
Abstract
Attachment insecurity is a transdiagnostic marker of risk associated with interpersonal emotion dysregulation and adverse psychosocial outcomes across the lifespan. Few interventions target the enhancement of attachment security in late adolescence. Most programs focus on strengthening the adolescent-caregiver relationship; meanwhile, youth increasingly spend less time with their families and look to peer relationships as a source of connection, particularly as they transition to college. Drawing from the principles of Emotionally Focused Therapy, we developed a psychotherapeutic peer mentorship program to enhance attachment security for insecurely attached youth during the transition to college. We tested the preliminary efficacy of Emotionally Focused Mentorship (EFM) in an open pilot trial by pairing (N = 82) insecurely attached first-year college students (i.e., “mentees”) with securely attached mentors. Across five weekly sessions, mentors helped mentees identify and express their emotions in close relationships by working through different relational scenarios. Attachment and mental health trajectories were self-reported three times over five weeks and analyzed using Bayesian growth curve models. Across five weeks, participants reported improvements in attachment anxiety and avoidance, emotion regulation difficulties, depressive symptoms, loneliness, and self-esteem. Participants who completed the intervention (n = 55) noted improvements in their psychological wellbeing and interpersonal relationships. Results are promising and highlight the need to conduct a randomized clinical trial to test if these effects are causal. Given rising mental health demands, trained peer mentors may be a cost-effective way to improve attachment and psychological outcomes for insecurely attached participants during the transition to college.
Keywords
Introduction
From the moment we are born, our survival depends on our ability to form attachment bonds with close others. In combination with genetic predispositions, repeated interactions with early caregivers create the lens through which we view the self and the social world, giving rise to attachment orientations (Ainsworth, 1969; Bowlby, 1982). Attachment orientations can be thought of as “working models,” templates that help us predict how others might view, treat, or rely on us, and in turn, how we should view, treat, and rely (or not rely) on others (Collins & Read, 1990). A robust literature indicates that attachment insecurity, marked by interpersonal emotion dysregulation and an over- or under-reliance on relationships, disrupts our capacity to maintain healthy close ties and predicts psychopathology across the lifespan (Kassel et al., 2007; Nada Raja et al., 1992). Insecure attachment patterns learned over time may help children get their needs met early in life; however, insecure patterns of attachment can become maladaptive as children enter new social environments in adolescence. For example, strategies like the suppression of one’s emotions and needs can leave teens feeling isolated amongst peers, contributing to the development of loneliness and depressive symptoms. Rather than relying on outdated regulation strategies, youth might benefit from learning new emotion regulation skills, such as the effective communication of their emotions and needs, to help them connect and build healthy, secure relationships.
Thus, drawing upon the developmental, social, and clinical literature, we designed and tested a novel psychotherapeutic intervention specifically for insecurely attached adolescents and young adults during the transition to college—Emotionally Focused Mentoring (EFM). EFM is a five-week program that pairs incoming college students ranking high on attachment insecurity with trained, securely attached mentors (i.e., lay therapists). Together, mentors and mentees explore the participant’s attachment tendencies and promote the use of adaptive interpersonal emotion regulation strategies in close relationships. In the present study, we introduce the EFM model and report the results of an open-trial pilot that tested the preliminary efficacy of EFM for improving attachment security, emotion regulation skills, and mental health outcomes in a sample of 82 insecurely attached adolescents. 1
Attachment orientations
Attachment styles or orientations refer to individual differences in the way people think, feel, and act in close relationships. A well-established self-report measure of attachment assesses how people rank on two dimensions: avoidance and anxiety (Collins & Read, 1990). Securely attached youth score low on both anxiety and avoidance. Based on the responsiveness, sensitivity, and acceptance they receive from caregivers, securely attached youth learn that they are lovable and worthy of belonging. They tend to report early life environments that were warm and stable, generally holding more positive views of themselves and others (Caldwell & Shaver, 2013; Mikulincer et al., 2009). In contrast, individuals ranking high on attachment insecurity score higher on attachment anxiety and/or avoidance. Their attachment figures may be more unpredictable, unreliable, unresponsive, critical, or abusive. In response to these environments, insecurely attached children typically adopt a negative view of themselves and/or others, learning to regulate their emotions in ways that fit their early familial contexts to help them meet their needs.
For example, adults with high attachment anxiety tend to hyperactivate or upregulate attachment needs/emotions in their relationships by amplifying their desire for intimacy and displaying hypersensitivity to rejection/abandonment (Caldwell & Shaver, 2013). They learn that they cannot always rely on close others; thus, they upregulate their emotions and needs to try to get the attention of aloof caregivers or close others. In contrast, people who rank higher on avoidance learn that it is more adaptive to deactivate or downregulate their needs, because they have learned that close others will not be responsive even when they protest. Therefore, to fit within this family structure, they learn to suppress their need for emotional intimacy, minimize emotional distress, and become hyper self-reliant (Caldwell & Shaver, 2013; Shaver & Mikulincer, 2002).
The emotion regulation strategies used by insecurely attached youth may be adaptive in early development, helping them maintain psychological and physiological homeostasis in early caregiving environments (Mikulincer & Shaver, 2019; Sbarra & Hazan, 2008). However, these strategies can become maladaptive when forming new relationships in adolescence or adulthood (Collins & Read, 1990). For example, anxiously attached teens typically display hypersensitivity to abandonment and have a strong desire for closeness that can inadvertently push others way (Caldwell & Shaver, 2013). In contrast, people who rank higher on avoidance may isolate themselves and fixate on being extremely independent, missing out on opportunities for close connection and social support (Caldwell & Shaver, 2013; Shaver & Mikulincer, 2002).
Insecure attachment as a transdiagnostic risk factor for poor health
Across various cultures and nationalities, approximately 30–40% of children develop an insecure attachment style (Agishtein & Brumbaugh, 2013), creating a risk for deleterious relational, psychological, and health outcomes. People with high attachment insecurity report difficulties maintaining high-quality friendships, citing challenges with self-disclosure, empathy, trust, self-esteem, intimacy, and emotion regulation (Bakermans-kranenburg, van Ijzendoorn, Steele & Roisman, 2009; Duemmler & Kobak, 2001; Meyers & Landsberger, 2002; Holland & Roisman, 2010). In romantic relationships, they experience (a) less commitment and satisfaction, (b) higher levels of conflict and poor conflict management skills, (c) difficulties seeking or receiving support from their partner, or (d) prolonged recovery after breakups (Collins & Read, 1990; Kirkpatrick & Davis, 1994; Sbarra & Emery, 2005; Sbarra et al., 2012). Attachment insecurity is also associated with a range of psychological conditions such as depressive symptoms, anxiety, post-traumatic stress disorder, eating disorders, personality disorders, and suicidal ideation (Love & Murdock, 2004; Nada Raja et al., 1992; O'Connor & Elklit, 2008; Shaver & Clark, 1994; Zachrisson & Skårderud, 2010). Insecurely attached adults also experience more physical health consequences, including poorer physiological responses to stress, less engagement in adaptive health behaviors, and more challenges trusting and interacting with healthcare providers (Huntsinger & Luecken, 2004; Holwerda et al., 2013; Maunder et al., 2006; Maunder & Hunter, 2008, 2016). The consequences of attachment insecurity are profound and long-lasting, impacting health, wellbeing, and the capacity to connect with others. Therefore, interventions promoting attachment security beyond childhood are needed to address these far-reaching consequences.
Can attachment security change in adolescence and young adulthood?
Attachment styles are relatively stable across the first two decades of life (Fraley, 2013), but they can change due to pivotal life events or within relationships (Fraley et al., 2021). In a literature review, Fraley (2019) argues that attachment-related working models can become more or less secure in response to romantic breakups (Kirkpatrick & Hazan, 1994), war-related trauma (Mikulincer et al., 2011), the transition to parenthood (Feeney et al., 2003; Simpson et al., 2003), social support or conflict interactions (Chow et al., 2016; Green et al., 2011; La Guardia et al., 2000), and psychotherapy (Johnson, 2009; Taylor et al., 2015). Although people often revert to their original attachment style (Fraley et al., 2021), longitudinal studies suggest that more enduring improvements in attachment security occur in the context of a safe relationship. For example, insecurely attached adults who enter highly satisfying marriages with a securely attached partner become more securely attached over time (Davila et al., 1999), potentially resulting from repeated positive interactions with their securely attached partner.
Adolescence and young adulthood is marked by the challenge of maintaining familial attachment while looking more and more to one’s peers for influence and support. While there are attachment-based therapies for young children, few interventions are designed for adolescents or young adults (Kobak & Kerig, 2015). Most notably, Attachment-Based Family Therapy (Diamond et al., 2016) is a multi-modal evidence-based treatment designed for teens experiencing depression or suicidal thoughts/behaviors; family sessions create reparative conversations and emotional attunement, helping the caregiver serve as a secure base and encouraging the teen to turn to the caregiver for support. One limitation of this program is that the enhancement of attachment security is focused on the caregiver-teen relationship, while some teens may be more invested in and impacted by peer relationships, potentially creating a mismatch in their desire to participate.
Attachment during the transition to college.
In late adolescence, the transition to college is characterized by dramatic changes to one’s social environment, igniting the expression of attachment-related emotion regulation strategies. As teens step into young adulthood and enter a more competitive academic sphere, they must manage a series of developmental tasks (e.g., creating a new social support system, navigating romantic relationships, and identifying potential career trajectories). This uprooting and reorganization of one’s social identity may elicit attachment behaviors, such as anxiety when meeting new people, avoidance of emotional intimacy, and calls for effective socioemotional skills. Taking advantage of this opportune time for intervention, one program called “The Connection Project” trains student facilitators to improve social connection among first-year college students to bolster their mental health; using attachment-based activities, student facilitators enhance connectedness amongst small groups of incoming students (Allen et al., 2021). Rather than meeting with a therapist, this peer-to-peer approach may appeal to incoming college students, particularly as they seek more independence and influence from peers.
The present study
Aligned with recent calls to build interventions promoting attachment security for adolescents and young adults (Thompson et al., 2022), we developed and tested a 5-week psychotherapeutic intervention to promote attachment security for insecurely attached participants during their transition to college called Emotionally Focused Mentoring (EFM). Using an attachment-based approach, we paired securely attached “mentors” trained in the principles of Emotionally Focused Therapy (Johnson, 2019) with insecurely attached mentees. Mentors targeted attachment insecurity by encouraging mentees to use adaptive interpersonal emotion regulation skills rather than relying on anxious and/or avoidant strategies. In EFM, mentor-mentee pairs meet for one hour a week to reflect on the mentee’s attachment tendencies and practice navigating challenging relational scenarios from a place of security. These scenarios provide a context for accessing, labeling, expanding, validating, and shaping attachment-related emotions. Mentors collaborate with and guide mentees to identify and clearly express their emotions to cultivate attachment security within and beyond the self. Mentors aim to serve two attachment functions during these 5 weeks: first, they serve as a safe haven, allowing mentees a safe space to discuss the challenges they face as they navigate interpersonal relationships. Second, they aim to function as a secure base, teaching mentees new emotion regulation skills, providing the confidence they need to navigate the world more effectively (Bowlby, 1988).
Following the NIH Stage Model of intervention development (Onken et al., 2014), we assessed EFM’s feasibility and acceptability with first-year college students (N = 11) and refined the intervention based on participant feedback (see Manvelian, 2021). The current study describes the next phase of EFM’s development through an open-pilot trial with 82 participants.
To examine whether EFM is a viable way to promote attachment security, emotion regulation skills, and mental health outcomes for adolescent populations, we conducted a pilot study in a preregistered, single-arm open trial (N = 82) with a sample of first-year college students. Our goal was to track changes across time in the key intervention targets (i.e., attachment insecurity, emotion regulation skills, and mental health) in a sample of participants who ranked high on attachment insecurity. These analyses were preregistered prior to data collection (https://osf.io/zhpj6/?view_only=6b198aa2d92b48568e8b0f2a0be976b1). 2
Across 5 weeks of Emotionally Focused Mentoring, we expected decreases in attachment insecurity, with greater decreases in attachment anxiety and smaller decreases in attachment avoidance. We note this difference because attachment avoidance often develops after a phase of anxious protest in childhood, when the child learns that their cries will not be met with sensitivity and has no choice but to suppress their emotions and needs (Ainsworth, 1969); thus, the turning “off” of one’s attachment needs may be more ingrained and difficult to change in adolescence compared to those who may be anxiously attached and need help attenuating emotion regulatory responses rather than awakening them. We also expected to see improvements in emotion regulation skills and mental health outcomes, including lower levels of depressive symptoms, anxiety, and loneliness. We investigated the correlated change among attachment insecurity, difficulties with emotion regulation, depressive symptoms, anxiety, loneliness, and self-esteem over time. We also re-assessed participants’ perceived acceptance and usefulness of EFM by asking participants at the final assessment whether they would recommend the program to a friend, if they believed the mentorship program enhanced their psychological wellbeing, and if the program improved their capacity to form healthy relationships.
Method
Participants
Mentors.
We recruited 11 securely attached peer mentors. We advertised the position via email. Applicants filled out the 18-item Revised Adult Attachment Scale (Collins, 1996) along with questions about how warm and responsive they feel they are, their interest in the lab, their qualifications, and their reason for wanting to become a supportive mentor for incoming students. Forty-six undergraduate students majoring in psychology applied to become a mentor, 30 were invited to interview, and 20 completed the interview process. Of the 20 interviewees, 11 ranked high on attachment security, exhibiting warm, welcoming, appropriate behavior during the interview, and were selected to serve as mentors for insecurely attached participants. Mentors were racially diverse; four identified as Hispanic/Latinx, four identified as Caucasian/White, one identified as Asian, one identified as African-American/Black, and one identified as multiracial, Hispanic and White. Eight identified as women and three identified as men. Mentors ranked high on attachment security, ranking low on attachment anxiety, M = 1.83, SD = .43, and attachment avoidance, M = 1.83, SD = .47, on the Revised Adult Attachment Scale (Collins, 1996).
Mentees.
Demographic statistics for participants ranking high on attachment insecurity.
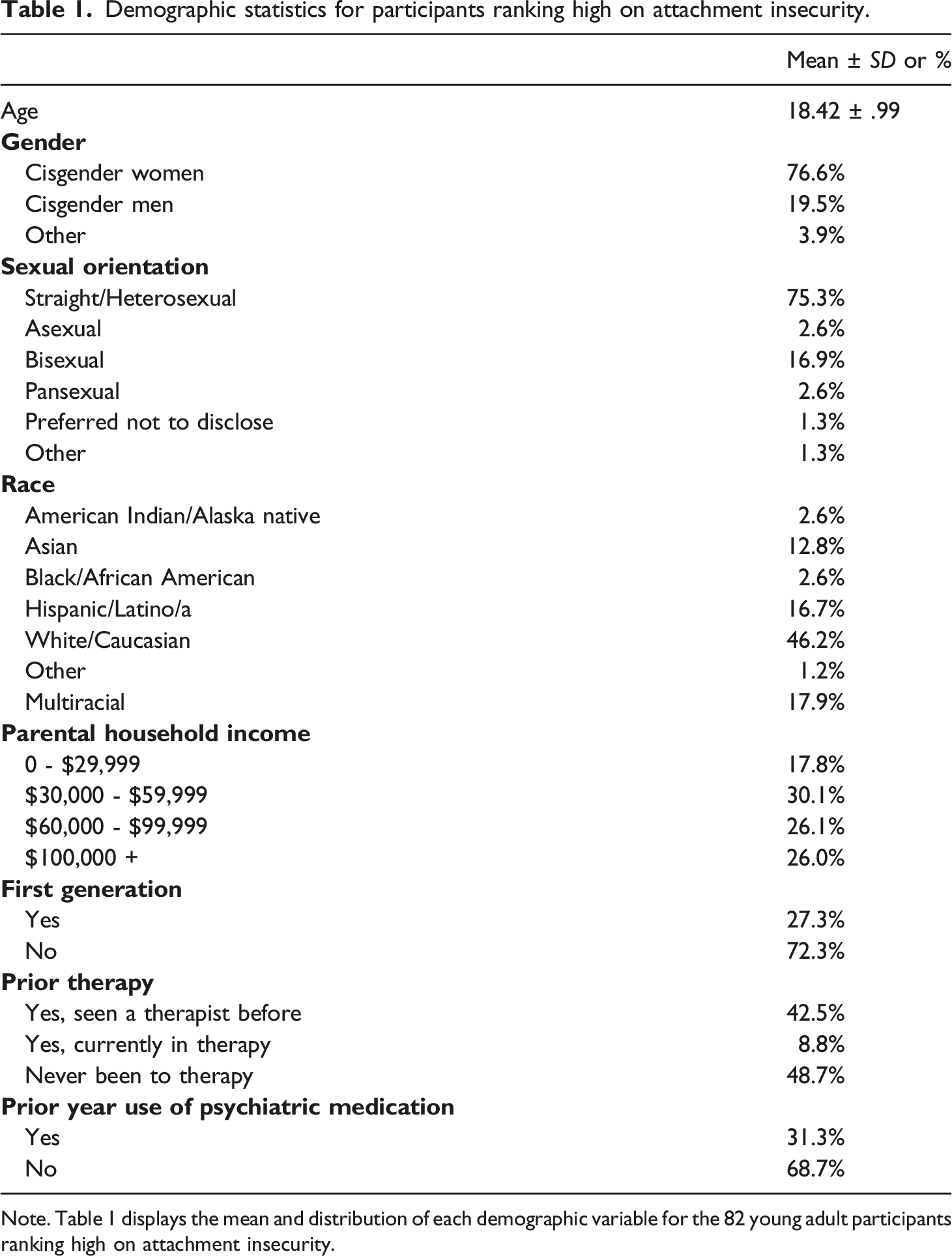
Note. Table 1 displays the mean and distribution of each demographic variable for the 82 young adult participants ranking high on attachment insecurity.
Figure 1 displays the CONSORT flow diagram for this study. In total, 1,419 potential mentees met the eligibility criteria to participate. Of this group, we contacted the 522 individuals ranking highest in attachment insecurity. Ultimately, 95 individuals were interested, and 82 participants completed session one. Of the 82 participants who completed session one, 72 completed three sessions, and 55 participants completed all five sessions. In total, 27 participants discontinued the study by the final assessment, and approximately one-third of participants finished the study online due to the impact of COVID-19 in March and April of 2020. We conducted independent samples t-tests on all study variables to assess attrition bias; there were no statistically significant differences between participants who did and did not complete the study. Consort diagram for the pilot study of emotionally focused mentoring.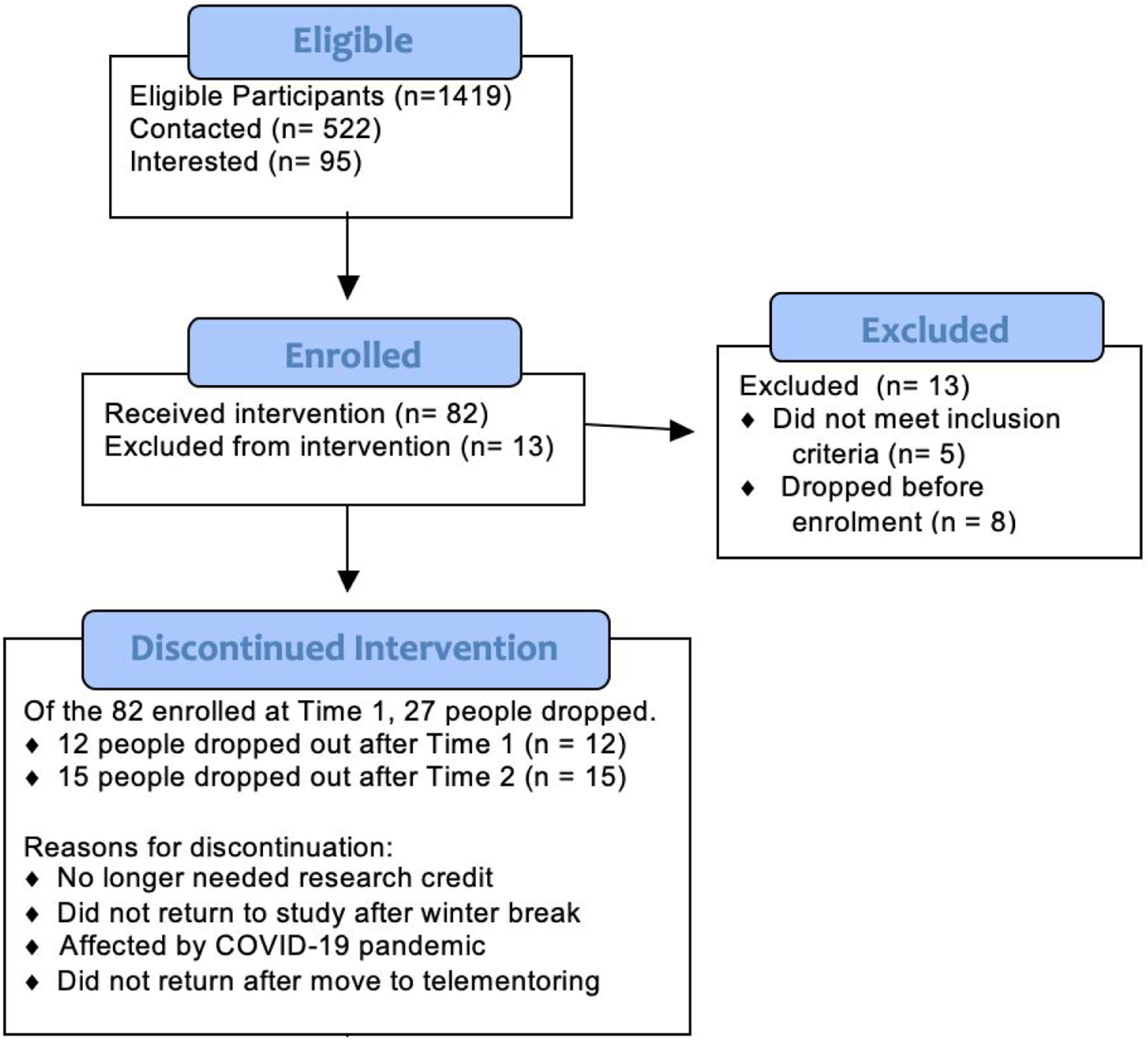
Procedures
This study is an open pilot trial, with no control group, meaning that all participants received the intervention. Participants were told the study was about a new program promoting social and emotional wellness for first-year college students. They were not informed of their score on the attachment measures. Participants were scheduled for a weekly appointment with a mentor who ranked high on attachment security for five weeks. They provided informed consent prior to enrollment and completed a 20-min survey prior to the first and third visit and after the fifth visit. They earned four research credits for completing the first session of the study. Participants did not receive additional compensation after the first session to assess if participants would continue mentorship without payment.
Mentor training
Lay therapists were taught to follow the same confidentiality guidelines as licensed clinical psychologists in the United States, following the ethical guidelines put forth by the American Psychological Association. Based on principles from Emotionally Focused Therapy (Johnson, 2019), mentor training focused on the following clinical skills: creating a warm therapeutic alliance (i.e., listening skills), cultivating emotional awareness (i.e., identifying underlying emotions), gradual exposure to emotions (i.e., deepening emotional experiences), and adaptive emotion regulation strategies (i.e., practicing how to communicate emotions when feeling activated without overwhelming others or pushing them away). Mentors were trained for 10 hours and completed one round of mentorship during the acceptability/feasibility study (Manvelian, 2021). For the current study, each mentor carried a caseload of 3–4 mentees at one time. The supervisor (program developer; advanced doctoral student; first author Atina Manvelian) listened to audio recordings provided feedback to mentors, encouraged self-reflection and choreographed role-plays to enhance mentorship skills; Group supervision each week was held for 1.5 hours, with 5–6 mentors present in each group.
Intervention: EFM content
EFM is a manualized intervention designed to promote attachment security for emerging adult populations using principles of Emotionally Focused Therapy (Johnson, 2019) 3 . The first session focuses on creating closeness between mentors and mentees, building an alliance through emotional attunement, and fostering trust through emotional disclosure about one’s identity, early attachment relationships, and social experiences in college. The subsequent four sessions introduce a relational scenario at the beginning of each session. Each scenario represents difficulties commonly occurring during close relationship formation, maintenance, and dissolution. Topics include Exploring Past Familial Relationships (Week 1), Maintaining Close Relationships (Week 2), Managing Conflict (Week 3), Setting Boundaries (Week 4), and Letting Go of Relationships (Week 5).
After reading each scenario, the mentors present three ways of responding that correspond to the three primary attachment styles (avoidance, anxiety, and security). The mentors ask mentees if there has ever been a time when they experienced a similar situation and which aspects of each response resonate with them. The mentors then help mentees reflect on how they might feel and behave in similar scenarios using this information. The goal of this process is to provoke attachment-related themes (e.g., how the mentee typically behaves when in conflict with a close other); the remainder of the hour focuses on the mentee’s personal experiences with these themes (e.g., “Can you tell us about a time when you were in conflict with someone you cared about?”). Throughout these discussions, mentors listen, validate, summarize, and encourage adaptive emotion regulation strategies, helping mentees practice identifying and expressing emotions and needs during challenging interpersonal scenarios. The majority of EFM took place in person.
However, in March of 2020, all recruitment efforts discontinued following the announcement of the coronavirus (COVID-19) pandemic when the risk of contracting COVID-19 increased in the United States, and EFM quickly adapted to be delivered via telehealth to allow 18 participants to finish their last mentoring session via Zoom, an online platform for videoconferencing. Mentors were provided with additional training to conduct telementoring during COVID-19; this training was provided by the first author of this manuscript who was an advanced doctoral student at the time the study was conducted. A telementoring protocol was followed and the HIPPA-compliant version of Zoom was used to maintain confidentiality. Aiming to mimic in-person procedures, surveys and exit interviews were administered online via Zoom, and participants were sent each relational scenario at the beginning of each session via the chat feature. Of the 82 participants, only 18 completed their final session via telementoring. Although the delivery of EFM was different, the content remained the same.
Measures
Participants completed the following surveys on three occasions.
Revised adult attachment scale – close relationships version (RAAS – CR)
The 18-item RAAS-CR assesses experiences in close relationships such as depending on others, worrying about rejection, and comfort with intimacy (Collins, 1996). The RAAS-CR yields scores for two subscales: the degree to which people are avoidantly attached (i.e., “I find it difficult to allow myself to depend on others”) and anxiously attached (i.e., “I often worry that other people don’t really love me”). Items were rated on a 1-5 Likert scale (1 = Not at all characteristic of me, 5 = Very characteristic of me), with higher scores representing higher levels of avoidance or anxiety. The Cronbach’s alpha internal consistency score was good for anxiety and avoidance; .83 and .82, respectively.
Difficulties in emotion regulation scale –short form (DERS)
The 18-item DERS measures people’s ability to “identify, understand, and accept emotional experiences, control impulsive behaviors when distressed, and flexibly modulate emotional responses as situationally appropriate ( Kaufman et al., 2016).” Example items include, “I pay attention to how I feel,” “I am confused about how I feel,” and, “When I am upset, I have difficulty controlling my behaviors.” Items were rated on a 1-5 Likert scale (1- Almost Never, 2- Sometimes, 3- About Half the Time, 4- Most of the Time, and 5- Almost Always), with higher ratings being suggestive of greater emotion regulation difficulties. The internal consistency of this scale was high (α = .93), suggesting strong reliability.
Beck depression inventory (BDI)
The BDI is a 21-item questionnaire that evaluates the intensity of depressive symptoms in normal and psychiatric populations (Beck et al., 1961). The BDI assessed symptoms include mood, suicidal ideation, changes in sleep/weight, fatigue, irritability, focus, and a sense of failure. Each item included four descriptive statements (rated 0–3, 3 indicating the greatest severity of depression) and participants chose the statement that best represented their symptoms. Clinical cut-off scores for the BDI are as follows: 1–10 indicates normal ups and downs; 11–16 indicates mild mood disturbance; 17–20 indicates borderline clinical depression; 21–30 indicates moderate depression; 31–40 indicates severe depression; 40+ indicates extreme depression. The internal consistency for the BDI was high (α = .90), indicating strong scale reliability.
Penn state worry questionnaire (PSWQ)
The 16-item PSWQ measures the trait of worry with response options ranging from 1 – Not at all typical of me to 5 – Very typical of me, with higher ratings suggesting higher levels of worry (Meyer et al., 1990). Rather than measure generalized anxiety symptoms, we used a measure of worry because it is prevalent during the transition to college and is positively correlated with generalized anxiety disorder (Meyer et al., 1990). Example items include, “My worries overwhelm me,” and “I am always worrying about something.” The Cronbach’s alpha for the PSWQ was .92, suggesting strong scale reliability.
UCLA loneliness scale
A shortened three-item version of the UCLA Loneliness Scale (Hughes et al., 2004) measured the degree of felt loneliness (Hughes et al., 2004). Items include “How often do you feel that you lack companionship,” “How often do you feel left out,” and “How often do you feel isolated from others?” Response options range from 1 = Hardly Ever to 3 = Often, with higher ratings representing higher levels of loneliness. The internal consistency was .83, indicating good scale reliability.
Rosenberg Self-Esteem Scale (RSES)
The 10-item RSES assessed global self-esteem, including feelings of self-acceptance and self-worth (Rosenberg, 1965). Example items include, “I feel that I have a number of good qualities,” “I certainly feel useful at times,” and “At times I think I am no good at all.” The scale ranges from one to four (1- Strongly Disagree to 4 - Strongly Agree), with higher ratings representing higher ratings of self-esteem. The Cronbach’s alpha is .89, suggesting high scale reliability.
Intervention Acceptability
The following questions gauged acceptability at the final assessment: (1) “Has the mentorship program improved your psychological wellbeing?” and (2) “Has the mentorship program improved your ability to have healthy relationships?” The participants rated the questions on a Likert-type scale ranging from Not at all, Somewhat, and Definitely. A binary (i.e., yes or no) question measured the participants’ willingness to recommend the program in the future (i.e., “Would you recommend this mentorship program to a friend?”).
Data analysis
Data were analyzed according to our preregistered hypotheses and our deidentified dataset is available here: https://osf.io/ygxws/?view_only=c00c73307a0b4e9e914a8ab529e9f1d2.
We retained 87.8% of participant data at Week 3 and 67.1% of the total participant data by Week 5. Bayesian t-tests revealed that compared to individuals who remained in the study, individuals that discontinued the study did not differ at baseline on our attachment and mental health variables. Furthermore, Little’s MCAR test provided evidence that data may be missing at random. Given the assumption that data were missing at random, missing values were imputed using the random forest method in the mice package available in R (Multiple Imputation by Chained Equations; Van Buuren & Groothuis-Oudshoorn, 2011). Variables included in the prediction matrix were those in the final analytical models. Missing data ranged from 13%–33%; therefore, we specified 30 imputations with 35 iterations within each imputation (burn-in iterations = 100), resulting in 30 complete datasets. In Bayesian modeling, pooling is achieved by combining the posterior draws of the sub-models. This process does not differ from the method employed by brms to generate posterior distributions, rendering pooling unnecessary (Bürkner, 2018; Zhou & Reiter, 2010). The results using list-wise deletion (i.e., complete case analysis) are similar to those obtained with multiple imputation. Therefore, the imputed results are presented.
We first specified a series of multilevel models using the brms package in R (Bürkner, 2017a) to assess how emotion regulation, attachment insecurity, and mental health outcomes changed over time. We used multilevel modeling within a Bayesian framework (Bürkner, 2017b) to account for the interdependence or autocorrelation between our subject’s responses over time, and we specified different family links (i.e., “Gaussian” or “Skew Normal”) designated to fit the normal or skewed distributions of continuous outcome variables within each growth curve model. 4
The brms package calculated a 95% highest density interval (HDI) for the growth curve or correlated change multilevel models. The HDI describes the uncertainty of the parameters, specifically describing how probable it is that the actual population parameter lies within the specified range, given the hypothesis and data. For example, a 95% HDI suggests a 95% probability that the true value of the population mean lies within that interval. If the HDI includes zero, the actual population mean is unlikely to lie within this specified range. The chains and iterations were set to 5 and 5000, respectively. Model convergence was confirmed using R-hat values (i.e., less than 1.1), effective sample size, and visualization of trace plots. No convergence issues were noted.
Results
Descriptive statistics
Descriptive statistics for key study variables.
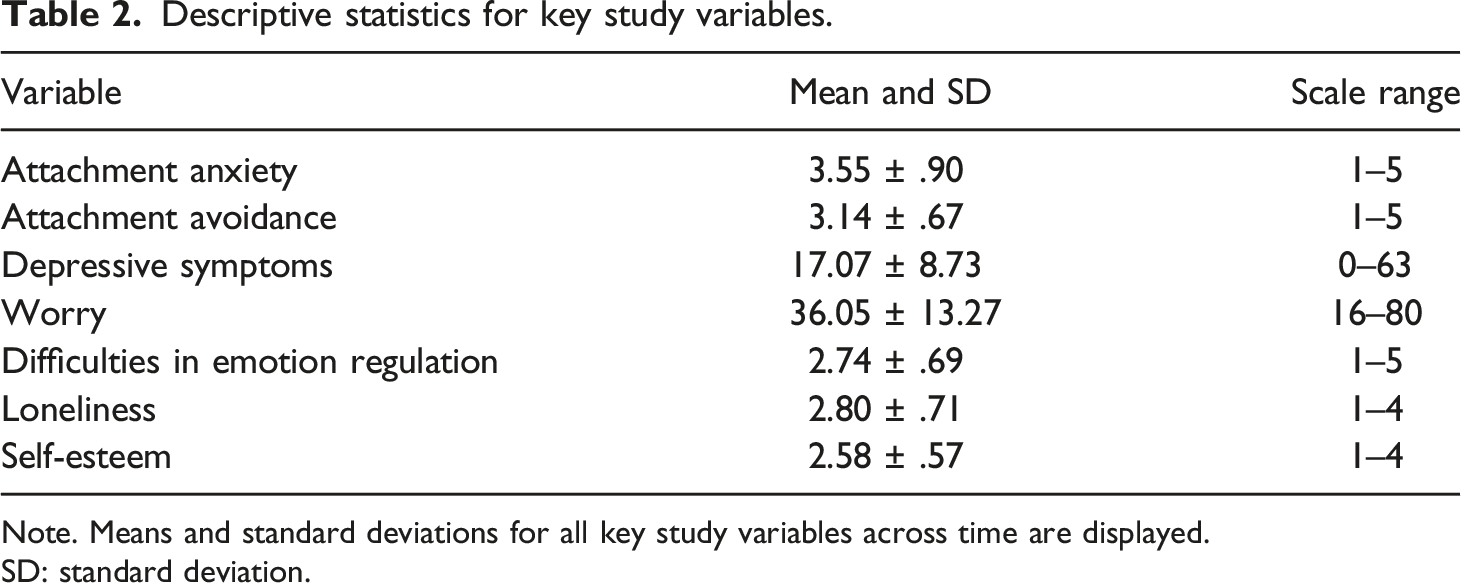
Note. Means and standard deviations for all key study variables across time are displayed.
SD: standard deviation.
Growth curve model results for key study outcomes.

Note. Bayesian growth curves model change over time for each of our dependent variables across five weeks of Emotionally-Focused Mentoring. Cohen’s d is reported as a within-person effect size (calculated as: (|m1 – m2|)/√ (s12 + s22 – (2rs1s2)).
b: unstandardized parameter estimate; SE: standard error; HDI: highest density interval.
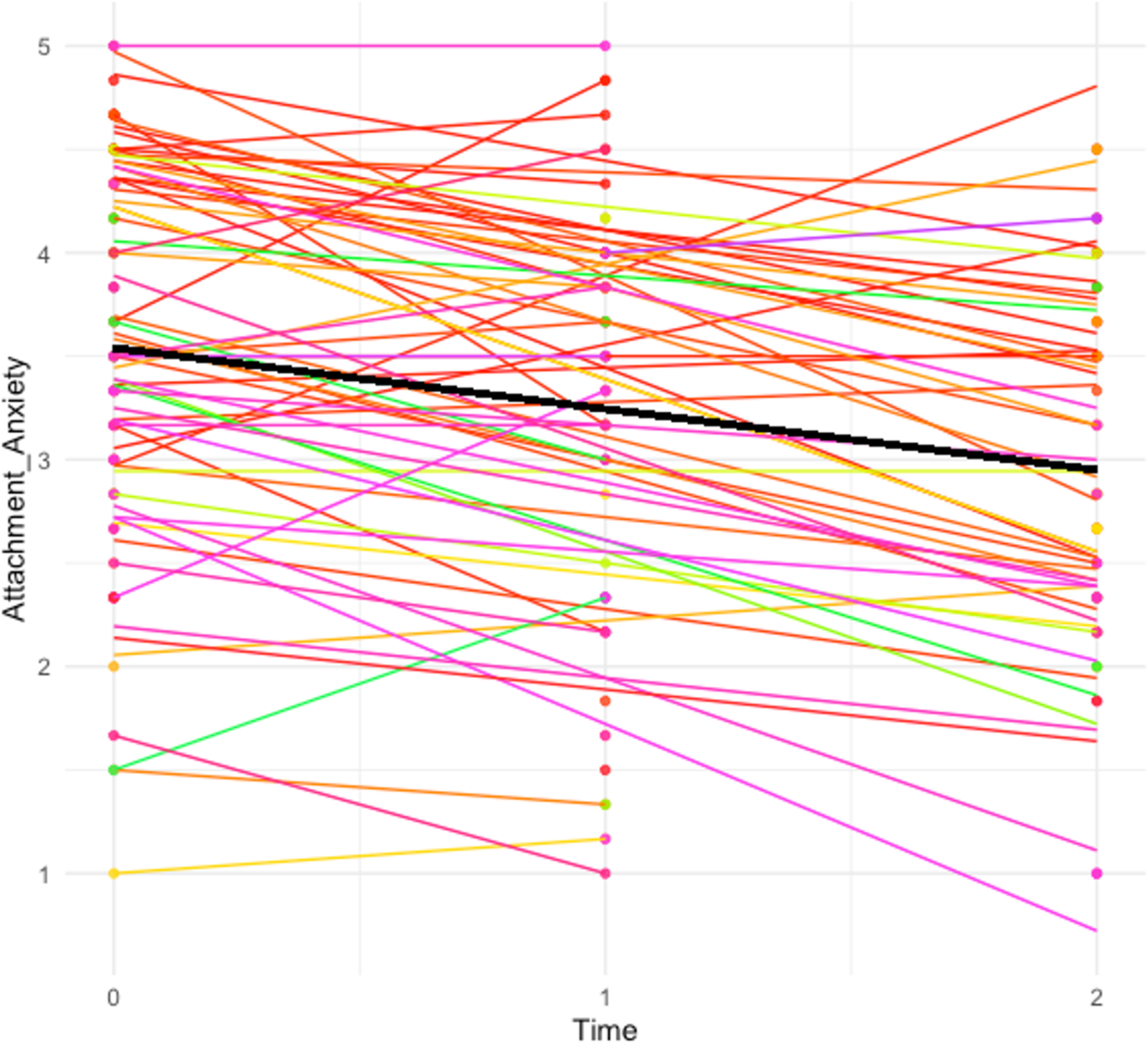
Changes in attachment anxiety across five weeks. Note. On average, across 5 weeks of Emotionally-Focused Mentoring, participants report decreases in attachment anxiety, yielding in a medium Cohen’s d effect size (b = −.31, SE = .05, 95% HDI [−.40, −.22], d = .55).
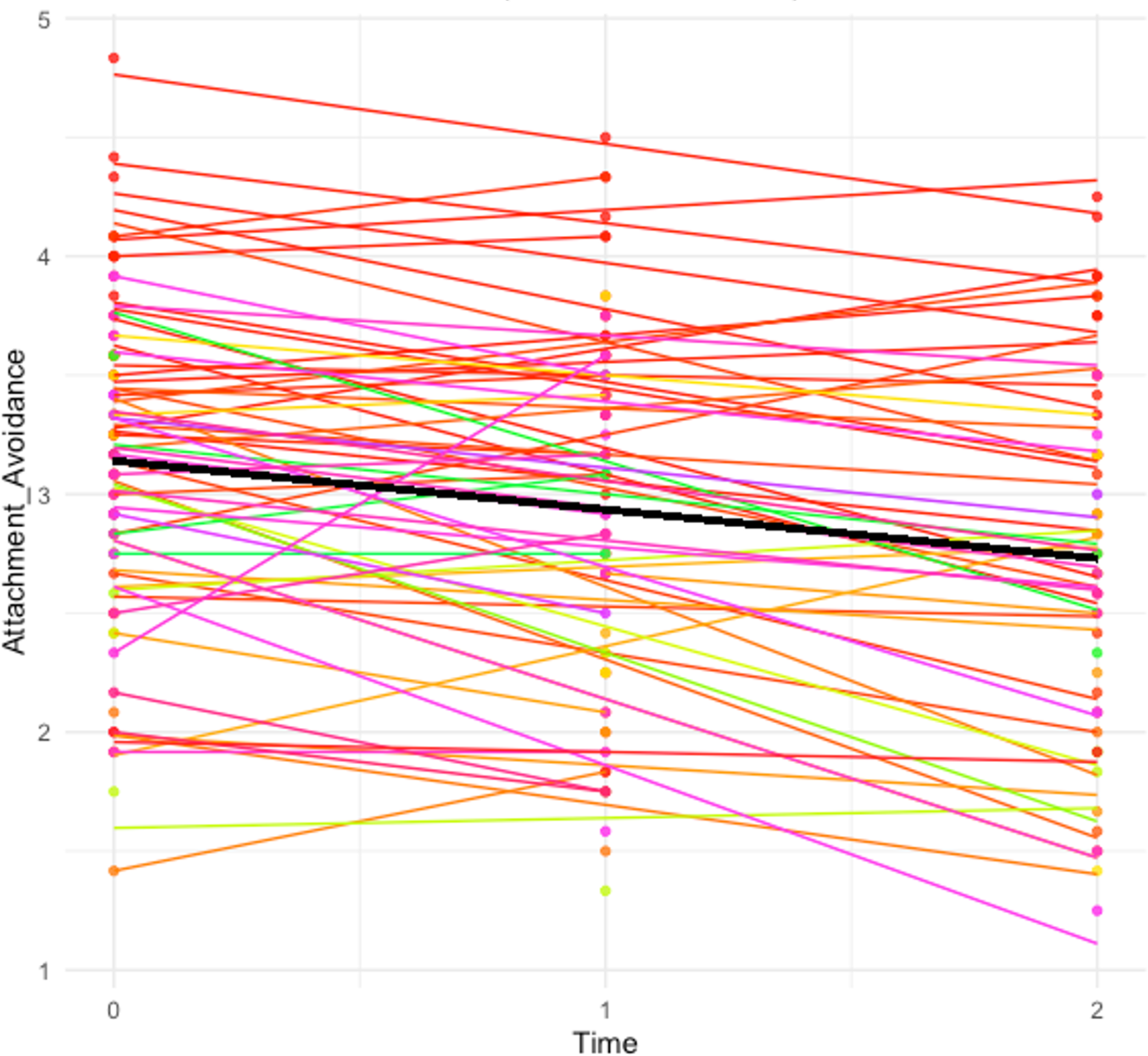
Changes in attachment avoidance across 5 weeks. Note. On average, participants also reported decreases in attachment avoidance across 5 weeks, yielding in a medium Cohen’s d effect size (b = −.22, SE = .03, 95% HDI [−.28, −.16], d = .51).
How do attachment insecurity, emotion regulation, and mental health outcomes change throughout mentorship?
Changes in attachment anxiety and avoidance
As predicted, the two dimensions of attachment insecurity decreased over time. On average, attachment anxiety decreased (b = −.31, SE = .05, 95% HDI [−.40, −.22], d = .55), and attachment avoidance decreased (b = −.22, SE = .03, 95% HDI [−.28, −.16], d = .51) at each two-week interval (see Figures 2 and 3).
Changes in difficulties with emotion regulation
As predicted, participants self-reported decreases in difficulties with emotion regulation (b = −.20, SE = .03, 95% HDI [−.26, −.15], d = .51).
Changes in depressive symptoms
Large decreases were noted in depressive symptoms on the Beck Depression Inventory (b = −2.85, SE = .34, 95% HDI [−3.53, −2.21], d = .55).
Changes in worry
Contrary to our prediction, there was no association between and time (b = −.04, SE = .66, 95% HDI [−1.33, 1.28]).
Changes in loneliness
Loneliness decreased on average (b = −.16, SE = .03, 95% HDI [−.23, −.09], d = .41).
Changes in self-esteem (exploratory)
Self-esteem increased on average (b = .14, SE = .02, 95% HDI [.10, .18], d = .41).
Correlations across time
Bayesian pearson change correlations for key study variables.
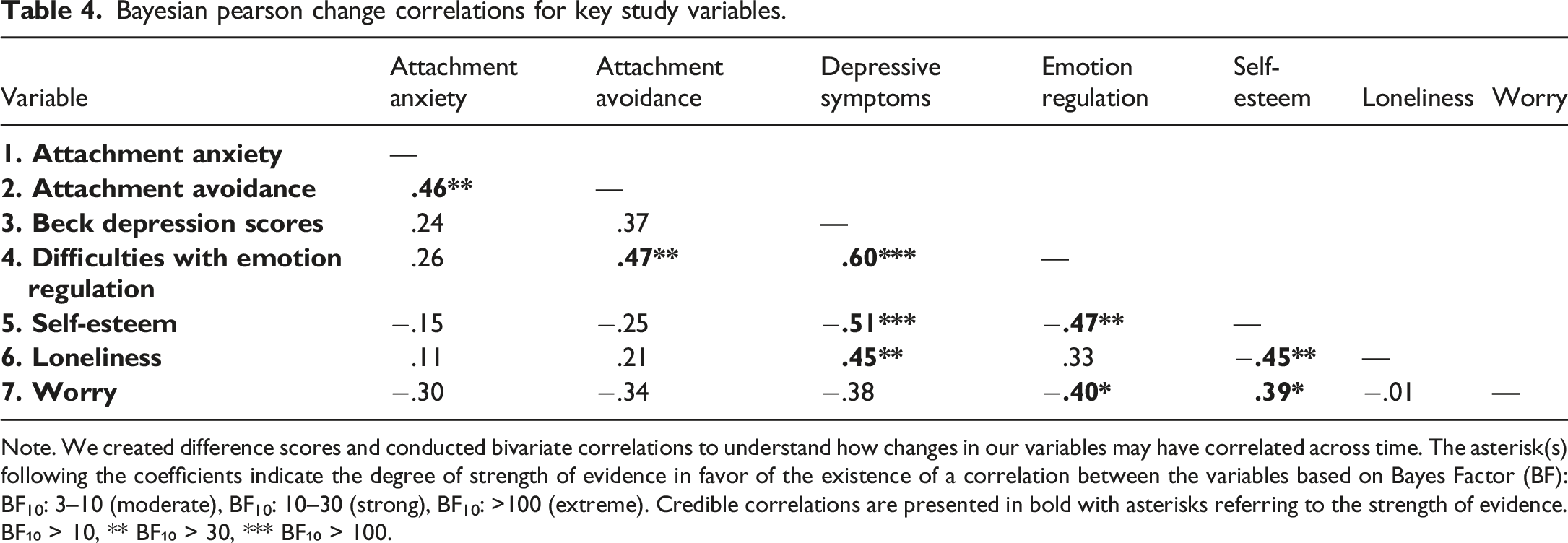
Note. We created difference scores and conducted bivariate correlations to understand how changes in our variables may have correlated across time. The asterisk(s) following the coefficients indicate the degree of strength of evidence in favor of the existence of a correlation between the variables based on Bayes Factor (BF):
BF10: 3–10 (moderate), BF10: 10–30 (strong), BF10: >100 (extreme). Credible correlations are presented in bold with asterisks referring to the strength of evidence.
BF₁₀ > 10, ** BF₁₀ > 30, *** BF₁₀ > 100.
Is the 5-week EFM intervention likable and acceptable?
Eighty-eight percent of participants reported that the program “definitely” improved their ability to have healthy relationships, and 12% reported that the program “somewhat” improved their ability to have healthy relationships. We observed the same pattern regarding whether participants believed the program improved their psychological wellbeing—88% noted that EFM “definitely” improved their psychological wellbeing and 12% indicated that EFM “somewhat” improved their psychological wellbeing. No participants indicated “Not at all” on our 3-point scale, signifying that everyone who completed the program felt they benefited psychologically or interpersonally. Furthermore, 100% of participants who finished the program noted that they would recommend the program to a friend.
Discussion
Long-standing interpersonal emotion dysregulation patterns characterize attachment insecurity. Across the lifespan, insecure attachment orientations represent a transdiagnostic predictor of psychopathology (Kassel et al., 2007; Nada Raja et al., 1992). Based on Emotionally Focused Therapy (Johnson, 2019), the current study presents a novel psychotherapeutic peer mentorship program designed to promote attachment security for insecurely attached participants during the transition to college. Although EFM can be adapted for other stages of life, we targeted the transition to college, given that youth face multiple social stressors, such as navigating new friendships or romantic relationships while maintaining connections with family. Emotionally Focused Mentoring (EFM) pairs lay therapists (or mentors) who rank high on attachment security with insecurely attached first-year college students (mentees) and targets attachment security and mental health outcomes by shaping interpersonal emotion regulation skills within a safe mentoring relationship. In the current study, we trained mentors to help their mentees understand their attachment tendencies while learning to identify and express their emotions to close others in an open, balanced manner rather than resorting to learned anxious/avoidant strategies. The development of EFM aligns with the NIH Stage Model of intervention development (Onken et al., 2014). Following a feasibility and acceptability investigation (Manvelian, 2021), this study examined EFM in an open trial with a larger sample (N = 82), but no control group, to first evaluate its ability to produce clinically meaningful within-person changes in attachment security, emotion regulation, and mental health outcomes across five weeks of EFM. We also continued the assessment of EFM’s acceptability by asking participants whether they would recommend the program to a friend and how much they believed the program improved their psychological wellbeing and their ability to create healthy relationships.
Changes in attachment security, emotion regulation, depressive symptoms, loneliness, and self-esteem
In line with the preregistered hypotheses (https://osf.io/zhpj6/?view_only=6b198aa2d92b48568e8b0f2a0be976b1), participants in the five-week EFM intervention reported improvements in attachment security, noting decreases on the dimensions of attachment anxiety and attachment avoidance. Participants also reported improvements in self-esteem, emotion regulation difficulties, and loneliness, yielding medium Cohen’s d effect sizes. Although the lack of a control group precludes claims of causality, these results demonstrate the potential power of a secure, trained peer mentor in improving attachment security and mental health outcomes for insecurely attached incoming college students in just 5 weeks. Mentors served as a safe haven and secure base for mentees, helping them develop the capacity to reflect on familial, peer, and romantic experiences, notice emotional avoidance, and practice expressing one’s emotions with greater skill and confidence. EFM showed promise to promote the use of adaptive interpersonal regulation strategies with the support of a mentor, indicating it is a potential treatment of transdiagnostic targets, such as holding a negative view of oneself or others, feeling lonely and isolated from others, or experiencing emotion dysregulation.
The assessment of feasibility and acceptability
We had 55 participants who completed the program (N = 55 of 82 or 67%). We believe there were several reasons for discontinuation, including no longer needing research credit, not returning after winter break, discontinuing after experiencing potential increases in worry, and stress related to the COVID-19 pandemic/academics. Future studies should work to mitigate these consequences as appropriate while recognizing that Emotionally Focused Mentoring may not be the best fit for every teen during this challenging phase of life.
All participants who completed the program indicated that EFM “definitely” or “somewhat” improved their ability to have healthy relationships. Similarly, all participants reported that EFM improved their psychological wellbeing and would recommend it to a friend. Participants received no monetary incentives, and yet, 55 participants attended all five sessions of EFM. Although it is unknown why other participants discontinued the study, EFM may be particularly helpful, likable, and beneficial to specific insecurely attached youth.
Even prior to the COVID-19 pandemic, the mental health needs of university students were increasing, exceeding the resources available on most college campuses (Oswalt, 2020). Thus, a program like EFM that leverages peer mentoring and promotes attachment security as a transdiagnostic lever for change could be a low-cost first line of treatment for students experiencing psychological or social difficulties. Leading to the development of a stepped care model, mentors can serve as lay therapists under the supervision of licensed clinicians, alleviating the extraordinary mental health demands placed on clinicians and allowing them to serve more patients. If a higher level of care is needed, mentors can refer their mentees to a licensed mental health clinician or a higher level of care, as done in this study.
Limitations and future directions
Our study has several limitations, all of which present opportunities for follow-up research. First, this pilot study used a small sample size of participants and was correlational in nature; thus, we cannot establish causal effects. A larger randomized clinical trial (RCT) is needed to establish whether EFM can improve attachment security and psychosocial wellbeing compared to a control condition, allowing us to account for the impact of extraneous variables. Second, although our sample was economically and racially diverse, including minority groups such as gender minorities and first-generation college students, it compromised of mostly female participants. Although the need for attachment is thought to be a biologically embedded, universal survival mechanism (Agishtein & Brumbaugh, 2013; Bowlby, 1982), the way that attachment needs are expressed can vary based on culture, gender, and other demographic factors. Thus, future studies could focus on recruiting more men and providing cultural humility training to mentors, helping them tailor EFM to promote attachment security based on each participant’s background and presentation (Kwon et al., 2013). Future studies should also assess for disability status, as this may impact the way that attachment tendencies are expressed or experienced.
Another consideration for EFM is the high suicidality rate that can accompany attachment difficulties. Supporting the Interpersonal Theory of Suicide, those who rank higher on attachment insecurity are more prone to experiencing thwarted belongingness, perceived burdensomeness, and relationship dysfunction, all of which can precede suicidal ideation or attempts (Sheftall et al., 2013). We observed this pattern in the present study, with approximately 27 participants (33% of the sample) reporting suicidal ideation in the past 2 weeks at baseline. As such, mentors were trained in suicide assessment, protocol, and referral. In future studies recruiting participants with attachment difficulties, the delivery of EFM should incorporate proper assessment and referrals for participants who endorse suicidality, particularly for adolescents and college populations (Mortier et al., 2018).
Another important question that can be addressed by using follow-up assessments in future studies is whether EFM can create sustainable changes beyond the duration of the intervention. Future RCTs should identify the conditions that give rise to the greatest sustainable changes in attachment security. To optimize EFM, future RCTs could also test if the attachment style of the mentor impacts participant outcomes and if more sessions of EFM might lead to bigger or more lasting increases in attachment security.
Moreover, the revision of EFM may benefit from a more thorough review of the mechanisms that promote attachment security with special consideration for the different dimensions of anxiety versus avoidance. For example, through the Attachment Security Enhancement Model, Arriaga and colleagues note that attachment anxiety can be decreased in situations that promote more positive models of the self and confidence in the self. In contrast, attachment avoidance might decrease in situations that involve more positive views of others, such as healthy patterns of dependence (Arriaga et al., 2018). Changing these negative models of self/other may require more exposure to one’s mentor and a diversity of attachment-related situations; nevertheless, we remain optimistic that even brief evidence-based interventions can bring about meaningful attachment changes.
Conclusion
Attachment insecurity is a transdiagnostic marker of distress associated with an array of adverse biopsychosocial outcomes, yet few interventions are peer-led and directly target attachment insecurity for participants during the transition to college. We designed EFM as a psychotherapeutic mentorship program to address this gap to promote attachment security for at-risk first-year college students. EFM is an experiential, attachment-based intervention where securely attached trained mentors are paired with more insecurely attached mentees. Mentors work with mentees to improve interpersonal emotion regulation skills to help them connect with close others. This initial investigation of EFM demonstrated within-person improvements in attachment security and related outcomes, including attachment avoidance, attachment anxiety, loneliness, depressive symptoms, difficulties with emotion regulation, and self-esteem. These results cannot speak to the causal effects of EFM. However, a randomized control trial could assess whether promoting healthy emotion regulation skills through a securely attached mentor can serve as a first-line defense, providing low-level, high-impact clinical care for youth compared to control conditions. We intend to further refine and test EFM, aiming to produce an innovative, implementable, and cost-effective intervention that can alter the lens through which insecurely attached youth perceive themselves, others, and the world.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author’s work on this project was supported by a Graduate Research Fellowship from the National Science Foundation (2017217558).
IRB protocol
IRB approval for this project was obtained from the Human Subjects Protection Program at the University of Arizona (Protocol # 1901276700).
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was pre-registered. The aspects of the research that were pre-registered were the aims, study design, and data analyses. The registration was submitted to the Open Science Framework: https://osf.io/zhpj6. Along with the intervention manual, the data used in the research are publicly posted and can be obtained here on the Open Science Framework: ![]() . Please contact Atina Manvelian
. Please contact Atina Manvelian