
Abstract
Research has increasingly recognized the links of communal coping—a shared appraisal of a stressor and collaborative action to manage it—to positive adjustment outcomes in chronic illness. However, past literature rarely examines if these two components have unique links to relationship and health outcomes, if one component is more strongly linked than the other component to these outcomes, or if the two components interact to influence outcomes. Additionally, the impact of shared appraisal and collaboration may depend on the source—the patient or the romantic partner. In a study of 200 patients with newly diagnosed type 2 diabetes and their spouses, daily reports of shared appraisal and collaboration, mood, support interactions, and patient self-care were collected over 14 consecutive days. Multi-level modeling showed that both patient and spouse reports of shared appraisal and collaboration were linked independently to support interactions and better mood for patients and spouses, while collaboration alone was linked to self-care. Further, collaboration was generally more strongly linked to behavioral outcomes—support and self-care—than shared appraisal, while links to mood were similar for shared appraisal and collaboration. Shared appraisal and collaboration also interacted such that shared appraisal was particularly beneficial for those who reported low collaboration. Finally, results suggested one’s own reports of shared appraisal and collaboration were more strongly linked to outcomes than partner reports. Overall, these findings demonstrate unique impacts of daily shared appraisal and collaboration on adjustment to chronic illness for patients and spouses.
The number of individuals in the United States coping with a chronic illness is a significant public health concern. To date, 24.3 million people are living with cardiovascular disease or lasting effects of a heart attack (Benjamin et al., 2019), and 34.2 million people are living with diabetes (Centers for Disease Control and Prevention, 2020). Management of these conditions is difficult due to the considerable lifestyle changes required, including dietary modifications, an exercise regimen, taking medication, and monitoring progression of the illness. Given the scope of these changes, the romantic partners of individuals with chronic illness are often affected as well. For example, spouses of persons with chronic illness may experience increased psychological distress and greater caregiving responsibilities (Rees et al., 2001).
Not only are romantic partners affected by a chronic illness, but partner involvement in management tends to have benefits for both couple members. One theory that demonstrates how partner involvement can help both couple members is communal coping. According to communal coping theory, persons benefit when they (1) appraise the illness as a shared problem and (2) collaborate with a partner to manage it (Helgeson et al., 2018; Lyons et al., 1998). Prior communal coping research has consistently demonstrated positive psychological and behavioral health outcomes across multiple contexts, including stressors that are collectively experienced by communities (e.g., refugee camps and natural disasters; Afifi et al., 2012, 2016) and stressors that are experienced by only one couple member (e.g., alcohol use disorders and diabetes; Helgeson et al., 2017; Rentscher et al., 2017). However, past literature has typically examined communal coping as a single construct and rarely examined the distinct effects of shared appraisal and collaboration on health. When examined within the same model, one component may have a stronger influence on health than the other; it may also be the case that these two components interact with each other to affect health. Further, within the context of chronic illness, the influence of these components may depend on who is engaging in shared appraisal or collaboration—the patient or their romantic partner. For example, romantic partner collaboration may play a more significant role in patient health than patient collaboration because partner collaboration indicates the provision of additional resources to the patient.
Given these gaps in the literature, the current investigation sought to elucidate the unique links between the two components of communal coping and daily illness management with three aims. First, we disentangled the effects of shared appraisal and collaboration by examining whether they were independently linked to relational and behavioral health outcomes within the same model. If they both independently predicted outcomes, we next determined whether shared appraisal or collaboration was more strongly associated with these outcomes. Second, we examined the interaction between shared appraisal and collaboration to determine if there was a synergistic effect between the two. Third, we examined whether patient shared appraisal/collaboration or spouse shared appraisal/collaboration were more strongly linked to outcomes. Below, we review prior literature relevant to each aim and introduce the current study.
Links of Shared Appraisal and Collaboration to Chronic Illness Management
Many studies that examine communal coping and health measure communal coping holistically without distinguishing between shared appraisal and collaboration (e.g., Van Vleet et al., 2018; Zajdel et al., 2018). Other studies focus on the effects of a single component—either shared appraisal (Karan et al., 2019; Rohrbaugh et al., 2008) or collaboration (Berg & Upchurch, 2007; Johnson et al., 2013). However, it is important to examine both components of communal coping because they may have unique effects on health outcomes, as suggested by emerging research. For example, in a cross-sectional analysis on the current sample, patient and spouse shared appraisal and collaboration were independently linked to reduced psychological distress and enhanced patient self-care (Zajdel & Helgeson, 2020). Additionally, a study of individuals with type 1 diabetes and their spouses showed that daily collaboration was linked to negative outcomes (e.g., higher blood glucose), while daily shared appraisal was linked to positive outcomes (e.g., better self-care; Berg et al., 2020). A multi-method analysis with this same sample indicated similar findings—that collaboration in the absence of shared appraisal was detrimental to health (Zajdel et al., 2022). Theoretical work also suggests that distinguishing the unique effects of shared appraisal and collaboration is important because they may have differential impacts on intermediary outcomes that influence distal health outcomes (Rentscher, 2019). For example, shared appraisal may have a stronger impact on allostatic processes, whereas collaboration may have a stronger impact on health behaviors.
Thus, the first study aim was to examine whether shared appraisal and collaboration are independently associated with relationship and health outcomes for individuals with type 2 diabetes and their spouses on a daily basis. We predicted that daily shared appraisal would be independently linked to more support interactions, better diabetes self-care, and better mood. Daily shared appraisal represents joint ownership over illness management, which should result in greater support provision from the spouse and increased recognition of support receipt from the patient (e.g., Helgeson et al., 2018). Additionally, viewing diabetes as a shared responsibility should result in a greater pool of resources from which the patient can draw, thus enhancing patient self-care behaviors. Finally, shared appraisal should result in better mood for both patients and spouses by reducing secondary stress appraisals associated with diabetes management in line with individual theories of stress and coping (Lazarus & Folkman, 1984).
We also hypothesized that collaboration would be independently linked to these same outcomes. Collaboration, the behavioral component, is likely linked to support and self-care because these are tangible behavioral actions that couple members can engage in to cope with and manage diabetes. Again drawing from individual theories of coping (Lazarus & Folkman, 1984), collaboration may be linked to better mood because distress should be reduced when couple members enact coping behaviors to address the stressor. We note that the majority of research has focused on patient outcomes, but appraisal and collaboration likely affect the spouse as well. Thus, we predicted similar links of daily shared appraisal and collaboration to both patient and spouse outcomes.
To further explore this research aim, we also compared the effects of shared appraisal to the effects of collaboration to determine if one component was more strongly linked than the other component to outcomes. Given limited past empirical evidence, we cautiously predicted that collaboration, the behavioral component of communal coping, would be more strongly linked to the behavioral outcomes—support and self-care, in line with existing theory (Rentscher, 2019). However, because both cognitive appraisals and behavioral coping mechanisms are expected to influence stress/distress within traditional models of coping (e.g., Lazarus & Folkman, 1984), we did not predict differences in the links of shared appraisal and collaboration to daily mood.
In our second study aim, we further elucidated the roles of shared appraisal and collaboration by examining the interaction between these components. We viewed this aim as exploratory because there is theoretical rationale for multiple patterns of interactions. First, the combination of high shared appraisal and high collaboration might confer greater benefits to health than a mere summative effect. Alternatively, high scores on one component of communal coping might buffer one from low scores on the other component of communal coping. For example, high shared appraisal might be particularly beneficial for individuals who do not collaborate, or collaboration might be particularly beneficial for individuals who do not hold a shared appraisal. Lastly, it may also be possible that one component is sufficient, and there are not interactive effects between shared appraisal and collaboration. Because previous research has traditionally focused on only a single component of communal coping, the extant empirical evidence does not suggest a particular pattern of interaction.
The Importance of Relationship Role: Patient Versus Spouse
The third study aim was to examine whether patient or spouse shared appraisal/collaboration were more strongly linked to outcomes. Although communal coping represents a dyadic phenomenon, it has largely been measured at the individual level because couple members may have different views regarding whether illness management is a shared problem or whether their relationship interactions are collaborative in nature. However, a meta-analytic review of linguistic “we-talk” (a marker of shared appraisal) showed stronger links of spouse than patient we-talk to relationship outcomes (Karan et al., 2019). Spouse shared appraisal may exert a stronger influence than patient shared appraisal because spouse shared appraisal is an indicator of spouse involvement in diabetes management. This supposition is consistent with the finding that links of spouse we-talk to good patient outcomes were mediated by patient perceptions of spouse support among individuals with type 1 diabetes and their spouses (Lee et al., 2020b).
To date, there are no studies that directly compare the relative strength of patient versus spouse collaboration to relationship and health outcomes. However, spouse collaboration might be more strongly linked to both patient and spouse relationship and health outcomes because it may signal that the spouse is providing increased resources for patient diabetes management. Given the findings from past studies, we tentatively hypothesize that spouse shared appraisal and spouse collaboration would be more strongly related than patient appraisal/collaboration to outcomes.
The Current Study
In this study, we used a daily diary design to examine the relations of shared appraisal and collaboration to: (1) patient and spouse reports of spouse supportive behavior, (2) patient and spouse reports of patient diabetes self-care behaviors, and (3) patient and spouse mood. Daily diary data permit a more immediate, in-the-moment assessment of the links of an individual’s thoughts and behaviors to relationship and health outcomes than in previous communal coping studies which primarily involve cross-sectional reports. The study expands on an earlier daily diary report that used a subsample of the current study (n = 123; Zajdel et al., 2018) in four ways: (1) we examined findings for the full sample of couples (n = 200), (2) we compared the independent links of shared appraisal and collaboration to outcomes, (3) we explored the potential interactive effects of shared appraisal and collaboration, and (4) we examined whether patient or spouse effects of shared appraisal/collaboration significantly differed from one another.
We conducted this research with individuals who were newly diagnosed with type 2 diabetes, a time at which daily communal coping may be particularly important as couples navigate their new lifestyles. Participants were recruited from the community using a range of outreach methods (e.g., public bus routes) rather a single recruitment source, resulting in a sample that was diverse with respect to education, income, and race. In this study we aimed to recruit roughly equal numbers of Black and White individuals because type 2 diabetes disproportionately impacts non-Hispanic Black individuals (CDC, 2020) and previous couples-based research is often focused on White couples (Williamson et al., 2022). Thus, we view the diverse community-based sample as a particularly important strength because the majority of previous relationship research is based on middle-class White couples. Given the diverse sample, we examined whether race was a moderator of the links of shared appraisal and collaboration to outcomes. However, we view these analyses as exploratory because we had no a priori hypotheses and because the primary goal was to examine the links of communal coping components to health outcomes.
Method
Participants
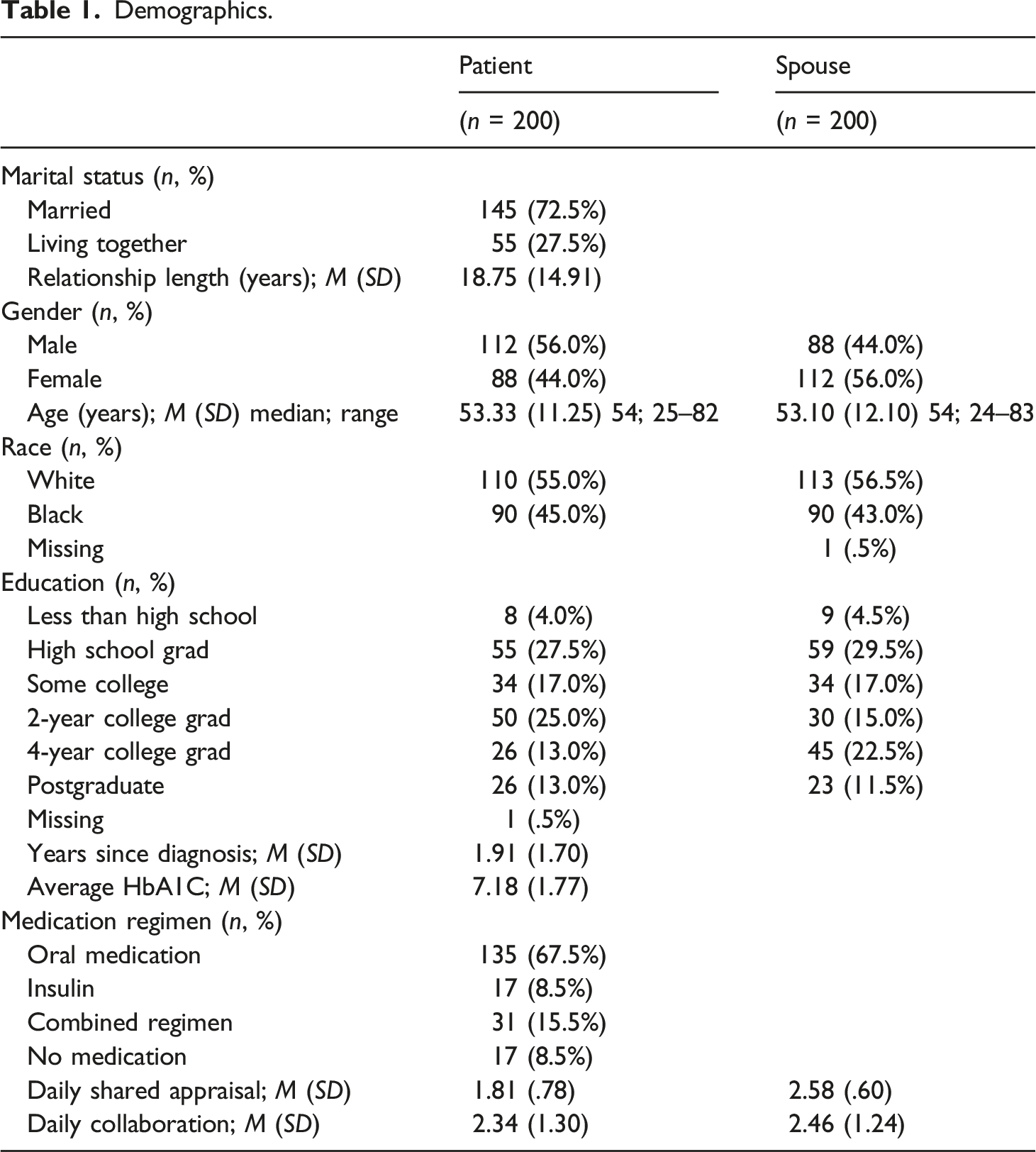
Demographics.
Recruitment
Participants were recruited from the community (i.e., community health fairs, mass media advertising, public bus advertisements, brochures in physician offices). Individuals had to have been diagnosed with type 2 diabetes within the past 5 years, not have another illness that affected their daily life more than diabetes (e.g., cancer), have a partner who did not have diabetes, and be married or cohabiting in a marital-type relationship for at least 2 years. Of the 658 individuals who contacted us, 419 were not eligible, largely because they were diagnosed more than 5 years ago. Further recruitment details are reported elsewhere (see Helgeson et al., 2017). Of the final 207 couples, seven couples were dropped from the analyses: three participants completed several surveys on the same day, two participants lost the iPads given to complete the surveys, one participant experienced a death in the family which prevented completion of the surveys, and one participant accidently erased data from the surveys. This resulted in a final sample of 200 couples.
Procedure
The study had several components, including an in-person interview and a 14-day daily diary protocol. Patients and spouses were each paid $50 for the in-person interview and $100 for the daily diary protocol. For the in-person interview, participants had the choice of being interviewed in their homes (72%) or at Carnegie Mellon University with mileage reimbursement (28%). The interview consisted of questionnaires, a videotaped discussion, and physical health measures. However, the current paper focuses on the daily diary protocol, described below.
Patients and spouses were each provided an iPad to complete questionnaires separately at the end of the day for 14 consecutive days. The questionnaires measured communal coping, support interactions, diabetes self-care behaviors, and mood (described below). Both patients and spouses completed an average of 12.24 (SD = 1.97) of the 14 daily diaries, which indicated good compliance. Of the days in which participants started the daily survey, there were no missing data on any of the main independent or dependent variables except for patient reports of perceived partner responsiveness (.12%; 3 cases) and spouse reports of patient diet (.04%; 1 case). Missing cases for patient reports of perceived partner responsiveness were imputed based on the control variables and independent variables used in our main models; however, the missing case for spouse report of patient diet was not able to be imputed because the patient did not complete the survey on that day (i.e., no patient report of daily shared appraisal or daily collaboration to use as predictors when imputing the missing case).
Measures
Demographic information was collected during the initial session. These variables included patient and spouse gender (0 = male, 1 = female), race (0 = White, 1 = Black), age, work status (0 = not currently working, 1 = currently working), education (1 = less than high school, 2 = high school graduate, 3 = some college, 4 = 2-year college graduate, 5 = 4-year college graduate, 6 = post-graduate degree), number of children, relationship length in years, and income (<$20,000 to over $100,000, with $10,000 increments between the two). Patient HbA1c was collected using the DCA Advantage Analyzer, years since diagnosis was calculated from the date of the in-person session using physician-verified date of diagnosis, and insulin status was categorized as 0 = not using insulin and 1 = using insulin.
All daily assessments were completed by both patient and spouse unless otherwise noted. We used brief versions of the in-person questionnaires to reduce burden. Where scales had two items, we used traditional multilevel modeling to determine the relationship between the items. Where scales had three or more items, we used variance component analysis to determine the reliability (Bolger & Laurenceau, 2013). Measures with more than two items and good reliability were averaged to create a mean score (e.g., mood).
Communal Coping
Shared Appraisal
Shared appraisal was measured by the item, “When you thought about diabetes today, did you view diabetes as ‘our problem’ (shared equally by you and your partner) or mainly your own problem?” (Lyons et al., 1998; Zajdel et al., 2018). Patients and spouses answered using the following options: “completely my partner’s problem,” “mostly my partner’s problem,” “both of our problem,” “mostly my problem,” and “completely my problem.” Because there were very few patients who choose “mainly my partner’s problem” (.6%) or “completely my partner’s problem” (.1%) and very few spouses who chose “mainly my problem” (1.1%) or “completely my problem” (.7%), we chose to recode these responses. Responses were rescored as 1 = non-communal appraisal (“completely my problem” or “completely my partner’s problem”), 2 = partly communal appraisal (“mostly my problem” and “mostly my partner’s problem”), and 3 = communal appraisal (“both of our problem”). Mean patient appraisal was 1.81 (SD = .78), and mean spouse appraisal was 2.58 (SD = .60).
Collaboration
Collaboration was measured by the item, “How much did you and your partner work together to take care of diabetes?” (Lyons et al., 1998; Zajdel et al., 2018). The five-point response scale ranged from 1 = “not at all” to 5 = “all of the time.” Mean patient collaboration was 2.34 (SD = 1.30), and mean spouse collaboration was 2.46 (SD = 1.24).
Partner Supportive Behavior
Instrumental Support
Patients were asked to respond to the following: “My partner helped me figure out how to take care of diabetes” and “My partner suggested things that might help me manage diabetes” from the Diabetes Family Behavior Checklist (Schafer et al., 1983). Spouses responded to the same items with modifications to reflect support provision (e.g., “I helped my partner figure out how to take care of diabetes”). The response scale ranged from 1 = “none of the time” to 4 = “most of the time.” These two items were strongly related to each other (patients: B = .53, p < .001, spouses: B = .49, p < .001).
Emotional Support
Patients were asked to think about their diabetes that day and respond to the following: “My partner was there for me by giving me his/her undivided attention”, “My partner tried to understand my situation”, and “My partner pointed out my strengths in managing diabetes” from the Emotional Support Scale (Fekete et al., 2007). Spouses responded to the same items with modifications to reflect support provision (e.g., “I tried to understand my partner’s situation”). The four-point response scale ranged from 1 = “none” to 4 = “most”. Reliability was good (patients: α = .56, spouses: α = .51).
Perceived Emotional Responsiveness
Patients were asked to think about how their spouse responded to them with respect to diabetes and indicate how much they felt understood, supported, judged, and ignored from the Perceived Emotional Responsiveness scale (Fekete et al., 2007). “Judged” and “ignored” were reverse scored, and the items were averaged (α = .66). Spouses were asked to think about how the patient responded to them that day with respect to diabetes and indicate how much they felt appreciated, ignored, helpful, or frustrated. “Ignored” and “frustrated” were reverse scored, and the four items were averaged into an index (α = .64). The response scale ranged from 1 = “not at all” to 4 = “a lot”.
Diabetes Self-Care Behaviors
Patients were asked: (1) “How much did you follow your diet today?” (1 = “not at all” to 5 = “very much”); (2) “Did you exercise today?” (“yes”, “no”); and (3) “Did you test your blood sugar today?” (“yes”, “no”). Spouses were asked: (1) “How much did your partner follow his/her diet today?” (1 = “not at all” to 5 = “very much” or “don’t know”); and (2) “Did your partner test his/her blood glucose today?” (“yes”, “no”, “don’t know”). Days in which the spouse responded with “don’t know” were excluded from analyses. Because these items demonstrated low reliability for patients (patient: α = .21; spouse: α = .45), all items were analyzed separately.
Mood
Depressed mood (sad, depressed, unhappy) and happy mood (happy, pleased, cheerful) were measured with six items from the Profile of Mood States (Usala & Hertzog, 1989). Three face-valid items were developed to measure angry mood (angry, annoyed, mad; Zajdel et al., 2018). Both patients and spouses rated each item from 1 = “not at all” to 5 = “a lot of the time” regarding how they felt over the course of the day. Internal consistencies were high for depressed mood (patients: α = .79, spouses: α = .75), happy mood (patients: α = .78; spouses: α = .79), and angry mood (patients: α = .81; spouses: α = .79).
Overview of Analyses
Prior to the main analyses, demographic and illness variables were examined to determine relations to both the independent variables (daily shared appraisal, daily collaboration) and outcomes of interest. Patient gender, patient race, spouse work status, spouse education, household income, and whether the patient was on insulin were significantly or marginally related to both the independent variables and outcome variables. Thus, we simultaneously examined the relations of this reduced set of demographic variables to the independent variables and outcome variables, eliminating demographic variables from the models one at a time if effects were not significant. Results showed that patient gender, spouse work status, spouse education, and household income were related to both the independent variables and outcome variables and were therefore controlled in subsequent analyses. Day was also included as a covariate to control for the effect of time; however, we did not control for weekday versus weekend because we did not collect this information. Full models for each analysis (including covariates) can be found in the Online Supplemental Material.
Multilevel modeling was used to account for the nesting of days within persons. We first ran a series of null hierarchical models for each dependent variable to confirm there was sufficient variation in the outcomes to proceed with analyses (>10% due to within-day variation). As suggested by Bolger and Laurenceau (2013), we calculated within-person (WP) and between-person (BP) effects for appraisal and collaboration to control for between-person variance in our examination of the daily (within-person) effects. WP variables were created by subtracting an individual’s average score from their score on a given day. BP variables were calculated by using the individual’s average shared appraisal/collaboration. All models report both WP and BP effects for shared appraisal and collaboration, but the focus of this research—and daily diary research in general—is on the effect of WP variables.
In our data, we had two sets of outcome variables: (1) outcomes that are unique to patient versus spouse role (e.g., receipt of support vs. support provision) and (2) outcomes that are the same for both patients and spouses (e.g., mood).
Outcomes Unique to Patient versus Spouse
Effects of Patient and Spouse Appraisal and Collaboration on Patient Support Receipt and Self-Care Behaviors.
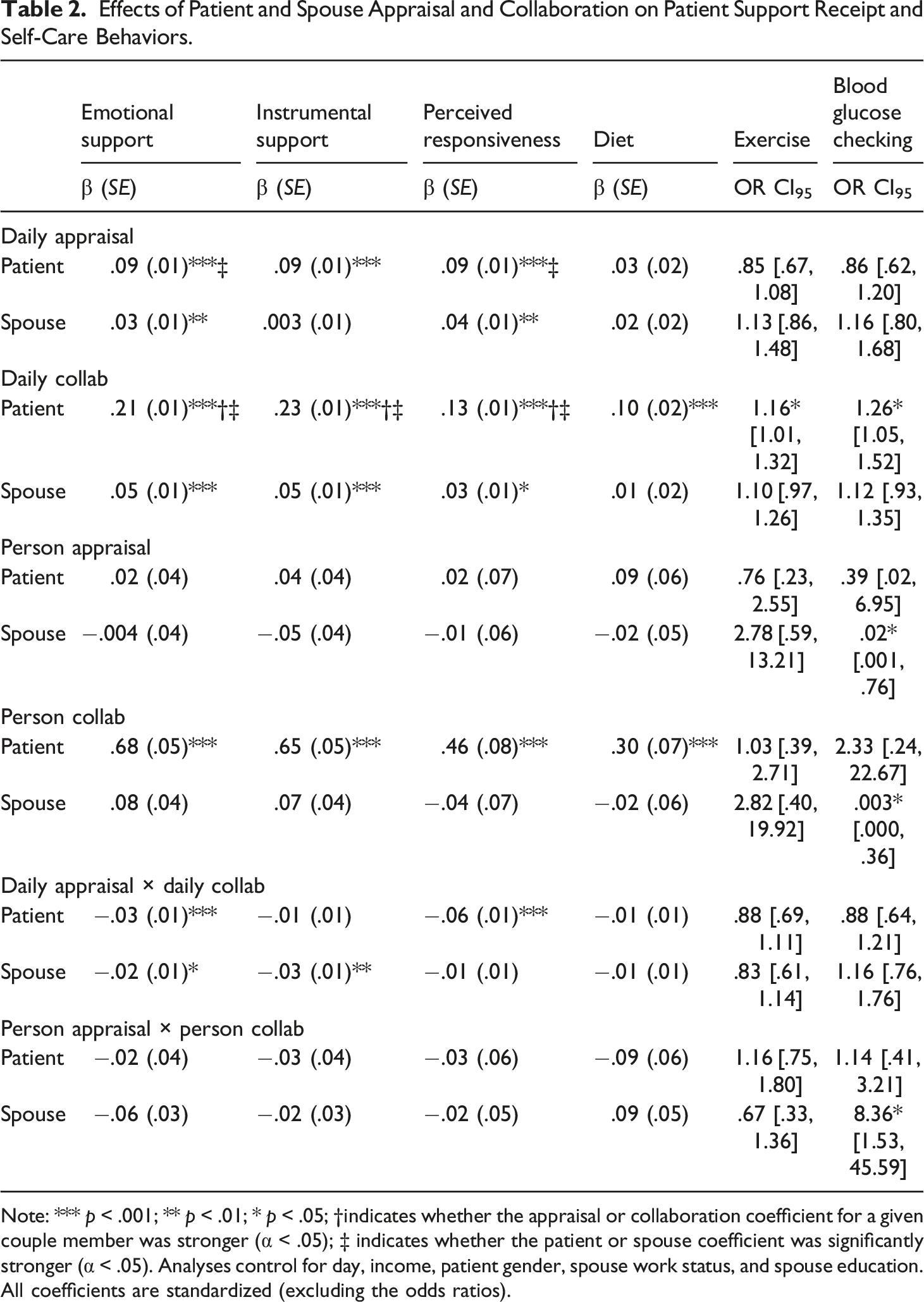
Note: *** p < .001; ** p < .01; * p < .05; †indicates whether the appraisal or collaboration coefficient for a given couple member was stronger (α < .05); ‡ indicates whether the patient or spouse coefficient was significantly stronger (α < .05). Analyses control for day, income, patient gender, spouse work status, and spouse education. All coefficients are standardized (excluding the odds ratios).
Effects of Patient and Spouse Appraisal and Collaboration on Spouse Support Provision and Self-Care Behaviors.
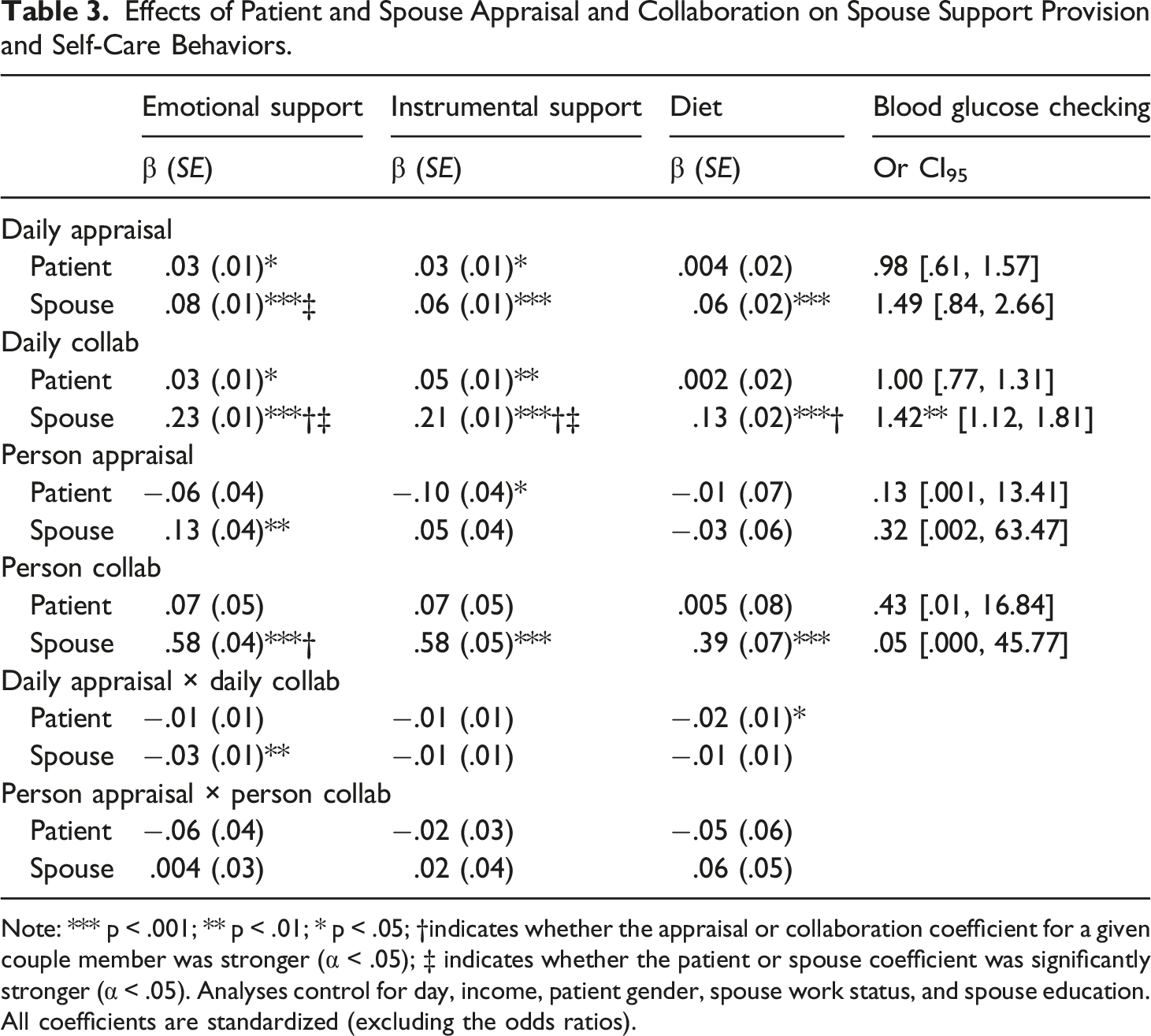
Note: *** p < .001; ** p < .01; * p < .05; †indicates whether the appraisal or collaboration coefficient for a given couple member was stronger (α < .05); ‡ indicates whether the patient or spouse coefficient was significantly stronger (α < .05). Analyses control for day, income, patient gender, spouse work status, and spouse education. All coefficients are standardized (excluding the odds ratios).
To address the second aim, we examined whether shared appraisal and collaboration interacted to predict outcomes (Tables 2 and 3). When interactions were significant, we also performed simple slopes analyses to determine whether slopes were significantly different from zero. Finally, to address the third aim (compare patient vs. spouse effects), when both patient and spouse effects for appraisal or collaboration were significant, we used z-score tests to compare the strength of the coefficients between patients and spouses (Tables 2 and 3).
Outcomes Common to Patients and Spouses
Effects of Patient and Spouse Appraisal and Collaboration on Patient Mood.
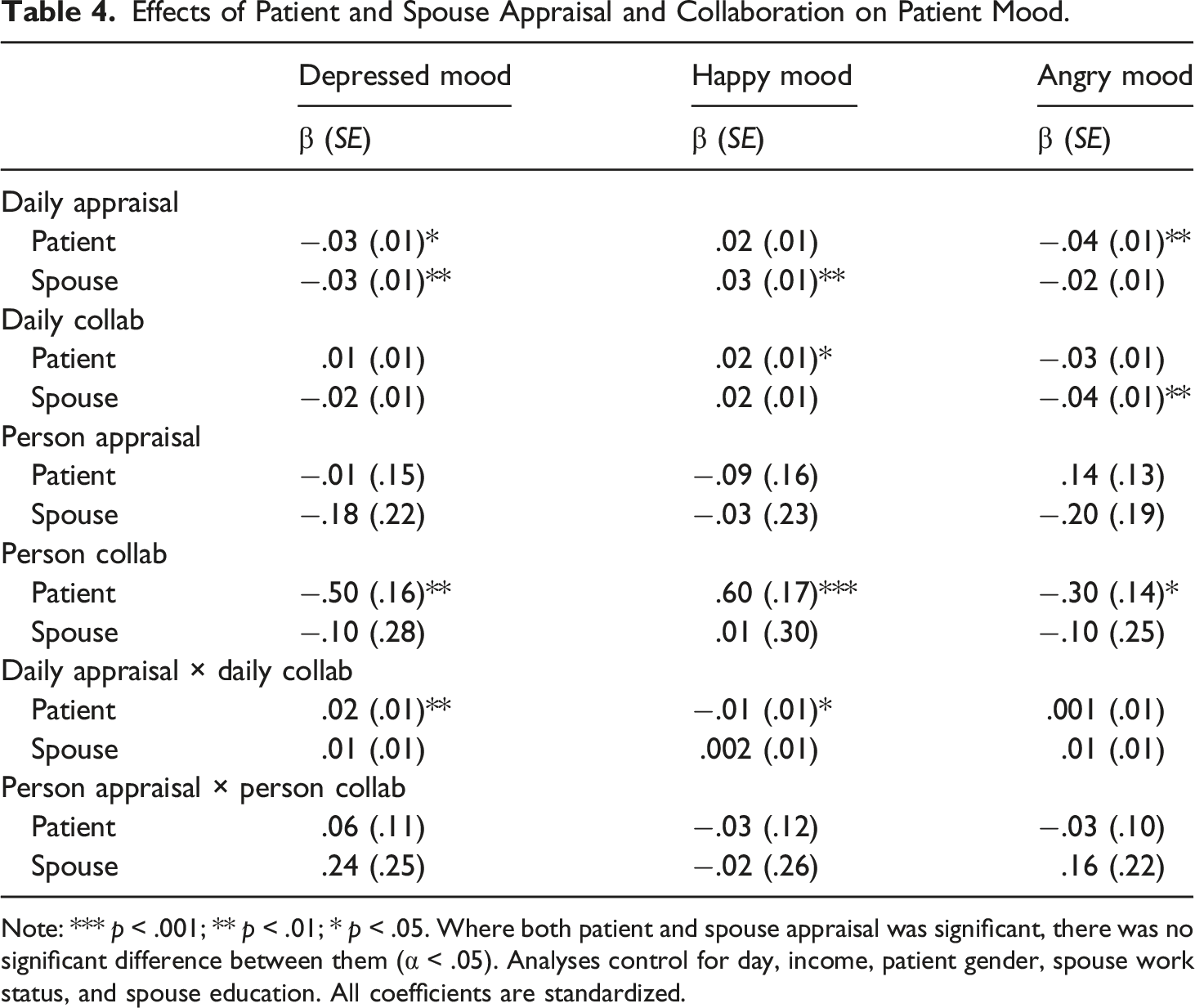
Note: *** p < .001; ** p < .01; * p < .05. Where both patient and spouse appraisal was significant, there was no significant difference between them (α < .05). Analyses control for day, income, patient gender, spouse work status, and spouse education. All coefficients are standardized.
Effects of Patient and Spouse Appraisal and Collaboration on Spouse Mood.
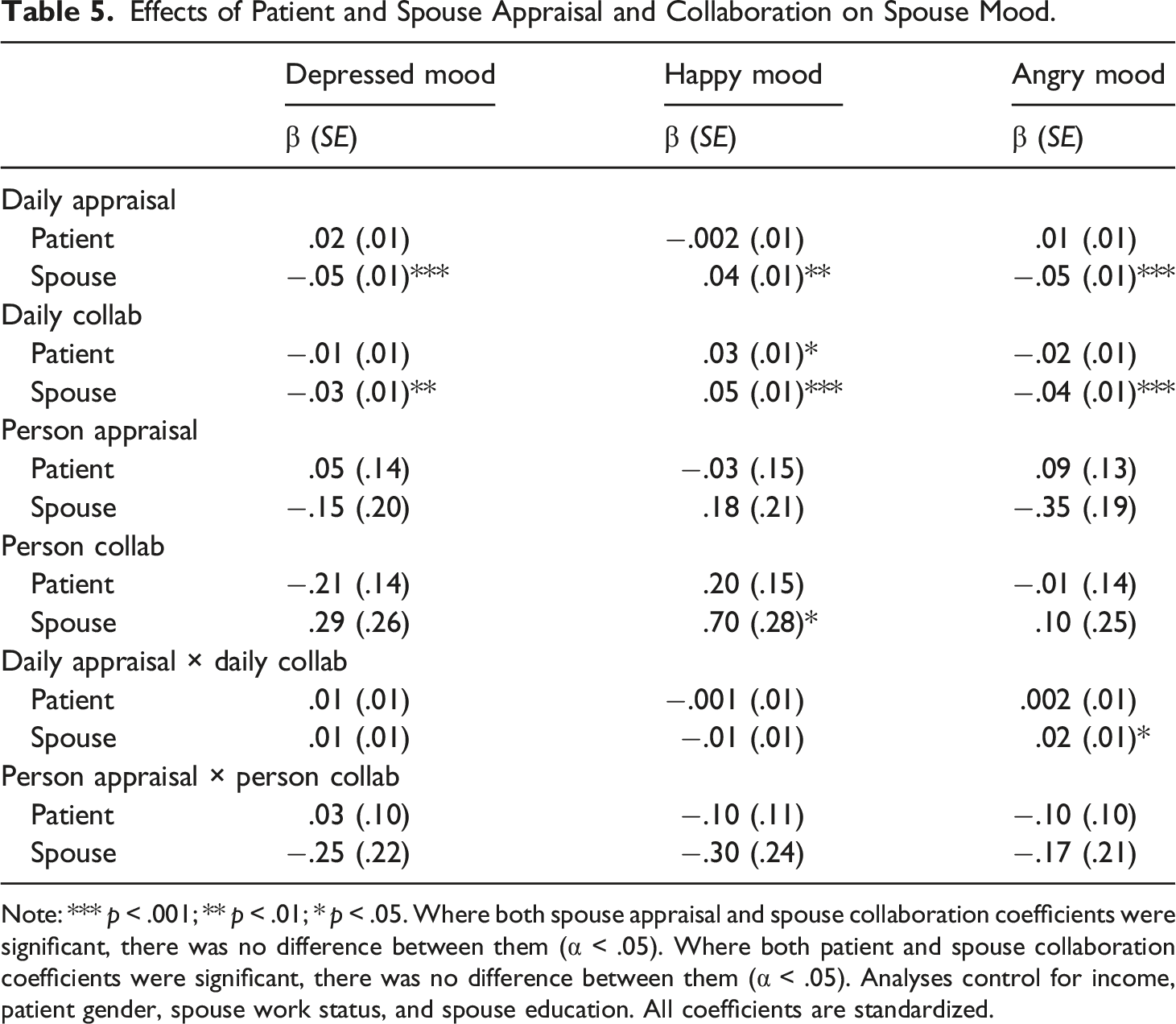
Note: *** p < .001; ** p < .01; * p < .05. Where both spouse appraisal and spouse collaboration coefficients were significant, there was no difference between them (α < .05). Where both patient and spouse collaboration coefficients were significant, there was no difference between them (α < .05). Analyses control for income, patient gender, spouse work status, and spouse education. All coefficients are standardized.
Results
Effects of Appraisal and Collaboration on Daily Support Interactions
Patient Outcomes
Aim 1
As shown in Table 2, patient daily shared appraisal was related to increased patient emotional support receipt, instrumental support receipt, and perceived emotional responsiveness. Spouse daily shared appraisal was related to increased patient emotional support receipt and perceived responsiveness, but not instrumental support receipt. Both patient daily collaboration and spouse daily collaboration were significantly related to increased patient emotional support receipt, instrumental support receipt, and perceived emotional responsiveness. Results largely generalized across patient race (Supplemental Table 3), with two exceptions: there was a race by patient daily appraisal interaction and a race by patient daily collaboration interaction for perceived responsiveness. Simple slopes analyses showed that there was a stronger relation between patient daily appraisal and perceived responsiveness (β = .10, p < .001) and between patient daily collaboration and perceived responsiveness (β = .18, p < .001) for Black individuals than White individuals (β = .05, p = .013, and β = .09, p < .001, respectively).
A comparison of the patient daily appraisal and daily collaboration coefficients revealed that patient daily collaboration was stronger than the effect of patient daily shared appraisal for emotional support receipt (z = −7.22, p < .001), instrumental support receipt (z = −7.20, p < .001), and perceived responsiveness (z = −2.02, p = .04). However, a comparison of the spouse daily shared appraisal and daily collaboration coefficients revealed that these effects were not significantly different for emotional support receipt (z = −.91, p = .36) or perceived responsiveness (z = .19, p = .84).
Aim 2
There were significant interactions between patient daily appraisal and patient daily collaboration for emotional support receipt (Supplemental Figure 1) and perceived responsiveness (Supplemental Figure 2). Both interactions showed that patient daily shared appraisal was more strongly related to patient reports of emotional support receipt and perceived responsiveness when patient daily collaboration was low than high. In other words, shared appraisal appeared to be more strongly linked to relational outcomes when there was less collaboration.
There were also significant interactions between spouse daily appraisal and spouse daily collaboration for emotional support receipt (Supplemental Figure 3) and instrumental support receipt (Supplemental Figure 4). Both interactions showed that spouse daily shared appraisal was more strongly related to patient reports of emotional support receipt and instrumental support receipt when spouse daily collaboration was low than high. Again, these findings suggest that shared appraisal appeared to be more strongly linked to relational outcomes when there was less collaboration.
Aim 3
A comparison of the patient and spouse daily shared appraisal coefficients revealed that the effect for patient daily shared appraisal was stronger than the effect for spouse daily shared appraisal for emotional support receipt (z = 3.76, p < .001) and perceived responsiveness (z = 3.09, p = .002). A comparison of the patient and spouse daily collaboration coefficients revealed that the effect of patient daily collaboration was stronger than the effect of spouse daily collaboration on emotional support receipt (z = 10.15, p < .001), instrumental support receipt (z = 9.85, p < .001), and perceived responsiveness (z = 5.17, p < .001).
Spouse Outcomes
Aim 1
As shown in Table 3, patient daily shared appraisal and spouse daily shared appraisal were significantly related to increased spouse emotional support provision and instrumental support provision. Only spouse daily shared appraisal was related to spouse perceived emotional responsiveness. Both patient daily collaboration and spouse daily collaboration were significantly related to increased spouse emotional support provision, instrumental support provision, and perceived emotional responsiveness. These results largely generalized across patient race (Supplemental Table 4), except for one interaction between race and spouse daily appraisal for perceived responsiveness: for Black individuals, there was a stronger relation between spouse daily appraisal and perceived responsiveness (β = .10, p < .001) than for White individuals (β = .05, p = .015).
A comparison of the patient daily shared appraisal and daily collaboration coefficients revealed that the effects were not significantly different for emotional support provision (z = −.16, p = .87) or instrumental support provision (z = −.75, p = .45). However, a comparison of the spouse daily shared appraisal and daily collaboration coefficients revealed that the effect of spouse daily collaboration was stronger than the effect of spouse daily shared appraisal for emotional support provision (z = −8.69, p < .001), instrumental support provision (z = −7.79, p < .001), and perceived responsiveness (z = −3.81, p < .001).
Aim 2
There were no significant interactions between patient daily appraisal and patient daily collaboration for spouse emotional support provision, instrumental support provision, or perceived responsiveness. However, there were significant interactions between spouse daily appraisal and spouse daily collaboration for spouse emotional support provision (Supplemental Figure 5) and perceived responsiveness (Supplemental Figure 6). Both interactions showed that spouse daily shared appraisal was more strongly related to spouse reports of emotional support provision and perceived responsiveness when spouse daily collaboration was low than high. These findings suggest that shared appraisal seemed to be more strongly linked to relational outcomes when there was less collaboration.
Aim 3
A comparison of the patient and spouse daily appraisal coefficients revealed that the effect of spouse daily shared appraisal was stronger than the effect of patient daily shared appraisal for emotional support provision (z = −3.09, p = .002), but the effects did not significantly differ for instrumental support provision (z = −1.46, p = .14). A comparison of the patient and spouse daily collaboration coefficients revealed that the effect of spouse daily collaboration was stronger than the effect of patient daily collaboration for emotional support provision (z = −11.29, p < .001), instrumental support provision (z = −8.27, p < .001), and perceived responsiveness (z = −5.35, p < .001).
Effects of Appraisal and Collaboration on Daily Self-Care
Patient Outcomes
Aim 1
Neither patient daily shared appraisal nor spouse daily shared appraisal were related to patient reports of dietary adherence, exercise, or blood glucose checking (Table 2). Patient daily collaboration was related to patient reports of increased diet adherence and an increased likelihood of patients reporting exercise adherence and blood glucose checking. Spouse daily collaboration was not related to patient reports of any of the three self-care behaviors. These results largely generalized across patient race (Supplemental Table 3), with two exceptions. First, there was an interaction between race and patient daily collaboration for diet adherence: for Black individuals, there was a stronger relation between patient daily collaboration and diet adherence (β = .13, p < .001) than for White individuals (β = .06, p < .001). Second, there was an interaction between race and spouse daily collaboration for blood glucose checking: there was no relation between spouse daily collaboration and likelihood of blood glucose checking for Black individuals (OR = .89, 95% CI [-.67, 1.17]), but spouse daily collaboration was associated with an increased likelihood of blood glucose checking for White individuals (OR = 1.34, 95% CI [1.04, 1.73]).
Because there were no models in which both daily shared appraisal and daily collaboration were significantly linked to outcomes, we did not compare coefficients.
Aim 2
There were no interactions between patient daily appraisal and patient daily collaboration for patient self-care behaviors. There were also no interactions between spouse daily appraisal and spouse daily collaboration for patient self-care behaviors.
Aim 3
Because there were no models in which both patient and spouse predictors were significantly linked to self-care outcomes, we did not compare coefficients.
Spouse Outcomes
Aim 1
Patient daily shared appraisal was unrelated to spouse reports of patient dietary adherence or blood glucose checking (Table 3). Spouse daily shared appraisal was significantly related to increased spouse reports of patient diet but was unrelated to blood glucose checking. Patient daily collaboration was not related to spouse reports of patient dietary adherence or blood glucose checking. In contrast, spouse daily collaboration was significantly related to a higher likelihood of spouse reports of patient dietary adherence and blood glucose checking. These results were not moderated by patient race (Supplemental Table 4).
A comparison of the spouse daily shared appraisal and spouse daily collaboration coefficients revealed that the effect of spouse daily collaboration was stronger than the effect of spouse shared appraisal for spouse reports of patient dietary adherence (z = −2.99, p = .003).
Aim 2
There was a significant interaction between patient daily appraisal and patient daily collaboration for dietary adherence (Supplemental Figure 7); however, simple slopes analyses showed that all three slopes were not significantly different from zero. There was also a significant interaction between spouse daily appraisal and spouse daily collaboration for blood glucose checking (Supplemental Figure 8), such that spouse daily appraisal was associated with a greater likelihood of blood glucose checking when spouse daily collaboration was low but was unrelated to the likelihood of blood glucose checking when daily collaboration was high. Like the results for other outcomes, this finding suggests that shared appraisal was linked to a greater likelihood of blood glucose checking when there was less collaboration.
Aim 3
Because there were no models when both patient and spouse predictors were significantly related to outcomes, we did not compare coefficients.
Effects of Appraisal and Collaboration on Daily Mood
Patient Outcomes
Aim 1
As shown in Table 4, patient daily shared appraisal was significantly related to lower patient depressed and angry mood. Spouse daily shared appraisal was related to lower patient depressed mood and higher patient happy mood. Patient daily collaboration was unrelated to patient depressed mood and patient angry mood but was linked to higher patient happy mood. Spouse daily collaboration was unrelated to patient depressed mood and patient happy mood but was linked to decreased patient angry mood. Because there were no models when both daily shared appraisal and daily collaboration were significantly related to outcomes, we did not compare coefficients. These results largely generalized across patient race (Supplemental Table 7), with two exceptions: there was a race by daily appraisal for both depressed mood and happy mood. Patient daily appraisal was related to lower patient depressed mood (β = −.06, p = .001) and higher patient happy mood (β = .04, p = .011) for Black individuals, but there was no relation between patient daily appraisal and patient depressed mood (β = .01, p = .695) or patient daily appraisal and patient happy mood (β = −.02, p = .247) for White individuals.
Aim 2
There were significant interactions between patient daily appraisal and patient daily collaboration for patient depressed mood (Supplemental Figure 9) and happy mood (Supplemental Figure 10). For depressed mood, the interaction showed that patient daily appraisal was related to lower patient reports of depressed mood when patient daily collaboration was low, but patient daily appraisal was unrelated to patient depressed mood when patient daily collaboration was high. For happy mood, patient daily appraisal was related to higher patient reports of happy mood when patient daily collaboration was low, but patient daily appraisal was unrelated to patient happy mood when patient daily collaboration was high. These findings suggest that shared appraisal was more strongly linked to mood when there was less collaboration.
Aim 3
A comparison of patient and spouse daily shared appraisal coefficients for depressed mood revealed that the two coefficients did not significantly differ (z = .16, p = .87). Because patient and spouse collaboration were not both related to happy or angry mood, we did not compare coefficients.
Spouse Outcomes
Aim 1
As shown in Table 5, patient daily shared appraisal was unrelated to spouse depressed mood, happy mood, and angry mood. However, spouse daily shared appraisal was related to lower spouse depressed mood, increased spouse happy mood, and lower spouse angry mood. Patient daily collaboration was unrelated to spouse depressed mood and spouse angry mood, but was related to increased spouse happy mood. Spouse daily collaboration was linked to decreased spouse depressed mood, increased spouse happy mood, and decreased spouse angry mood. These results were not moderated by patient race (Supplemental Table 8).
A comparison of the spouse daily shared appraisal and spouse daily collaboration coefficients revealed that these effects were not significantly different for spouse depressed mood (z = −1.18, p = .24), spouse happy mood (z = −.69, p = .49), or spouse angry mood (z = −.60, p = .55). There were no models where both patient daily shared appraisal and daily collaboration were related to outcomes.
Aim 2
There was a significant interaction between spouse daily appraisal and spouse daily collaboration for spouse angry mood (Supplemental Figure 11). The interaction showed that spouse daily appraisal was more strongly related to lower spouse reports of angry mood when spouse daily collaboration was low than high. Again, this finding seems to suggest that shared appraisal was more strongly linked to angry mood when there was less collaboration.
Aim 3
A comparison of patient and spouse daily collaboration coefficients for happy mood revealed that the patient effect of daily collaboration was not significantly different from the spouse effect (z = −1.17, p = .24). There were no other models where both patient and spouse predictors were linked to outcomes.
Discussion
Prior communal coping research generally assesses communal coping holistically or only examines one component of communal coping—either shared appraisal or collaboration—rather than examining both components simultaneously. The few studies that do include both components generally do not examine the effects of both shared appraisal and collaboration within the same model despite the conceptual differences between these components—namely, that one represents a cognitive construct while the other represents a behavioral construct. Thus, we sought to examine whether daily shared appraisal and daily collaboration are independently linked or interact with each other to predict mood, support, and self-care outcomes. We also assessed the relative strength of each component to these critical daily outcomes in the context of type 2 diabetes management. Finally, because previous studies have rarely examined whether patient or spouse communal coping is more beneficial for relationship and health outcomes, we sought to compare patient and spouse effects as well. Below, we discuss each of the findings, implications for communal coping research, and potential future directions.
The first study aim was to distinguish whether appraisal and collaboration were independently linked to supportive interactions, self-care, and mood. Consistent with predictions, patient and spouse daily shared appraisal and daily collaboration were independently associated with both supportive interactions and better mood as reported by both patients and spouses. A shared appraisal may be related to supportive interactions and mood for both couple members either because individuals feel they are part of a team in managing diabetes, or because a shared appraisal may reduce secondary stress appraisals regarding possible coping resources (Lazarus & Folkman, 1984). In contrast, collaboration consists of tangible actions, which may serve as an observable signal to couple members that they are working as a team to manage the stressor—thereby decreasing distress and enhancing recognition of support attempts (Helgeson et al., 2018).
Consistent with our hypotheses, daily collaboration was generally more strongly linked to behaviors—such as support interactions and diabetes self-care—than shared appraisal was, whereas there were no differences in the relative strength of the associations of shared appraisal and collaboration to mood. Theory suggests that collaboration may have particular importance for behavioral outcomes because partner collaboration serves as a particularly important resource for health behavior change (Renstcher, 2019; Rohrbaugh, 2014). Despite the lack of empirical research testing this hypothesis, our findings address this gap and show that joint action may be linked to positive management behaviors, suggesting that addressing joint behaviors may be a particularly critical component to include in future health interventions.
Although shared appraisal did not show direct links to self-care, it is possible that shared appraisal influences self-care indirectly through effects on intervening variables. Indeed, some recent research suggests that shared appraisal may only be indirectly related to self-care via collaboration (Zajdel & Helgeson, 2020). Future research should examine this issue by assessing potential mediating variables, such as stress appraisal and coping resources, as well as the potential for collaboration itself to act as a mediator between shared appraisal and health outcomes.
For our second study aim, we found evidence that shared appraisal and collaboration interacted to predict support outcomes and some measures of self-care and mood. Although this interaction was not observed for all outcomes, the pattern of the significant interactions was similar: having a view of diabetes as a shared problem was more strongly related to good outcomes when collaboration was low than high. In other words, when a romantic partner perceives low levels of collaboration, a shared appraisal might be particularly important. Thus, shared appraisal appeared to buffer individuals from the potential negative effects of a low level of collaboration and indicates that higher levels of one communal coping component may buffer against the negative impact of lower levels of the other communal coping component. Couples who do not collaborate or work together to manage diabetes may be unable to do so for a variety of reasons that are not reflective of the quality of their relationship. For example, perhaps one partner cannot exercise with the other due to their own health limitations, different work schedules, or differing interests. In these situations, couples may still benefit by viewing diabetes as a shared responsibility and viewing this major stressor as something that impacts them both. Conversely, couples who do not see diabetes as a shared responsibility but who still exercise together, cook together, or solve issues related to diabetes together may also reap benefits for a variety of relationship and health outcomes.
The third study aim was to examine whether patient shared appraisal/collaboration or spouse shared appraisal/collaboration was more strongly linked to adjustment outcomes, hypothesizing stronger effects for spouses than patients on both patient and spouse outcomes. Contrary to our hypotheses, one’s own appraisal/collaboration seemed to be more strongly related to one’s own outcomes. Patient appraisal/collaboration was generally more strongly linked to patient reports of relationship and health outcomes, and spouse appraisal/collaboration was generally more strongly linked to spouse reports of relationship and health outcomes. It may be that one’s own appraisal/collaboration is more strongly linked to one’s own perceptions in the moment, as daily diary questionnaires capture more transient, in the moment assessments. However, spouse appraisal/collaboration may be more influential than patient reports over a longer period of time, which might explain the divergence between our findings within this daily study and the findings in other studies (e.g., Karan et al., 2019).
There was one exception to this pattern in our findings: spouse shared appraisal and collaboration was sometimes linked to better patient mood when patient shared appraisal and collaboration was not. This is consistent with prior meta-analytic evidence showing that spouse we-talk (an indicator of shared appraisal) is more strongly linked to outcomes than patient we-talk (Karan et al., 2019). Spouses’ perceptions of the illness as shared may boost patient mood because the problem is reframed as a couple-level stressor, which may make behaviors consistent with spousal involvement more likely to occur.
Finally, we explored the extent to which race moderated the relations of appraisal and collaboration to outcomes, though we had no a priori hypotheses. Some interactions appeared, although race was not a consistent moderator across outcomes. In all but one case, the pattern of the interaction was the same: the positive relations of shared appraisal and collaboration to outcomes were stronger for Black individuals than White individuals. Communal coping might be particularly beneficial for Black families because Black individuals have historically faced a host of structural and economic inequalities (Hill-Briggs et al., 2021), leading them to rely more on their family networks for support (Sarkisian & Gerstel, 2004). Future research needs to replicate these findings before strong conclusions can be drawn. However, given that the majority of prior research in this area has utilized White samples, these findings suggest that researchers should be careful not to generalize conclusions from these White samples to other racial/ethnic groups.
Overall, these results demonstrate unique links of both daily shared appraisal and daily collaboration to mood and support behaviors in patients with type 2 diabetes and their spouses, as well as links of collaboration alone to diabetes self-care outcomes. Additionally, patient self-care behaviors were not strongly related to each other and instead seemed to reflect separate domains of management, which indicates the potential for spouse collaboration to play a role in each domain of self-care. Importantly, because both shared appraisal and collaboration were included in the same models, these results indicate that there may be unique links to daily fluctuations in relationship and health above and beyond their shared overlap. Given these findings, we urge future researchers to continue to explore the functioning of shared appraisal and collaboration by separating these constructs and examining their effects on outcomes over time. It is possible that shared appraisal influences intervening or intermediary outcomes such as support behaviors, which can modify more distal health outcomes such as psychological well-being and diabetes self-care management behaviors. To understand more about the unique effects of shared appraisal and collaboration, researchers need to identify the specific mediators that account for each of their links to relationships and health.
Additionally, although communal coping is a dyadic process, results indicated that each person’s perception of appraisal and collaboration was more strongly linked to their own reported outcomes. Future research should continue to examine the conditions under which patient and spouse perceptions of shared appraisal and collaboration agree or diverge. It is also worth noting that spouses reported enhanced mood on days when either patients or spouses engaged in greater shared appraisal and collaboration. Given the robust literature on caregiving burden (Pinquart & Sörensen, 2003), these findings suggest that patient and spouse communal coping may buffer the potential burden experienced by spouses. Future research should explore whether communal coping is always beneficial for spouses, or whether there are conditions under which either shared appraisal or collaboration could be harmful for spouses. Some work has addressed personality characteristics of patients and spouses that influence the benefits of communal coping on patients (Lee et al., 2020a; Van Vleet & Helgeson, 2019), but no study to our knowledge has examined moderators of the effects of communal coping on spouse health.
These results hold implications for a number of potential future directions in this area. First, research should examine the unique mechanisms that underlie the effects of appraisal and collaboration. For example, shared appraisal might be linked to mediators that represent cognitive perceptions (e.g., self-efficacy) or specific biological mediators (e.g., cardiovascular, endocrine, and immune system activation; Rentscher, 2019). On the other hand, collaboration may be more strongly linked to clinical health endpoints through mediators that represent behavioral actions (e.g., health behaviors). Second, we urge future researchers to continue to employ longitudinal research designs to understand the role of communal coping over time. In this study, we recruited participants who were newly diagnosed with diabetes in order to assess communal coping during the initial transition period. However, it is possible that communal coping operates differently over time further away from this initial diagnosis point or during periods of better or worse health. Third, future researchers should examine the antecedent variables that give rise to shared appraisal and collaboration, which could involve personality characteristics of couple members (e.g., attachment orientation) as well as relationship characteristics (e.g., closeness). Fourth, because the benefits of communal coping have been well-established, it is time to identify moderators of communal coping effects on both patient and spouse health. Relevant to these last two points, it is important to understand the operation of communal coping within culturally, racially, and ethnically diverse contexts. As just one example, East Asian cultural norms that emphasize potential concerns around burdening close others (Campos & Kim, 2017) might preclude communal coping or undermine its benefits in those contexts.
Overall, study strengths include the fact that individuals were relatively recent in their diagnosis of diabetes, whereas most studies examine couples that have been coping with diabetes for many years. Studying couples in which individuals were recently diagnosed provides insight into communal coping during the initial stages of the coping process when stress and uncertainty may be high and couples are trying to establish a self-care regimen. Additionally, although the sample was not a probability-based sample, this community-based sample was diverse in terms of age, social status, education, and race, all of which increase the generalizability of our findings and set it apart from studies that focus on White, middle-class couples.
Before concluding, we acknowledge several study limitations. First, brief versions of well-validated scales with limited scale options were used to accommodate the daily diary design and reduce participant burden; however, they may not have captured the full range of variance among participants. Second, because our data are cross-sectional, we cannot make causal claims that shared appraisal or collaboration cause changes in outcomes. However, we view these daily diary reports as an initial effort to explore the effects of shared appraisal and collaboration on a daily basis, providing a more ecologically valid assessment of these variables. Future research should seek to determine the causal direction between the components of communal coping and mood, support, and self-care as well as the links between shared appraisal and collaboration. Finally, we note that the participants in this study were self-referred, and thus may not be representative of the general population. For example, couples who report higher marital quality or are more satisfied with their relationship may be more likely to participate in couples-based research. However, we recruited participants from the community using a variety of methods (e.g., local churches, bus advertisements, community centers, health fairs, hospital registry) rather than relying on patients who attended a single physician practice or health care center to try to diversify the participants in our study. We do acknowledge though that as with any convenience sample, our results may not be generalizable to the general population.
In sum, this study suggests that daily shared appraisal and daily collaboration are independently linked to better psychological health, behavioral health, and relational outcomes for both patients with type 2 diabetes and their spouses. However, collaboration appeared to be more important than shared appraisal for behavioral outcomes. In addition, there was some evidence of buffering between shared appraisal and collaboration, such that scoring high on one component buffered the individual from the deleterious effects of scoring low on the other component. These findings hold implications for the development of interventions for those coping with a chronic physical illness. Interventions that help couples view the stressor as shared and identify joint actions in which patients and romantic partners can engage may be especially beneficial for couples at an early stage of adjustment to chronic illness, in which health behavior management patterns may not yet be established. If interventions can increase shared appraisal and collaboration for patients and spouses on any particular day, both patients and spouses may experience better adjustment to chronic illness.
Supplemental Material
Supplemental Material - Links of daily shared appraisal and collaboration to support, mood, and self-care in type 2 diabetes
Supplemental Material for Links of daily shared appraisal and collaboration to support, mood, and self-care in type 2 diabetes by Melissa Zajdel, Jeanean B Naqvi, Nynke MD Niezink and Vicki S Helgeson in Journal of Social and Personal Relationships
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been supported by R01DK095780 from the National Institute of Health. The research was conducted when all authors were affiliated with Carnegie Mellon University. Melissa Zajdel is now a postdoctoral scholar at the National Human Genome Research Institute in Bethesda, Maryland was supported in part by funding from the Intramural Research Program of the National Human Genome Research Institute (ZIAHG200395). Jeanean Naqvi is now a postdoctoral scholar at the University of California, San Diego Department of Family Medicine.
Open research statement
As part of IARR’s encouragement of open research practices, the author have provided the following information: This research was not pre-registered.
The data used in the research can be shared with the public. The data can be obtained via emailing the senior author at
Supplemental material
Supplement material for this article is available in online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.