
Abstract
Informal caregivers provide critical support to the growing population of individuals diagnosed with Alzheimer’s disease and related dementias (ADRD). To assist caregivers, researchers’ dominant theoretical model has been a stress and coping approach for nearly four decades. Although the stress and coping approach is appropriate for many caregivers, it may be too narrow a lens for understanding caregivers who are primarily focused on maintaining their relationship with their loved one and providing the highest quality of care. This study was designed to empirically explore Shared Identity Theory, which emphasizes the inherent value of the relationship between care partners (“shared identity”) and how their shared identity relates to caregiver burden and exemplary care. This exploratory study examined Shared Identity Theory using structural equation modeling in a national sample of 263 informal ADRD caregivers. Our analyses provided support for an overall factor of Shared Identity that explained its four component factors (Communal Orientation, Communal Strength, Collective Identity, and Shared Goals). We then found that shared identity had a substantial positive relationship with exemplary care and a substantial negative relationship with caregiver burden. Shared identity seems to benefit both care recipients and the caregiving relationship. This study suggests the importance of expanding the scope of the caregiving literature to include a primary focus on this powerful relationship.
Introduction
Demographics in the United States are rapidly changing, with older adults expected to outnumber children in less than two decades (Vespa et al., 2018). As the U.S. population ages, cases of Alzheimer’s disease or related dementias (ADRD) are expected to rise dramatically from the current 6.2 million to 13.8 million by 2060, pointing to a demand for caregivers to assist this growing population (Alzheimer’s Association, 2023). Increasing age is the greatest known risk factor for developing ADRD, with the risk of developing ADRD doubling every five years after 65 years old (Alzheimer’s Association, 2023).
Unpaid or “informal caregivers” provide critical support and most of the help to individuals diagnosed with ADRD (National Alliance for Caregiving & AARP, 2015). In 2019, there were approximately 16.3 million informal caregivers of people with ADRD in the U.S., providing an estimated 18.6 billion hours of assistance, valued at approximately $244 billion (Alzheimer’s Association, 2020). Compared to caregivers of individuals without dementia, ADRD caregivers provide more care on average per month and such caregiving eventually becomes a one-sided form of helping as the disease progresses. Despite the prevalence and importance of caregiving, the National Academies of Sciences, Engineering and Medicine (2016) reports that “the need to recognize and support caregivers is among the most significantly overlooked challenges facing the aging U.S. population, their families, and society” (p. 1).
Caregiver burden and quality of care
In researchers’ efforts to understand and support caregivers, they frequently have focused on the extensive costs of this role. This understandable emphasis on the many emotional, physiological, social, and financial costs is often termed “caregiver burden” (Zarit et al., 1986). Dementia caregivers tend to experience more stress and depression in comparison to caregivers of people without dementia (Alzheimer’s Association, 2020), as well as a high degree of burden (46%) compared to caregivers of people without dementia (38%; National Alliance for Caregiving & AARP, 2015). Although some research suggests that caregiving stress can increase susceptibility to adverse physical health outcomes (Lovell & Wetherell, 2011), other research suggests that caregivers had lower mortality than non-caregivers (Roth et al., 2018).
Researchers have found that caregiver burden also negatively relates to the quality of care that caregivers provide (Harris et al., 2011). “Quality of care” has been defined as a multidimensional construct (Christie et al., 2009), which includes (a) exemplary care (Dooley et al., 2007), (b) caregivers’ responsiveness to care recipients’ needs (Morrow-Howell et al., 1998), and (c) the absence of potentially harmful caregiving (Williamson & Shaffer, 2001). Dooley et al. (2007) defined exemplary care as caregivers helping their care recipients “maintain a sense of dignity, self-respect-and ego integrity” (p. 360). We focused on exemplary care because it refers to the highest quality of care in comparison to adequate care or the simple absence of potentially harmful caregiving. Including exemplary care and caregiver burden allowed us to focus both on the best form of care and on how caregiving can be burdensome. Caregiver burden negatively relates to exemplary care (Harris et al., 2011) and positively relates to abuse of dementia patients and increased odds of nursing home placement (Stall et al., 2019).
Shared identity theory
Because caregiving research has been focused on caregivers’ stress and its negative links with quality of caregiving, scholars have naturally focused on a stress and coping lens to understand the caregiving experience (McClendon & Smyth, 2013; Pearlin et al., 1990). Although the stress and coping framework is essential in understanding many caregivers’ experiences (which we describe below), there is a need to broaden the theoretical perspective to more fully encompass the variations in caregiving. Specifically, Lang and Fowers (2019) argue that it is critical to expand the conceptualization of the Alzheimer’s caregiving relationship beyond a caregiver- and burden-centric perspective with their Shared Identity Theory (Lang & Fowers, 2019). Rather than focusing solely on one member of the dyad, this theory emphasizes the inherent value of the relationship between care partners (“shared identity”) and how this shared identity relates to caregiver burden and exemplary care. This perspective emphasizes the human capacity for loving relationships and how these relationships inspire action, such as exemplary caregiving.
Although prior research has examined related concepts of relationship quality, we believe the construct of shared identity deepens the conceptualization of the relationship in two ways. First, this research uniquely captures care partners’ rich history together, a perceived oneness in their identity, the communal strength of their relationship, the extent of the caregiver’s communal orientation, and their shared goals. These features add considerable depth to a conceptualization of a central relationship beyond the relationship satisfaction (Lawrence et al., 1998) or closeness (Whitlatch et al., 2001; Fauth et al., 2012) that comprise the extent of momentary assessments of the caregiving relationship (when that relationship is assessed at all). This deeper conceptualization of the care partners’ relationship is necessary to understand the complexity of their relationship and how this relationship, built over the years (i.e., prior to dementia onset and thereafter), relates to important caregiving outcomes—exemplary caregiving and caregiver burden. Second, the study investigates the theoretical structure of shared identity for understanding close relationships in ADRD, a unique model that has not been investigated until present and that further broadens the stress and coping theories, which we outline below.
Expanding the conceptualization of caregiving
The primary way we are attempting to expand the conceptualization of caregiving is that whereas many stress and coping caregiving researchers underemphasize a central aspect of caregiving—the relationship between the caregivers and the care recipient, we are interested in deepening the assessment of this aspect of caregiving. These scholars primarily focus on caregivers’ coping styles regarding their stress, and minimally account for the relationship between caregivers and care recipients. Coping researchers do discuss the care partners’ changing relationship in some ways, including the stress tied to the loss of intimate exchange between care partners (i.e., relational deprivation, Pearlin et al., 1990) and attributing recipients’ increasing behavioral and psychological symptoms to this loss to care (Boss & Yeats, 2014). Researchers also focus on the ambiguous loss caregivers face with ADRD, as they are unable to predict the pattern of their loved one’s decline. Several researchers also have attempted to capture the quality of the relationship between caregivers and care recipients (Quinn et al., 2012) by exploring constructs such as “relationship closeness” (Whitlatch et al., 2001; Fauth et al., 2012) and “relationship quality” (Lawrence et al., 1998). Prior studies of care partners’ closeness suggest that closer relationships may mitigate negative outcomes for care recipients, like behavioral symptoms (Perren et al., 2007) and cognitive and functional decline (Norton et al., 2009), with mixed outcomes for caregivers.
Although researchers have found that closeness between care partners was associated with reduced caregiver depression levels and caregiver burden (Williamson & Schulz, 1990), closeness prior to dementia was associated with worsened caregiver affect and overall mental health ratings longitudinally (Fauth et al., 2012). This literature on the associations of relationship closeness and outcomes for caregivers and care recipients is mixed and raises the question of how care partners’ relationship with their loved ones (both prior to dementia onset and currently) relate to caregiving outcomes and well-being.
Although this literature contributes to understanding caregiving relationships, researchers most often conceptualize closeness by measuring caregivers’ satisfaction with their relationship (McClendon & Smyth, 2013). Capturing caregivers’ relationship satisfaction minimally accounts for a lifelong relationship with its rich history and depth. Lang and Fowers (2019) predicted that the richer, deeper, and more multidimensional concept of shared identity strongly influences caregivers’ experiences. Many caregiver actions and experiences cannot be accounted for if attention is limited to relationship satisfaction. Therefore, we suggest a broader perspective to more fully encompass the variations in caregiving.
A need for broadening theory
Because caregiving research has been focused on caregiving stress and its negative links with quality of caregiving, scholars have adopted a stress and coping lens to understand the caregiving experience (McClendon & Smyth, 2013; Pearlin et al., 1990). For instance, Pearlin et al. (1990) provided a seminal model, the “stress process paradigm” to help explain how caregiving stress affects mental and physical health among informal ADRD caregivers. They defined caregiver burden as a subjective stressor, which is affected by the caregivers’ demographic factors and their caregiving history (e.g., pre-dementia relational conflict). Pearlin et al. (1990) suggested that care recipients’ behavioral and psychological problems, relational deprivation (i.e., the loss of a confidant in their loved one), and caregiver burden affect mental and physical outcomes both directly and indirectly. The researchers suggested that various coping techniques and social support can buffer the effects of burden on stress outcomes. Other researchers have expanded this model to include quality of caregiving outcomes as well (e.g., McClendon & Smyth, 2013).
Many dementia researchers have adopted stress and coping models to guide their interventions targeting caregiver burden and quality of care (Schulz et al., 2020). However, research on the efficacy of these interventions has been mixed. Meta-analyses have found that interventions had no effect on caregiving burden (Acton & Kang, 2001; Brodaty et al., 2003). In contrast, Cheng et al.’s (2020) systematic review and meta-analysis of 131 randomized controlled trials suggested that these interventions resulted in small improvements in reduced burden/stress, depressive symptoms and anxiety, and these effects remained stable or grew in strength in follow-up periods. Given the inconsistent results across studies, it is reasonable to consider complementary theoretical directions that can provide greater understanding of the full range of caregiving experiences.
Extant stress and coping models have been critiqued theoretically as underemphasizing important aspects of the caregiving experience (Braithwaite, 1996; Lang & Fowers, 2019). Although a stress and coping approach may be appropriate for caregivers struggling with a high degree of burden, stress and coping models appear insufficient for understanding all caregivers’ needs because they imply that caregiving is a problem to be solved with stress relief for all caregivers. The universal application of stress and coping approaches may fit less well for caregivers who do not see caregiving as overly burdensome because they are dedicated to providing exemplary care rather than stress management. When caregivers are focused on a caring relationship with their loved one, interventions may need to emphasize caring more than coping.
One way to understand the limitations of stress process models is to recognize that the positive aspects of caregiving are not central in many coping theories (McClendon & Smyth, 2013; Pearlin et al., 1990), despite caregivers acknowledging the positive impact of this role (Lloyd et al., 2016). In a recent national poll, 85% of family caregivers described caring for a loved one with dementia as rewarding (National Poll on Healthy Aging, 2017). Lawton and colleagues’ (1991) two-factor model of caregiving appraisal acknowledges that caregiving can be both demanding and satisfying. Although these researchers have made strides in examining the positive aspects of caregiving, many stress and coping theorists neglect the positive aspects of these caregivers’ experience.
Building a complementary, broader perspective
Shared identity theory emphasizes the inherent value of the relationship between Alzheimer’s caregivers and their care recipient loved ones, expanding the existing literature’s predominant and pervasive focus on caregiver- and coping-centric approaches. Shared identity theory builds on four lines of theory and research that exemplify the human capacity for loving relationships and how these relationships inspire relationship behaviors: (a) communal orientation, (b) communal strength, (c) collective identity, and (d) shared goals.
First, drawing on Clark and Aragón (2013), “communal orientation,” which represents the caregiver’s general inclination to treat others communally, in contrast to a focus on benefit exchange between parties (Clark & Aragón, 2013). We believe that high-quality, informal Alzheimer’s caregiving likely follows these general communal norms as caregivers dedicate significant time to their loved one’s needs without expecting return benefits, a necessary aspect of communal relating that has not been explored in extant theory (Williamson & Schulz, 1990). We believe this is worth exploring because an individual inclination toward taking a communal approach to relationships in general is likely to underlie the ability to act communally. We expect communal orientation to predict communal behavior because it puts the caregiver in a position to want to act in the care recipient’s interests without expecting reciprocity. This desire to care for others is a foundational element for care that may not be reciprocated. Clark and Aragón contrast communal orientation with exchange orientation, in that one expects reciprocation in the latter and may even terminate relationships that are insufficiently reciprocal. We expected a positive relationship between communal orientation and shared identity, which means that strong shared identity will include a general orientation to less cost-counting in relationships.
Second, care partners’ shared identity includes “communal strength,” defined by Mills et al., (2004) as the degree to which care partners feel motivated specifically to provide for their loved ones’ needs. We argue that communal strength is an important aspect of shared identity given that the strength of the bond between care partners is essential in carrying them through daily challenging tasks. Despite the hardships of caregiving, care partners can respond readily to their loved ones’ needs and may feel quite distressed if they were unable to meet those needs. Communal strength may also contribute to greater meaning in caregiving as their loved ones’ needs are met.
Third, care partners’ shared identity includes “collective identity” as identity transcends the individual by also including close relationships and group memberships (Brewer, 2007). Brewer reported that when collective identity was activated, individuals displayed more other-oriented behaviors because the individual sees the self and the other as having shared interests. From this perspective, we anticipate that caregivers with a collective identity would view their relationship as an extension of themselves and perceive significant oneness with their care partner. Therefore, Lang and Fowers (2019) proposed that when caregivers share a collective identity with care recipients, it would encourage exemplary caregiving.
Fourth, Lang and Fowers (2019) argued that a shared identity includes care partners’ history of “shared goals,” or goals that can be achieved only with others, such as love, communication, or teamwork. This concept follows from Fowers’s (2015) view that human social nature predisposes us to pursuing shared goals, not just individual goals that can be achieved independently. Care partners often have a history of pursuing shared goals or actions together, such as building a family. Although their shared goals may shift as the care recipient declines, care partners can continue to practice shared goals together, such as continuing to share affection. Shared Identity Theory proposes that caregivers’ and care recipients’ communal orientation, communal strength, collective identity, and shared goals comprise a shared identity, making this unique relationship irreplaceable.
Some evidence indicates that one aspect of shared identity is related to caregiving quality. Several studies (Christie et al., 2009; Dooley et al., 2007; Williamson & Shaffer, 2001) found that communal relationships in caregiver dyads were positively associated with exemplary care and negatively correlated with potentially harmful actions. Researchers also found that family satisfaction, cohesion, communication and empathy were positively associated to caregiver quality (Panyavin et al., 2015). The literature suggests that family relationships between caregivers and care recipients play a significant role in caregiving.
The present study
This exploratory study was designed to empirically investigate Lang and Fowers’s (2019) Shared Identity Theory to deepen the understanding of dementia caregiving beyond caregiver- and coping-centric perspectives of stress and coping models using structural equation modeling. Our initial aim was to assess the first empirical model of shared identity. Our primary hypothesis was that a second order factor structure would emerge with communal orientation, communal strength, collective identity, and shared goals as first order factors and shared identity as a second order factor, following Shared Identity Theory. In other words, the hypothesis is that a general second-order factor of shared identity accounts for each of the four first order factors. As Kline (2015) describes this procedure, “the second order factor is measured only indirectly through the indicators of the first-order factors” (p. 319). That is, the observed (measured) variables are accounted for by the first order factors and the first order factors are accounted for by the second order factor. Our second aim was to examine whether shared identity is negatively related to caregiver burden. Our final aim was to assess whether shared identity would be positively related to exemplary caregiving.
Method
Transparency and openness
The deidentified data and the Mplus syntax is available on the Open Science Framework The url is: https://osf.io/bp39c/ Neither the hypotheses nor the analytic plan was pre-registered.
Participants
A power analysis indicated that for a power level of .90, 209 participants would be necessary to estimate a RMSEA of .09 with 519 degrees of freedom (Preacher & Coffman, 2006). This exploratory study included a national sample (U.S.) of 263 informal dementia caregivers. Inclusion criteria included being at least 18, providing unpaid care for at least 15 hours per week for the past year, caring for a romantic partner or relative diagnosed by a neurologist or psychiatrist with ADRD, residing in the United States, English literacy, and the absence of any motor or visual impairments that impair survey completion. Caregivers were recruited utilizing web-based sampling (i.e., via the Alzheimer’s Association’s “TrialMatch” and dementia caregiver Facebook support groups), convenience sampling (i.e., in local adult daycare centers, and geriatric research and practice settings in Miami, FL), and snowball sampling techniques. Participants were offered an incentive of a $10 Amazon gift card or to use this incentive as a donation to the Alzheimer’s Association. Most caregivers (62.3%) selected the donation option.
Demographic Characteristics of Participants (N = 263).

Procedures
Following IRB approval, we piloted the survey with seven caregivers to assess the length and administration of the survey. Based on participant feedback, some items were revised for readability and the final survey was administered in either a web-based or a paper survey, depending on the participant’s needs. Participants first completed the informed consent page and screening questions to indicate appropriateness for the study. Those meeting the inclusion criteria completed the survey measures. Most participants completed the online survey through the Qualtrics website for the web-based format. Participating geriatric practitioners provided the paper format in their offices.
Measures
Predictor measures
Communal orientation
Communal orientation was measured with the Communal Orientation Scale (COS; Clark et al., 1987), a 14-item scale that assesses how important it is to be responsive to others’ needs and feelings. A sample item was, “I believe people should go out of their way to be helpful.” Additionally, the COS measures the participant’s expectation that others will interact with them communally. The original measure included a 5-point scale ranging from “1 = extremely uncharacteristic of me” to “5 = extremely characteristic of me”; however, the responses options were modified to “1 = extremely unlike me” to “5 = extremely like me” based on pilot participant feedback. Following the guidelines of Brown (2015) and Pallant (2005), we conducted a one-factor confirmatory factor analysis (CFA) on the COS and removed items if they had standardized factor loadings below .3, or if the loadings were conceptually inappropriate to our research questions (See Supplemental Materials, Supplementary Table S1 for all removed items from each scale). We assessed all measures in this study with this approach. Accordingly, four items were removed from the COS, resulting in a revised scale of 10 items. The removed items focused on respondents’ expectations of others being responsive to their personal needs and feelings. Because our research questions pertained to respondents’ caregiving approach, we only retained items focused on how they expect to treat others. The 10 individual items were used as indicators of communal orientation. Williamson and Schulz (1990) found adequate reliability for the COS with a sample of Alzheimer’s caregivers (α = .70). In this study, the internal consistency was acceptable (α = .71).
Communal strength
The Communal Strength Measure (Mills et al., 2004) assessed the caregivers’ motivation to respond to their care recipient’s needs. For instance, a sample item included, “How high a priority for you is meeting the needs of the care recipient?” The original scale included 10 items, with an 11-point agreement scale ranging from “0 = not at all” to “10 = extremely.” Following the same procedure used with the COS, two items were removed based on low factor loadings. The eight individual items were used as indicators of communal strength, with one item reverse scored. This measure demonstrated internal consistency among college students (α ranging from .84 to .95; Mills et al., 2004). After removing the two items the internal consistency in this sample was acceptable (α = .78).
Collective identity
The Relationship Closeness Scale (RCS; Noelker, 1996, Whitlach et al., 2001) and the Inclusion of Others in the Self Scale (Aron et al., 1992) assessed the collective identity of care partners. The RCS is a 6-item measure of perceived closeness, a 4-point agreement response scale, and two items reverse scored. A sample item is: “My relationship with my relative has always been close.” Caregivers answered the same questions based on the relationship at the time of the assessment (i.e., postdementia diagnosis) and prior to dementia onset (i.e., predementia diagnosis), as suggested by Fauth et al. (2012). Based on a one-factor CFA for each scale, all items were retained for the final analyses as indicators of collective identity. The postdementia scale demonstrated internal reliability in previous dementia caregiver samples (α = .90; Whitlatch et al., 2001 and .86; Fauth et al., 2012). Because we modified the RCS for this study, we report the internal consistency for those modifications here (the RCS postdementia questionnaire α = .73 and the RCS predementia questionnaire α = .89).
The Inclusion of Others in the Self Scale (Aron et al., 1992) is a single-item, pictorial measure of closeness with others. Participants selected one of the seven Venn-diagram like pictures with varying degrees of overlap to best portray their relationship with their care recipient. Aron et al. reported a two-week test-retest reliability of .83 and an alternate form reliability of .93. Because it is a single-item indicator, we could not analyze its internal consistency in this sample.
Shared goals
Shared goals were measured with revised items of the Relationship Flourishing Scale (Fowers et al., 2016). The original 12-item scale is based on a theory of romantic relationship flourishing, with one of the measured domains as goal sharing. The original 12-item scale was assessed for reliability and validity by Fowers et al. (2016). For this study, shared goals was measured with 3 items adapted from the shared goals domain. The following items were included: “I have had more success in my important goals because of the care recipient’s help,” “The care recipient has shown interest in things that are important to me throughout our relationship,” and “It is natural for me to do things that continue to keep our relationship strong.” We examined the internal reliability of these three items and found an alpha coefficient of .66.
Outcome measures
Caregiving burden
The 12-item self-report version of the Zarit Burden Interview (ZBI; Bédard et al., 2001) measured caregivers’ subjective burden. Caregivers rated items on a response scale ranging from “0 = never” to “4 = nearly always.” A sample item is “Do you feel that you have lost control of your life since your relative’s illness?" The short version of the ZBI demonstrated internal consistency in a sample of family caregivers (α = .88; Bédard et al., 2001) and a sample of informal caregivers (α = .87; Quinn et al., 2012). The one-factor CFA on the ZBI led to removing one item from the scale, resulting in 11 items for the final analyses and an acceptable internal consistency in this sample (α = .90). The mean item scores were calculated, with higher scores representing greater burden.
Exemplary care
The Exemplary Care Scale (Dooley et al., 2007) is an 11-item self-report scale, with a response scale, ranging from “1 = never” to “4 = always.” A sample item is: “When at all possible, I make sure that (care recipient) gets to do some of the things that he/she enjoys [e.g., visiting friends, listening to music].”) Harris et al. (2011) found a one-factor solution with a CFA and internal consistency in a diverse sample of dementia caregivers (α = .74). A CFA with this sample led to retaining all items of the scale and an acceptable internal consistency (α = .80). The mean item scores were calculated, with higher scores representing more exemplary care.
Control variables
Social desirability
Given that self-report measures were used to assess all constructs, we assessed the degree of socially desirable responding with the 16-item Balanced Inventory of Desirable Responding Short Form (BIDR-16; Hart et al., 2015). This measure includes Impression Management (IM) and Self-Deception enhancement (SD) scales, with eight items each. IM represents a tendency to rate oneself consciously in an inflated manner, while SD captures an unconscious inclination to perceive oneself positively (Hart et al., 2015). The response scale ranged from “1 = not true” to “7 = very true”. A sample item is “I never regret my decisions.” The subscales demonstrated adequate internal consistency in diverse samples of adults (α ranged from alphas.63 to .84, for SD and from .66 to .74 for IM; Hart et al., 2015). In this sample, the internal consistencies of the two scales are adequate (α = .75 for SDE and α = .71, for IM).
Demographic characteristics
Caregivers shared basic demographic information, including their relationship to the care recipient, the length of time they have provided care for this individual, and the number of weekly hours they provided care. Caregivers were also asked, “What is the care recipient’s stage of dementia?” with the following response choices: early (forgetfulness, memory loss), middle (wandering, agitation), and late (incontinent, speech difficulties, bedbound). Caregiving stages included 32.3% in the early stage, 44.1% in the middle stage, and 23.6% in the late stage.
Analytic plan
We used RStudio to assess the pattern of missingness and to investigating whether the assumptions of SEM were met (RStudio Team, 2015; Version 1.0.136). Only .001% of the data were missing, and the assumptions of (a) normality, (b) multicollinearity, and (c) linearity were met.
We utilized the Mplus Version 8.2 to analyze the proposed hypotheses (Muthén & Muthén, 1998). We followed Kline’s (2015) recommended two-step approach to SEM to examine Lang and Fowers’s (2019) Shared Identity Theory (i.e., Aim 1). We first assessed the proposed second order factor measurement model. When a measurement model revealed misfit, we modified the model structure based on the theory of shared identity and guided by the fit indices. Once the measurement model estimated good fit to the data, we followed the second step to estimate the hypothesized structural model (i.e., Aims 2 and 3), which included caregiving outcomes. Given that the model included a single-item indicator (Inclusion of Others in the Self) for a first order factor, we treated that measure as categorical and used the weighted least square mean and variance adjusted (WLSMV) estimator from Mplus for all SEM analyses. The WLSMV estimator handled missing data with casewise deletion (Muthén & Muthén, 1998). The polychoric correlation matrix table for the variables is found in Supplementary Table S2 in the Supplemental Material.
Results
Measurement model
Second-order factor measurement model of shared identity
The hypothesized measurement model included four first-order latent variables: Communal Orientation, Communal Strength, Collective Identity, and Shared Goals (Figure 1). The hypothesized indicators for each latent variable were the eponymous scale items, except for Collective Identity. We anticipated that the indicators of the Collective Identity latent variable would include the six items of the Relationship Closeness Scale-Predementia, the six items of the Relationship Closeness Scale- Postdementia (Whitlach et al., 2001), and the single-item Inclusion of Others in the Self Scale (Aron et al., 1992). We predicted that these four first order factors would be explained by a second-order latent variable we named Shared Identity (Figure 1). Proposed Structural Model of Shared Identity Theory. COS: Communal Orientation Scale; CS: Communal Strength; RCS: Relationship Closeness Scale; RCSP: Relationship Closeness Scale Post-Dementia Onset; IOS: Inclusion of Others in Self Scale; RFS: Relationship Flourishing Scale.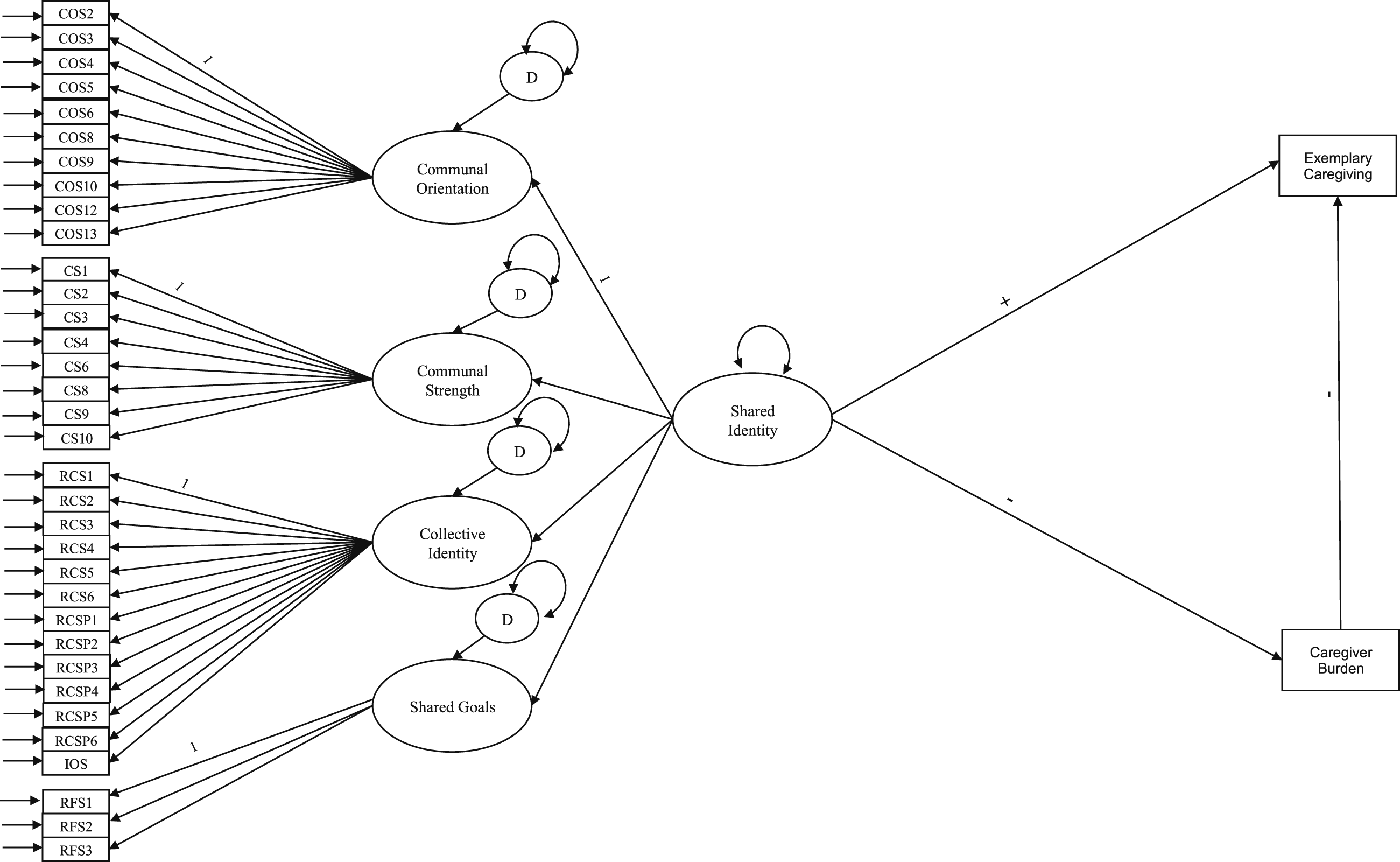
To test the hypothesized measurement model of Shared Identity, we conducted a CFA. This second-order measurement model converged on a solution and revealed adequate fit: CFI = .92; TLI = .92; SRMR = .07; RMSEA = .06 (90% CI = .05, .06). All first order factors were significantly and positively related to the second order factor of Shared Identity (Figure 2). We allowed the error terms to correlate among theoretically related Relationship Closeness Scale items assessing the relationship predementia and postdementia based on modification indices and because these items assessed relationship facets that could be expected to remain consistent prior to and after dementia onset: “My relationship with my relative has always been close,” “My relative always makes me feel that whatever I do for him/her is not enough,” and “My relative is often critical of me.” We also allowed the residuals of the Shared Goals and Collective Identity variables to correlate, as it is theoretically likely that care partners with a collective identity would also have shared goals. Second-Order Factor Measurement Model of Shared Identity. Standardized coefficients for the second-order factor measurement model of shared identity are presented, with the standard errors in parentheses. Comparative fit index = .92; Tucker Lewis index = .92; standardized root mean square residual = .07; and root mean-square-error of approximation = .06 (90% CI = .05, .06). COS: Communal Orientation Scale; CS: Communal Strength; RCS: Relationship Closeness Scale; RCSP: Relationship Closeness Scale Post-Dementia Onset; IOS: Inclusion of Others in Self Scale; RFS: Relationship Flourishing Scale. All associations were statistically significant (p < .001).
Structural model
Given that the measurement model fit adequately, we defined the structural model, as recommended by Kline (2015; Figure 3). The subsequent structural model of Shared Identity predicting Exemplary Care and Caregiver Burden revealed good fit to the data: CFI = .91; TLI = .91; SRMR = .07; and RMSEA = .06 (90% CI = .05, .06). The findings indicate that Shared Identity is positively associated to Exemplary Care (β = .71, p < .001) and negatively associated with Caregiver Burden (β = −.51, p < .001). Structural Model of Shared Identity. Standardized coefficients for the structural model of shared identity are presented, with the standard errors in parentheses. Significant paths are represented by solid lines and non-significant paths by dashed lines. Comparative fit index = .92; Tucker Lewis index = .91; standardized root mean square residual = .07; and root mean-square-error of approximation = .06 (90% CI = .05, .06). COS: Communal Orientation Scale; CS: Communal Strength; RCS: Relationship Closeness Scale; RCSP: Relationship Closeness Scale After Dementia Onset; IOS: Inclusion of Others in Self Scale; RFS: Relationship Flourishing Scale. All paths with solid lines were statistically significant (p < .001).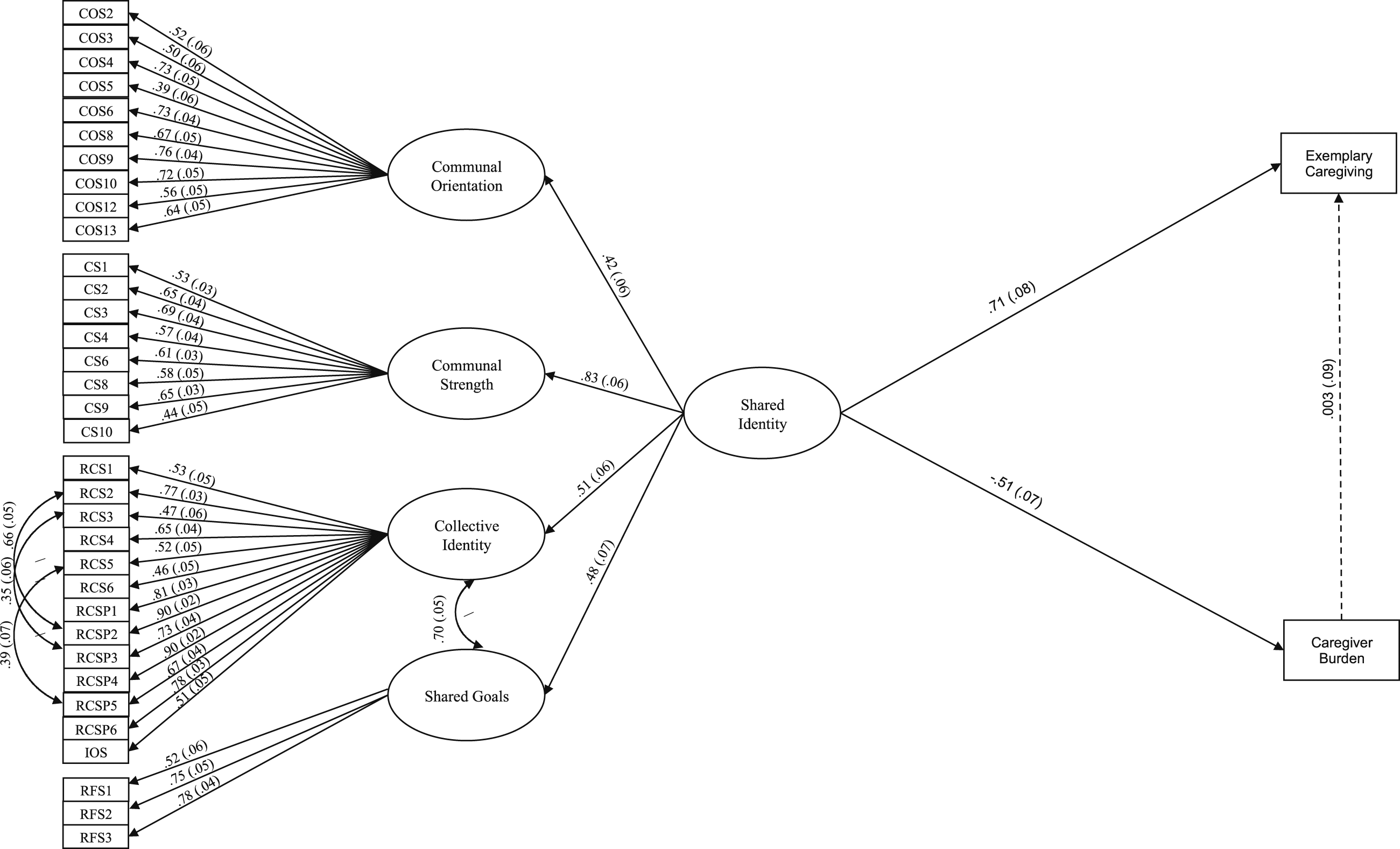
Structural model with covariates
Lastly, we added covariates to the structural model to assess whether these variables affected the strength and direction of the hypothesized relationships. We tested the associations between demographic variables and caregiving outcomes and found that one demographic variable was significantly correlated to caregiver burden: SD (r = −.29, p < .001). T-tests indicated differences in caregiver burden between men (M = 1.67, SD = .88) and women (M = 2.03, SD = .78), t(261) = −2.79, p = .006, between White caregivers (M = 2.02, SD = .79) and Black caregivers (M = 1.57, SD = .89), t(261) = 3.02, p = .003, between caregivers caring for loved ones in the early stages (M = 1.74, SD = .77) versus the middle stages (M = 2.25, SD = .79) of dementia, t(261) = −5.17, p < .001, and between caregivers who lived with their loved one (M = 2.08, SD = .78) versus not (M = 1.56, SD = .81), t(261) = 4.51, p < .001. Three variables were also associated with Exemplary Caregiving: SD (r = .31, p < .001), IM (r = .28, p < .001), and the care recipient’s age (r = −.05, p = .02).
As expected, the addition of the control variables reduced the fit of the structural model, with SRMR being particularly affected: CFI = .92; TLI = 92; SRMR = .18; RMSEA = .05 (90% CI = .04, .05). The only point of adding the covariates was to assess whether the magnitude of the relationship between Shared Identity and the criterion variables changed. These relationships were slightly decreased, but the standardized direct effect of Shared Identity on Exemplary Caregiving remained statistically significant (β = .65, p < .001), as did the negative association between Shared Identity and Caregiver Burden (β = −.45, p < .001).
Discussion
This study is the first to empirically examine Shared Identity Theory (Lang & Fowers, 2019), which suggests the importance of deepening the conceptualization of the Alzheimer’s caregiving relationship. We believe this study complements and expands the literature beyond the stress and coping framework because that framework does not capture the full range of caregiving experiences and therefore the needs for all caregivers. Our results indicate that shared identity, a neglected aspect of caregiving in stress and coping models, is related to both caregiver burden (negatively) and exemplary caregiving (positively). These results suggest the importance of the rich relationship between caregivers and their loved ones that results from an extensive relationship history and provides significant positive experience even during caregiving.
The creation of shared identity
This exploratory study found promising results for the construct of shared identity among informal Alzheimer’s caregivers. Structural equation modeling provided evidence for the second-order factor of Shared Identity and four first-order latent factors—Communal Orientation, Communal Strength, Collective Identity, and Shared Goals. The adequate fit of the measurement model suggested that Shared Identity can be measured as a second-order factor.
Communal orientation
The first-order latent factor of Communal Orientation loaded onto the second-order factor of Shared Identity, suggesting that caregivers’ communal orientation or style is an important aspect of shared identity. Caregivers’ openness and social responsibility to others appears to be an aspect of forming a close bond to a specific person in their life.
Communal strength
The first-order latent factor of Communal Strength loaded onto the second-order factor of Shared Identity, suggesting that communal strength is the strongest component of care partners’ shared identity. Communal strength indicated the priority that caregivers feel for meeting the needs of their loved one. Unique and special relationships often include substantial communal strength (Mills et al., 2004). For instance, adult children caring for their parents or romantic partners may be more willing to endure the hardships in caring for their loved one because they view the relationship communally. Because this scale assesses the respondent’s willingness to help a specific person, this scale is likely to be highly salient to an ADRD caregiver.
Collective identity
The first-order latent factor of Collective Identity loaded onto the second-order factor of Shared Identity, indicating that collective identity is a key component of shared identity. Many caregivers seem to share a collective identity through which they and their loved one have mutually shaped one another’s identity, meaning that caregivers tend see their care recipient loved one as an extension of themselves. Therefore, many caregivers help care recipients readily, viewing their assistance as a mutual benefit for both of them.
Shared goals
Lastly, the first-order latent factor of Shared Goals loaded onto the second-order factor of Shared Identity, indicating that goal sharing is a viable construct in the Alzheimer’s caregiving literature and is part of Shared Identity. In close relationships, both parties can develop shared goals over time, given the mutuality of their relationship. These goals can include love, teamwork, and handling shared suffering. Of course, not all relationships include a history of shared goals of love and affection. Some relationships are distant or exploitive, and these relationships likely consist of fewer shared goals.
The benefits of shared identity
This study suggests that shared identity may be beneficial for both caregivers and their loved ones. The significant negative association between shared identity and caregiver burden suggests that shared identity was inversely related to caregiver burden. This result is consistent with previous caregiver relationship quality studies (Quinn et al., 2012; Williamson & Schulz, 1990). Our study clarifies that caregiving may not be burdensome for all caregivers, requiring extensive coping strategies. Rather, some caregivers may experience caregiving as rewarding and meaningful, consistent with Shared Identity Theory.
Additionally, the results indicated that shared identity may serve as a critical component in supporting care recipients’ needs as well. Shared identity was positively associated with exemplary caregiving. Therefore, caregivers with stronger shared identity were more likely to individualize care while also respecting and promoting the dignity of their loved one. Whereas prior researchers found that caregivers’ close relationships with their loved one were associated with caregivers’ responsiveness to their partners’ needs and the absence of harmful caregiving behaviors (Chen et al., 2013; Williamson & Shaffer, 2001), our study highlighted the powerful relationship between this deep connection and exemplary care. Even as their loved one declines in later stages of illness; this bond may help caregivers provide the highest quality care. Therefore, shared identity appears to be strongly related to two key caregiving outcomes: negatively with caregiver burden and positively with exemplary caregiving.
Clinical implications of shared identity
This study suggests that Shared Identity Theory may have important implications for professionals serving informal caregivers. Shared identity appears to be prominent in the caregiving experience, suggesting that clinicians would be wise to carefully explore the caregivers’ relationships with their loved ones. Exploring how the relationship evolved can help clarify current relationship dynamics between care partners. In addition, this study suggests the value of assessing the shared history between care partners, such as the shared activities they enjoyed or memories they shared together.
Understanding the shared history and quality of the relationship between care partners can help practitioners tailor interventions to include elements of the stress and coping paradigm and/or a shared identity perspective. Our study suggests that the less shared identity caregivers reported, the more caregiver burden they experienced. Therefore, individuals with a lower degree of shared identity may benefit from stress and coping interventions to help them with experienced burden (e.g., an intervention such as Resources for Enhancing Alzheimer’s Caregiver Health (REACH) to address burden; [Gitlin et al., 2003]). This technologically advanced intervention includes psychoeducational materials, teaching caregiving skills, providing group support, and introducing active coping strategies. This approach may be helpful to the many people report feeling compelled to provide care because they are the only ones available. Their willingness to do so is admirable, even if it is not based on a positive relationship with the person with dementia.
In contrast, an exclusively stress and coping focus with those who have a strong shared identity with their care partner would likely be inappropriate. This study indicated that shared identity was inversely related to burden. Therefore, clinicians may assist these caregivers by providing opportunities to reflect on their memories of their loved ones and discuss the meaningful aspects of their new role. One potentially helpful intervention is reminiscence therapy, which helps caregivers and their loved ones by participating in shared activities to help promote the recollection of their history (Cotelli et al., 2012). These authors found that reminiscence therapy assisted in improving care recipients’ mood and cognitive abilities. Through reminiscing about shared experiences, the practitioner can help activate and strengthen the protective factor of care partners’ shared identity.
Although our study indicated that shared identity is inversely related to caregiving stress, some caregivers may still experience stress as their loved one declines and as their relationship shifts to a more one-sided form of care. Given the complexity and evolving nature of the care process, some caregivers may benefit from a combination of stress and coping and a shared identity approach to treatment. The unique importance of this study is in suggesting to researchers and clinicians that exploring the value of shared identity among caregivers, rather than adopting a one-size-fits-all approach. This can enable more nuanced assessments of which treatment approaches work best for whom.
Directions for future research
Future research is necessary to further assess the appropriateness of and extension of the Shared Identity approach for informal dementia caregivers. First, it is necessary to replicate these exploratory findings and to directly compare this model to the explanatory capacity of the widely accepted stress and coping framework. We recognize that the stress and coping approach is valuable for many caregivers (McClendon & Smyth, 2013; Pearlin et al., 1990) and therefore, this comparison can help practitioners and researchers in understanding the variety of caregiving experiences.
Second, future research should focus on developing measures designed specifically to assess shared identity to adequately represent this important construct. This initial exploratory study pragmatically utilized extant measures for an initial empirically evaluation of this concept. However, some of the indicators of shared identity were not originally validated with a sample of informal dementia caregivers, including the Communal Strength Measure (Mills et al., 2004), the shared goals items (Fowers et al., 2016), and the Inclusion of Other in the Self measure (Aron et al., 1992). Therefore, we recommend research designed to generate measures that more directly represent the four factors of shared identity, and to assess the construct validity of each new measure. Additionally, some demographic items were not previously validated, including the question: “What is the care recipient’s stage of dementia?” We encourage researchers to utilize validated measures of ADRD staging to adequately capture the care recipient’s presentation.
Third, we utilized individual items as the indicators for all first-order latent factors in our measurement model. All item indicators, except for the CSM scale, were treated as categorical. The CSM (Mills et al., 2004) has 11 response categories, and given so many categories, the items can barely be viewed as categorical, although the response options do not have equal intervals. We decided to treat the CSM items as continuous indicators for pragmatic reasons as the statistical program selected (Mplus) cannot accommodate a categorical indicator with more than 10 levels, and we did not want to lose data by collapsing categories. We acknowledge this as a limitation, and we recommend creating new measures for communal strength or using methodologically sound approaches to combine the categories.
Fourth, future research should assess shared identity longitudinally. It is possible that caregivers’ responses included a retrospective bias in this cross-sectional framework, as they were prompted to assess their relationship currently and prior to dementia onset. Because prior research suggests that relationship closeness is not always beneficial for caregiver well-being longitudinally, future research should assess shared identity over time to understand its relationship with, e.g., ambiguous loss. Furthermore, our cross-sectional approach does not clarify the direction of the relationship between shared identity and caregiving quality. It may be that caregiver burden predicts shared identity, e.g.. Through longitudinally studying shared identity, future researchers could assess whether relationship quality early in the illness predicts burden and exemplary care later, and they could track how caregivers’ relationship with their loved one potentially changes as the disease progresses. Experience sampling would also be beneficial to assess the caregiving experience over time within individuals. Caregiving research often relies on assessing caregiving outcomes aggregated across individuals (i.e., between-person data), which is very useful, but it ignores the potential within-person variations of the caregiving experience. It is possible that caregiver burden, and the quality of caregiving shifts based on variations in the course of the illness or in daily life circumstances. Through moment-by-moment sampling of caregivers’ shared identity, degree of burden, and quality of caregiving, over a short period of time, future scholars would more accurately capture caregivers’ experiences both at the within-person level and at the between-person level.
Fifth, although our analyses were based on a national sample of unpaid dementia caregivers, it was not a representative sample, raising concerns about the generalizability of our findings. The convenience, snowball, and web-based sampling methods likely attracted help-seeking caregivers and those who are connected to care resources, including online and in-person support groups, geriatric practitioners, research centers, etc. There may also be variation in results as a function of sampling approaches (convenience vs. random sampling) among informal caregivers. Our convenience sampling also limited our ability to stratify caregivers by the stage of their care recipient’s disease or specifically by the type of etiology of their dementia process. Furthermore, it is important for future researchers to examine how shared identity may vary by different caregiving relationships (e.g., romantic relationships, friends, children).
Sixth, we utilized self-report measures to test all constructs; hence, questions of respondent veracity can be raised. We managed this limitation through utilizing socially desirable responding as a control variable on the outcomes and the results suggested that social desirability minimally affected the relationships explored. Future studies, however, may also consider exploring behavioral indicators of shared identity through observational research.
Importantly, we recognize that caregiving is strongly informed by cultural and gender values, and it is critical to account for racial and ethnic differences, gender, and relationship differences in future studies. For instance, we found that African American/Black caregivers were less likely to experience caregiver burden than White caregivers. This finding is consistent with Pinquart & Sörensen's (2005) meta-analysis of 116 empirical studies that suggest that African American caregivers experience the least amount of burden in comparison to other racial/ethnic groups. Therefore, although the Shared Identity Theory did not initially account for cultural differences among caregivers, future researchers would benefit from assessing how Shared Identity Theory varies across different cultural groups. Therefore, it is important for future researchers to assess the validity of shared identity with more stratified samples.
Finally, we did not assess social support provided by people outside the caregiving/recipient dyad. It is possible that support from outside the dyad may be an important factor in the possibility of shared identity. Respite provided by others may allow the caregiver to provide exemplary care to the person with ADRD. This possibility merits further study. We also did not assess the ability status of caregivers, which may have influenced caregiver burden.
Conclusion
This study provides preliminary support for Shared Identity Theory (Lang & Fowers, 2019), which addresses the limitations of the caregiving literature by explicitly expanding the conceptualization of the Alzheimer’s caregiving relationship. We found that shared identity appears to be a rich, strong component of caregiving relationships, in that it is positively related to exemplary caregiving and negatively associated with experienced burden. This study suggests that it is sensible to continue to expand the scope of the caregiving literature to include a primary focus on the nature of the caregiving relationship, which has been underemphasized to date.
Supplemental Material
Supplemental Material - Exploring shared identity theory as an expanded conceptualization of Alzheimer’s caregiving
Supplemental Material for Exploring shared identity theory as an expanded conceptualization of Alzheimer’s caregiving by Samantha F. Lang, Blaine J. Fowers and Jue Wang in Journal of Social and Personal Relationships
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.