
Abstract
Spousal support may help ameliorate the health consequences of stressful situations by downregulating cortisol. To examine how cortisol levels change in conjunction with spousal social support during discussions of a stressful situation, 191 married couples engaged in two 10-minute interactions addressing a personal (i.e., non-marital) problem. We coded for positive and negative social support provision and receipt, assessed the perception of received support, and collected salivary cortisol samples. We found that wives’ display of more negative behaviors while receiving support was associated with an increase in wives’ cortisol levels via an indirect (mediated) effect of perceived partner responsiveness. Overall, results suggest a link between support behaviors, changes in cortisol and perceived partner responsiveness, with more consistent links between support behaviors and responsiveness ratings relative to other paths, and cortisol effects found more often in wives than husbands. Exploratory analyses also suggest that cortisol levels coming into an interaction may impact elements of support interactions. The implications of the role of cortisol and partner responsiveness to the provision of spousal support are discussed.
Keywords
Introduction
Being married correlates with better overall health (Kiecolt-Glaser & Wilson, 2017). Potentially accounting for this effect is that romantic partners are a powerful source of social support (Holt-Lunstad et al., 2008), buffering against the impact of chronic life stress on health (Broadhead et al., 1983; Cobb, 1976). Currently, however, the precise mechanisms explaining this phenomenon are not well understood (Thoits, 2011).
One explanation is that stress triggers a complex set of processes including the release of the hormone cortisol, which mobilizes resources (e.g., increasing blood sugar) in response to external demands (Fries et al., 2009). Chronic stress yields prolonged elevations of cortisol that can lead to dysfunction of the hypothalamic-pituitary-adrenal (HPA) axis (Kemeny, 2003), damaging body processes such as immune function and increasing health risks (McEwen & Wingfield, 2003). Indeed, HPA axis dysfunction is associated with depression (Kunugi et al., 2006), obesity (Steptoe et al., 2004), and cardiovascular disease (Girod & Brotman, 2004). Social support may influence health by modifying these negative impacts of chronic stress, and this stress buffering hypothesis (Cohen & Wills, 1985) is supported by both clinical and animal research suggesting that social processes modify the HPA axis (Hostinar et al., 2014; Rosal et al., 2004).
Researchers in this area often characterize social support broadly and without reference to more specific actions between partners, so little is known about how particular support behaviors covary with cortisol levels. This is a notable omission as behavioral interaction is a component of most supportive exchanges (cf., invisible support; Bolger et al., 2000), and at least some of the palliative effects of social support occur during an interaction. For instance, the mere presence of a supportive partner while anticipating a stressful task is associated with attenuated increases in cortisol, whereas a lack of support is associated with greater increases in cortisol (Ditzen et al., 2008b; Heinrichs et al., 2003; Kirschbaum et al., 1995). Additionally, expression of physical intimacy during a lab stress task was associated with faster cortisol recovery in men (Ditzen et al., 2019). These findings dovetail with studies demonstrating that negative couple interactions are associated with increased cortisol activity (Heffner et al., 2006; Kiecolt-Glaser et al., 1996), whereas positive conflict communication behaviors (Seiter et al., 2019), affectionate interactions (Ditzen, Hoppmann, & Klumb, 2008a) and physical contact (Ditzen et al., 2007; Grewen et al., 2005) elicit decreases in cortisol and healthier daily cortisol patterns (cf., Fehm-Wolfsdorf et al., 1999). Partner support and cortisol are also associated outside of the context of a supportive interaction. For example, couples who reported greater satisfaction with support showed lower levels of cortisol reactivity during marital conflict (Heffner et al., 2004).
Despite these findings, the ameliorative effects of enacted social support cannot be assumed. In fact, receiving social support can increase psychological distress (e.g., Bolger et al., 2000) by drawing excessive attention to stressors and interfering with the recipient’s sense of self-efficacy (Howland & Simpson, 2010). Positive support behaviors have also demonstrated paradoxical effects on outcomes such as marital satisfaction (e.g., Lawrence et al., 2008). Correspondingly, some hypothesize that social support may have positive effects only when enacted skillfully (Rafaeli & Gleason, 2009) and in ways that are responsive to the stressed person’s needs (Gable et al., 2012). Some recent mechanisms found for effective social support include viewing stress as enhancing rather than debilitating (Nguyen et al., 2020), the mood of the support provider (Goldring & Bolger, 2022), and facilitation by support seekers (Forest et al., 2021). This literature suggests that support may not be perceived as supportive, even if the behaviors involved are deemed as “positive” by third-party observers. This includes situations where well-intended or even expert-recommended forms of support might not be perceived as effective support. Therefore, it is important to evaluate an individual’s perception of the support received, which may be a better barometer for its effectiveness than the behavior itself. Thus, the concept of perceived partner responsiveness (PPR) – feeling understood, valued and cared for – has been of increasing interest. PPR is rooted in theories of intimacy (Reis et al., 2004) and is connected to how partners understand and care for the core self, and is one of many ways partners might evaluate partner support. Ratings of PPR are influenced by a partners’ self-reported actions, as well as internal perceptions of one’s own responsiveness that get projected onto the partner, which both positively predict relationship outcomes (Lemay & Clark, 2015; Lemay et al., 2007).
Several studies associate PPR with lowered stress responses. For instance, indicators of a partner’s attentiveness during a stressful task led to higher ratings of PPR and caused participants to feel less stressed and show fewer signs of behavioral vigilance (Kane et al., 2012). Likewise, in response to marital conflict, spouses who were satisfied with support from partners had lower cortisol and less negative affect than those less satisfied (Heffner et al., 2004). A 10-year longitudinal study further showed that individuals with higher ratings of PPR had healthier basal cortisol (Slatcher et al., 2015), linking perceived support and HPA axis functioning via cortisol. However, these studies do not separately measure support objectively received from subjectively perceived, and do not measure PPR and cortisol reactivity in response to a specific interaction. Distinct measures would help establish whether certain behaviors associate with cortisol functioning by themselves or via PPR, or if perceived support quality retains positive effects when controlling for behavioral observations of the supportive exchange.
We aimed to address whether certain objectively rated better (i.e., positive) or worse (i.e., negative) social support behaviors - as defined by previous relationship researchers (Pasch et al., 2004; Sullivan et al., 2010) - associate with higher and lower cortisol levels, respectively, and potentially impact cortisol change across a support interaction. The presence of a verbally supportive partner may attenuate cortisol (Ditzen et al., 2008b; Heinrichs et al., 2003), but it is unclear what aspects of support solicitation and provision are influential. Demonstrating that skilled support lowers cortisol would identify an important mechanism implied by the stress-buffering hypothesis. We also evaluated the role of PPR in the association between observed support and cortisol. Behaviors and perceptions are not always correlated, and the latter may be more influential to ultimate health outcomes (Haber et al., 2007). We also assessed expectations of PPR prior to the support discussion and collected ratings after the interaction, allowing us to control for a more general sense of PPR from prior relationship experiences and focus on the effects of PPR for a specific supportive interaction. We know of no studies investigating the effects of support behavior and PPR on cortisol reactivity, or whether frequencies of support behaviors impact cortisol either directly or by enhancing PPR. Clarifying how these elements of supportive interactions are linked would represent an important step in identifying potentially modifiable processes that might enhance the quality of support and its effect on biological stress response systems.
To address these gaps, we observed married couples engaging in two discussions designed to elicit support. We measured salivary cortisol levels and expected/perceived support quality before and after the discussions. Social support receipt and provision behaviors were measured with observational coding of the discussions. We hypothesized that more frequent negative support receipt and provision behaviors would be associated with higher levels of cortisol for both spouses in each of the two interactions (hypothesis 1a). We hypothesized that positive social support provision and receipt behaviors would be associated with lower levels of cortisol for both spouses in each of the two interactions (hypothesis 1b). We also hypothesized that more frequent positive and negative support provision and receipt behaviors would be associated with higher and lower post-interaction appraisals of PPR, respectively (hypothesis 2). We hypothesized that more favorable appraisals of PPR would negatively correlate with cortisol levels (hypothesis 3). No hypotheses were made regarding expectations of PPR, which was only used as a control variable in the analyses to account for more general expectations from previous interactions. Finally, we developed a path model to evaluate the hypothesis that changes in perceived partner responsiveness mediate the associations between support behaviors and cortisol change (hypothesis 4).
Method
Participants
Married couples (N = 191) were recruited from a small city in the Northeastern region of the U.S. using community and online advertisements. Participants had to be married, cohabiting, above the age of 18, fluent in English, not currently in couples therapy, and not in the process of separation/divorce. To have a hormonally homogenous sample, women were required to be premenopausal and not currently pregnant or nursing. Six couples were in same-gender marriages and were excluded from the current analyses, yielding an effective sample of 185 couples (50% cisgender women, 50% cisgender men). Average age for men was 34.02 (SD = 7.21, range = 19–56) and 32.44 (SD = 6.51, range = 19–51) for women. Participants identified as African American (men = 5.9%, women = 3.2%), Asian American (men = 5.9% men, women = 4.9%), American Indian (men = 0%, women = 0.5%), Latine (men = 4.3%, women = 3.2%), Middle Eastern (men = 3.2%, women = 4.3%), mixed race (men = 1.1%, women = .5%) and White (men = 79.5%, women = 82.7%). Average years of education was 13.41 (SD = 5.61) for men; with the modal degree being high school diploma/GED (36.2%), followed by bachelors (28.1%), and then master’s degrees (20.5%). For women, the average years of education was 14.15 (SD = 5.01); the modal degree was a master’s (29.2%) followed by bachelors (27.0%) and high school diploma/GED (21.6%). For husbands, 81.6% (N = 151) reported being employed with a modal income of $30,000 to $39,999 per year (N = 34, 18.4%), whereas 75.0% (N = 138) of wives reported being employed currently with a modal income of $0 to $9,999 (N = 48, 25.9%). More than half (59.5%) of couples had children who lived with them, with an average of 1.34 (SD = 1.36) children per home. Couples had been married an average of 6.48 years (SD = 6.13), with marital length ranging from just married to approximately 24 years.
Procedure
As part of a larger series of research questions, the saliva samples collected were used to measure cortisol as well as other biological variables (not described here). Participants were asked to not eat or drink anything other than water and not use tobacco products for 2 hours prior to their visit to ensure saliva sample purity. Because cortisol levels fluctuate throughout the day, lab visits were always scheduled for 5:00pm to maintain consistency across subjects. Couples completed individual informed consent and then were brought to separate rooms for the first set of questionnaires. At this time, each spouse was asked to think of something they would like to work on or change about themselves that they can discuss with their partner. They were told that the topic must be something about the individual and not about a relationship problem. This became the topic for that spouse’s social support task. The modal topic pertained to changes in physical health for wives (e.g., exercising more, quitting smoking; 34.1% for wives and 22.2% for husbands), and work-related stress/transitions for husbands (22.7%; cf., 14.6% for wives), followed by some form of broad personality/mood change (e.g., being patient, less depressed) for both wives (17.8%) and husbands (20.5%). The next most frequent topic for both husbands (10.3%) and wives (13.5%) pertained to some circumscribed behavioral change (e.g., becoming more organized).
Spouses were brought together for the first 10-minute discussion. They provided baseline saliva samples for cortisol measurement and completed a questionnaire related to the upcoming discussion. Ordering of the discussion topics was randomized. Couples were given brief instructions for the support discussion and then completed questionnaires measuring their expectations for their own and their spouse’s responsiveness in the upcoming discussion, which was videotaped for later coding. Following the first discussion, spouses were brought to separate rooms again to provide a second saliva sample and complete questionnaires for approximately 30 minutes. This intermediary period was introduced to allow time for any cortisol changes to return to baseline. Spouses were then brought together to complete the second support discussion using the same approach as the first, followed by the third saliva sampling and set of questionnaires completed separately. Afterward, they were brought together to receive information about the study and compensation ($100). On average, there was an interval of 29.98 minutes between the first (baseline) and second cortisol sample, and there was an average of 57.17 minutes between the second and third cortisol sample, which were spaced to mitigate any potential carryover across cortisol measurements.
Measures
Support Behavior was measured using observational coding via the Social Support Interaction Coding System (SSICS; Pasch et al., 2004). The SSICS requires coders to assign each speaker turn to one of six helper codes for the support giver (Positive Instrumental, Positive Emotional, Positive Other, Negative, Neutral, Off-Task), or one of four helpee codes for the support receiver (Positive, Negative, Neutral, Off-Task). We describe the codes briefly here and refer readers to the full coding system for additional detail. Helper Codes: Positive Instrumental support was coded for specific advice or feedback regarding actions that could be taken, or questions aimed toward formulating a plan of action. Positive Emotional support related to the partner’s feelings about the topic (e.g., clarifying feelings, providing reassurance). Positive Other support was coded for other positive support behaviors, such as showing a willingness to help. Negative helper support was coded when negative communication behaviors were observed, such as criticizing, withdrawing, or minimizing. Helpee Codes: Positive support receipt was coded when the support receiver used constructive communication behavior, such as analyzing the problem or clearly expressing needs. Negative support receipt was coded when the support receiver used negative communication behavior during the interaction, such as rejecting help or being defensive. All support behavior was quantified as the number of positive (sum of Positive Instrumental, Positive Emotional and Positive Other) and negative helper behaviors, and positive and negative helpee behaviors, for each spouse. Positive behavior frequencies ranged from 1–42, and negative behaviors from 0–16.
Each videotaped interaction was randomly assigned to two trained coders to reduce the influence of natural variation across coders and to measure inter-rater reliability for all videos. The mean of the two sets of code counts for each interaction was used to calculate final code counts for each video. Interrater reliability was acceptable (average ICC = .87). Outliers were reduced in magnitude so that they retained their place in the distribution but were within normal limits. Code counts were examined for skew and corrected as needed using standard square root or log transformations.
Perceived Partner Responsiveness (PPR) was measured just prior to and after each supportive discussion using three items adapted from Maisel and Gable (2009). Prior to each interaction, spouses rated three items on a scale of 1 (not at all) to 5 (very much): “In the upcoming discussion, I expect that my partner will (1) make me feel he/she understands me, (2) make me feel he/she values my abilities and opinions, and (3) make me feel cared for.” After each interaction, spouses rated three items on the same 5-point scale above: “In the discussion I just completed, my partner …” Scores for the 3 items were averaged separately for pre-discussion (average α = .91) and post-discussion (average α = .92) PPR scores. Support providers completed an analogous set of questions measuring the extent to which they expected to provide or provided responsive support. Univariate outliers were handled in the same fashion. PPR scores required a square root transformation to correct skew.
Cortisol samples were collected using Sarstedt Cortisol Salivette® Devices. Participants were asked to place a small sponge under their tongue for 2 minutes. These samples were first stored on ice until the end of the experiment, then transferred to a −80°C freezer while they awaited processing. Cortisol samples were analyzed using Salimetrics® High Sensitivity Salivary Cortisol Enzyme Immunoassay Kits. The sensitivity of the assay is 0.007 μg/dL. The inter- and intra-assay variation was 6.0% CV and 4.6% CV, respectively. Processing of the samples was carried out in accordance with the manufacturer’s instructions. Salivary cortisol levels have been shown to reflect plasma cortisol concentration (Kirschbaum & Hellhammer, 1994), particularly when using the Salimetrics® assay (Izawa & Suzuki, 2007).
Data analysis
Intercorrelations between primary study variables for husbands’ discussion topic (below diagonal) and wives’ discussion topic (above diagonal).
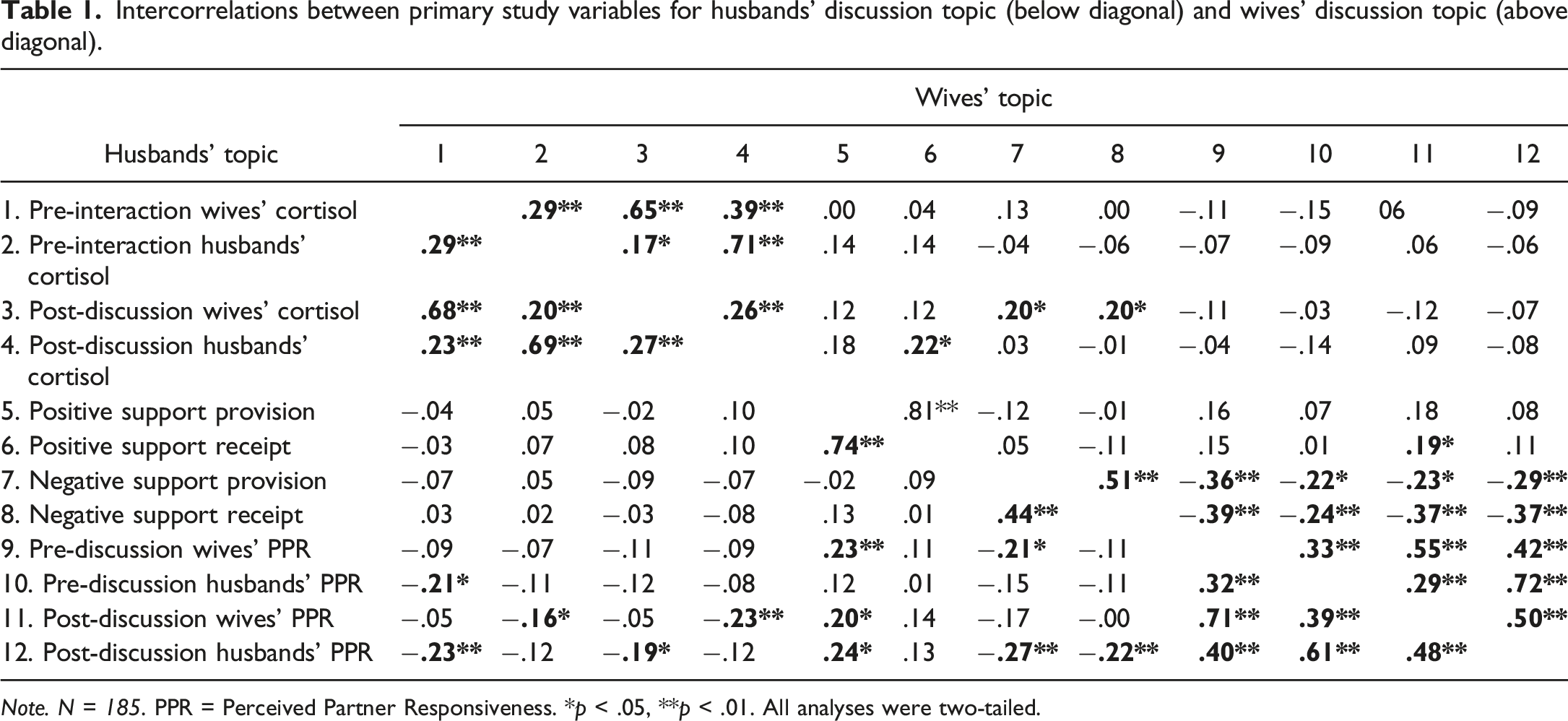
Note. N = 185. PPR = Perceived Partner Responsiveness. *p < .05, **p < .01. All analyses were two-tailed.
Using Structural Equation Modeling (SEM) in AMOS 25 and an actor-partner interdependence framework (Kenny et al., 2006), we developed a path model (Figures 1 and 2) evaluating the impact of support provider and receiver positive and negative behaviors on changes in cortisol directly and indirectly through PPR. We then tested for mediation effects in R using the PRODCLIN method (MacKinnon et al., 2007) based on our initial model results.
1
This allowed us to test our hypotheses by assessing the direct effects of support behaviors on cortisol levels (hypothesis 1a-b), direct effects of support behaviors on PPR ratings (hypothesis 2a-b), direct effects of PPR ratings on cortisol (hypothesis 3), and to test PPR as a mediator of the link between support behaviors and cortisol (hypothesis 4). Post-discussion cortisol (controlling for initial cortisol levels) was the outcome in all models, whereas post-discussion PPR (controlling for pre-discussion PPR) was tested as a mediator for the association between support behaviors and post-discussion cortisol. Each discussion (i.e., husband and wife topic) was analyzed separately, and each discussion was analyzed once with husband’s PPR and cortisol as the mediator and outcome, respectively, and then again with the wife’s. Across models, husbands’ and wives’ PPR had correlated disturbance terms (i.e., residual variances), as did their post-discussion cortisol levels. For the SSICS codes, husbands’ and wives’ positive behaviors (i.e., positive provision and receipt) were allowed to intercorrelate, as were husbands’ and wives’ negative behaviors. We planned to specify any additional covariances between the SSICS codes based on significant association emerging at the bivariate level. The following indicators are used here to indicate acceptable model fit in SEM (Kenny, 2020; Kline, 2011): non-significant χ2 value, .90 ≤ CFI ≤1.0 (“good fit” if CFI ≥.95), 0 ≤ RMSEA <.10 (“good fit” if RMSEA ≤.05), and .08 ≤ SRMR. Social support behavior during wife discussions predicting residualized post-discussion PPR and cortisol. Two path models are depicted which tested hypothesized associations between support behaviors by both partners, pre- and post-perceived partner responsiveness (PPR), and post-discussion cortisol (controlling for baseline levels) for wife discussions. Standardized coefficients for the model that included only wife assessments of PPR and cortisol for wife discussions are displayed as the left value for each path (marked as “W”), and those for the model that included only husband assessments of PPR and cortisol for wife discussions are displayed as the right value for each path (marked as “H”). All SEM analyses were two-tailed. *p < .05, **p < .01, ***p < .001. Social support behavior during husband discussions predicting residualized post-Discussion PPR and cortisol. Two path models are depicted which tested hypothesized associations between support behaviors by both partners, pre- and post-perceived partner responsiveness (PPR), and post-discussion cortisol (controlling for baseline levels) for husband discussions. Standardized coefficients for the model that included only husband assessments PPR and cortisol for husbands’ discussions are displayed as the left value for each path (marked as “H”), and those for the model that included only wife assessments of PPR and cortisol for husbands’ discussions are displayed as the right value for each path (marked as “W”). All SEM analyses were two-tailed. *p < .05, **p < .01, ***p < .001.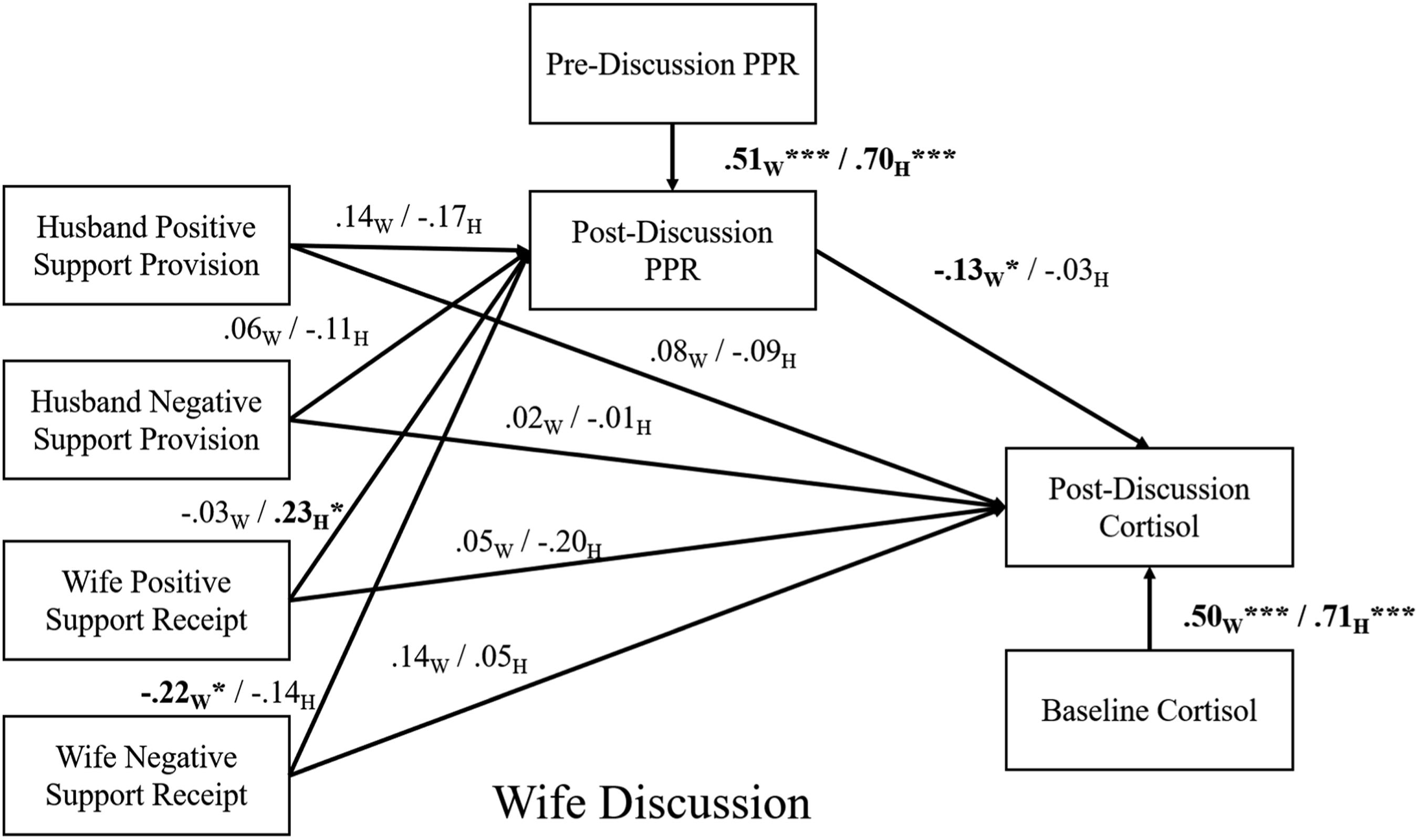

Results
Preliminary analyses
Missing data
Using the missing data pattern analysis feature in SPSS 25, we found 51.4% of cases had fully complete data, with the remaining cases having at least one missing value across spouses. Missing values predominantly came from the interaction tasks due to technical difficulties (N = 55 couples). There were 29 couples where at least one individual did not provide useable cortisol data at one of the two samplings. In cases where PPR scores were missing a singular item, the value was imputed using the scale mean, which is acceptable given the high reliability of the measure (see Schafer & Graham, 2002). There remained 23 couples where at least one of the pre- or post-PPR scores had missing values. Missing data on one variable was uncorrelated with missing data on another (rs ranged from |.02| to |.09|). Given this, and that missing data were largely related to randomly distributed technical problems, we assumed that the data were missing at random. As a further test, dummy codes for each variable were created to denote missing data across the SSICS codes, cortisol samples, and PPR measures. Correlations between these variables ranged from −.09 to .08, overall indicating that data missingness was orthogonal across these sets of variables. For the descriptive and bivariate analyses, we estimated coefficients based on the available data, so the listwise ns vary across analyses.
Descriptive analyses
Positive and negative social support provision and receipt behaviors differed in several ways across husbands’ and wives’ interaction topics. Wives displayed more negative support receipt behavior during their discussions relative to their husbands during his discussion topic, t (129) = −2.76, p = .007, d = .48. Additionally, husbands displayed more negative support receipt behaviors in their discussions when compared with their wives who were in the support-giving role, t (130) = −3.53, p = .001, d = .62. There were no significant differences in SSICS codes depending on whether the husbands’ or the wives’ task occurred first, except that husbands displayed more negative support receipt behaviors when their topic was discussed second, t (129) = −2.53, p = .013, d = .46. Positive support receipt and provision were highly correlated in both the husbands’ and wives’ task, as were negative support behaviors. In the wives’ task, increased positive support provision from the husband significantly associated with lower levels of wives’ negative receipt behavior. Husbands’ post-topic PPR scores were higher than their baseline PPR assessment, t (179) = −2.05, p = .04, d = .31, and pre- and post-PPR scores were highly correlated for both spouses in all discussions.
Means and standard deviations of cortisol assessments.
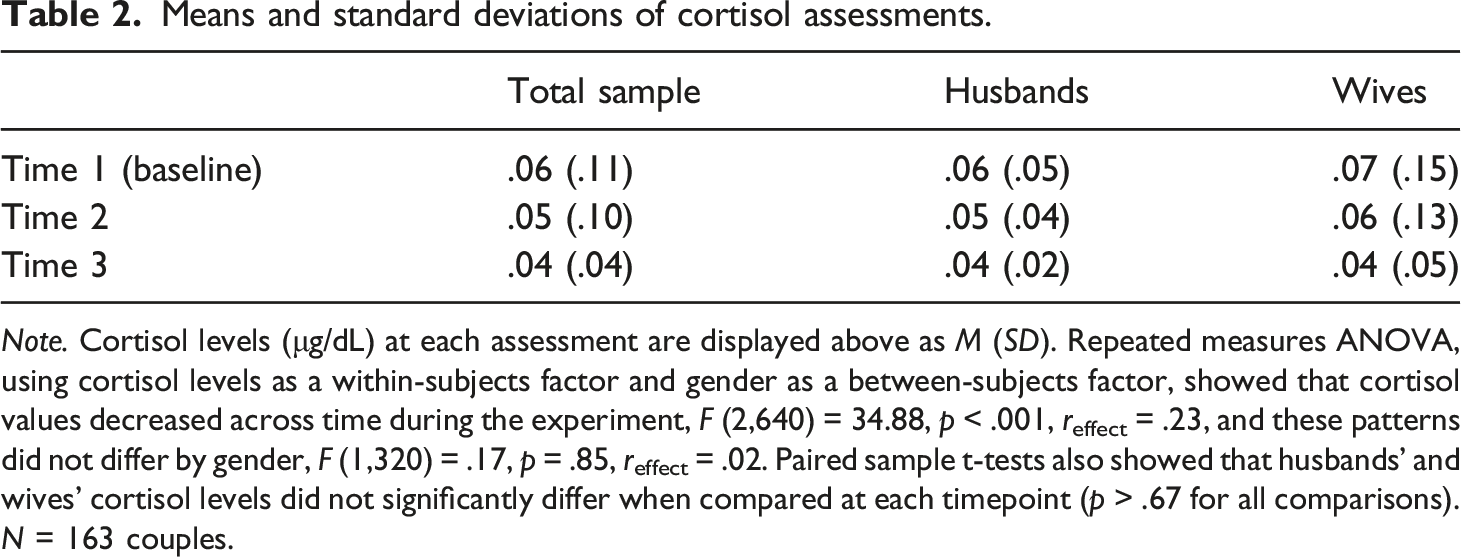
Note. Cortisol levels (μg/dL) at each assessment are displayed above as M (SD). Repeated measures ANOVA, using cortisol levels as a within-subjects factor and gender as a between-subjects factor, showed that cortisol values decreased across time during the experiment, F (2,640) = 34.88, p < .001, reffect = .23, and these patterns did not differ by gender, F (1,320) = .17, p = .85, reffect = .02. Paired sample t-tests also showed that husbands’ and wives’ cortisol levels did not significantly differ when compared at each timepoint (p > .67 for all comparisons). N = 163 couples.
Relative to baseline levels, cortisol was lower at the post-interaction samplings following both the wives’ discussions (t [157] = 10.42, d = 1.66, for husbands, and t [155] = 7.25, d = 1.16, for wives, ps < .001), and husbands’ discussions (t [157)] = 8.97, d = 1.43, for husbands and t [155] = 7.89, d = 1.27, for wives, ps < .001). Husbands’ post-interaction cortisol levels were higher when their discussion was first, t (154) = 3.53, p = .001, d = .57, and when wives’ discussions were second, t (149) = −5.12, p < .001, d = .84, perhaps reflecting some small gender differences in men and women’s comfort with the support task. Baseline cortisol levels were highly correlated with post-discussion assessments for both husbands and wives (see Table 1).
Bivariate correlations
As displayed in Table 1, higher pre- and post-discussion PPR scores for both spouses were generally associated with fewer negative behaviors in both spouses and more positive support behaviors by wives. These findings suggest that both expectations of PPR and evaluations of PPR were linked to actual support behavior in the expected directions. Regarding cortisol, wives’ positive support receipt and provision behaviors and pre- and post-PPR scores were negatively associated with cortisol. Negative support behaviors were positively associated with cortisol pre- and post-interaction. In the husbands’ task, baseline cortisol levels were negatively associated with partners’ PPR ratings. Higher post-interaction cortisol for each spouse was associated with lower post-discussion PPR scores in their spouses. For the wives’ task, negative behaviors by both spouses were linked to higher post-discussion cortisol levels for wives. Contrary to expectations, wives’ positive support receipt behaviors were linked to higher husband post-discussion cortisol.
Taken together, associations between cortisol and observed behavior in the wives’ interaction task (consistent with hypotheses 1 and 2) were evident; but, in the husbands’ task, there were more clear links between cortisol and perceived partner responsiveness (consistent with hypothesis 3 and 4). These latter findings suggested that wives and husbands with higher pre- and post-discussion cortisol had lower pre- and post-discussion PPR scores in the husbands’ discussion. They also were generally robust when partialling out support behavior variables. Specifically, husbands’ post-discussion PPR ratings following their discussion remained correlated with wives’ baseline cortisol levels, r = −.22, p = .03, and wives’ post-interaction cortisol, r = −.20, p = .049. Wives’ post-discussion PPR scores after the husbands’ discussion were also still correlated with husbands’ post-interaction cortisol levels, r = −.24, p = .014. This suggests that some of the correlations between PPR scores and cortisol were, to an extent, orthogonal to the support behaviors actually exchanged during the discussion.
Path models: Does providing or receiving social support and/or change in PPR predict change in cortisol?
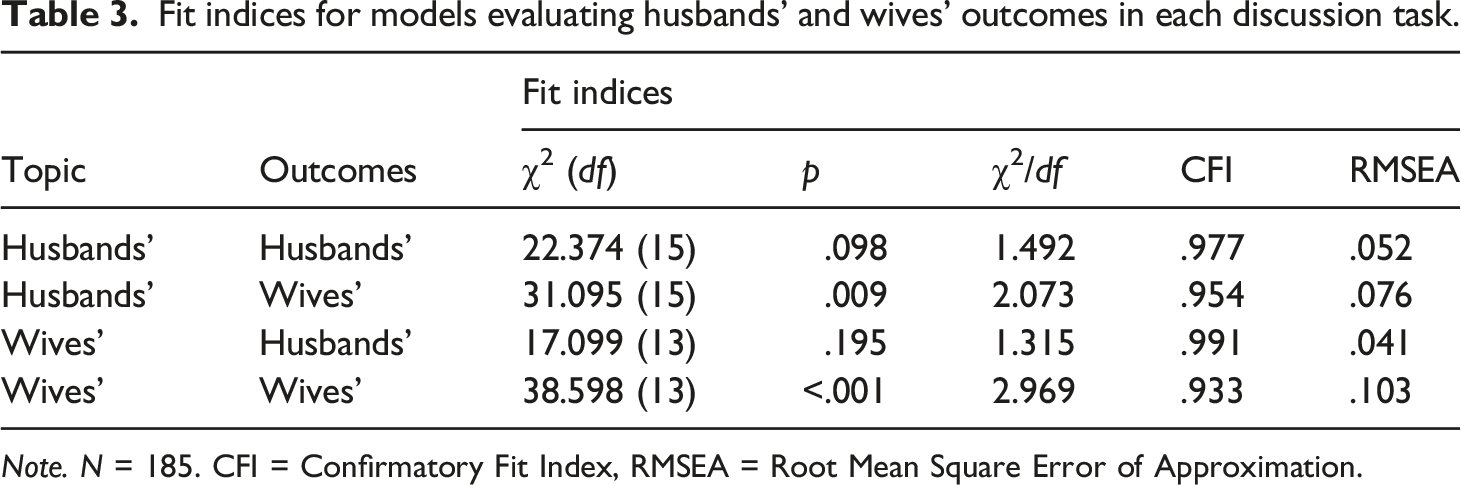
We analyzed path models specifying effects from SSICS support provider and receiver codes to changes in cortisol, directly and as mediated by residualized PPR scores, which measured the extent to which individuals felt more or less supported than they expected. Husbands’ and wives’ outcomes in each task were analyzed separately (see Figures 1 and 2). Model fit indices (Table 3) ranged from passable (wives’ discussion topic/wives’ outcomes) to excellent (wives’ discussion topic/husbands’ outcomes). Fit indices for models evaluating husbands’ and wives’ outcomes in each discussion task. Note. N = 185. CFI = Confirmatory Fit Index, RMSEA = Root Mean Square Error of Approximation.
Exploratory analyses
Several bivariate associations between wives’ cortisol levels and husbands’ PPR during the husbands’ interaction task were no longer significant when both pre- and post-interaction variables were modeled together. One interesting possibility is that wives’ pre-interaction cortisol is driving these associations, such that wives with higher levels of pre-interaction cortisol provided lower quality support as a result of higher cortisol levels. This lower quality support, in turn, corresponded to lower perceived quality of partner support by the husbands following their interaction. This explanation received support in exploratory partial correlation analyses that controlled for baseline cortisol. We found that wives’ baseline cortisol explained the association between their post-discussion cortisol and their husband’s evaluation of their responsiveness, r = −.06 p = .456. Controlling for husbands’ baseline cortisol only moderately attenuated the association between their post-discussion cortisol and wives’ evaluation of their own responsiveness, r = −.16, p = .053, suggesting a stronger effect for wives. Moreover, controlling for pre-discussion PPR did not meaningfully impact the association between wives’ post-interaction cortisol and husband’s post-interaction PPR, ruling out an alternative explanation for why the parallel multivariate tests produced null results. These findings considered overall suggest a pathway by which wives’ cortisol levels may predict the quality of their support, which in turn influences men’s perceptions of the provided support.
Discussion
Social support plays a role in improved health, but the mechanisms underlying this connection remain elusive. In line with longstanding calls to evaluate specific acts of support provision and receipt (Barrera, 1986) alongside their putative biological linkages (Uchino, 2004), we explored whether the way in which married partners exchange social support is linked to cortisol functioning, a presumed mechanism linking stress, social support, and health outcomes.
We found that support behaviors were not consistently linked to changes in cortisol following a supportive interaction, with the exception that husbands’ positive behaviors while receiving support paradoxically predicted increases in cortisol for wives (counter to hypothesis 1). However, we found that support behaviors were linked to perceived partner responsiveness in the expected directions, consistent with hypothesis 2. Specifically, wives who exhibited more positive behaviors in both discussions were rated more favorably by husbands, and both partners’ more negative behaviors while receiving support were associated with rating their spouses lower in PPR. Additionally, we found that wives’ ratings of PPR associated with decreases in their own cortisol levels during their discussions, aligned with hypothesis 3. Lastly, we found evidence for mediation (hypothesis 4) in which wives’ more frequent displays of negative support behavior were associated with increases in cortisol indirectly via declines in their ratings of PPR. Though not explicitly hypothesized, our exploratory analyses suggest that baseline cortisol potentially plays an important role in the association between perceived partner responsiveness and cortisol. These findings suggested that higher cortisol levels prior to a support discussion may influence the exchange of support in ways that depreciate perceived responsiveness of the support provider. Taken together, our findings show evidence that observable support behaviors exhibited by couples are closely linked to feeling understood, validated and cared for by a partner, and that these effects account for increases in cortisol for wives when they display more negative support behaviors. More broadly, our data also show that skillful delivery of support is evaluated more favorably by partners, but is inconsistently and at times paradoxically linked to cortisol responses.
Our study showed for the first time that negative support behaviors exhibited by wives lead to increases in cortisol, but only when accompanied by low ratings of perceived partner responsiveness. This represents an important advancement in our understanding of PPR as a mechanism through which support behaviors can affect our biological stress response system. This builds upon past research using self-report measures that showed that PPR mediated the association between emotional support and longitudinal health outcomes (Selcuk & Ong, 2013). At the same time, these effects were only observed for wives, and only in the case of negative behaviors while receiving support. In other words, we did not find that positive displays of support reduced cortisol responses, but rather that negative behaviors increased them for wives.
Our counterintuitive finding that husbands’ display of positive behaviors while receiving support associated with increased cortisol for wives is intriguing and warrants further exploration. Although consistent with the paradoxical effects found for positive communication on cortisol during conflict (e.g., Fehm-Wolfsdorf et al., 1999; Robles et al., 2006), this finding is somewhat misaligned with the notion that skilled support by one partner would attenuate cortisol levels in the other. Rather, they suggest that positive behaviors displayed by the support receiver tie into higher cortisol levels in those providing support. A greater positive receipt behavior may signal a greater readiness for change, which in some cases could harbinger potential stress (e.g., changing jobs) or a lifestyle change (e.g., diet) for the other partner as well. Importantly, these findings provide evidence that specific communication behaviors not only associate with cortisol levels, but are also linked to proximal changes in cortisol functioning within the context of a given support exchange.
The finding that skillful delivery of support, as assessed specifically by displays of more positive and fewer negative support behaviors, was generally associated with perceived partner responsiveness in expected directions has not previously been shown. Given how consistently PPR is associated with relationship well-being, these findings provide important insight into how couples might support each other in specific ways that will increase feelings of understanding, validation and caring. For example, positive support giving behaviors (e.g., providing emotional comfort) and positive support receiving behaviors (e.g., clearly expressing one’s needs) may increase perceived partner responsiveness in couples. Moreover, these findings shed light on the important role of the person receiving support in how partners feel about support interactions. The role of the support receiver’s specific actions in a support transaction is understudied in couples research (e.g., Lawrence et al., 2008), relative to a long-standing focus on how spouses provide support. Our study shows that couples who are better at all aspects of support – including soliciting, receiving and providing support – are more likely to perceive each other as responsive.
Our exploratory finding that wives’ baseline cortisol levels fully accounted for the association between husband PPR ratings and wife post-interaction cortisol also warrants further study. It is plausible that wives with higher initial cortisol levels may be more stressed – either proximally or in general – and thus had fewer personal resources to provide support, a fact reflected in their spouse’s evaluation of their responsiveness. We also found a parallel pattern for husbands that closely approached significance. Given that husbands’ and wives’ cortisol levels were correlated, this pattern may reflect some form of physiological synchrony (Helm et al., 2014) between husbands’ and wives’ pre-interaction cortisol levels, which in turn filtered into appraisals of the interaction. These effects are consistent with previous research that subjective evaluations of self- and partner-supportiveness are associated with cortisol levels (e.g., Slatcher et al., 2015). However, rather than appraisals of responsiveness during an interaction attenuating cortisol levels, these findings suggest that cortisol levels going into an interaction may correlate with less favorable appraisals of partner responsiveness thereafter. This may also reflect a form of projection of negative support processes based on having currently high levels of stress. Extending Lemay’s model of projection of PPR (Lemay & Clark, 2015; Lemay et al., 2007), it is possible that one’s own awareness of high stress levels (and ability to regulate stress) could potentially create lower expectations of responsiveness that lead to partners’ actual lower ratings of responsiveness. This process of projection may also be evident in our findings that partners who showed more negative behaviors while receiving support rated partners lower in responsiveness.
Several of the correlations between partner responsiveness and cortisol emerged independent of the behaviors exchanged during the interaction. This adds to the growing evidence highlighting the idiosyncratic nature of how social support is experienced (Gleason et al., 2008), the discrepancy between the effects of actual received support and the perception of support (Haber et al., 2007), the influence of motivated cognition on support processes (Lemay & Clark, 2015), and the generally more robust associations of perceived support with health-related outcomes (Ditzen & Heinrichs, 2014). Importantly, we found that wives who reported greater than expected levels of PPR during their interaction topic had corresponding declines in cortisol levels, suggesting that something palliative also may be happening inside the supportive interaction. Although these behaviors emerged while controlling for observed behavior (SSICS codes), the frequency counts we used may have missed something in the interaction process, or elements of the interaction not specifically targeted by the SSICS (e.g., affect) may have played a role in subsequent cortisol changes. Further research is needed to determine what elements of the interaction appear to underscore the enhanced perception of responsiveness for wives.
Strengths and limitations
This study has several important strengths. This is the first study to test perceived partner responsiveness as a mechanism linking observable support behaviors and cortisol levels. The use of social support interactions and observational coding provides a more objective sample of how social support processes may play out for couples in real time. We also used an established social support interaction paradigm (Pasch & Bradbury, 1998) and coding system, making our findings comparable to other studies of social support processes in marriage (e.g., Sullivan et al., 2010). In addition, the range of discussion topics adds naturalistic variability to our design, so that the emergent effects can be interpreted as consistent across a diverse array of support needs. Likewise, we used a sample of established marriages that varied in length, suggesting that the effects identified for both observed behavior and perceived support occur in more stable unions, but are not tethered to a particular relationship stage.
This study also has several limitations. The topic of discussion, which varied in how stressful the content appeared to be and in the emotional depth of disclosure, was not considered. Though this approach carries advantages, as mentioned above, heterogeneity may have attenuated effect sizes, which were predominantly small. Likewise, the topics selected pertained mostly to personal change, which may reflect some form of chronic role strain, stressful life event, or both (Kiecolt, 1994), with these different backdrops potentially linking to cortisol functioning in different ways. Future studies could measure how stressful the topics are to each individual partner and examine the ways that support processes change across types of topics. Alternatively, researchers could employ a standardized lab-based stressor (Ditzen et al., 2008a, 2008b) or focus on a single circumscribed topic that occurs naturalistically (Kroenke et al., 2006). These paradigms carry their own limitations, but a clearer picture may emerge as different approaches converge on particular effects, or may suggest influences particular to one form of stress or another. Another limitation is that all couples undertook the social support interaction tasks, as opposed to some engaging in a control task, limiting our ability to interpret husbands’ and wives’ significant decreases in cortisol across the interaction tasks as reflecting something about the social support processes therein. This would align with other findings that a verbally supportive partner (vs. being alone) can buffer the impacts of a stress induction on cortisol (e.g., Ditzen et al., 2008b), but would extend the phenomenon to encompass a broader range of supportive situations. Inclusion of a parallel dyadic task would also help isolate support as the operative mechanism. It may be useful to include some other type of interaction context (e.g., conflict), which could help determine if any of the presently observed effects for specific communication behaviors are specific to support or domain-general (e.g., negative communication).
Additionally, the use of broad positive and negative categories of support behavior does not lend itself to specific recommendations about what spouses can do to respond to each other’s needs and reduce partners’ physiological reactivity. Future studies could examine the effects of contingent support behaviors, or assess whether it would be helpful for spouses to identify for themselves what kind of support they tend to respond well to and communicate this to partners. Additionally, although the decision in this study to measure and control for PPR expectations prior to the discussion allowed us to isolate PPR more specific to this interaction, it is also possible that this primed participants to examine their own and their partners’ responsiveness more closely. This priming could have impacted ratings of PPR, or even support behavior. Future studies more closely focused on the impact of PPR expectations are warranted. Lastly, as with all studies, the results should be confirmed with larger and more diverse samples to enhance generalizability, including (but not limited to) more racially and ethnically diverse couples, non-U.S. couples, sexual and gender minority couples, couples with disabilities, and non-monogamous couples.
Conclusion
The current study examined whether observations of social support behavior were linked to cortisol changes and ratings of perceived partner responsiveness, whether partner responsiveness was linked to changes in cortisol, and explored the possibility that these three sets of variables formed a possible causal pathway. Our findings suggest that the effects of positive and negative communication behaviors observed during conflict also extend to the context of social support. Overall, we did not find evidence of a stress-buffering effect for more skillful support, but did find a pattern in which more skillful support was generally linked to higher perceived partner responsiveness. We found that negative support receipt behaviors (e.g., rejecting help, criticizing spouse) for wives in particular appeared to have a “stress-amplifying” effect on cortisol by way of lower ratings of partner responsiveness. We also found preliminary evidence that baseline cortisol levels may negatively impact aspects of support interactions that should be replicated in future studies. These findings suggest that couples would benefit from using more positive support skills and fewer negative support behaviors to enhance experiences of perceived partner responsiveness, and that wives in particular may mitigate physiological reactivity to supportive discussions by using fewer negative support behaviors. We recommend that these findings be integrated into couple interventions to enhance social support skills, specifically for couples to learn and practice more positive expressions of support in place of more negative tactics. We also recommend tailoring this type of intervention to a couple’s specific needs and preferences for support.
Footnotes
Author’s note
The writing of this paper was supported by the Office of Academic Affiliations, Advanced Fellowship Program in Mental Illness Research and Treatment, Department of Veterans Affairs. The findings do not necessarily reflect the opinions or policies of the Department of Veterans Affairs.
Acknowledgments
Tarah Midy, Davis Brigman, Edwin Ortiz, Samantha Wagner, Christina Colon, Malaina McKenzie, Meghan Axman, Jacklyn Sullivan, Kathy Benhamou, Nadav Bashary, Karina Hain, Shelby Rakusin, Sophie Rodenbush, Christopher McKiever, Emma Ryan, Leslie Apacible, Bijan Kashani, Callie Patsellis, Melissa Blankstein, and Geancarlo Jordan assisted with data collection and analysis. Kieran Sullivan and Laurie Pasch consulted on the behavioral coding system. Terrence Deak and Mary Ann Swain provided guidance and feedback on the project. We are grateful for their help.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the SUNY/RF Research Collaboration fund (PI: Mattson).
Open research statement
As part of IARR’s encouragement of open research practices, the author(s) have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared but are available upon request. The materials used in the research are available upon request. Data and materials may be requested by contacting the authors via email, particularly Richard Mattson (