
Abstract
The current study examined couple-level profiles to reveal systematic patterns of health and well-being in older couples. Using latent profile analysis, dyadic profiles were constructed in a national sample of 535 older, different-sex couples based on couples’ marital quality, psychological well-being, and physical health. Results revealed 4 distinct profiles: Maritally Satisfied and Healthy (63.5%), Maritally Dissatisfied and Moderately Healthy (14.7%), Maritally Satisfied with Unhealthy Wives (12.3%), and Maritally Satisfied with Unhealthy Husbands (9.3%). Husband age and education, wife education, and marriage length were significant predictors of class membership. Within-class partner concordance analyses confirmed that the latter two profiles featured the largest discordance between partners’ health and well-being. Most couples in this sample of older adults belonged to a class who demonstrated successful aging in all domains. A smaller group maintained high marital quality despite physical and psychological difficulties, and other couples were moderately healthy but maritally dissatisfied.
Keywords
Introduction
People age with remarkable heterogeneity in their physical health, psychological well-being, and the extent to which they can participate and enjoy life’s activities. According to Rowe and Kahn (1997), successful aging involves maintaining good health, preserving cognitive and physical function, and sustaining emotional well-being with high social engagement. Prior work has documented nine different profiles with varying irregularity between health, social functioning, and cognitive and psychological well-being (Smith & Baltes, 1997). Importantly, however, these profiles were examined at the individual-level, ignoring the robust dyadic and bidirectional evidence that exists within the domains of successful aging—including between marital quality and psychological well-being (Proulx et al., 2007; Sharabi et al., 2016), between marital quality and physical health (Birditt & Antonucci, 2008; Kiecolt-Glaser et al., 2005; Robles et al., 2014; Umberson et al., 2006), and between psychological well-being and physical health (Falconier et al., 2015; Monin et al., 2016). Thus, examining couples’ profiles in the domains of aging is a valuable next step given the increasing centrality of the marital relationship as networks shrink in older age (De Jong Gierveld et al., 2009).
Only one prior study provides a basis for the examination of couples’ profiles. Ko and colleagues (2007) constructed dyadic profiles of successful aging in a sample of 287 middle-aged and older married couples living in Utah. In a latent profile analysis of five broad dimensions—physical health, cognitive function, personality, social support, and marital satisfaction—two candidate solutions emerged. In both the two-profile and four-profile solutions, most couples belonged to a successful aging group that was positive across all indicators. Although the two-profile solution showed the best fit with the data, the four-profile result revealed more distinct and conceptually meaningful groups. In addition to the generally positive profile, the results produced a group that was maritally unsatisfied but average or high on other measures, maritally satisfied but unhealthy, and one that was lower in cognitive function compared to other groups but otherwise satisfied and healthy.
Despite this initial and valuable work, it is not without important limitations. Ko and colleagues’ sample suffered from methodological constraints, including the use of a smaller sample size for LPA, being geographically limited to one area, and those with cardiovascular disease were excluded. In addition, Ko’s study, did not identify or examine within-class, between-partner discordance on indicators of aging. Given the prevalence of health conditions among older dyads, which can either be similar or completely different health challenges (Polenick et al., 2020), identifying profiles of couples who are discordant on health dimensions seems likely (e.g., one partner is in good physical health, the other is not). As such, this past work found classes that may not replicate because they do not represent an older adult population (geographically and health-wise), and it systematically excluded certain classes that may organically arise without strict exclusion criteria. Finally, this past work did not predict, but identified classes that were discordant across domains (e.g., good physical health, poor relational health), which is not consistent with aging theories. Thus, our understanding of the heterogeneity of how couples age across and between domains remains limited. The current study aimed to address these lingering questions to understand the various ways couples age together. We first consider these findings in the context of individual and dyadic aging theories and prior bidirectional literature on dyadic multidimensional health.
Individual and dyadic aging theories
Similar to successful aging, many theories of aging are individual in nature and do not consider the interplay between a partner’s domains. However, a robust literature exists on the importance of marriage, social networks, and social isolation/loneliness on physical and psychological health (Umberson et al., 2006). Both relational developmental theories and prominent aging theories suggest that couples will grow closer as they age (e.g., Burke et al., 2019). Indeed, Socioemotional Selectivity Theory (SST; Carstensen, 1996; Löckenhoff & Carstensen, 2004) posits that as individuals age, their motivation shifts to prioritize aspects of life that optimize the future because they view time as limited. In the context of romantic relationships, this can cause couples to seek emotional intimacy and develop their relationship with their partner (Carstensen et al., 1999). Emotionally, individuals might adjust their emotional experiences by avoiding negative states and intensifying positive states. Indeed, research suggests that younger individuals gravitate toward problem-focused coping strategies (i.e., instrumental behaviors that deal directly with the problem or its effects) and older individuals shift more toward emotion-focused coping strategies (Löckenhoff & Carstensen, 2004). Finally, in the context of physical health, individuals and couples might shift to prioritize health behaviors to maximize and extend life.
Extending SST to the dyadic context, Li and Fung (2011) proposed the Dynamic Goal Theory of Marital Satisfaction (DGTMS), which suggests that partners have multiple goals (e.g., instrumental goals, companionship goals, and personal growth goals, etc.) throughout the lifespan. The DGTMS posits that younger couples may prioritize more personal growth goals, middle-aged couples may prioritize instrumental goals, and older adults prioritize companionship goals (Carstensen, 1996; Li & Fung, 2011). Thus, theoretically, older couples should prioritize their relationship over other goals. However, other scholars argue that this must consider the unique interplay of psychological, relational, and physical health of both partners (Burke et al., 2019; Polenick et al., 2015).
The interplay between marital quality, psychological well-being, and physical health
Abundant literature has linked higher marital quality to better psychological well-being (e.g., Proulx et al., 2007) and better physical health (Robles et al., 2014). Indeed, couples’ ability to resolve conflict is associated with fewer depressive symptoms (Sharabi et al., 2016), better subject subjective health (Umberson et al., 2006) and objective health (including better immune and cardiovascular functioning; Kiecolt-Glaser et al., 2005), and decreased mortality risk (Birditt & Antonucci, 2008). Importantly, these associations are dyadic and longitudinal (e.g., Falconier et al., 2015; Monin et al., 2016; Siegel et al., 2004). However, not all couples with a depressed partner experience relationship distress, dissatisfied couples do not always develop psychological distress, and those with health problems do not always experience relational or psychological distress (e.g., Uebelacker & Whisman, 2006). In sum, higher marital quality can enhance physical health and psychological well-being, and lower marital quality can diminish physical and psychological health, but this link is certainly bidirectional and may be somewhat gendered in different-sex couples as discordance can exist between partners for a variety of reasons. Thus, examining the heterogeneity of successful aging in dyads must utilize methodologies that go beyond mean-level differences.
Concordance and discordance between partners among aging domains
Ko and colleagues’ (2007) found considerable consonance between spouses. Not only did most participants have high functioning across domains, but also husbands and wives reported similar levels of functioning. Moreover, in all classes, husbands and wives had comparable levels of functioning within each domain, even when there were discrepant levels of functioning across domains. This pattern aligns with the extensive literature showing concordance in spouses’ health, health behaviors, and psychological well-being across time (Davillas & Pudney, 2017; Kiecolt-Glaser & Wilson, 2017), particularly through shared resources such as finances, social network, food pantry, mood states, and even joint participation in health behaviors (Wilson & Novak, 2021).
The most surprising discovery from Ko and colleagues (2007) was the emergence of three profiles that featured discrepant levels of functioning across domains. The maritally dissatisfied group showed low relationship scores but physical health scores that were average or better, yet husbands and wives were similarly dissatisfied and similarly healthy. The maritally satisfied but unhealthy group showed the opposite pattern. Results were age-graded: the maritally dissatisfied, healthy group was largely comprised of middle-aged couples, whereas 90% of the maritally satisfied, unhealthy group were older adults. These patterns were unexpected from the mechanistic perspective that focuses on mutual influences among domains, but they do align with aging theories. On average, the prevalence of many chronic conditions, including hypertension (a focal outcome in the Ko study) increases with age, and according to some work, marital satisfaction may be higher as well—through both attrition of unhappy couples and favorable social-emotional changes. The theory of selection, optimization, and compensation explains that individuals can hold this apparent tension by embracing attainable goals and letting go of unrealistic goals (Löckenhoff & Carstensen, 2004). In this case, older couples may choose to focus on the goals of investing in and enjoying their marital relationship, resilient to the normative onset of common health issues like hypertension.
The type of pattern that was missing from Ko and colleagues’ (2007) results is one of discordance between partners. Whether through genetic or lifestyle factors, distinct groups may exist wherein one partner is unhealthier than the other. This type of profile may be more common among older adults, especially in caregiving dyads. Certainly, a partner’s poor physical health may strain the relationship and make it more difficult to mutually exchange emotional and instrumental support (Booth & Johnson, 1994). In turn, the healthy spouse may experience higher stress from caring for the other partner, leading to worse psychological, physical, and relational health outcomes (Iveniuk et al., 2014; Pruchno et al., 2009). As such, we expect that profiles may emerge in which couples are discordant in terms of physical health or psychological well-being.
The present study
The present study examined three dimensions of successful aging—psychological, physical, and relational health indicators—within a large national sample of older married couples using dyadic latent profile analysis (LPA; Muthen & Muthen, 1998–2017). LPA is a latent variable mixture modeling technique that identifies unobservable subgroups within a sample based on individuals’ shared characteristics and meaningful difference from participants in other subgroups. This method enables researchers to (1) move beyond sample averages and general trends (i.e., homogeneous) to identify distinguishable characteristics (i.e., heterogeneous) within a population, and (2) allows the inclusion covariates which are used to predict class membership. Thus, LPA offers unique strengths to answer research questions that are not possible with other methodologies (such as response surface analysis or moderation analysis).
We sought to build upon Ko and colleagues’ important work in a few key ways. First, Ko’s sample was drawn from one part of the country and excluded individuals with cardiovascular health problems. By comparison, the current study used a larger, national sample (N = 535 couples) without health exclusions and with the most recent standards of evaluating model fit in latent profile analyses. Second, we chose indicators that were similar to Ko and colleagues’ past work (depressive symptoms, marital satisfaction, and self-rated health), but we also chose indicators that differed, including affective communication, which is strongly associated with physical health, psychological well-being, and marital quality (Proulx et al., 2007; Sharabi et al., 2016) and also that older couples shift from problem solving to emotion-focused coping (Löckenhoff & Carstensen, 2004). We also examine the unique contribution of perceived stress, which is highly tied to physical health and relationship functioning and dyadically intertwined (Randall & Bodenmann, 2009), especially among older couples (Birditt et al., 2014). Third, we also sought to empirically test within-class between partner differences. We examine whether classes exist where there is concordance or discordance between partners. Based on prior work, we expected that a subgroup of couples would emerge who were concordant and high functioning in all domains, another would emerge that had lower marital quality but were moderately healthy in other domains, and finally that other profiles might emerge in which couples would have more psychological and physical difficulties with varying levels of marital quality.
Fourth and finally, we examined relevant demographic and life course factors as covariates: relationship length, age, education, and retirement status. We anticipated that longer relationship length, older age, lower education, and neither partner being retired will be associated with membership in the unhealthy profile (worse couples’ physical health, psychological well-being, and marital quality); e.g., Curl & Townsend, 2014), as well as more discordance between partners. In contrast, we predict that shorter relationship length, younger age, higher education, and if both partners were retired will be associated with membership in the healthy profile (better physical health, psychological well-being, and higher marital quality) as well as more concordance between partners. The following research questions guided the present study: Research Question 1: What dyadic profiles of psychological, physical, and relational health emerge from a large, national sample of married older couples? Research Question 2: Do psychological, physical, and relational health differences exist between couples within classes? Research Question 3: What demographic characteristics predict class membership? Does a longer relationship, older age, higher education, and being retired predict greater likelihood of belonging to a concordant profile?
Methods
Procedures
Data were from Project Couple Retire, a large national survey in the US that began in 1994 and focused on physical and mental health over time during retirement (Sandberg & Harper, 1999). Data were purchased from The Donnelley Corporation, a major marketing firm, who mailed surveys to 9328 addresses, and guaranteed that each of the addresses represented a randomly selected different-sex (cisgender men and women), married couple with at least one partner between ages 55 and 75 from each state in the U. S. Of all mailed questionnaires, 591 were returned due to people no longer meeting the inclusion criteria, they were no longer living at the address, or were the wrong addresses. Of the remaining 8,737, only 1611 were returned for research. The overall response rate for the study was 18.4%, which is common among lengthy, mailed surveys with studies of older adults (Kaldenberg et al., 1994). Further filtering removed 997 because only one partner responded or because the questionnaires were too incomplete (missing complete scales), and the remaining 614 cases were further cleaned for outliers resulting in 535 couples used in the data analysis. Each partner was instructed to fill out the surveys separately and then return their completed questionnaires in a self-addressed, stamped envelope provided by the researchers. This study received research oversight approval from the Institutional Review Board at a large university in the western United States.
Sample
This study utilized paired data from 535 different-sex couples (consisting of cisgender men and cisgender women). To confirm if gender identity (cisgender husband-wife dyads) was an accurate empirical distinguisher between partners, an omnibus test of model distinguishability was performed. Results from the Structural Equation Model for all the variables included in the LPA led us to treat husband-wife dyads as distinguishable by gender identity (χ2 = 135.78 (36), p < .001).
The mean age for men was 64.98 (SD = 4.38; median = 65, range = 49–79) and for women was 62.40 (SD = 5.50; median 63, range = 40–76). The average length of marriage was 36.2 years (SD = 4.38; Median = 40.00; Range = 2–52 years). About 75% of husbands were in their first marriage (with 17.6% in their second, and 6% in their third or subsequent marriage; up to eight) and 76% of wives were in their first marriage (19% in the second and 5% in third or subsequent marriage; up to six). Finally, the majority of the sample were Caucasian (97%), median income for men was $20,000 to $29,999 for women was $10,000–$19,999, and 70% of the wives and 65% of the husbands were not employed outside of the home at the time of response. The husbands that did work out of the home worked and average of 29.95 hours a week (SD = 17.96; Median = 38, Range = 0–90) and wives worked an average of 28.45 hours (SD = 16.43; Median = 35; Range = 0–70). Further sample and procedure description is provided in Harper and Sandberg (2009).
Measures
Psychological Health Indicators
Depressive symptoms
Depressive symptoms were measured via 14-items from the Center for Epidemiological Studies Depression Scale (CES-D), “a short self-report scale designed to measure depressive symptomatology in the general population” (Radloff, 1977, p. 385). Responses ranged from 0 (rarely or none of the time, less than 1 day) to 3 (most or all of the time, 5 to 7 days) and higher scores represented more depressive symptoms. For this sample, Cronbach alpha reliabilities were .86 for husbands and .90 for wives. The clinical cut-off score for major depression is greater than or equal to 16.
Perceived stress
Perceived stress was assessed via 53 items from the Hassles and Uplifts Scale (HUS; DeLongis et al., 1988), which assessed health, work, intra and interpersonal, and environmental stressors during the past week. Each item was assessed on a four-point Likert scale from 0 (none) to 3 (a great deal). Responses were summed (used the summary score method as proposed by Aldwin and colleagues, 2014), with a possible range of 0–158. For this sample, Cronbach alpha reliabilities were .94 for husbands and .94 for wives.
Relational Health Indicators
Problematic affective communication
Perceptions of problematic affective communication were measured by 13 items from the revised Marital Satisfaction Inventory (Snyder, 1997), and assesses the dissatisfaction of affect of conversations or how conversations are processed. Responses were assessed as 1 (true) or 0 (false) and scores were added together so that higher scores indicating more reported problems in affective communication.
Marital satisfaction
The three-item Kansas Marital Satisfaction Scale (Schumm et al., 1983) was used to measure marital satisfaction. Each question is scored on a 7-point Likert scale, ranging from 1 (extremely dissatisfied) to 7 (extremely satisfied), resulting in a total score ranging from 3 to 21 where higher scores indicate more satisfaction. The Cronbach’s alpha reliability coefficient in this study was .97 for husbands and .97 for wives. The cutoff score for distressed vs nondistressed couples is 17 (Crane et al., 2000).
Physical Health Indicators
Health satisfaction
Participants were asked to respond to “How satisfied are you with your overall health?” with responses ranging from 1 (extremely dissatisfied) to 7 (extremely satisfied). The higher the score, the more satisfied the individual was with his or her health.
Total health problems
Total health problems were measured using the Charlson comorbidity index (Charlson et al., 1987). This index assesses the presence of a wide range of potential comorbid health conditions, such as heart disease, asthma, ulcers, and stroke. Respondents reported whether they experienced the health condition 1 (yes) or 0 (no). Items were summed to produce a total score reflecting the total number of comorbid health problems.
Predictors of class membership
In the LPA, indicator variables are explained by latent group classification and are therefore distinct from covariate predictors which explain latent group classification. In the present study, we included husband and wife age and education as individual covariates. Couple retirement status was included as two dummy coded variables (both retired; 0 = only one partner, 1 = both partners retired; neither retired 0 = both retired, 1 = neither retired). Relationship length was included as a continuous variable (in years).
Analytic Plan
Little’s MCAR test indicated a total of 0.171% of all values for the main variables were indeed missing completely at random: chi-square = 56.043 (df = 42; p = .072). Full Information Maximum Likelihood made use of all available observations (Muthen & Muthen, 1998–2017). Consistent with Ko and colleagues (2007), we conducted a dyadic LPA with continuous indicators using Mplus 8.1 (Muthen & Muthen, 1998–2017). In addition to identifying unique profiles, LPA allows the inclusion of covariates (i.e., demographic and factors) to predict class membership. The dyadic LPA was conducted at the couple level by including both husbands’ and wives’ 6 measures (affective communication, marital satisfaction; depressive symptoms, perceived stress; self-reported health, number of comorbidities) as parallel inputs, consisting of 12 variables in total. Each indicator was correlated with the partner’s score on the same construct, reflecting the dyadic nature of the couple (e.g., husband marital satisfaction with wife marital satisfaction).
To address RQ1, successive LPAs where classes were iteratively added to the model one by one to identify which solution best fit the data (Nylund et al., 2007). Model fit was evaluated by the log-likelihood, Bayesian information criterion (BIC), Akaike’s information criterion (AIC), Lo-Mendell- Rubin likelihood ratio test (LMR), and the Bootstrapped Likelihood Ratio Test (BLRT). Lower log-likelihood, BIC, and AIC values indicate better fitting models. The LMR and BLRT is used during the class enumeration process to determine whether the specified model fits the data significantly better than a model with k - 1 classes. A statistically significant LRT value indicates that the model with k classes is the better fit. Entropy values greater than .8 demonstrated sufficient distinction between classes, with higher values signifying better delineation (Lo et al., 2001). Finally, theoretical relevance and the rule of parsimony also played a critical role in identifying the best class solution for the data. We performed post-hoc analyses of variance (ANOVAs) to validate that the latent classes were significantly different from one another on the indicator variables by first exporting the posterior probabilities from MPlus and second conducting ANOVAs with tukey’s HSD for significant differences between classes in SPSS software (version 25.0).
After we identified the best fitting unconditional model, RQ2 involved calculating difference scores between each partner within each class: (husbandscore – wifescore). Classes and individual partners were then ranked according to their mean between and within classes. A posthoc ANOVA was performed using the SPSS program (version 24.0) to examine if there were significant differences between classes among difference scores. Finally, to answer RQ3, covariates were added to the analyses and the LPA was rerun to examine which variables significantly predicted class membership. A multivariate logistic regression within the LPA simultaneously regressed the best fitting latent profile solution (using latent class posterior probabilities identified in Step 1) on all covariate predictors. The largest class was specified as the reference class, and odds ratios for each covariate predictor were interpreted accordingly.
Results
Summary of class enumeration fit statistics for 1 to 5 class models.
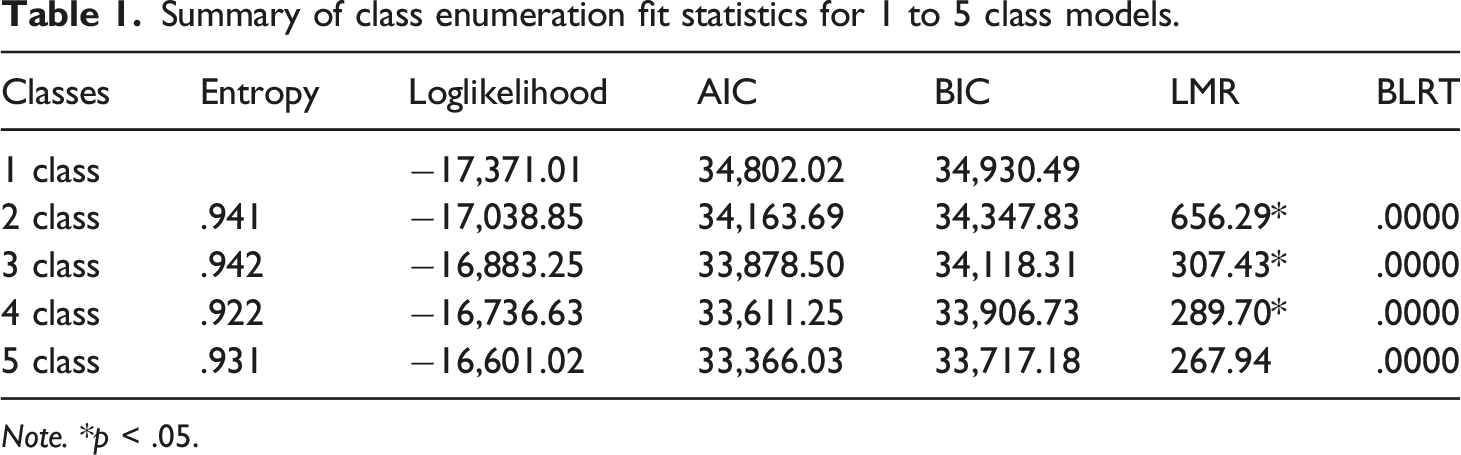
Note. *p < .05.
Descriptive statistics of older couples’ marital quality, psychological well-being, and physical health (N = 535).

Problematic Affective Communication, where higher scores = worse. *Hassles Intensity Score.
Income: 1 = <$9,999, 2 = $10K-$19,999, 3 = $20K-$29,999, 4 = $30K-$39,999, 5 = $40K-$49,999, 6 = $50K-$59,999, 7 = $60K-$69,999, 8 = >$70K.
cutoff of 17.
cut off of 16.
Description of profiles (RQ1)
The Maritally Satisfied and Healthy class included over half of the sample (63.5%). They had the lowest problematic affective communication (MHusband = 1.43; MWife = 1.99), the second highest marital satisfaction (MHusband = 19.76; MWife = 19.89), were the most satisfied with their health (MHusband = 5.47; MWife = 5.75), had the least health problems (MHusband = 1.53; MWife = 1.09), and the lowest depressive symptoms (MHusband = 3.55; MWife = 3.59) and perceived stress (MHusband = 36.73; MWife = 40.22).
The Maritally Dissatisfied and Moderately Healthy class comprised ∼15% of the couples. They had the most problematic affective communication (MHusband = 5.50; MWife = 10.25) and lowest marital satisfaction (MHusband = 16.30; MWife = 13.51). However, both the husband and the wife had moderate health satisfaction (MHusband = 5.02; MWife = 4.98) and both partners had moderate numbers of health problems (MHusband = 1.97; MWife = 1.73). Conversely, wives had among the highest rates of depressive symptoms (MWife = 11.94) and perceived stress (MWife = 57.15), both compared to husbands in this group (Depressive symptoms: MHusband = 7.23; Perceived stress: MHusband = 50.64), and relative to wives in the other classes (Depressive symptoms: MWives = 10.54 and 7.71; Perceived stress: M Wives = 54.20 and 49.99, respectively).
The third largest class, the Maritally Satisfied with Unhealthy Wives, comprised 12% of the total sample. This profile had low levels of problematic affective communication (Husband: MHusband = 1.75; Wife: MWife = 2.60) and the highest marital satisfaction of all groups (Husband: MHusband = 20.17; Wife: MWife = 19.93). Husbands’ health satisfaction and health problems (health satisfaction: MHusband = 5.29; health problems: MHusband = 1.99) were lower than their wives, whose health was the worst in the entire sample (Wives health satisfaction: MWife = 2.86; wives’ health problems: MWife = 3.85). Both husbands and wives in this class had moderate-to-high depressive symptoms (Husband: MHusband = 5.19; Wife: MWife = 10.54) and perceived stress (Husband: MHusband = 35.62; Wife: MWife = 54.30).
Finally, the smallest profile in the sample (9.3%) was the Maritally Satisfied with Unhealthy Husbands. Both partners had moderately low levels of problematic affective communication (MHusband = 3.83; MWife = 3.22) and moderately high relationship satisfaction (Husband: MHusband = 18.69; MWife = 18.73). However, in contrast with Maritally Satisfied with Unhealthy Wives, the husbands had more health problems (MHusband = 2.96; MWife = 1.78) and lower health satisfaction than their wives (MHusband = 4.24; MWife = 5.43). They also had the highest depressive symptoms (MHusband = 19.09) and perceived stress (MHusband = 60.31) of the entire sample and compared to wives in this class (depressive symptoms: MWives = 7.71; perceived stress: MWives = 49.99). See Figure 1 for a graphical representation of results. Dyadic profiles of older couples’ marital quality, psychological well-being, and physical health. Note: HAFFCOM = husband problematic affective communication; WAFFCOM = wife problematic affective communication; HMARSAT = husband marital satisfaction; WMARSAT = wife marital satisfaction; HHSAT = husband health satisfaction; WHSAT = wife health satisfaction; HHPROB = husband number of health problems; WHPROB = wife number of health problems; HDEPRESS = husband depressive symptoms; WDEPRESS = wife depressive symptoms; HSTRESS = husband perceived stress; WSTRESS = wife perceived stress.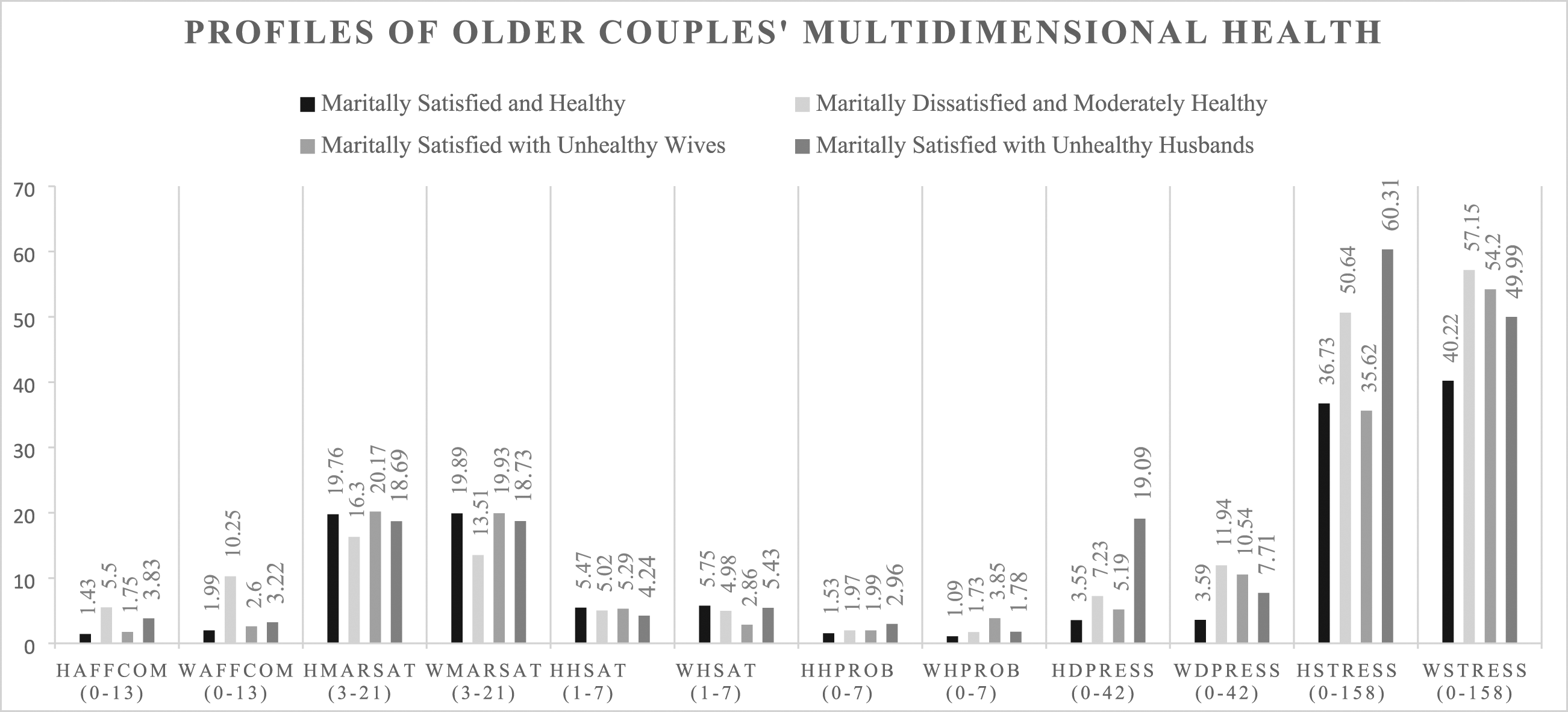
Within-class couple concordance (RQ2)
Within-couple mean difference scores by class with between and within ranking across indicators (N = 535).
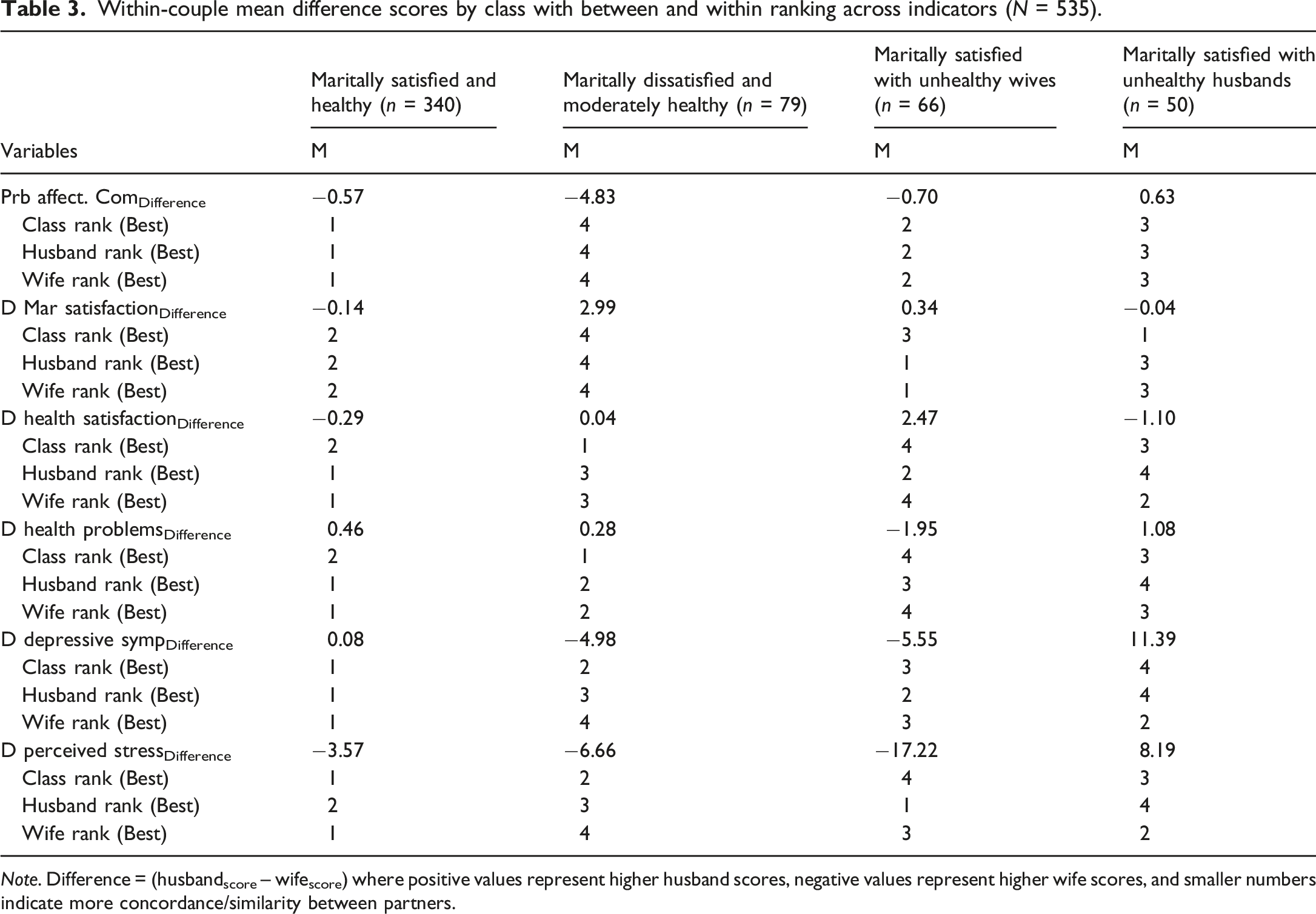
Note. Difference = (husbandscore – wifescore) where positive values represent higher husband scores, negative values represent higher wife scores, and smaller numbers indicate more concordance/similarity between partners.
Demographic associations with profiles (RQ3)
Results from the covariate regression analyses indicated that husband age and education, wife education, and marriage length were significant predictors whereas retirement status was not a significant predictor of profile membership (Supplemental Table 3). Specifically, older husband age was associated with an 8.1% decrease and more husband education was associated with a 15.3% decrease in the odds of being in the Maritally Dissatisfied and Moderately Healthy class compared to the reference class (Maritally Satisfied and Healthy class). More wife education was associated with a 16.0% decrease and longer relationship was associated with a 2.7% decrease in the odds of being in the Maritally Satisfied with Unhealthy Wives class compared to the reference class. Finally, more husband education was associated with a 11.7% decrease in the odds of being in the Maritally Satisfied with Unhealthy Husbands class, relative to the reference group.
Discussion
The present study utilized dyadic data from 535 older, different-sex couples to identify and predict typologies of couples based on psychological, relational, and physical health indicators. Results revealed 4 distinct classes: Maritally Satisfied and Healthy (63.5%), Maritally Dissatisfied and Moderately Healthy (14.7%), Maritally Satisfied with Unhealthy Wives (12.3%), and Maritally Satisfied with Unhealthy Husbands (9.3%). We also found key predictors of class membership and interesting patterns of within-class, between-partner differences on the indicators.
Maritally satisfied and healthy class
Similar to Ko et al.’s (2007) findings, where a majority of the sample belonged to the successful aging group (47% of their sample), our results indicated that over 63% of couples were happy, healthy, and relationally satisfied. The couples in the Maritally Satisfied and Healthy class seemed to fare well in all 12 indicators of class membership, including the best emotional communication, the second highest marital satisfaction, highest health satisfaction, the least health problems, and the lowest depressive symptoms and perceived stress relative to the other classes. These couples also had among the smallest differences between partners across domains, which is again in line with Ko et al.’s (2007). Taken together, perhaps couples in this class fared better because they had lower genetic biological or predispositions for poorer health, which could ultimately set the stage for better interpersonal interactions. Conversely, higher marital satisfaction may have buffered against poorer psychological and physical health, such that their relationship staved off those issues. Regardless, this finding demonstrates that the majority of older couples in a national sample aged successfully and had good physical, relational, and psychological health—at least among those who were well enough to complete the survey and had an intact marital relationship. Importantly, husbands and wives with higher levels of education were more likely to be in the Maritally Satisfied and Healthy class compared to all other classes. Previous research has found more education is associated with better health (Leopold & Engelhartdt, 2013) and better relational functioning (Robles et al., 2014). Thus, it could be that education level could drive differences or membership in this class. Finally, couples who had been together longer were more likely to be in the Maritally Satisfied and Healthy class compared to the Maritally Satisfied with Unhealthy Wives class. This fits with previous literature suggesting concordance is likely greater in longer-term marriages (Kiecolt-Glaser & Wilson, 2017). Likewise, couples in the unhappy class were more discordant, suggesting that people in longer marriages were both happier and more concordant.
Maritally dissatisfied and moderately healthy class
About 15% of the couples in the study were in the Maritally Dissatisfied and Moderately Healthy class, which parallels Ko and colleagues’ (2007) maritally dissatisfied class who functioned well in other domains. These couples were more dissatisfied than all the other couples in the sample, with more problematic affective communication and the lowest marital satisfaction, and mean scores suggesting clinical distress. The wives in this class had the highest rates of depressive symptoms and perceived stress. Across classes, those in this class exhibited the largest differences between partners for both problematic affective communication and marital satisfaction, with wives reporting much more problematic communication and greater dissatisfaction than husbands. It seems that the wives’ psychological well-being in this class tracked most closely with marital distress: depressive symptoms and stress were higher in this class than those in the Unhealthy Wife class. This finding may be explained in two ways. First, perhaps wives’ depressive symptoms and stress make it difficult for couples to engage emotionally and, thus, the relationship suffers (Walker et al., 2013). Alternatively, wives in this class may feel hopeless about their relationship, lacking connection to their partner, which in turn is associated with higher depressive symptoms and stress. This explanation aligns with prior findings that wives are the emotional barometers, i.e., more accurate perceivers of relational difficulties (Doss et al., 2003). Finally, younger husbands were more likely to be in this class than the Maritally Satisfied and Healthy Class. Perhaps couples have not had more experience and success with resolving marital difficulties because they are younger. Thus, in line with socioemotional selectivity theory (Löckenhoff & Carstensen, 2004), couples in this class may have not had time to work through differences—and in this case the wives suffer more psychologically.
Maritally satisfied with unhealthy wives and maritally satisfied with unhealthy husbands classes
The remainder of the sample fell into two classes, Maritally Satisfied with Unhealthy Wives and Maritally Satisfied with Unhealthy Husbands, where one partner had greater psychological and physical health difficulties than the other partner and compared to those in other classes. Nevertheless, they were satisfied in their marriage and had low levels of problematic affective communication. These two classes extend Ko et al.’s (2007) findings to reveal novel discordant classes of couples wherein either the husband or wife is unhealthy. Although the present study did not include whether one partner identified as a caregiver, this pattern tracks with the large and growing number of caregiving dyads. Although prior research has found that poorer physical and psychological well-being is associated with lower marital quality (Iveniuk et al., 2014; Pruchno et al., 2009), these couples demonstrate resilience in their marriage in the face of one partner’s illness, especially through better affective communication, which is in line with socioemotional selectivity theory (Löckenhoff & Carstensen, 2004).
Implications for theory and health promotion, prevention, and intervention
Our findings have important implications for theory and health prevention, promotion, and intervention. First, our findings extend and add nuance to both individual (SST) and dyadic (DGTMS) aging theories. Whereas individual aging theories suggest that with age comes prioritizing emotional, relational, and physical health (SST), our study highlights the unique interplay between the individual’s domains, contextual factors (age, education, SES, etc.), and the dyadic relationship. A majority of the couples in this study aged well together in all domains perhaps either because of ample resources and less contextual challenges or favorable genetic conditions. Other couples in this class faced unique challenges, barriers, and constraints psychologically, physically, or contextually and yet excelled in their companionship goals and relational health. Finally, some had fewer physical, psychological, or contextual challenges yet struggled relationally. Thus, individual theories of aging must fully consider the embeddedness in the socioecological context, rather than conceptualizing them as separate or distinct domains. Dyadic theories of aging should fully consider and identify how individuals in dyads contribute to the physical, psychological, or relational challenges of both partners and the developmental trajectory of the relationship. While these considerations warrant further theoretical development and empirical testing, perhaps successful aging should not be conceptualized as an individual phenomenon but consider the situatedness within long-term social relationships.
Given these implications for theory, our findings underscore the importance of dyadic health promotion, prevention, and intervention. Importantly, many dyadic health frameworks do exist (e.g., Berg & Upchurch, 2007; Lewis et al., 2006), but they have yet to permeate through all aspects of the healthcare field. Our study continues to build a case for true couple-level care and highlight the need for providers to be sensitive to the possibility that a partner may be affected when there is poor mental, physical, or relational health (Siegel et al., 2004). Healthcare providers would do well to (1) screen partners of identified patients, (2) offer referrals for relationship education and couples therapy to target psychological and relational health, and (3) enroll and target both partners in health promotion efforts for systemic collaboration and cooperation between partners (Martire & Helgeson, 2017).
Limitations and directions for future directions
With the cross-sectional design, the current findings reflect between-person and-couple associations; patterns will not necessarily replicate within-persons, over time. Although prior findings of individuals’ longitudinal profiles suggests that most individuals remain in the same subgroup over time (Gerstorf et al., 2006; Lovden et al., 2005), future research should utilize longitudinal data to follow couples’ trajectories and profile membership across the lifespan. The sample also included partners across generational cohorts, thus we were unable to tease out the unique experiences across each. Future research with different birth cohorts is needed to untangle the generational effects and identify successful aging processes in marital dyads.
Although at the time of data collection the sample was representative of the U.S. (compared to Census data) in regard to age, length of marriage, number of children, income, employment, the current sample was still homogeneous in terms of race and ethnicity, with White participants overrepresented and participants of color underrepresented. As such, profile membership may be different in a more diverse sample. Health disparities are increasingly greater and more pronounced. Future research must recruit, be sensitive to, and include more diverse representations of couples. Additionally, more contextual factors should be included as class predictors that may influence how psychological, relational, and physical health disparities play out over time, including neighborhood safety, geographic region and rurality, social network characteristics, and cultural norms (Priest et al., 2020). Importantly, future research should include same-sex couples to determine what profiles exist amongst older sexual minority couples and how patterns diverge from heterosexual couple relationships. Importantly, the present study did not ask about other aspects of identity (disability status, class information, etc.) and future research should assess these domains. The current data were self-reported and therefore subject to response bias. More objective measurement of both relational, psychological, and physical health indicators should be utilized in future research. Further, the present study did not identify whether a partner (or both partners) identified as a spousal caregiver. This can be especially important when partners have discordant health conditions that require separate lifestyle changes (Polenick et al., 2020). Finally, the present sample yielded a small amount of couples retained compared to those recruited, and the generalizability may be limited to those who participated. Participants who are willing to participate in dyadic research are, on average, happier and more relationally satisfied than those who decline to participate (Barton et al., 2020). Future research should use multiple and diverse sampling procedures and identify differences based on recruitment strategy.
Conclusion
The findings from the current study highlight the heterogeneity of older couples’ multidimensional health and how marital satisfaction, psychological, and physical health cluster in divergent ways—concordant in good health and happiness versus discordant between partners. While our study highlights that many couples age successfully, other couples may need more intervention in one or more domains. We hope these results will spur more couple-level data analytic approaches in identifying patterns, predictors, and trajectories of successful aging.
Supplemental Material
Supplemental Material - Aging together: Dyadic profiles of older couples’ marital quality, psychological well-being, and physical health
Supplemental Material for Aging together: Dyadic profiles of older couples’ marital quality, psychological well-being, and physical health by Josh R Novak, Stephanie J Wilson, Ashley E Ermer and James M Harper in Journal of Social and Personal Relationships
Footnotes
Author’s note
Josh R. Novak is an assistant professor in the Department of Human Development and Family Studies at Auburn University. Stephanie J. Wilson is an assistant professor in the Department of Psychology at Southern Methodist University. Ashley E. Ermer is an assistant professor in the department of Family Science and Human Development at Montclair State University. James M. Harper is emeritus professor in the School of Family Life at Brigham Young University.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Alabama Agricultural Experiment Station and the Hatch program of the National Institute of Food and Agriculture, U.S. Department of Agriculture, and the National Institute on Aging (R00 AG056667).
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly or individually shared because it was not approved by the individual participants nor the university conducting the original research. The materials used in the research cannot be publicly shared but are available upon request, including syntax files (input and output) and an explanatory memo. The materials can be obtained by emailing:
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.