thoughts and emotions to their parents. In light of these, we proposed that parents’ PTSS may be associated with children’s PTSS by influencing children’s self-disclosure.
Parents’ PTSS, and children’s feelings of safety and self-disclosure, may all be involved in the mechanisms of intergenerational effect of PTSS between parents and their children. However, because previous studies have only examined the unique roles of these factors, it has been difficult to elucidate their combined role, and thus, the underlying mechanisms of effect of parents’ PTSS on children’s PTSS remain unclear. Integrating these various theories and factors into a larger theoretical framework and examining the combined role of these factors could be helpful for elucidating this issue, contributing to the relieving of children’ PTSS.
Theoretically, parents’ actions are an important factor prompting or inhibiting adolescents’ willingness regarding disclosure (e.g., Tilton-Weaver, 2014), wherein parenting behaviors may be associated with children’s self-disclosure (e.g., Ihemedu, 2018; Soenens et al., 2006; Vieno et al., 2009). Extant studies have reported that parenting with warmth and acceptance can increase disclosure in children (e.g., Blodgett Salafia et al., 2009; Smetana et al., 2006) because it creates a climate in which adolescents feel comfortable revealing personal issues (e.g., Smetana et al., 2006). Such family environments are also conducive to good parent–child relationships, in which adolescents feel supported by parents, and thus, children’s feeling of safety can also be improved, in accord with Feeney and Collins’ (2015) model of thriving through relationships. Experiencing improved feelings of safety means that individuals worry less about the negative results of sharing with others (e.g., Zhen et al., 2018), and are more eager to share their feelings with parents and others. In contrast, parenting behaviors characterized by hostility and aggression (e.g., Bryant et al., 2018; Chemtob et al., 2013; Davies et al., 2008) not only lead directly to an environment involving excessive control over children and thus less disclosure by children (e.g., Soenens et al., 2006), but also threaten children’s feelings of safety and increase their worries regarding disclosure, making them less likely to disclose. That is, parenting behaviors may have a direct association with children’s self-disclosure, as well as having an indirect relationship with children’s self-disclosure by affecting children’s feelings of safety.
The literature reviewed above suggests that parents’ PTSS can exert positive effects on their children’s PTSS via parenting behaviors, children’s feelings of safety, and children’s self-disclosure. However, the specific utility of these mediators’ combined roles has not been evaluated. Particularly, in China, the parental expression of love, support, and warmth is usually expressed by heightened intrusiveness, such as thorough concern, control, and governance of their child rather than the verbal or bodily expression of love and praise (Xia et al., 2015). This may be seen as overprotective parenting behavior in some ways. Thus, parenting behavior may have a different role in Chinese culture. Moreover, extant studies mainly focused on families affected by war (e.g., Lambert et al., 2014; Wittekind et al., 2010; Yehuda et al., 2008; Zhou et al., 2017) revealing intergenerational effect of PTSS between parents and children. Although children who are direct victims of natural disasters have been reported to exhibit PTSS following natural disasters (e.g., Cohen et al., 2016; Zhang et al., 2015; Zhou et al., 2018), it is currently unclear whether findings from studies of families affected by war also apply to families affected by natural disasters. Furthermore, cooperative intervention approach models suggest that, with a lack of studies and psychological services treating adolescents’ psychological distress from a family perspective, adolescents’ distress is likely to persist for long period after natural disasters, despite government agencies, social groups/individuals and schools providing post-disaster psychological services to adolescents (Zhou, 2020). Studies on intergenerational effect of PTSS following natural disasters may inform the development of effective strategies for relieving persistent distress among adolescents. In light of this previous research, the current study assessed the roles of parents’ PTSS and parenting behaviors, and their children’s feelings of safety and self-disclosure, in children’s PTSS following the occurrence of Super Typhoon Lekima in China. Drawing on the theoretical and empirical studies above, we proposed that parents’ PTSS may exert an effect on children’s PTSS via multiple indirect pathways, including parenting behaviors, children’s feelings of safety, and children’s self-disclosure. To be specific, parents’ PTSS may positively influence children’s PTSS via parenting behaviors, children’s feelings of safety, and children’s self-disclosure, respectively, via paths from parenting behaviors to children’s feelings of safety and children’s self-disclosure, respectively, and via paths from parenting behaviors to children’s feelings of safety and then to children’s self-disclosure.
Methods
Participants and procedures
Super Typhoon Lekima occurred in China, August, 2019, affecting 14.024 million people. 2.097 million people were urgently transferred and resettled, 57 people died, 14 people disappeared, and direct economic loss reached 53.72 billion Yuan. All procedures of this study were approved by the Research Ethics Committee of Department of Psychology and Behavioral Sciences, Zhejiang University and was conducted 3 months after the typhoon. We focused on Wenling city in Zhejiang province, which was severely affected by the Lekima typhoon. We firstly contacted the Zhejiang Research Institute of Education Science and informed them of the study’s aims and methods of investigation, then contacted the Wenling Education Bureau for assistance. With the approval of these two education authorities, three primary schools were chosen. With the help of school principals and psychologists, 16 classrooms of approximately 45 students each were selected. All students in the selected classrooms attended school on the assessment date, and all agreed to participate in the investigation and complete self-report questionnaires. The purpose of the study and the voluntary nature of the students’ participation were highlighted before the survey, and written informed consent was obtained from all students and their guardians. Assessments were conducted under the supervision of trained psychology postgraduate students.
With the help of the educational agencies and selected school principals, parents of students in these three schools were recruited to answer an electronic questionnaire via WeChat (a free messaging and calling app that is widely used in China). The purpose of the study and voluntary nature of participation were explained to participants before the survey by researchers and children’s teachers via WeChat, providing a convenient way to conduct self-report questionnaires. Written informed consent was obtained from all participants, and the questionnaires were distributed. After the questionnaires were completed, participants were informed that if they needed support, psychological and counseling services were available via a family psychological service website.
In this study, children and parents independently completed their respective questionnaires, and we finally obtained data from 866 parent–child dyads. All participants were Chinese. Of the 866 children, 452 (52.2%) were cisgender male, 377 (43.5%) were cisgender female, and 37 (4.3%) did not report their gender. Children’s mean age was 10.55 years (standard deviation [SD] = 0.93 years; range 9–13 years; median = 11.00 years), and 10 (1.2%) did not report their age. Of the 866 parents, 201 (23.2%) were fathers and 665 (76.8%) were mothers. Parents’ mean age was 37.99 years (SD = 4.91 years; range 28–63 years; median = 37.00 years), and 146 (16.9%) did not report their age; 297 (34.3%) families had a monthly income >10, 000 RMB and 569 (65.7%) had a monthly income ≤10, 000 RMB (the monthly income of 10, 000 RMB is considered an average income level in China; Chinese National Bureau of Statistics, 2022); 644 (74.4%) parents had an educational level lower than high school and 222 (25.6%) parents had a bachelor’s degree; 789 (91.1%) were married and 77 (8.9%) had an “other” marital status (e.g., divorced or single); 392 (45.3%) parents had a single child, 428 (49.4%) had two children, and the remaining parents (5.3%) had three or four children; 69.2% of parents and 65.2% of children reported that they had been injured or trapped during the Typhoon Lekima, and 31.4% of parents and of 25.6% children reported that their relatives and friends had been injured or trapped, while 22.4% of parents and 16.4% of children reported they had lost property.
Measures
Parents’ and children’s trauma exposure
Trauma exposure was assessed using a self-developed trauma exposure scale, which was adapted from previously used typhoon and hurricane exposure scales (e.g., Chan & Rhodes, 2014; Hall et al., 2019; Weems et al., 2007). This scale included 10 items that assessed typhoon exposure, including injuries, deaths, witnessing the typhoon affecting others, being washed away or trapped during the storm, and damage to home or properties or infrastructure. These items were classified into three types: respondent injured or trapped, family members or friends injured or trapped, and loss of property. All items were rated as yes (1 = yes) or no (0 = no).
Parents’ and children’s PTSD
Posttraumatic stress disorder was assessed using the revised PTSD Checklist (e.g., Zhou et al., 2019) from Weathers’ (2013) PTSD Checklist for DSM-5, which include 20 items. Participants were asked to rate the frequency of symptom items experienced on a 5-point scale from 0 (not at all) to 4 (extremely). The scale has four subscales: intrusions, negative cognition and emotion alteration, avoidance, and hyperarousal. The DSM-5 PTSD Checklist has confirmed psychometric properties, with good convergent discriminant validity (ralerting-CV and rcontrast-CV were 0.94 and 0.92; Wortmann et al., 2016) and reliability (Cronbach’s alpha >0.81; Ashbaugh et al., 2016). It has also been widely adopted in previous studies with adults (e.g., Cero & Kilpatrick, 2020) and adolescents (e.g., Zhou et al., 2021). In this study, children and their parents independently completed the items of this checklist, which was designed to assess the frequency of PTSD symptoms in relation to their typhoon-related experiences, and it exhibited good internal consistency (Cronbach’s alpha = 0.93 for adolescents and 0.96 for parents).
Parenting behavior
Parenting behavior was assessed using a revised scale adapted from the Jiang et al.’s (2010) revised short-EMBU, which assesses children’s perceived parenting behavior. The scale contains 21 items, divided into three types of parenting behavior: rejection (six items), emotional warmth (seven items), and overprotection (eight items). Each of the items was rated on a four-point Likert scale with 1 representing “never” and 4 representing “always.” This scale had good construct and criterion validity and adequate test–retest reliability in a prior study (0.70–0.81; Jiang et al., 2010). In this study, we revised the text to be applicable to parents. For example, the item “My parents praised me” in Jiang et al.’s (2010) questionnaire was changed to “I praised my children” in the revised questionnaire. In the current study, the revised questionnaire exhibited adequate reliability (Cronbach’s alpha = 0.73).
Children’s feelings of safety
Feelings of safety were assessed using Quan et al.’s (2020) Perceived Security Questionnaire. This questionnaire is a 10-item scale designed to measure feelings of life safety (e.g., My life is stable), belonging (e.g., I believe others in our group), and control-related feelings (e.g., I can do something by myself). All items are rated on a five-point scale ranging from 1 (completely disagree) to 5 (completely agree). This scale had good construct validity in a previous study (Liu et al., 2009). In the current study, the questionnaire exhibited adequate reliability (Cronbach’s alpha = 0.76).
Children’s self-disclosure
Self-disclosure was assessed using Zhen et al.’s (2018) revised Distress Disclosure Index from Kahn and Hessling (2001). This index contains 12 items (e.g., I am willing to talk about my distress), rated on 5-point Likert-type scale ranging from 0 (strongly disagree) to 4 (strongly agree). The scale had good mean test–retest reliability (0.80) and adequate convergent validity (rs > 0.16) in previous studies (Kahn et al., 2012). In the current study, the index showed adequate reliability (Cronbach’s alpha = 0.75).
Data analysis procedures
Little’s Missing Completely at Random (MCAR) test was first used to assess whether the pattern of missing data was random. The findings suggested that the data were missing in a non-random fashion, χ2 (345) = 445.248, p < .001, and robust maximum likelihood estimates were used to handle the missing data. Descriptive analyses were conducted for all of the measures administered. Pearson’s correlations were calculated to examine the associations between the major variables. The statistical analyses were conducted using Mplus 7.0 software (Muthén & Muthén, 2012). To evaluate model fit, we used chi-square values, the comparative fit index (CFI), the Tucker-Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean residual (SRMR). A non-significant chi-square value indicated good model-data fit. The general cutoff values for accepting a model were equal to or greater than 0.90 for the CFI and TLI, and less than 0.08 for the SRMR and RMSEA.
To test our hypotheses, several procedures were used in the current study. Regarding the role of trauma exposure in PTSS (Gil, 2015; Milligan-Saville et al., 2018), parents’ and children’s trauma exposure were controlled as covariates in the following analysis. First, a direct effects model was established to test the direct effect of parents’ PTSS on children’s PTSS. Second, based on the direct effects model, we included three types of parents’ parenting behaviors (rejection, emotional warmth, and overprotection), children’s feelings of safety and self-disclosure between parents’ PTSS and children’s PTSS, and built a multiple indirect effects model (see Figure 1) in which the paths from three types of parents’ parenting behaviors to children’s feelings of safety and self-disclosure, and the path from children’s feelings of safety to self-disclosure were added. In this model, to avoid I type error, we examined the correlation between three types of parenting behaviors. Third, we removed the non-significant paths in Figure 1 to obtain a parsimonious model of multiple indirect effects. Finally, we used bias-corrected bootstrap confidence intervals (CIs) to assess the significance of indirect effects of parents’ PTSS on children’s PTSS, in which a 95% CI of the path coefficient that did not include 0 indicated significance. Hypothesized multiple indirect effects model; P-PTSS = parents’ posttraumatic stress symptoms, C-PTSS = children’s posttraumatic stress symptoms.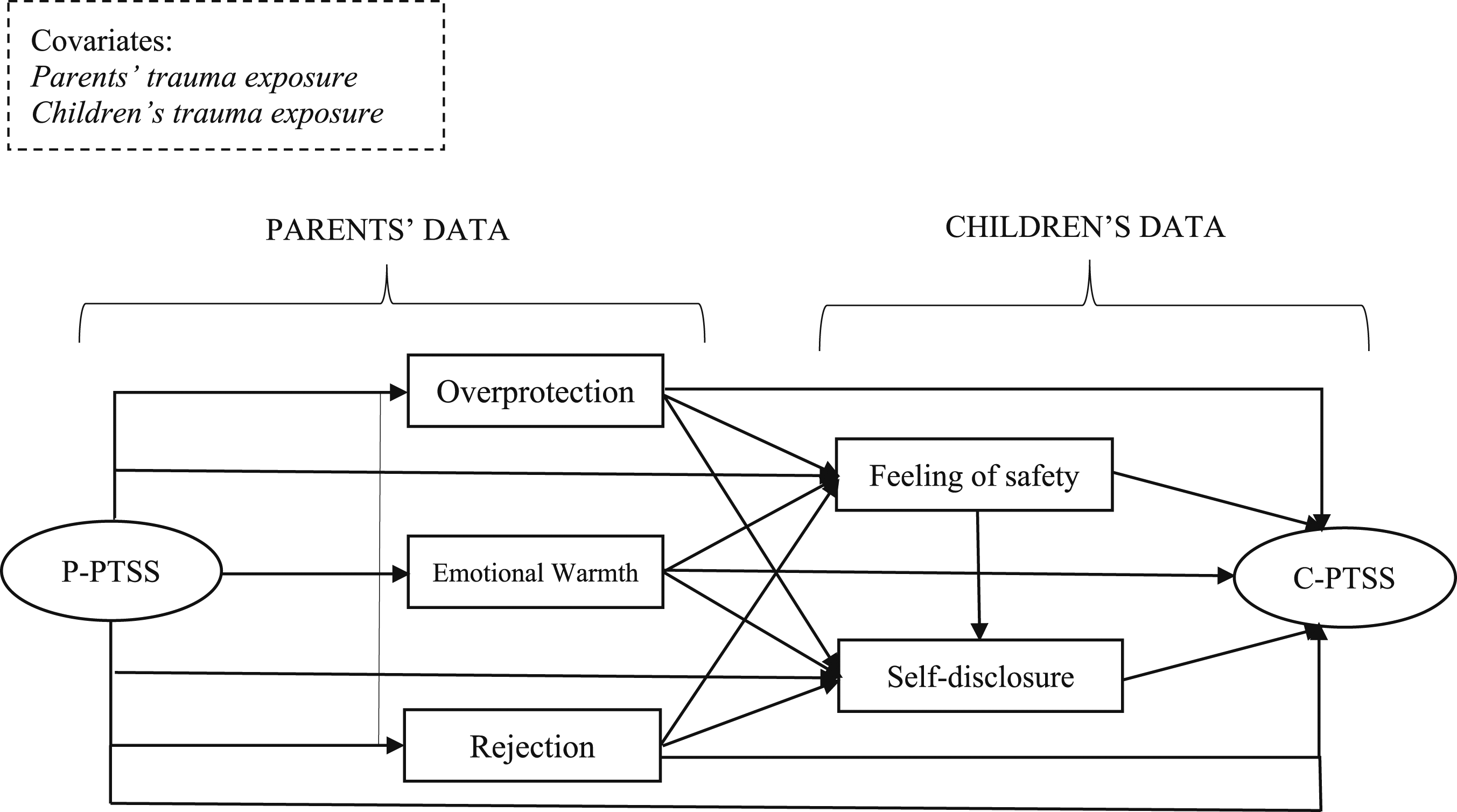
Results
Descriptive statistics and correlations among main measures
Correlations among main measures.
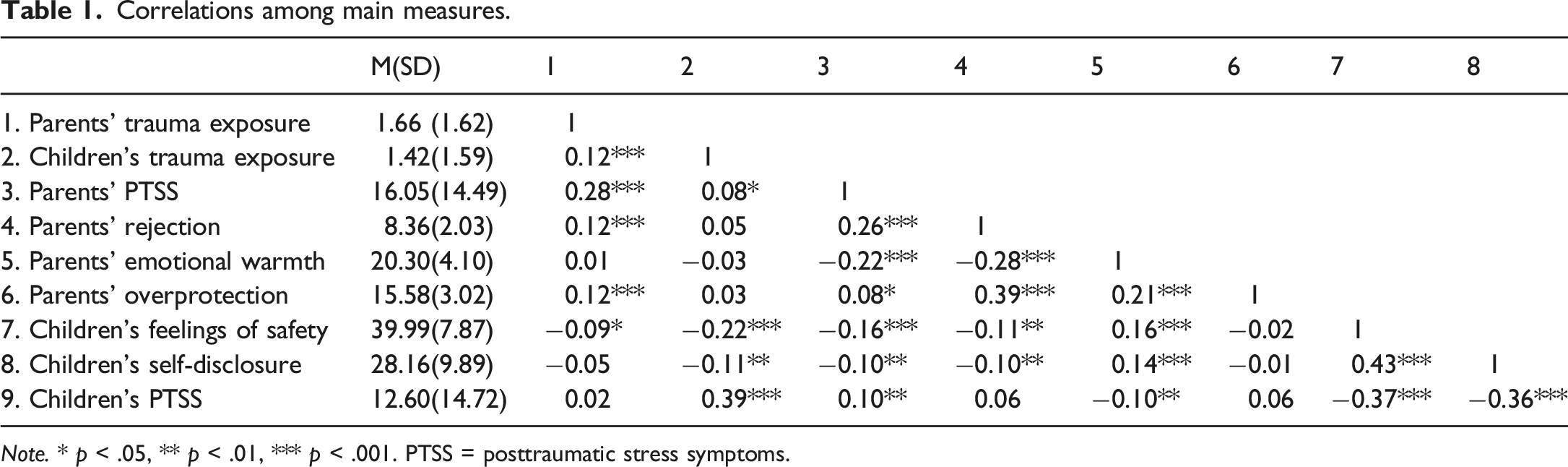
Note. * p < .05, ** p < .01, *** p < .001. PTSS = posttraumatic stress symptoms.
Analysis of multiple indirect effects of parents’ posttraumatic stress symptoms on children’s posttraumatic stress symptoms
We first built a direct effect model of parents’ PTSS to predict children’s PTSS after controlling for parents’ and children’s trauma exposure; the model showed good fit indices, χ2(33) = 215.956, CFI = 0.967, TLI = 0.956, RMSEA (90% CI) = 0.080 (0.070–0.090), SRMR = 0.072. The results of path analysis indicated that parents’ PTSS had a positive effect on children’s PTSS (β = 0.11, p < 0.01). Next, we built the multiple indirect effects model (as shown in Figure 1), and the model fit the data well, χ2(63) = 287.234, CFI = 0.965, TLI = 0.942, RMSEA (90% CI) = 0.064 (0.057–0.072), SRMR = 0.053. The results revealed that, after controlling for parents’ and children’s trauma exposure, the paths from parents’ PTSS to their own emotional warmth and rejection and children’s feelings of safety, the paths from parents’ emotional warmth to children’s feelings of safety and self-disclosure, the paths from children’s feelings of safety to their own self-disclosure and PTSS, and the path from children’s self-disclosure to their own PTSS were significant. No other paths were significant.
To obtain a parsimonious model of multiple indirect effects, we removed the non-significant paths and re-ran the model. The final parsimonious model (see Figure 2) showed good fit indices, χ2(71) = 294.376, CFI = 0.965, TLI = 0.949, RMSEA (90% CI) = 0.060 (0.053–0.068), SRMR = 0.059. The results of the path analysis also identified the significant paths identified above. Furthermore, these findings suggested that after controlling for parents’ and children’s trauma exposure, parents’ PTSS had a significant positive indirect association with children’s PTSS by decreasing children’s feelings of safety or by decreasing children’s feelings of safety and thus reducing their self-disclosure. Parents’ PTSS also exerted a significant indirect positive effect on children’s PTSS by decreasing parents’ emotional warmth and, in turn, reducing children’s feelings of safety or self-disclosure, and by reducing parents’ emotional warmth parenting and, in turn, decreasing children’s feelings of safety and reducing children’s self-disclosure. Final parsimonious model of multiple indirect effects; P-PTSS = parents’ posttraumatic stress symptoms, C-PTSS = children’s posttraumatic stress symptoms.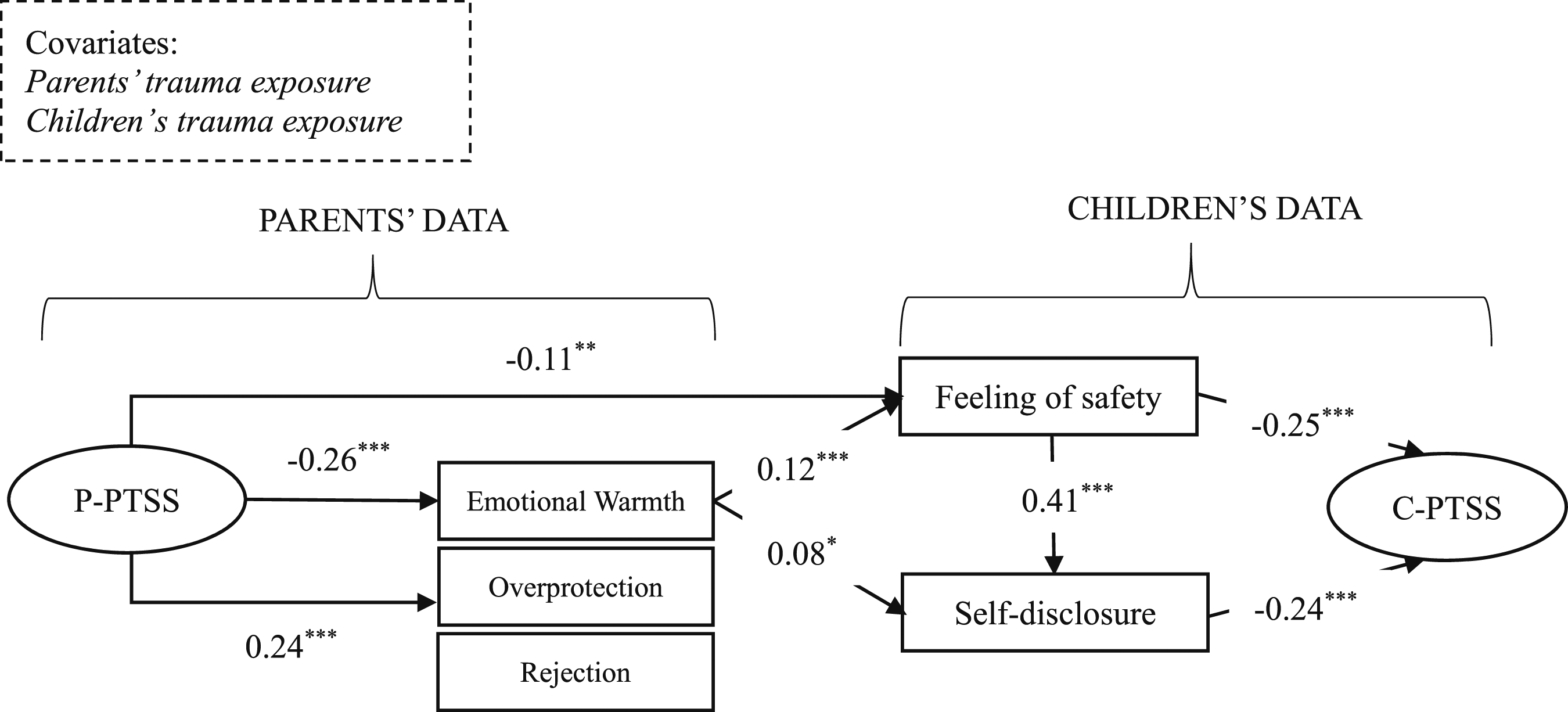
Bias-corrected bootstrap tests of mediating effects.
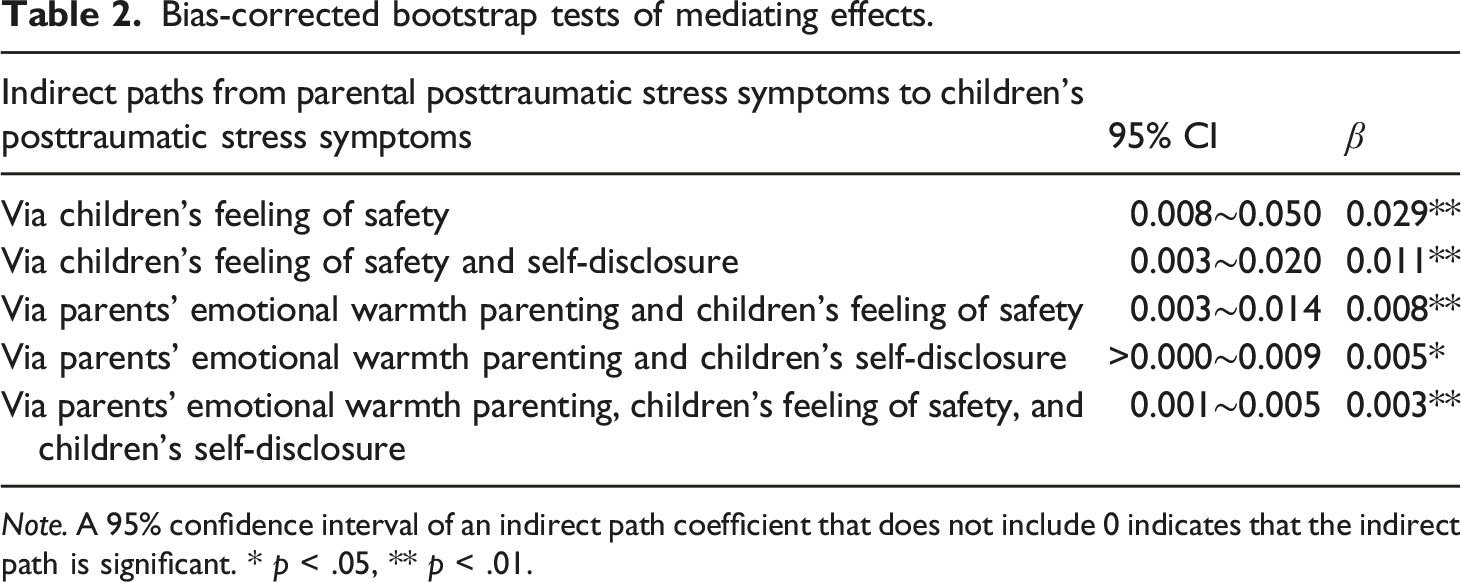
Note. A 95% confidence interval of an indirect path coefficient that does not include 0 indicates that the indirect path is significant. * p < .05, ** p < .01.
Discussion
This is the first study to examine the intergenerational effects of parents’ PTSS on children’s PTSS following Super Typhoon Lekima. After controlling for parents’ and children’s exposure to the disaster, we found that parents’ PTSS exhibited direct and positive effects on children’s PTSS. This result was consistent with previous studies on the impacts of war (e.g., Lambert et al., 2014; Wittekind et al., 2010; Yehuda et al., 2008), suggesting that the intergenerational effect of PTSS between parents and children is common across trauma types. In subsequent analyses that included parents’ parenting behaviors, children’s feelings of safety, and self-disclosure of parents’ PTSS and children’s PTSS, parents’ PTSS exhibited a significant positive effect on children’s PTSS via these mediators. This finding suggests that parenting behaviors, children’s feelings of safety, and self-disclosure were important mechanisms affecting the intergenerational effects of PTSS. These findings could inform interventions focusing on these factors to block the intergenerational effect of PTSS, using a family-based approach.
Specifically, we found that parents’ PTSS exerted an indirect effect on children’s PTSS by decreasing children’s feelings of safety, or by decreasing children’s feeling of safety and then reducing self-disclosure. Parents with PTSS may be physically present but psychologically absent because of their PTSS (e.g., Dekel et al., 2016), causing difficulty in taking responsibility for family care tasks, such as parenting their children. In light of these, children’s feelings of safety in the present study appeared to be threatened by parents’ PTSS. This phenomenon could increase children’s hyperarousal state to trauma-related cues, in turn leading to a set of symptoms of PTSS, such as reexperiencing, avoidance, or numbing (e.g., Doron-LaMarca et al., 2015). Moreover, experiencing reduced feelings of safety may cause children to worry about the negative results of sharing or disclosure, thus making them less inclined to share with parents, keeping secrets from parents, putting a barrier between themselves and their parents (e.g., Finkenauer et al., 2002). Consequently, parental support may not be accessible because parents do not understand their children’s emotional states. This process may trigger negative emotional feelings in adolescents (e.g., Ihemedu, 2018), aggravating PTSS.
The current findings also suggested that parents’ PTSS was indirectly associated with children’s PTSS by reducing parents’ emotional warmth, in turn leading to children’s reduced feelings of safety. Parents’ emotional warmth is characterized by parents’ encouragement, praise, love, and emotional support (e.g., Arrindell et al., 2005; Jiang et al., 2010). For parents with PTSS, intrusion and avoidance symptoms can elicit insensitive parenting behavior (e.g., Van Ee et al., 2016), reducing emotional warmth parents provide to children, wherein children may have reduced feelings of safety following stressful events, in accord with Feeney and Collins’ (2015) theoretical model. This, in turn, may increase fear and negative cognition about self and world (Quan et al., 2020), leading to the occurrence of PTSS in children. Because children with reduced feelings of safety may not want to share their feelings or thoughts with parents and, in turn, may exhibit more PTSS, the current study suggests that parents’ PTSS has a positive relation to children’s PTSS by reducing their emotional warmth and, in turn, decreasing their children’s feelings of safety and reducing children’s self-disclosure.
Moreover, living in a family environment with less parental emotional warmth because of parents’ PTSS, children are less likely to disclose with parents because receiving positive responses from parents is perceived to be difficult (e.g., Finkenauer et al., 2002; Tilton-Weaver et al., 2010). By sharing with others, however, individuals can clarify their psychological states, come to terms with events, and realize the reconstruction of traumatic events (e.g., Quan et al., 2020), which can ultimately lead to relief of PTSS. In contrast, it may increase the severity of PTSS. Thus, the current study revealed that parents’ PTSS also has an indirect association with children’s PTSS by reducing parents’ emotional warmth and consequently leading to a decrease in children’s self-disclosure.
Interestingly, parents’ PTSS had a positive association with overprotection, but overprotective parenting had a non-significant relationship with children’s feelings of safety, self-disclosure, and PTSS. Theoretically, a central problem of PTSS is a reduced capacity to suppress fear under safe conditions (e.g., Jovanovic et al., 2010; Norrholm et al., 2011), and individuals with PTSS may also show difficulty inhibiting fear to threat-related cues (e.g., Jovanovic et al., 2010). Thus, parents with PTSS might worry about their children’s safety following trauma experiences, leading them to increase their control of children’s behaviors and routines to protect them from harm, ultimately leading to increased overprotection of children. However, when parents overly protect children, they may communicate that the world is a dangerous place, preventing the child from learning how to deal with stressful situations (e.g., Gere et al., 2012), limiting children’s learning and use of action-oriented coping strategies (e.g., Cheron et al., 2009; Nolen-hoeksema et al., 1995). Thus, children may have difficulty experiencing feelings of safety and self-disclosure, or resolving PTSS. Moreover, parental control is understood as an expression of love and care for Chinese children (Xia et al., 2015). Therefore, children may not have experienced different levels of feelings of safety and self-disclosure than they did before.
Several limitations of the current study should be noted. First, because parents and children were assessed using self-report questionnaires, participants’ reporting bias was difficult to exclude. Second, only including a sample of individuals exposed to a typhoon might limit the generalizability of the current results. Third, because this was a cross-sectional study, the potential causal relationships between variables should be interpreted with caution. Fourth, demographic information is not comprehensive (e.g., sexual orientation and disability were not recorded) because of the limited number of questionnaire items. Moreover, additional factors that may influence a child’s PTSS, self-disclosure, and feelings of safety were not included in the current study, such as parental daily involvement, prior trauma exposure, and parental marital status. Future studies could consider controlling for more potential influential factors to draw more rigorous conclusions.
Despite these limitations, the current study integrated the mechanisms of parents’ parenting behaviors, children’s feelings of safety and self-disclosure into a larger framework, contributing new insights to extend current understanding of the intergenerational effect of PTSS. Additionally, the current findings suggest that, if parents’ PTSS is not resolved, it can transit to their children via changes to parenting behaviors and children’s feelings of safety and self-disclosure, leading to persistent PTSS despite schools providing substantial support to children. From a clinical perspective, on one hand, the current findings indicate that addressing parents’ distress is important for relieving children’s PTSS (Zhou, 2020). Clinical workers could directly relieve parental PTSS using existing interventions, such as trauma-focused cognitive-behavioral therapy, or eye movement desensitization and reprocessing, to protect children from suffering PTSS. On the other hand, carrying out interventions to disrupt the predictive paths of PTSS may also be valuable, including providing parental emotional warmth to children, creating a safe environment to support children’s feelings of safety, and encouraging children to share feelings and thoughts with their parents.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the General Project for National Social Science Fund of China (Grant No. 20BSH167).
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared but are available upon request. The data can be obtained by contacting Xiao Zhou or Rui Zhen by the emails: