
Abstract
This study tested whether communication neglect (CN) mediated the relationship between caregivers’ reports of care receivers’ cognitive status and/or problem behavior and thoughts about potential harmful behaviors (PHB) toward their care receiver. It also examined if caregivers’ expressed anger and a positive pre-morbid relational history moderated the prediction of CN on PHB. Family caregivers (N = 339) in the U.S. completed the survey via Qualtrics. Results suggested that CN is a meaningful mediator explaining how PHB might occur. Caregiver expressed anger moderated the prediction of CN on PHB/physical abuse. Lastly, caregivers’ perceptions of a positive pre-morbid relational history were a potential protective factor against PHB. When caregiver expressed anger was moderate or high, the prediction of CN on PHB/physical abuse was positive, but its strength was reduced as pre-morbid relational history became stronger.
Keywords
Introduction
As the world population is aging, caregiving of older adults has increasingly become a common experience for many families. While many caregivers view caregiving as rewarding, caregiving is complex and emotionally taxing. Caregivers have to provide instrumental needs while navigating medical and financial systems and resources to ensure they utilize services and support to provide proper care. Caregiving demands, thus, may take a toll on caregivers’ well-being. Negative impacts on caregivers’ mental and physical health, financial stability, relational strains with the care receivers or their social networks have been noted (Ho et al., 2008; Lai, 2012; Quinn et al., 2009). Caregiver frustration and anger because of these stresses may affect how they interact with their care receivers (Crespo & Fernández-Lansac, 2014; MacNeil et al., 2010).
One possible consequence of caregivers’ negative emotions and stress is elder abuse and mistreatment. Different definitions of elder abuse have been recommended by the Centers for Disease Control and Prevention, the World Health Organization, and the National Research Council. The essence of these definitions suggests that within a trusted relationship, elder abuse and mistreatment are intentional/repeated acts or failure to act to meet caregiving needs which result in harm to an older person in care. Thus, elder abuse implies a relational breakdown in addition to harm to the older care receiver.
Much of the research attention has been given to identifying types of abuse (e.g., physical abuse, psychological abuse, financial exploitation, neglect, sexual abuse), impacts of elder abuse (e.g., physical injuries, emotional distress, cognitive decline, loss of family trust) (Mikton et al., 2021), and victim risk factors (e.g., cognitive deficit, poor physical health, limited social support, problem behaviors) or perpetrator risk factors (e.g., substance misuse, high levels of stress, depression) (Roberto, 2016). These findings have helped establish evidence-based programs and protocols for elder abuse awareness, prevention, screening, and detection. What is less understood, though, are the mechanisms (i.e., processes) whereby elder abuse may take place when risk factors are present, as well as protective factors that may buffer these effects. Thus, an understanding of how risk factors may work to exacerbate, and protective factors may work to reduce such harmful tendencies has theoretical and practical implications.
Scholarly effort has been devoted to addressing these issues. Caregiver burden (Lee, 2009) or caregiver verbal aggressiveness (Lin, 2018), for instance, may explain why elder abuse or potential harmful behavior may occur. Based on Sorenson’ (2006) conceptualization of communication neglect, Lin (2020) proposed another possible explanatory mechanism, communication neglect – caregivers intentionally avoid engaging in meaningful interactions with their care receivers. While definitions of elder abuse focus on whether tangible caregiving needs are met, or whether caregivers physically/verbally threaten/harm the safety/well-being of their care receiver, communication neglect focuses on the absence of communication/interaction for relational and identity purposes. Lin’s (2020) study found preliminary empirical support suggesting communication neglect a possible mechanism through which elder abuse occurred. Furthermore, an increase in caregiver expressed anger exacerbated the relationship between communication neglect and psychological abuse.
Given that Lin (2020) was the first and only study that considered communication neglect as a mediator, and caregiver expressed anger as a moderator in the relationship between communication neglect and elder abuse, these relationships were tested again in this study with a different sample to see if these earlier findings corroborate. The second goal was to focus on a factor that may intensify the relationship between communication neglect and potential harmful thoughts (i.e., caregiver expressed anger when performing caregiving duties) and a factor that may mitigate this tendency (i.e., a positive pre-morbid relational history).
Thoughts about potential harmful behavior
Instead of measuring actual occurrence of elder abuse (Lin, 2018, 2020), the current study measured elder abuse as caregivers’ thoughts about physically or psychologically harming their care receivers (PHB). This modification was made to address potential social desirability biases or threats of disclosure commonly noted in studies examining sensitive or controversial topics (Krumpal, 2013). Krumpal suggested that methods such as self-administration, or questions asked in a neutral way may reduce participants’ concerns about their identity being disclosed. Participants may be more inclined to report their negative thoughts honestly than to report their negative behaviors. Although questions may be raised as to whether PHB is a meaningful indicator of elder abuse, it has been frequently considered in caregiving research (e.g., Beach et al., 2005; Cheng et al., 2013; Lee, 2009). Beach et al. argued that even though PHB is not as serious as the actual occurrence of elder abuse in terms of immediate harm, it is an indicator that caregiving quality is compromised. It may serve as a precursor to an abuse in the future and, therefore, signal the need for early intervention (Beach et al., 2005). Furthermore, studies measuring PHB have examined the same caregiver- and care receiver-related risk factors used in studies that measured the actual occurrence of abuse, and they found similar results. For instance, Lee’s (2009) study showed that caregiver burden mediated the relationship between two predictors (i.e., reports of care receivers’ cognitive impairment, reports of care receivers’ problematic behaviors) and PHB. Thus, methodologically and conceptually, PHB is an appropriate indicator to be considered.
Caregivers’ reports of care receivers’ cognitive status and problem behaviors
Caregivers’ reports of older adults’ diminished cognitive status (caregivers’ reports of the severity of care receivers’ cognitive impairment) and problem behaviors (caregivers’ reports of having to manage care receivers’ behaviors that may deem disruptive, uncooperative, or inappropriate) have been associated with an increased risk in abuse (Dong et al., 2014; Lin, 2020). Caregivers’ reports of care receivers’ problem behaviors could increase caregivers’ stress (Gaugler et al., 2005; Savundranayagam et al., 2005) or caregiver anger-resentment (Coon et al., 2003; Garcia & Kosberg, 1992). In these cases, caregivers may resort to abusive or coercive behaviors out of frustration, emotional negativity, or extreme caregiver fatigue. In other words, negative emotions and negative cognitive appraisal are possible explanations as to why elder abuse occurs.
From a communication accommodation perspective (Giles et al., 1991), caregivers may interpret care receivers’ problem behavior or communication issues due to cognitive decline as non-accommodating. They may respond to non-accommodating behaviors negatively by avoiding communicating with their care receivers. Such response could increase the likelihood of elder abuse if continued. Thus, a non-accommodative response, such as communication neglect, could be mediating care receivers’ problem behaviors/cognitive issues and abuse.
Communication neglect, caregiver anger, and elder abuse
Sorenson (2006) suggested that communication neglect can be classified as a sub-type of emotional abuse. That is, caregivers may continue to provide necessary instrumental care for their older care receiver but avoid engaging in meaningful communication with him/her. Consequently, older care receivers could feel relationally or socially isolated, particularly if contact with their caregivers is an essential part of their connection to the world. Communication is an integral part of one’s well-being (Fowler et al., 2015). Negative social exchange between caregivers and their care receivers, such as rejection, are harmful for care receivers (Newsom et al., 2005). Intentional failure to provide emotional support or relational connection through communication could be considered emotional abuse. Like the notion of “silent treatment” which is regarded as a punitive (Williams et al., 1998) and a manipulative tactic to change a receiver’s behavior (Buss, 1992), caregivers may enact intentional communication neglect when they are irritated with, want to reprimand, or force a change in the care receiver’s behavior.
As the caregiving process can be physically and emotionally draining, negative emotions are frequently noted, such as those associated with depression (Beach et al., 2005). Anger-related emotions and expression of anger are perhaps the least understood affective reaction compared to other types of emotions (Crespo & Fernández-Lansac, 2014). Family caregivers may be hesitant to admit to experiencing anger with their care receiver due to a feeling of guilt or shame (See et al., 2022). In this case, experienced anger may manifest itself in subtle ways such as passivity suggested in silent treatment as discussed above (Vitaliano et al., 1993).
It should be noted that a broad conceptualization of anger includes anger feelings, experience of anger but not expressing it (anger-in) and expression of anger (anger-out) (Spielberger & Reheiser, 2010). Crespo and Fernandez-Lansac (2014) found 41% of participants showed a moderate-severe level of expressed anger. They argued that caregiver expressed anger has an impact on quality care and could lead to potential harmful behaviors when anger feelings are combined with anger expression. Coon et al. (2003) found that those who experienced a lower level of anger expression were able to do better in intervention classes focusing on skills to manage depression.
The current study took Buss and Perry (1992) approach to aggressiveness, specifically the sub-dimension of expressed anger (Anestis et al., 2009). Buss and Perry (1992) argued that anger “may function as a prelude to physical and verbal aggression” (p. 457). It is possible when caregivers engage in communication neglect as a response to care receivers’ display of problem behaviors or communication difficulties, they may also brood about negative emotions such as anger. When expressed, caregivers’ PHB tendency may increase. Thus, this study proposed that caregiver expressed anger might moderate the relationship between communication neglect and PHB.
Lin (2020) found that communication neglect mediated the relationship between care receivers’ problem behaviors and psychological abuse. Moreover, the relationship between communication neglect to psychological abuse was moderated by caregivers’ anger and hostility. That is, CN significantly predicted psychological abuse, and caregivers’ anger and hostility intensified the effect. Lin (2020) argued that communication neglect may not simply be a coping strategy for caregivers to de-escalate tensions and/or decompress frustrations with their care receiver as one might think. Instead, it could be a warning sign for concurrent or future verbal attack and emotional harms, especially when caregiver anger or hostility become prevalent. Thus, communication neglect and these caregiver traits combined can be a toxic environment for both caregivers and care receivers.
Taken together, with a different sample, change in how elder abuse and caregiver expressed anger were measured compared to those measured in Lin (2020), the following hypotheses were proposed to see if CN is a significant mediator and caregiver expressed anger a significant moderator (see Figure 1 for the hypothesized model): Hypothesized model – The moderated mediation models with caregiver expressed anger and pre-morbid relational history as Moderators. Note. PHB = Potential Harmful Behavior. The predictor box includes two variables: Reports of OA’s problem behavior and OA’s cognitive status. They were tested separately. The dependent variable box includes two variables, PHB-Psychological abuse, and PHB-Physical abuse. They were tested separately.
Communication neglect will mediate the relationship between caregivers’ reports of their care receivers’ cognitive status and their potential harmful behaviors.
Communication neglect will mediate the relationship between caregivers’ reports of their care receivers’ problem behaviors and their potential harmful behaviors.
Caregiver expressed anger will moderate the relationship between caregivers’ communication neglect and their potential harmful behaviors.
Positive pre-morbid relational history: A protective factor against elder abuse
While much of the research has identified community-based resources, such as social support or social connections, as important protective factors against elder abuse (e.g., Dong & Simon, 2008; Quinn et al., 2009; Storey, 2020), there is relatively scant evidence demonstrating that a positive pre-morbid relational history between caregiver and care receiver helps reduce its occurrence. Limited evidence suggests it can. For instance, a positive pre-morbid relational history was found to be a protective factor against physical and psychological abuse and neglect in a Hong Kong study (Fang et al., 2019). Conversely, a negative previous relationship was a risk factor for abuse (Orfila et al., 2018). While not directly examining the context of elder abuse, Steadman et al. (2007) found that caregivers who had satisfactory pre-morbid relationships with their care receiver demonstrated better problem-solving skills and communication skills when dealing with a care receiver’s problem behaviors or memory issues. Other relevant evidence shows that current relationship quality between caregiver and care receiver affects family members’ willingness to take on the caregiver role (Brody, 1990), and their level of depression and tendency to engage in harmful behaviors (Williamson & Shaffer, 2001).
If the occurrence of elder abuse indicates relational breakdown, a positive pre-morbid relational history may serve as a resource for caregivers. It seems logical that caregivers may be less likely to engage in abusive behaviors when they have a warm regard for the person they care for. The previous ongoing relationship provides relational capital from which caregivers can draw to help appraise their stresses and choose coping strategies that will continue the positive relationships (Fang et al., 2019). Tensions and negative emotions due to caregiving, such as caregiver anger, may be interpreted differently by caregivers who report a positive pre-morbid relational history than by those who report a poor one with their care receivers.
Taken together, it is possible that a positive pre-morbid relational history may “tame” caregiver anger by facilitating reappraisal of the troublesome caregiving situations (i.e., problem behaviors and cognitive decline). Even though communication neglect in and of itself creates social isolation for care receivers, which may already have detrimental effects on their well-being, protective factors such as satisfying pre-morbid relational history may “contain” the damages from further devastating consequences such as abuse or thoughts about harmful behaviors.
Accordingly, a hypothesis was proposed (see Figure 1 for the hypothesized model):
Caregivers’ reports of pre-morbid relational history with their family care receiver will moderate the impacts of caregiver expressed anger on the relationships between communication neglect and potential harmful behaviors.
Method
Participants
Family caregivers (N = 339) completed an online questionnaire via Qualtrics (Mage = 44.93, SD = 15.07; cisgender Male = 105 (31%), cisgender Female = 234 (69%)). Most participants self-identified as White (74%), followed by African American (14.2%), Hispanic (7.7%), American Indian/Alaska Native (1.2%), and Asian (1.2%). Approximately 10.3% of the participants resided on the East coast, 12.4% on the West coast, 23% in the Midwest, and 54.2% living in other parts of the U.S. For educational attainment, approximately 44.8% of the participants completed college or more advanced degrees, 22.4% completed some years in college, 32.7% completed high school, and 2.9% completed some years in high school.
On average, participants had been caregivers for 3.85 years (SD = 4.59) and spent approximately 34.68 hours per week (SD = 30.76) caring for their older family member (Mage = 77.86, SD = 8.45). More than half (50.1%) of the care receivers were participants’ parents, 29.5% were grandparents, 11.8% were spouses, and 8.6% were other family members. Participants either lived with their family care receiver (45.4%) or visited the older care receiver for certain hours per day (37.2%) or per week (13%).
Procedure
Means, standard deviations, reliabilities, scale ranges of and correlations among all variables.
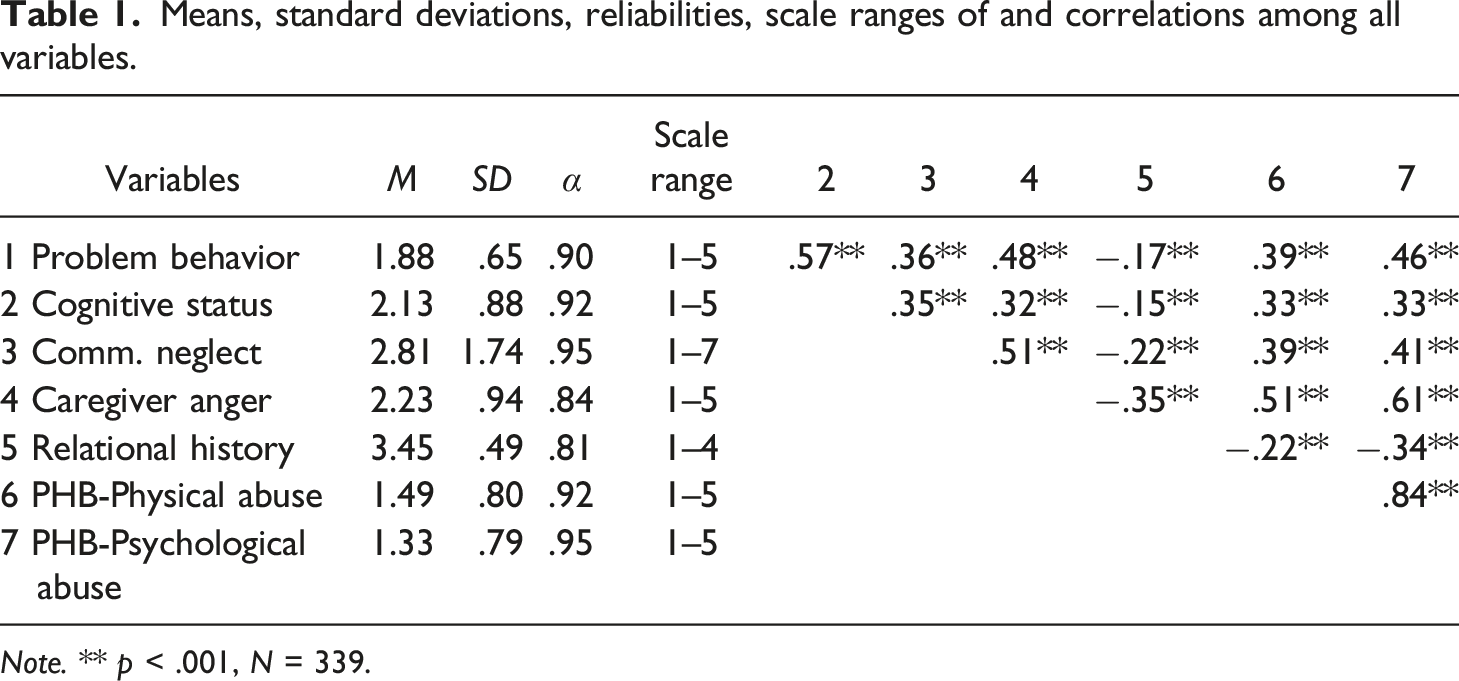
Note. ** p < .001, N = 339.
Measurements
Older adults’ problem behaviors
A problematic behavior scale (Pearlin et al., 1990) was used to measure each participant’s assessment of his/her older care receiver’s behaviors. Participants indicated how many days in the past week they had to personally deal with certain care receivers’ behaviors (14 items, 1 = no days, 4 = 5 or more days; e.g., “repeat questions/stories,” “cling to you or follow you around,” “become irritable or angry”).
Older adults’ cognitive status
A cognitive status scale (Pearlin et al., 1990) was used to measure participants’ perception of their older care receiver’s cognitive status (8 items; 1 = Not at all difficult; 5 = Can’t do it at all). Sample questions are “remember recent events,” “understand simple instruction,” and “recognize people that he/she knows.”
Communication neglect
A communication neglect scale (Lin, 2018, 2020) was used to measure participants’ tendency to engage in behaviors such as to “avoid engaging in the conversation with the older care receiver” or “not pay attention to what he/she did when I was in the room” (10 items; 1 = Not at all, 7 = Always). This scale was developed based on the Couple’s Interaction Rating System (CIRS; Heavey et al., 1996), specifically its two subdimensions, withdrawal and avoidance, which reflected Sorenson’s (2006) conceptualization of intentional communication neglect of older adults in the caregiving context.
Caregiver expressed anger
One dimension of Buss and Perry’s (1992) aggressiveness scale was adapted to measure participants’ aggression manifested in anger in the context of caregiving. Specifically, the instruction was modified to ask participants to indicate the degree to which they experienced anger when taking care of this aging family member (7 items; 1 = Strongly disagree; 5 = Strongly agree). Some sample questions are “When frustrated, I let my irritation show,” “I have trouble controlling my temper.”
Pre-morbid relational history
Two scales were used to assess participants’ perceptions of their relationship with this family care receiver prior to the onset of the caregiving needs. The first measure was the Williamson and Shaffer (2001) mutual communal behaviors scale (MCBS). It assessed how often participants engaged in behaviors that expressed communal feelings between them and their care receiver (5 items; 1 = Never; 4 = Always). Sample items are “I enjoyed helping him/her,” “When he/she had a need, he/she turned to me for help.” The second scale was adapted from the Williamson and Shaffer (2001) relationship rewards scale. It included four items that assessed how often participants found their pre-morbid relational history with this family care receiver rewarding (1 = Never; 4 = Always). Sample items are “I felt very emotionally close to him/her,” “He/she made me feel good about myself.” These 9 items were used together to measure caregivers’ perceptions of relational history with the care receiver. The higher the score, the more positive participants felt their pre-morbid relational history was.
Potential harmful behaviors
The Williamson and Shaffer (2001) 10-item potential harmful behavior scale was used to measure how often participants think of engaging in psychological and physical abuse when interacting with the older care receiver (1 = Never, 5 = Almost always). Five items gauged impulses of psychological abuse (e.g., “I want to scream and yell at him/her,” “I want to threaten to abandon him/her”) and five items gauged impulses of physical abuse (e.g., “I want to hit or slap him/her,” “I want to withhold food from him/her”).
Results
H1a and H1b asked if communication neglect mediated the prediction of caregivers’ report of their care receivers’ (1) cognitive status or (2) problem behavior on PHB. Hayes’ (2013) macro PROCESS Model (model (4) was used to test H1a and H1b. Macros PROCESS is a regression-based approach, similar to OLS regression to estimate direct effects of X on Y and indirect effects of X on Y through mediator(s). In each model estimation, the variable, either caregiver reports of their older care receiver’s problem behaviors or care receiver’s cognitive status was entered as the independent variable (X). Given that reports of cognitive status and problem behaviors could be related, one was entered as a covariate when the other was entered as the independent variable. Two other covariates (i.e., caregiver’s sex, and hours per week caregivers spent on caregiving responsibilities) were entered as they have been noted to influence the occurrence of elder abuse (National Research Council, 2003). All covariates were included in all the analyses. Communication neglect was entered as the mediator (M). Potential harmful thoughts, “thoughts about physically harming the older care receiver” and “thoughts about emotionally harming the older care receiver” were entered separately as the dependent variable (Y). There was no missing data for any of the variables except for one covariate, number of hours spent on caregiving. For that variable the mean was entered for missing cases (n = 29).
Four mediation tests were performed and significant indirect effects were found for all of them (see Figure 2). Communication neglect mediated the relationship between reports of problem behavior and both types of potential harmful behaviors (PHB-Phy: Indirect = .08, SE = .03, 95% CI [.033, .139]; PHB-Psy: Indirect = .08, SE = .03, 95% CI [.035, .142]). It also mediated the relationship between reports of cognitive status and both types of potential harmful behaviors (PHB-Phy: Indirect = .05, SE = .02, 95% CI [.017, .078]; PHB-Psy: Indirect = .05, SE = .02, 95% CI [.019, .080]). Thus, H1a and H1b were supported. Significant results of the mediation models – Reports of older care receivers’ problem behaviors or cognitive status on PHB/Psychological and physical abuse through communication Neglect. Note. *p < .05; **p < .01; ***p < .001. N = 339. Regression weights are unstandardized values. The dotted line indicates non-significant effect after communication neglect was included.
H2 asked if caregiver expressed anger moderated the relationships between communication neglect and two forms of PHB. Hayes’ (2013) macro PROCESS (Model 14) was used, with bootstrap analyses with 5,000 iterations. The same variables described above were entered. In addition, caregiver expressed anger was entered as the moderator (W), which was estimated at three levels (-1SD, Mean, and +1SD). The indirect path was interpreted as significant when the 95% bias-corrected confidence interval for the indirect effect did not contain zero (Hayes, 2013).
Treating caregiver expressed anger as the moderator, four moderated mediation tests were performed and only two of them were significant and reported here (see Figure 3). First, the overall model was significant when reports of problem behavior was the independent variable and physical abuse was the dependent variable, F (7, 331) = 29.08, p < .001, R
2
= .38. The test of the moderated mediation was significant (index = .07; SE = .03, 95%CI [.017; .139]). That is, the relationship between communication neglect and caregivers’ thoughts about physical abuse was significantly intensified by caregiver expressed anger at Mean and +1SD levels, when they perceived their older care receiver displaying problem behaviors. The second significant result was when reports of older adult’s cognitive status was the predictor and thoughts about physical abuse was the dependent variable F (7, 331) = 29.08, p < .001, R
2
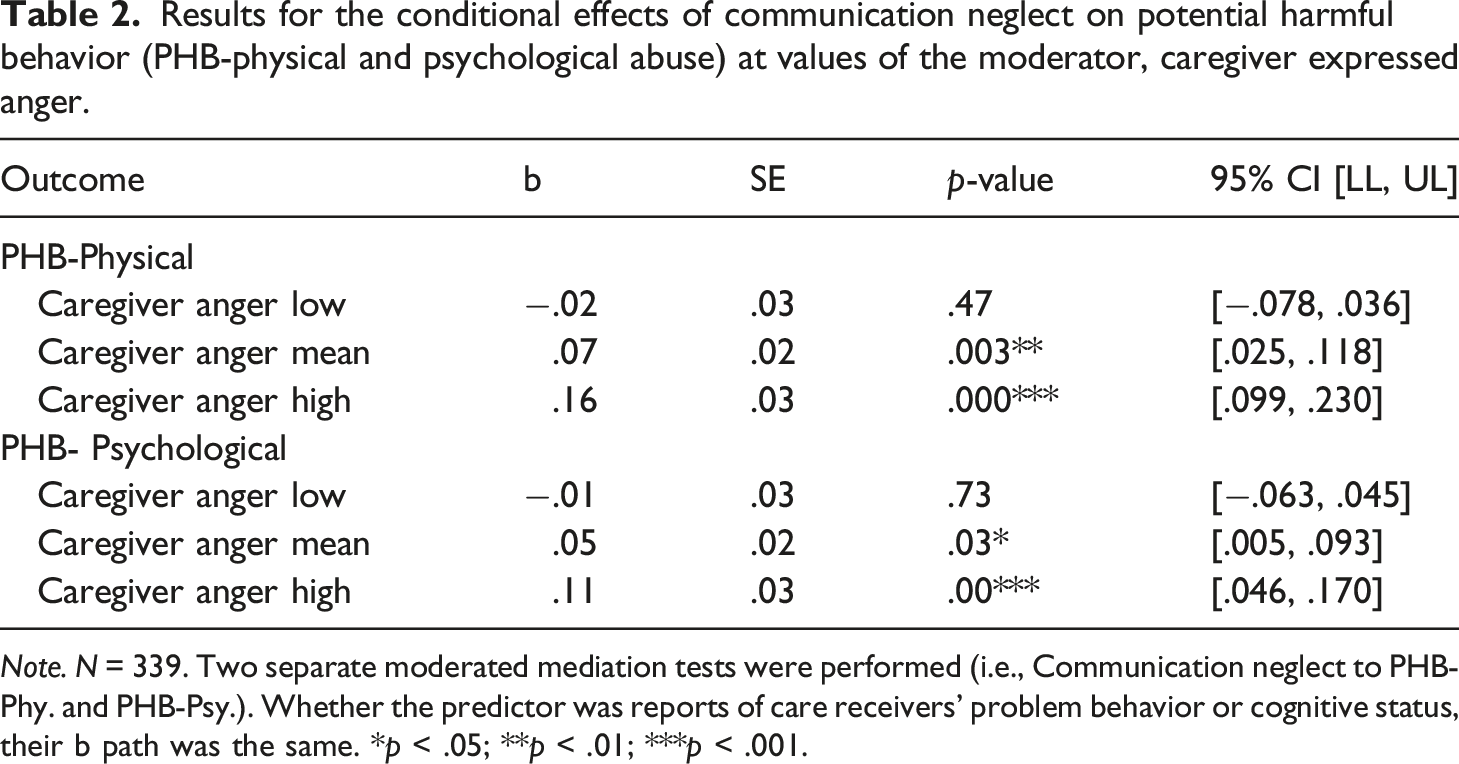
= .38. The test of moderated mediation was significant (index = .04; SE = .20, 95% CI [.010; .086]). The relationship between communication neglect and caregivers’ thoughts about physical abuse was significantly intensified by caregiver expressed anger at Mean and +1SD levels, for those who reported their older care receiver displaying cognitive issues (see Table 2). Significant results of the mediated moderation models – Reports of older care receivers’ problem behaviors or cognitive STATUS on PHB-Physical abuse through communication neglect and caregiver expressed anger as moderator. Note. *p < .05; **p < .01; ***p < .001. N = 339. The indirect effect is contingent upon caregiver expressed anger. Unstandardized regression coefficients are reported. The dotted line indicates non-significant effect after communication neglect was included. Results for the conditional effects of communication neglect on potential harmful behavior (PHB-physical and psychological abuse) at values of the moderator, caregiver expressed anger. Note. N = 339. Two separate moderated mediation tests were performed (i.e., Communication neglect to PHB-Phy. and PHB-Psy.). Whether the predictor was reports of care receivers’ problem behavior or cognitive status, their b path was the same. *p < .05; **p < .01; ***p < .001.
When the variable of psychological abuse was the dependent variable, moderated mediation tests were non-significant (Reports of problem behavior: Index = .05; [95% CI = −.003, .105]; Reports of cognitive status: Index = .03; [95% CI = −.001, .064]). Even though conditional effects of expressed anger of CN on PHB-Psy were significant at Mean and +1SD levels (see Table 2), the overall tests were not.
In short, caregiver expressed anger significantly moderated the relationship between communication neglect and PHB-Phy. An increase in caregiver expressed anger increased the prediction of communication neglect on thoughts about physical abuse. H2 was partially supported.
Summary of conditional indirect effects with pre-morbid relationship As moderator at different levels of caregiver expressed anger.

Note. b Path (mediator = communication neglect; outcome = PHB/Physical Abuse). *p < .05; **p < .01; ***p < .001.
The results also suggested how pre-morbid relational history moderated caregiver expressed anger (see Table 3). When caregiver expressed anger was low, different degrees of pre-morbid relational history did not moderate the relationship between communication neglect and thoughts about physical abuse. When caregiver expressed anger was average and high, relational history moderated the relationships between communication neglect and PHB-Phy. Relationship between CN and PHB-Phy was still positive, but such effect (b value) decreased as pre-morbid relational history became stronger. In other words, perceptions of a positive relational history smoothed out the intensity of caregiver expressed anger on the relationship between communication neglect and PHB-Phy. H3 was partially supported.
Discussion
To recap, the findings suggest that when caregivers reported their care receiver displaying problematic behaviors or having cognitive-related issues, they were more likely to communicatively neglect their care receiver, which in turn predicted impulses to engage in physical abuse or psychological abuse. Furthermore, when caregiver expressed anger increased, the influence of communication neglect on impulses of physical abuse was exacerbated.
H3 results showed that caregivers’ reports of a positive pre-morbid relational history played a role in moderating the impacts of different levels of caregiver expressed anger. When caregiver expressed anger was low, relational history did not significantly moderate the relationship between communication neglect and PHB/physical abuse. That said, the direction of the effects suggested that prediction of CN on PHB-Phy was negative as relational history became stronger. When caregiver anger was moderate and high, the results painted a slightly different picture. That is, even though communication neglect positively predicted PHB/physical abuse, as pre-morbid relational history increased in strength, the impact of communication neglect on PHB/physical abuse was significantly reduced (see Table 3). A positive pre-morbid relationship may not reverse the positive prediction of communication neglect on PHB/physical abuse when caregiver expressed anger increases, but it may lessen its effect.
What increases the likelihood of potential harmful behaviors?
The current study provided additional empirical evidence corroborating previous findings (Lin, 2020) that communication neglect was one of the mechanisms whereby abuse may occur. Caregivers may choose to avoid interacting with their care receivers when they find caregiving to be challenging, such as care receivers displaying problem behavior or cognitive decline. Such a response may not simply be a passive coping strategy but instead, a warning sign of a concurrent or future occurrence of abuse. The finding of the current study and Lin (2020), thus, suggest that CN can be a precursor to expressed abuse.
In addition to predicting thoughts about abuse, CN itself has social implications but also health and relational implications. Care receivers who are socially isolated from regular human interactions are found to have depression, increased mortality (Cacioppo & Cacioppo, 2014) and risk for being subjected to abuse (National Research Council, 2003). Caregiving is enacted and accomplished through communication. When caregivers display communication neglect, it implies that they are not actively acquiring information from their care receivers about their well-being, coordinating and negotiating caregiving needs with their care receivers, or making effort to maintain care receivers’ dignity and identity. A lack of these activities may negatively impact care receivers’ health and emotional stability. Furthermore, persistent avoidance and withdrawal from interacting with relational partners are common strategies individuals use when they desire relationship dissolution (Baxter, 1998), particularly in the early stages of relational breakdown. In the caregiving context, when caregivers cannot terminate the relationship with their care receivers, they may not only continue neglectful communication but also harbor resentment and stress (such as the notion of anger-in discussed above; Vitaliano et al., 1993). This may be why, when caregiver anger was entered as the moderator (H2), communication neglect still significantly predicted impulses of abuse, but its effect was considerably reduced compared to when caregiver expressed anger was not included in the model.
In short, communication neglect is a meaningful communication variable central to the occurrence of abuse and mistreatment. Research on elder abuse has identified a host of risk factors or profiles that likely lead to abuse, but fewer studies offered “process-oriented” mechanisms to put these profiles “in action.” Thus, dysfunctional communication such as caregiver communication neglect or perceived care receiver’s under-accommodative behaviors (Lin, 2018) should be included in elder abuse detection and caregiver training to raise awareness.
Another factor that might increase the likelihood of potential harmful behaviors is caregiver expressed anger. It intensified the relationship between communication neglect and PHB-physical abuse whereas in Lin (2020), it intensified the relationship between communication neglect and actual occurrence of psychological abuse in the past. This different result (i.e., types of abuse) may be due to a few reasons. First, caregiver expressed anger was conceptualized differently in these two studies. In Lin (2020), it was conceptualized as a trait whereas in the current study, it is conceptualized as a state. Previous studies have found that both state and trait are related to caregiver aggression (e.g., Gates et al., 2003). Thus, it is possible that while both anger trait and state are risk factors for aggression, different samples may manifest their anger differently. Elder abuse research indicates that when one type of abuse occurs, it usually suggests other types of abuse occur simultaneously (Roberto, 2016). Thus, it is possible that caregiver expressed anger, state or trait, may intensify both types of abuse, and depending on specific caregiving characteristics in each sample, either physical or psychological abuse takes precedence. For example, increased caregiver depression and reports of their care receivers’ under-accommodative behaviors moderated caregivers’ psychological abuse but not physical abuse (Lin, 2018).
Secondly, participants in the current study were asked to report their “thoughts” about harmful behaviors, not their actual behaviors as measured in Lin (2020). They might be more truthful about their thoughts than about their actions, especially those that are considered more violent ones such as physical harm. Thus, measurement differences may contribute to the different findings. Thirdly, it could be due to the increased demands of caregiving in the current sample. A 2020 National Alliance for Caregiving report showed an increase in the types of caregiving needs compared to its 2015 investigation. This report suggests that not only has the proportion of family members providing care to older family members increased since 2015 when the study was conducted last time, an increase in the types of needs has also been observed. More caregivers in the 2020 survey reported their care receivers having long-term physical conditions, emotional or mental health issues, and memory problems, such as Alzheimer’s or other forms of dementia. Compared to Lin’s study (2020) where the data were collected in 2015, the data of this study were collected in 2021. It is possible that the trend indicated in the National Alliance for Caregiving report (2020) is reflected in this group of participants. Furthermore, a contextual factor that might explain the increase in caregiving needs in 2021 was the pandemic (Cohen et al., 2021). With both the general trend and the impact of the pandemic, caregivers may be overwhelmed by the amount of time required and therefore, experience negative emotions and abusive impulses, especially pertaining to physical harm. Future research may benefit from considering additional caregiving characteristics to understand the joint influence of communication neglect and caregiver expressed anger. As anger may ultimately be expressed behaviorally or communicatively, management of negative emotions is needed for caregiver training (Coon et al., 2003).
Taken together, communication neglect and caregiver expressed anger are a toxic combination of behavioral and emotional expression of caregiving. It is associated with actual occurrence of psychological abuse (Lin, 2020) and PHB-Phy, as found in the current. Even though PHB may not pose immediate danger to care receivers’ well-being and safety; it signals caregivers struggling with caregiving demands, and possible future occurrence of abuse.
What protects against the likelihood of potential harmful behavior?
A positive pre-morbid relational history was found to be a protective factor against elder abuse, which corroborates previous research (e.g., Steadman et al., 2007; Williamson & Staffer, 2001). Caregivers’ perceptions of the past relationship itself did not significantly predict reduced physical abuse as found in previous studies. Instead, its influence is manifested at different levels of caregiver expressed anger. These findings help us understand how a satisfying pre-caregiving relationship might function to “protect” care receivers from harm.
Social exchange theory or equity theory suggests that relationships between caregiver and care receiver may be out of balance as caregiving needs increase, which may increase caregiver burden or distress. For instance, Ybema et al. (2002) found that perceptions of inequity were associated with caregiver emotional exhaustion and depersonalization. However, in long-term relationships such as family relationships, a dyad may have relational capital accumulated over the years if family members spent time cultivating the relationships. Thus, a positive relational history functions as a resource in maintaining relational equity in caregiving contexts (Braun et al., 2009). This relational foundation may motivate caregivers to react more positively when they experience caregiver anger when encountering problematic interactions with their care receiver. In the current study, when caregiver expressed anger was low, CN did not significantly moderate the relationship between communication neglect and PHB-Phy (approaching significance, p = .055). Even so, as relational history became stronger, a higher score on CN predicted a lower score on PHB-Phy. This direction was still encouraging. It is possible that when caregiver expressed anger is low, caregivers may still be able to constrain their impulses of physical abuse by being reminded of the rewarding and mutually beneficial relationships they had with their care receivers in the past. Their frustration and emotional exhaustion may thus be interpreted more positively, at least being directed away from the care receiver, and they may be motivated to seek alternative responses. Crespo and Fernández-Lansac (2014) suggested that since family caregivers may consider expression of anger to be a less acceptable negative emotion when caring for a family member, they may be more inclined to develop strategies to control it. A positive pre-morbid relational history may help suppress such emotions, especially when anger expression level is low. Given that this result is not significant, future research should continue exploring the moderating effect of relational history when caregiving expressed anger is low.
When caregiver expressed anger increased (i.e., moderate and high), stronger pre-caregiving relationship appeared to reduce the strength of potential harmful behaviors as it reduced more than half of the b values (see Table 3). When a caregiver’s expressed anger escalates, it may take a greater effort to manage his/her irritability. Caregivers may be more likely to perceive their care receivers’ behaviors as uncooperative or under-accommodative (Lin, 2018), and less likely to appraise the situation in positive lights (López et al., 2013). Consequently, they are less likely to choose constructive coping strategies to respond. Relational imbalance may overpower the influence of a positive relational history. Thus, while a positive relational history is helpful in reducing the strength of such association, it cannot eliminate thoughts about physical abuse. However, by reducing the strength, caregivers’ tendency to engage in actual abusive behaviors might be significantly weakened.
While these findings suggest the importance of cultivating a positive family relationship early on, it is important to recognize that unfortunately, family members may elect to abuse, whether it is through physical or psychological abuse, to exert power or control (Brandl, 2000; Tueth, 2000). A positive pre-morbid relationship may not be attainable in dysfunctional families. An understanding of family cycle of violence through the lens of power and control is critical to PHB/abuse prevention and early intervention of family dynamics.
In short, pre-morbid relational history should be taken into consideration, in addition to gender, family members’ availabilities, financial stability, or geographical distance, when needs for caregiving emerge. The ways in which family members communicate with each other and how their relationships evolve over time feed into their current caregiving relationships. Pre-morbid relational history may influence caregivers’ willingness to seek support, interpret caregiving tasks positively, and work patiently with their care receivers when burdens and depressed affects are felt. In this sense, prevention of elder abuse and mistreatment should begin by identifying a dysfunctional cycle of family violence and creating a healthy and satisfying communication climate early in one’s family life.
Limitations and future research
First, this is a self-reported and online survey. It was difficult to verify authenticity in terms of participants being caregivers. That said, participants were asked specific questions to gauge their caregiving experiences to ensure participants’ identity as caregivers (see the Method section). Secondly, participants who had no, or limited internet access were not included in the study. Those who have internet access may also have more access to resources available for caregivers. They may feel less isolated or less stressed when encountering problematic interactions with their care receivers compared to those who have no or limited internet access. Future research should recruit participants via both online and offline venues to better capture caregiving experiences. Thirdly, based on participants’ responses to the open-ended questions (not included in the analysis in this study) regarding their caregiving tasks and their reports of their care receiver, their care receivers seemed to be cognitively alert (cognitive status mean = 2.13) and behaviorally easy to work with (problem behavior mean = 1.88). These care receiver characteristics may partially explain the potential floor effect observed in this study. That said, several significant results were found, which suggests the value of the proposed models. While illness such as dementia has been identified as a risk factor for the occurrence of abuse (e.g., Roberto, 2016), we should not assume that care receivers who do not have such medical conditions are exempt or are less likely to suffer from mistreatment, as there are many other at-risk factors in elder abuse (e.g., National Research Council, 2003). Next, it should be noted that this study did not obtain information about caregivers’ disability status (with a physical disability or with a mental illness). As caregiving is emotionally and physically-taxing for many, future research should examine the ways in which caregivers’ disability status influence the variables examined in this study. In addition, this study examined one dyadic factor (i.e., a positive pre-morbid relational history) that may protect against elder abuse. Future research should examine if other individual- or dyadic-level factors such as caregiver self-efficacy or caregiver/care receivers’ positive communication accommodation buffer the impact of communication neglect on elder abuse. Lastly, Sorenson (2006) suggested that CN could be a sub-type of psychological abuse, but he did not empirically test this assertion. In light of the results of this study, this assertion should be examined to see if CN functions as an independent influence on physical and psychological abuse as suggested by the current study or as a sub-type of psychological abuse.
Conclusion
Communication with care receivers could become laborious as their cognitive functions decline or problematic behaviors become frequent. Neglectful communication could be a proper and temporary coping strategy if care receivers’ instrumental needs are met. That said, communication neglect, when persisted over time, may affect caregiving quality; it may also be a manifestation of a “silent cry” from both sides: a relational breakdown is occurring, and help is needed to release tensions between them. One possible way to intervene or break the likely vicious cycle is to increase relational capital within the family prior to the needs for caregiving. Instead of treating family caregiving and elder abuse as an aging-related issue pertaining only to old age and after caregiving needs begin, it should be understood from a lifespan perspective as relational dynamics within the family throughout its history have long-term implications.
Footnotes
Author’s note
Mei-Chen Lin (Ph.D., University of Kansas) is Professor in the School of Communication Studies at Kent State University. Her research interests include intergroup communication and identity management, communication and aging, elder abuse, and political identity and media use.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the author has provided the following information: This research was not pre-registered. The data used in the research are available. The data can be obtained by emailing: