
Abstract
Mothers with young children were particularly susceptible to elevated stress levels during the COVID-19 pandemic. This study examined dynamic, reciprocal, longitudinal relationships between maternal perceived stress, perceived relationship quality with the partner, and mother-to-child bonding. The sample consisted of n = 1,394 mothers of children aged 0 to 3 years who completed online questionnaires at three time points between May 2020 to May 2022. We analyzed a Random Intercept Cross-Lagged Panel Model with maternal stress, relationship quality with the partner, and mother-to-child bonding, enabling the separation of stable between-person differences and dynamic within-person processes. At the between-person level, lower partner relationship quality was associated with higher average stress (r = −.20) and impaired mother-to-child bonding (r = −.29), while stress and impaired bonding were strongly correlated (r = .56). At the within-person level, increases in partner relationship quality predicted intraindividual decreases in stress (βT1→T2 = −.19; βT2→T3 = −.21) and, at trend level, decreases in impaired bonding (βT1→T2 = −.15; βT2→T3 = −.16). The results demonstrate the interrelation of stable components of maternal stress, relationship quality, and bonding. Additionally, they highlight the dynamic role of the maternal perceived relationship quality with the partner in shaping maternal stress and bonding, positioning relationship quality as a resilience (or risk) factor for maternal well-being during crises. An exploratory model including sociodemographic and pandemic-related variables further showed that factors such as maternal education, income, family size, and work changes significantly shaped baseline stress and relational functioning. Hence, support services should focus on strengthening the relationship with the partner while being tailored to families’ structural contexts to mitigate stress, promote bonding, and prevent adverse consequences for mothers, children, and families.
Introduction
While becoming a parent is often accompanied by positive emotions and a sense of meaning, this transition can also be associated with heightened perceived stress, negative emotions (e.g., worry, anxiety), changes in the couple relationship dynamic, sleep disturbance, and financial strain (Nelson et al., 2014). These challenges are particularly pronounced in the early postpartum period, when parents rely strongly on social support (Saur & Dos Santos, 2021). During the COVID-19 pandemic, however, access to social support was substantially reduced, leaving families to rely primarily on intrafamilial relationships (Buechel et al., 2022; Gao et al., 2022). Within this context, two central relational domains are especially relevant: the perceived quality of the partner relationship, where applicable, and the parent’s emotional connection to their child, commonly conceptualized as bonding (Hahlweg, 2016; Le Bas et al., 2020). Importantly, analyses based on an earlier dataset from the same study addressed in the present work indicate that mothers, in particular, experienced heightened psychological burden, including elevated levels of perceived stress, during the pandemic (Reck et al., 2025; Woll-Weber et al., 2025). Consequently, for mothers in the early postpartum years during the pandemic, both partner relationship quality and mother–child bonding may have functioned as sources of resilience or as additional stressors, depending on their quality. Understanding how maternal stress and intrafamilial relationship processes unfold is therefore critical, especially in crisis contexts.
The Interplay Between Maternal Perceived Stress and Partner Relationship Quality
Numerous studies have shown a link between mothers’ perceived stress and their perceived relationship quality with their partner: Some suggest pathways leading from perceived stress to problems in the parental relationship, including reduced relationship quality (Milek et al., 2017), while others argue for a pathway from partner relationship quality to maternal stress (Martin & Brock, 2023). During the pandemic, the prevalence of elevated stress levels among postpartum women was markedly higher than in pre-pandemic periods (Gao et al., 2022; Suárez-Rico et al., 2021). Furthermore, couples often experienced increased relationship problems and lower relationship quality with the partner compared to pre-pandemic times (Pietromonaco & Overall, 2022; Vigl et al., 2022). In line with pre-pandemic studies, several longitudinal studies during the pandemic found an association between high perceived stress and poor partner relationship quality (Balzarini et al., 2023; Overall et al., 2022). It seems reasonable to posit that pandemic-related stress resulted in negative processes within the couple relationship, such as maladaptive coping with increasing challenges, which could then have impacted partner relationship quality, as suggested by Pietromonaco and Overall (2021). Conversely, circumstances during the pandemic (e.g., lockdowns) and resulting struggles in the partner relationship (e.g., more conflicts) may have contributed to increased stress and mental health problems for mothers (Daugherty et al., 2022; Xie et al., 2022). For instance, results from a cross-lagged panel model (CLPM) in a sample of pregnant women during the pandemic, showed that maternal perceived partner relationship quality predicted later depression and anxiety symptoms, but not vice versa (Xie et al., 2022).
The Link Between Maternal Stress and Mother–To-Child Bonding
Maternal bonding, defined as the mother’s emotional connection to her child, is crucial for healthy child development (Le Bas et al., 2020) and has been repeatedly linked to maternal stress (O'Dea et al., 2023). Similar to difficulties in the relationship between the mother and her partner, it is plausible that elevated maternal stress may negatively affect the mother-to-child bond, while bonding impairments and the resulting negative emotions (e.g., guilt, shame) may, in turn, increase maternal perceived stress (de Cock et al., 2017; Reck et al., 2016; Yazdanimehr et al., 2023). A significantly higher proportion of mothers giving birth during the pandemic reported impairments in the mother–child bond compared with those who gave birth before the pandemic (Fernandes et al., 2021; Mousavi et al., 2021). In addition, studies during the pandemic indicate a positive association between mothers’ perceived stress and impaired bonding (Fernandes et al., 2021; Power et al., 2024). Despite the potential for reciprocal associations between the two constructs, most studies conducted both before and during the pandemic have primarily examined the effects of perceived stress on impaired bonding (O'Dea et al., 2023). In a prior study based on the same sample used in this paper, Reck et al. (2025) analyzed the first two of the three measurement points available at that time using a CLPM and found that impaired bonding predicted subsequent maternal perceived stress during the pandemic, whereas perceived stress did not predict later bonding impairments. These findings highlight the need for approaches capable of detecting not only potential longitudinal effects of stress on bonding, but also effects in the opposite direction.
Partner Relationship Quality and the Mother–Child Bond: Interlinked Intrafamilial Relationships
The mother’s perceived relationship with the partner and maternal bonding are highly interrelated and should therefore not be treated as independent levels within the family system (Cox & Paley, 2003; Tichelman et al., 2019). Poor partner relationship quality seems to be connected to lower-quality parenting practices (Chen et al., 2022; Roos et al., 2021), with potential long-term effects on the parent-child relationship and offspring development (Claussen et al., 2022). On the other hand, mothers’ perceived support by their partner, a crucial aspect of overall relationship quality, may be a protective factor for impaired bonding (Cuijlits et al., 2019). Although studies suggest that both of these intrafamilial relationships were challenged during the COVID-19 pandemic, longitudinal research examining their interrelation during this period remains scarce.
Interconnected Family Dynamics Between Maternal Stress, Partner Relationship Quality, and Bonding: Research Gaps and Study Aims
Although several studies conducted before and during the pandemic indicate longitudinal associations between maternal stress, relationship quality with the partner, and bonding (Balzarini et al., 2023; Power et al., 2024; Tichelman et al., 2019), several important gaps in the literature remain. First, previous studies have often examined only one direction of potential longitudinal effects between two of these constructs, without considering the reverse direction or possible bidirectional dynamics. On the one hand, elevated perceived stress and psychological burden may have led to lower partner relationship quality and impaired bonding (Liu et al., 2022; Overall et al., 2022). On the other hand, high-quality intrafamilial relationships may have served to mitigate perceived stress while negative experiences in intrafamilial relationships potentially increased stress levels and their adverse consequences (Mousavi et al., 2021; Pauly et al., 2022; Reck et al., 2025; Tepeli Temiz & Elsharnouby, 2022). Additionally, mothers’ relationship quality with their partner may be closely linked to the quality of the mother–child bond (Tichelman et al., 2019). Moreover, reciprocal dynamics between these processes may contribute to vicious cycles of heightened stress and deteriorating relationship quality within the family system, particularly when spending prolonged periods together at home due to pandemic-related restrictions. Therefore, examining maternal stress, partner relationship quality, and mother–child bonding within a longitudinal reciprocal framework appears crucial for a more comprehensive understanding of their interrelations during the pandemic.
Second, previous studies examining maternal perceived stress, partner relationship quality, and bonding have rarely focused on intraindividual changes in these constructs over time. While initial studies suggest that intraindividual changes in maternal stress are associated with changes in partner relationship quality, most have only examined their co-occurrence or investigated dynamic processes in one direction (Pauly et al., 2022; Rusu et al., 2020; Tepeli Temiz & Bilican, 2024). Studies examining such dynamic effects involving maternal bonding – or all three constructs simultaneously – remain particularly scarce, and, to the best of the authors’ knowledge, the present study is the first to investigate all three constructs jointly in a longitudinal framework in the context of the COVID-19 pandemic. To better capture these complex and dynamic intrafamilial processes, longitudinal analyses should distinguish between stable between-person differences and within-person fluctuations. Failure to separate these levels of analysis, as occurs in traditional cross-lagged panel models (CLPMs), may lead to misleading conclusions about developmental or causal processes. Advanced methodological approaches such as the Random-Intercept Cross-Lagged Panel Model (RI-CLPM; Hamaker et al., 2015) allow researchers to disentangle between- and within-person effects. While such distinctions are generally important in longitudinal research, they may be particularly relevant in the context of the COVID-19 pandemic, where rapidly changing circumstances and regulations likely contributed to substantial within-person variation in family dynamics and parental stress. A better understanding of these family processes during the COVID-19 pandemic offers valuable insights into the most effective ways of providing support to families during such exceptional times.
Addressing these research gaps, we hypothesized and tested reciprocal longitudinal associations between mothers’ perceived stress, their perceived relationship quality with their partner, and maternal bonding within a model that separates stable between-person differences and dynamic within-person fluctuations. To this end, an RI-CLPM was applied to longitudinal data from a German community sample across three time points during the COVID-19 pandemic.
Method
Participants and Procedure
The data for this study was assessed as part of the longitudinal online survey “CoviFam”, which is a COVID-19-specific subproject of a larger longitudinal observational study (“COMPARE_interaction”). The online survey link was offered to a community sample of parents with children between 0 and 3 years in Germany, Austria, and Switzerland to assess their psychosocial well-being during the COVID-19 pandemic. Parents were recruited via medical institutions (e.g., birth clinics, pediatricians, gynecologists), professional regional and national networks (e.g., midwifes, nurses), and different social media networks (i.e., Instagram, Twitter, Facebook). Data was collected from May 2020 to May 2022. The first measurement point (T1) spanned from May to November 2020. The online survey link was reopened and participants of the first wave were contacted again in February and March 2021 for a second measurement point (T2) and in February until May 2022 for a third measurement point (T3), when regulations were stricter again (see Figure 1 for the severity of regulations). Participants provided their informed consent online. The study was approved by the ethics committee of the medical faculty, Ruprecht-Karls-University, Heidelberg, in agreement with the Ludwig Maximilian University, Munich (vote: S-446/2017). Covid-19 situation in Germany from January 2020 to May 2022. Trajectories of cases, deaths, and government response during the COVID-19 pandemic in Germany. Confirmed deaths are shown cumulatively. Grey areas represent the study measurement times. Figure based on the Oxford COVID-19 Government Response Tracker (https://github.com/OxCGRT/covid-policy-tracker/blob/master/documentation/index_methodology.md)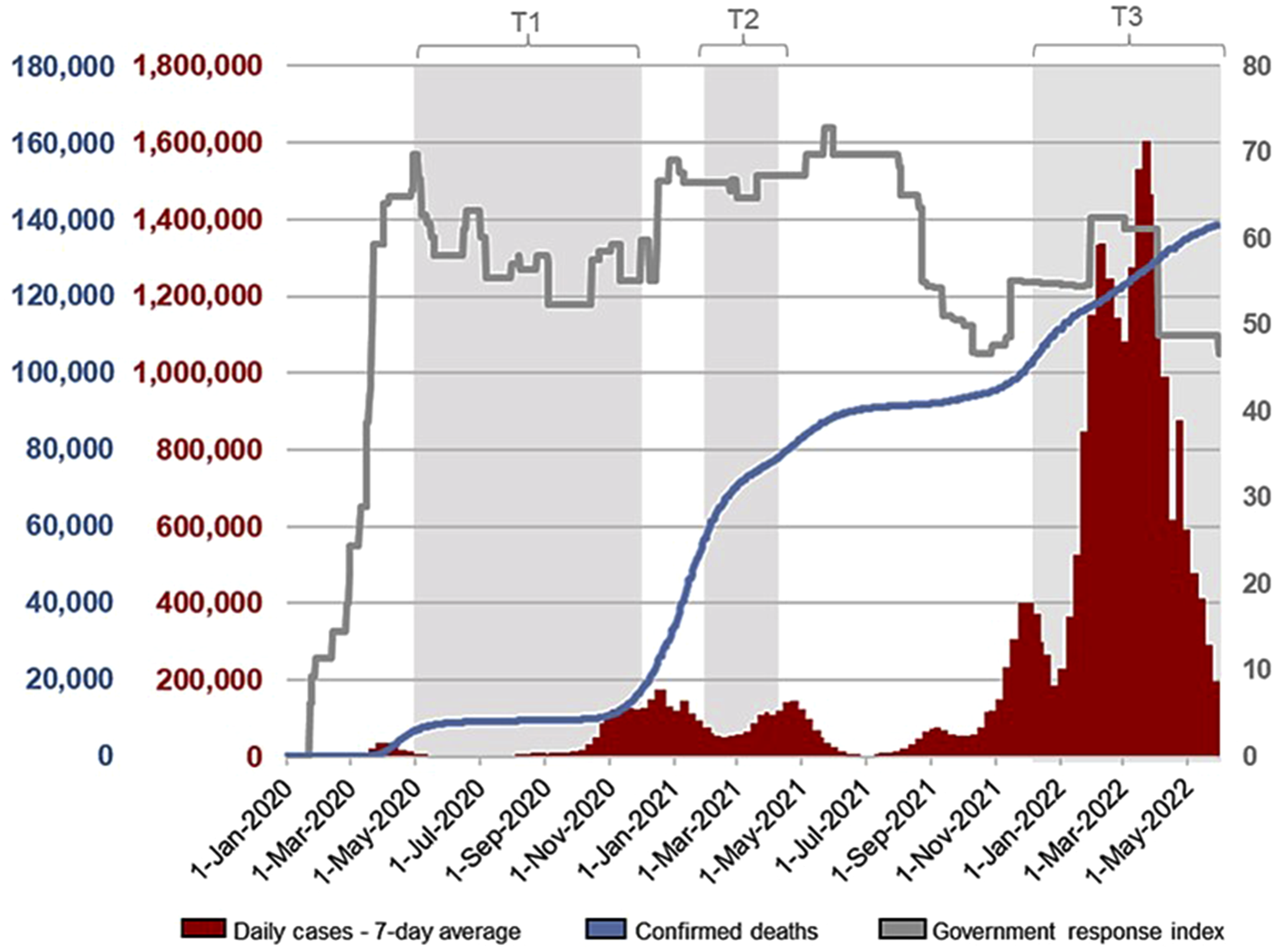
Demographic Information of the Sample (nT1 = 1,394, nT2 = 544, nT3 = 305)
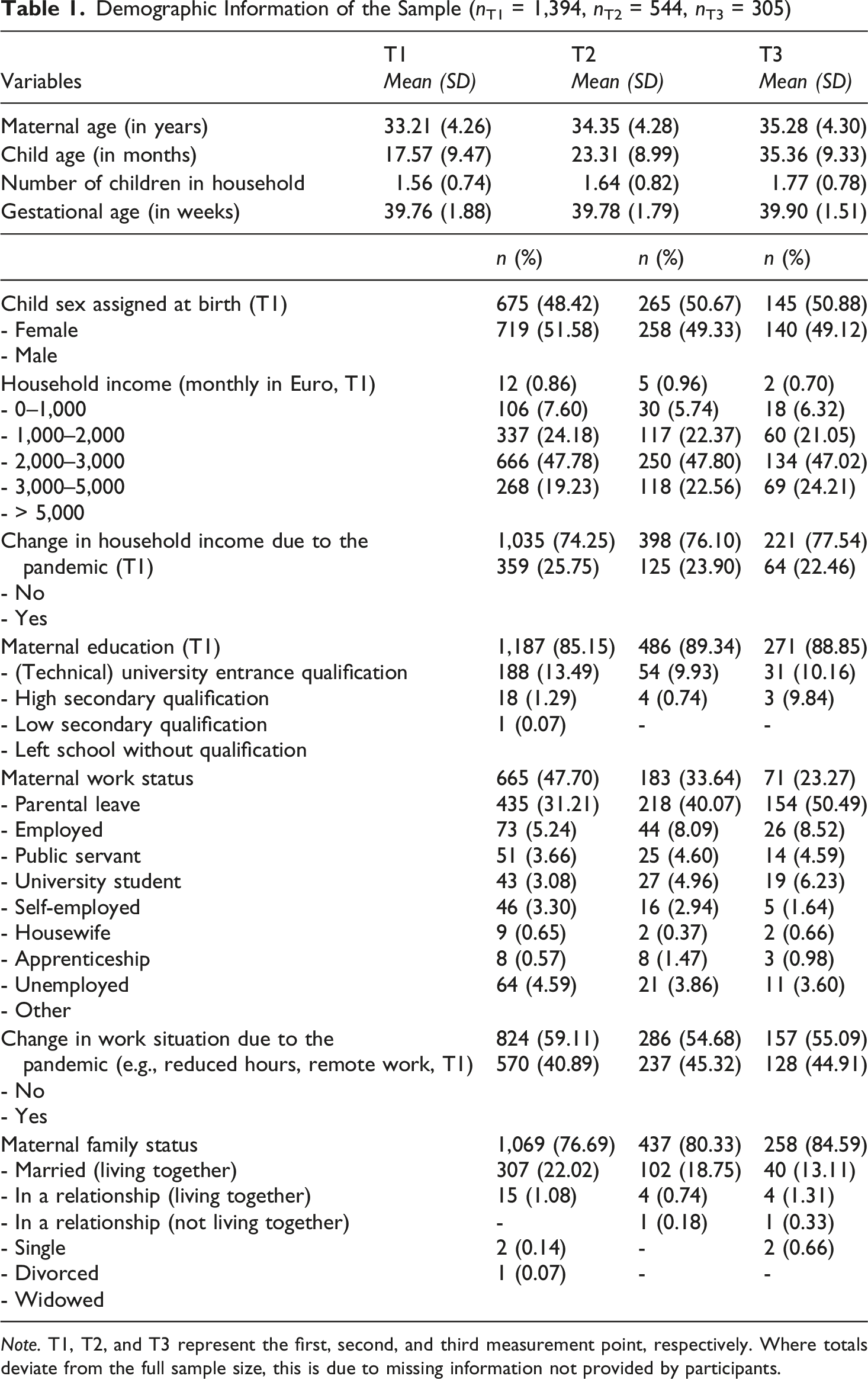
Note. T1, T2, and T3 represent the first, second, and third measurement point, respectively. Where totals deviate from the full sample size, this is due to missing information not provided by participants.
Regarding attrition analysis, first, T1 data of n = 544 mothers who participated at both T1 and T2 (and optionally also T3) were compared to T1 data of mothers who only participated at T1 (n = 818): The groups did not differ significantly on most sociodemographic and outcome variables at T1: Differences were only found for (1) mothers’ age (t = −4.83, p < .001), with mothers in the longitudinal sample being slightly older (M T1andT2/T1toT3 = 33.88 years, M onlyT1 = 32.73 years, d = 0.27). The difference for (2) perceived stress was negligible in effect size with mothers in the longitudinal sample reporting slightly lower values (t = 2.52, p = .012; d = 0.14; M T1andT2/T1toT3 = 18.04, M onlyT1 = 19.04). For (3) school degree, (4) monthly net income, (5) family status, and (6) changes in occupation due to the pandemic, the significant differences were negligible in effect size (Wilcoxon’s W = 19,259, p < .001, Cliff’s delta = −0.12; W = 194,584, p = .003, Cliff’s delta = −0.09; χ 2 (4) = 9.38, p = .032, Cramer’s V = 0.08; χ2 (1) = 6.97, p = .008, Cramer’s V = 0.07, respectively). The first step of the attrition analysis indicates no meaningful differences between mothers who continued after T1 and those who dropped out after T1, with respect to the assessed sociodemographic and outcome measures. The second step of the attrition analysis also indicated no meaningful differences between mothers who continued after T2 (n = 232) and those who dropped out after T2 (n = 292), with respect to the assessed sociodemographic and outcome measures at T2: The groups did not differ significantly on any sociodemographic or outcome variables, except that children of mothers who took part at all three time points were slightly younger, with a negligible effect size (Wilcoxon’s W = 37,294, p = .047, d = 0.18, M T1toT3 = 22.66 months, M T1toT2 = 24.27 months).
Measures
Multiple constructs of family context and general demographics were assessed in the aforementioned larger online survey. For this study, maternal perceived stress, relationship quality with the partner, and impaired bonding were the constructs of interest.
Perceived Stress
Mothers’ self-reported perceived stress was assessed using the German version of the Perceived Stress Scale (PSS-10) as published by Reis et al. (2019) (original version by S. Cohen et al. (1983)). The instrument contains 10 items (e.g., “In the last month, how often have you been upset because of something that happened unexpectedly?”). Items are answered on a 5-point Likert scale (0/“never” to 4/“very often”). Higher sum scores, ranging from 0 to 40, indicate higher perceived stress. The internal consistencies of the scale were equal or above 0.88 at all time points (Cronbach’s α = 0.88 at T1, α = 0.90 at T2, α = 0.90 at T3).
Relationship Quality With the Partner
For the assessment of mothers’ perceived relationship quality with their partner, the abridged version of the German partnership questionnaire “Partnerschaftsfragebogen” (PFB-K, Hahlweg, 2016) was applied. Nine of its 10 items describe the partner’s potential behavior within a relationship (e.g., “He/She tells me that he/she likes me”) or mutual/joint couple behavior (e.g., “We talk to each other for at least half an hour in the evening”). Participants were asked to indicate on a 4-point Likert scale from 0 to 3 (“never/very rarely” to “very often”) how often such behavior occurs in their relationships. A 10th item assessed overall couple relationship satisfaction and was rated on a 6-point scale from 0 to 5 (“very unhappy” to “very happy”). This 10th item is not part of the sum score and was therefore excluded from further analysis. The PFB-K consists of three sub-scales (i.e., disagreement, affectionateness, and communication). An overall sum score was calculated as follows: [(9-disagreement) + affectionateness + communication] (Hahlweg, 2016). Higher overall sum scores, ranging from 0 to 27, indicate higher relationship quality. The internal consistencies of the scale were equal or above 0.85 at all time points (Cronbach’s α = 0.85 at T1, α = 0.87 at T2, α = 0.88 at T3).
Maternal Impaired Bonding
To assess maternal impaired bonding, the German version of the Postpartum Bonding Questionnaire (PBQ-16, Reck et al., 2006), originally developed by Brockington et al. (2001), was applied. The items (e.g., “I feel distant from my baby”) are scored on a 6-point Likert scale (0 for “always” to 5 for “never”). Higher sum scores, ranging from 0 to 80, represent more impaired bonding, hence lower maternal bonding quality. The internal consistencies of the scale were equal or above 0.85 at all time points (Cronbach’s α = 0.85 at T1, α = 0.87 at T2, α = 0.86 at T3). It should be noted that the PBQ-16 has been validated only for use during the first year postpartum. Given that our sample included mothers of children aged 0–3 years, we applied a slightly adapted version in which the term “baby” was replaced by the more general term “child.” Based on expert consensus, this adaptation was deemed the best available proxy for assessing the mother–child relationship across the full age range studied, as alternative validated instruments are only applicable for toddlerhood onward. To address potential age-related differences, child age was therefore included as a control variable in an exploratory model.
Statistical Analyses
All analyses were conducted in R, version 4.5.1 (R Core Team, 2025) using RStudio, version 2025.5.1.513 (Posit team, 2025) applying the lavaan package (Rosseel, 2012) as the primary tool for structural equation modeling. In preliminary analyses, paired t-tests with Cohen’s d (J. Cohen, 1988) were used to examine changes in the main outcome measures across time points. Dynamic longitudinal relationships between the model variables (i.e., perceived stress, relationship quality, and impaired bonding) were investigated by applying an RI-CLPM over three measurement points (T1, T2, T3). This approach enabled the separation of stable trait-like between-person differences (captured in a random intercept for each model variable) and dynamic intraindividual within-person processes (captured by a latent factor for each model variable for each time point). Parameter estimates were obtained by a maximum-likelihood estimation with robust estimators of model fit (MLR), robust (Huber-White) standard errors, and a scaled test statistic that is (asymptotically) equal to the Yuan-Bentler test statistic, as it is robust against the violation of normal distribution (Rosseel, 2020). A full-information maximum-likelihood (FIML) approach was applied to compensate for missing data. At the item level, however, no missing data occurred in the computation of sum scores, as all items of the main questionnaires were mandatory in the online survey, in contrast to sociodemographic variables that were not compulsory and could therefore contain missing values.
The random intercept of each variable was identified by its observed score, with factor loadings constrained to 1. Error variances for the observed scores were constrained to zero, ensuring that all variance was captured by the latent factor structures. Model parsimony was evaluated by comparing an RI-CLPM with freely estimated stability and cross-lagged paths to one with paths constrained to be equal over time, testing whether the stability and cross-lagged effects from T1 to T2 were equivalent to those from T2 to T3. To evaluate the quality of model fits, a range of fit indices was inspected, including the comparative fit index (CFI), the Tucker Lewis Index (TLI; also called the non-normed fit index), the root-mean-square error of approximation (RMSEA), and the standardized root-mean-square residual (SRMR). In line with Hu and Bentler (1999) and Little and Kline (2016), cut-off values for good model fit were CFI >.90, TLI >.90, SRMR <.09, and RMSEA <.08. Cut-offs for excellent model fit were CFI >.95, TLI >.95, SRMR <.08, and RMSEA <.06. As common model fit indices may be biased due to the large numbers of parameters and variables, additional reliance is placed on the unbiased standardized root-mean-square error of approximation (uSRMR; Shi et al., 2018; Ximénez et al., 2022). Intraclass correlations (ICCs) were computed for all three model variables to examine the proportion of variance attributable to stable between-person differences versus within-person processes.
Transparency and Openness
The study was pre-registered prior to analyses (see https://aspredicted.org/DHR_OLH). Originally, a traditional CLPM was preregistered because only two of the three measurement points were available at time of preregistration. However, with the third measurement point available, enabling the computation of an RI-CLPM, we decided to deviate from the preregistration, given the major methodological benefits of the RI-CLPM over traditional CLPMs (Hamaker et al., 2015). Neither the model variables nor the research question on their longitudinal associations were modified.
Results
Preliminary Analyses Regarding Maternal Perceived Stress, Partner Relationship Quality, and Impaired Bonding
Mean, Standard Deviations, and t-Test Results of the Perceived Stress Scale (PSS-10), Partnership Questionnaire (PFB-K), and the Postpartum Bonding Questionnaire (PBQ-16) at the Three Measurement Times
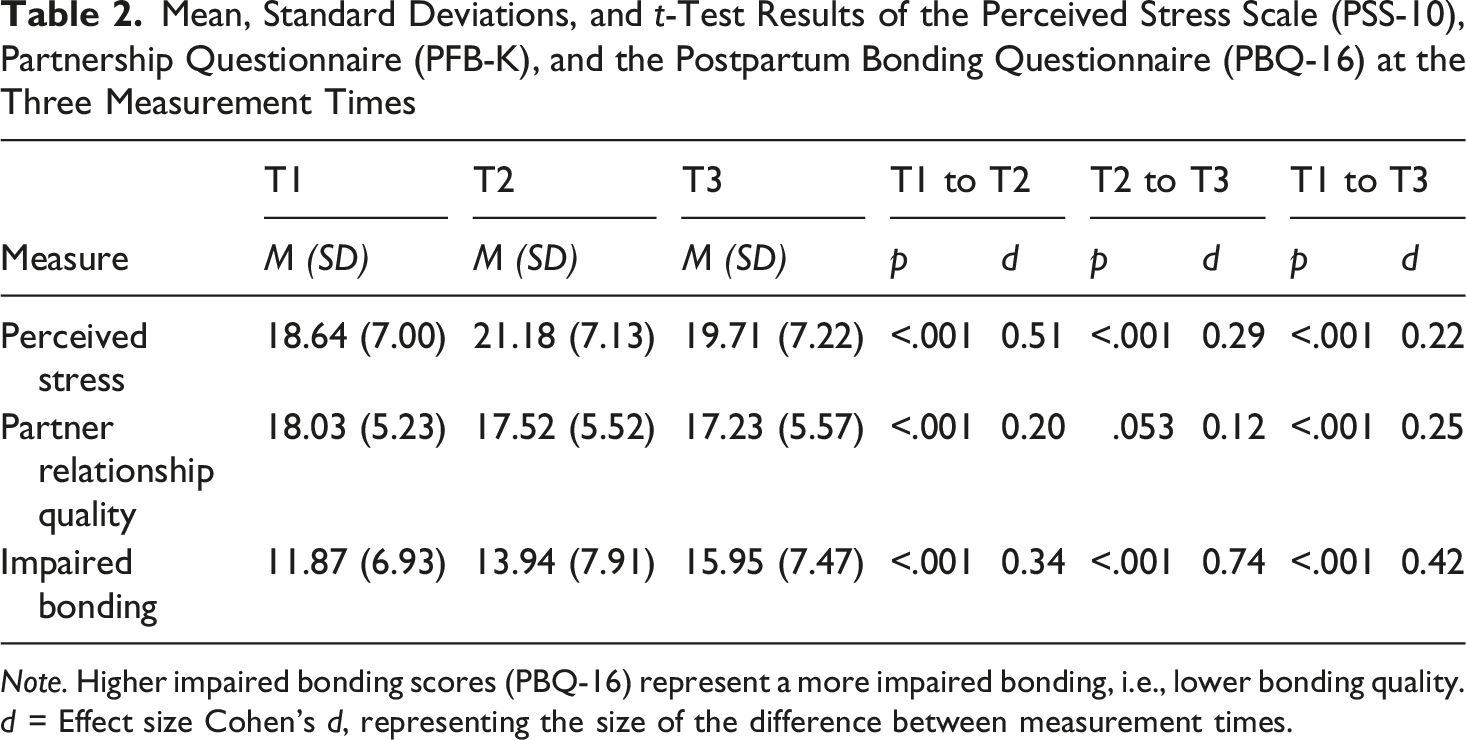
Note. Higher impaired bonding scores (PBQ-16) represent a more impaired bonding, i.e., lower bonding quality. d = Effect size Cohen’s d, representing the size of the difference between measurement times.
Pearson Correlations of Perceived Stress, Partner Relationship Quality, and Impaired Bonding at the Three Measurement Times
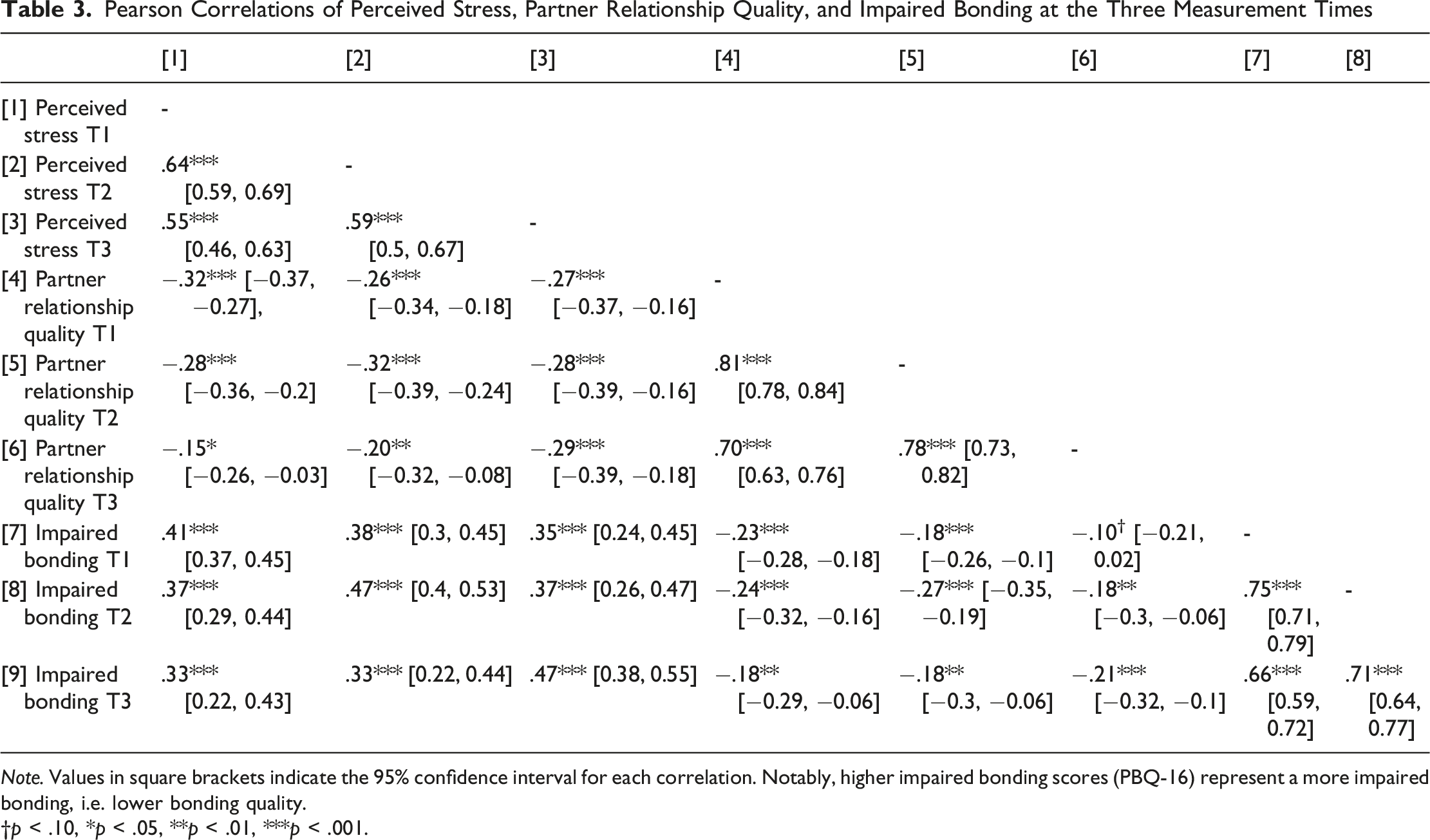
Note. Values in square brackets indicate the 95% confidence interval for each correlation. Notably, higher impaired bonding scores (PBQ-16) represent a more impaired bonding, i.e. lower bonding quality.
†p < .10, *p < .05, **p < .01, ***p < .001.
Significant Correlations Above .10 Between Main and Sociodemographic/Pandemic-Related Variables
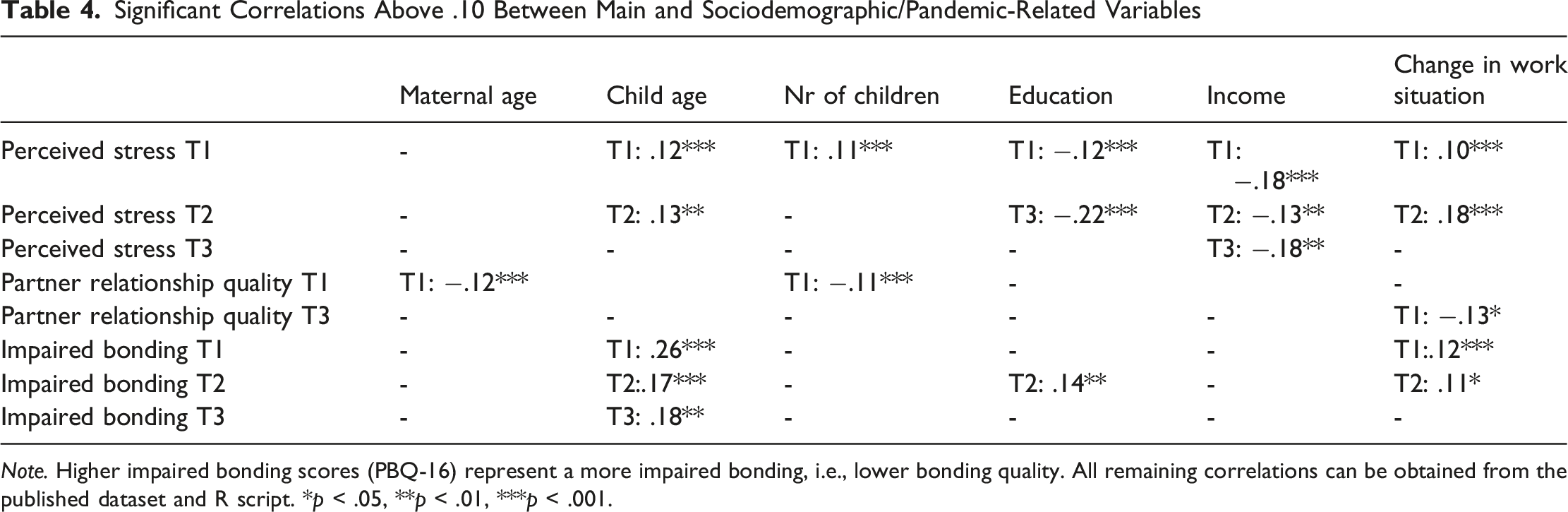
Note. Higher impaired bonding scores (PBQ-16) represent a more impaired bonding, i.e., lower bonding quality. All remaining correlations can be obtained from the published dataset and R script. *p < .05, **p < .01, ***p < .001.
Between- and Within-Person Effects Between Maternal Perceived Stress, Partner Relationship Quality, and Impaired Bonding (RI-CLPM)
First, the unconstrained RI-CLPM with freely estimated stability and cross-lagged paths was compared to a model with paths constrained to be equal over time. Both models exhibited excellent global fit according to commonly used fit indices (free model: χ
2
(3) = 2.36, p = .501 CFI = 1.000, TLI = 1.006, RMSEA = 0.000 (90% CI: 0.000-0.095), SRMR = 0.011, uSRMR = 0.011; constrained model: χ
2
(18) = 15.48, p = .629, CFI = 1.000, TLI = 1.004, RMSEA = 0.000 (90% CI: 0.000-0.044), SRMR = 0.023, uSRMR = 0.023). Model fit was evaluated using robust (scaled) χ
2
and fit indices to account for non-normality. The constrained model was retained because the equality constraints did not significantly worsen fit, Δχ2 (15) = 13.10, p = .59, and because it showed lower AIC (41,753.340 vs. 41,768.907) and BIC (41,942.516 vs. 42,036.906) values than the free model, indicating greater parsimony. Although the TLI exceeded 1 in both models – suggesting slight over-fitting – the constrained model’s TLI was closer to 1, indicating a lesser risk of overfitting. The selected constrained model with standardized coefficients is displayed in Figure 2. Note that model parameters were constrained to be time-invariant in their unstandardized form; however, the standardized coefficients varied across time points due to differences in the relative variances of the variables at each time point. Results of the random-intercept cross-lagged panel model. Outer gray area labeled “between-person differences” incorporates the random intercepts connected by non-directional paths. Inner area labeled “within-person processes” represents the interindividual changes connected by directional paths at each time point. Dashed lines indicate statistically non-significant effects, solid lines statistically significant effects. BON = impaired bonding, REL = partner relationship quality, PS = perceived stress. ***p < .001; **p < .01; *p < .05; †p < .1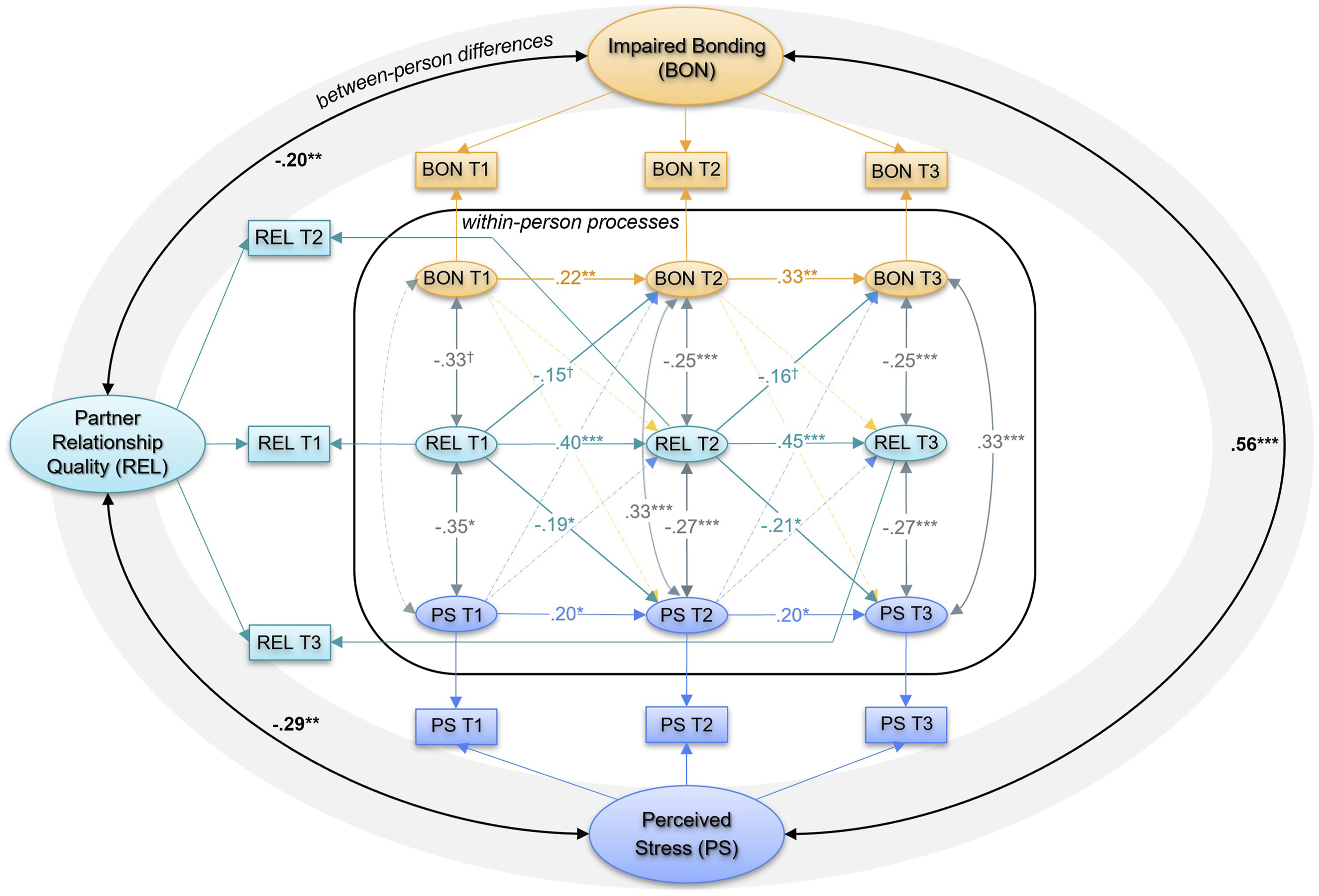
Intraclass correlations (ICCs) indicated that 50.4% of the variance in perceived stress (ICCPerceivedStress = 0.504), 66.3% of the variance in partner relationship quality (ICCRelationshipQuality = 0.663), and 77.6% of the variance in impaired bonding (ICCImpairedBonding = 0.776) were attributable to stable between-person differences. The remaining 49.6%, 33.7%, and 22.4% of the variance, respectively, reflected within-person fluctuations over time.
At the between-person level, all three random intercepts were significantly associated (see Figure 2): Mothers with generally higher relationship quality with their partner reported lower overall levels of perceived stress and impaired bonding, while higher average levels of perceived stress were linked to generally more impaired bonding.
Regarding within-person processes, autoregressive effects were significant for all three variables between all time points with standardized coefficients ranging from β = 0.20 to β = .45 (see Figure 2). Furthermore, all within-person cross-sectional correlations (range: │r│ = .18–.35) were statistically significant, except for the association between impaired bonding at T1 and both perceived stress (p = .17) and relationship quality with the partner (p = .06) at T1. These effects suggest that when relationship quality improves, perceived stress and impaired bonding decrease simultaneously, while increases in perceived stress and impaired bonding co-occur (at T2 and T3).
Most interestingly, a significant cross-lagged effect (βT1→T2 = −.19; βT2→T3 = −.21; p = .03) of perceived relationship quality with the partner on perceived stress was found, indicating that intraindividual increases in relationship quality, relative to the mother’s “typical” average or trait, predicted subsequent decreases in perceived stress. Conversely, intraindividual decreases in relationship quality were associated with subsequent increases in perceived stress (see Figure 2). Furthermore, the cross-lagged effect of perceived relationship quality on impaired bonding was marginal (βT1→T2 = −.15; βT2→T3 = −.16; p = .055), suggesting that intraindividual increases in relationship quality may predict decreases in impaired bonding, and vice versa. Based on the benchmark values provided by Orth et al. (2024), these cross-lagged effects are classified as large in magnitude (β > .12). All remaining cross-lagged effects were nonsignificant.
Finally, two robustness checks were conducted. First, comparing the model based on the full sample, including all available participants (n = 1,394), with the model based on a restricted sample, including only participants with data from at least two time points (n = 596), yielded nearly identical results and parameter estimates. The only minor difference was that the autoregressive effect of perceived stress was significant in the full sample (p = .048) but fell just below the significance threshold in the restricted sample (p = .052).
Results of the Exploratory RI-CLPM With Sociodemographic and Pandemic-Related Control Variables on the Between-Person Level
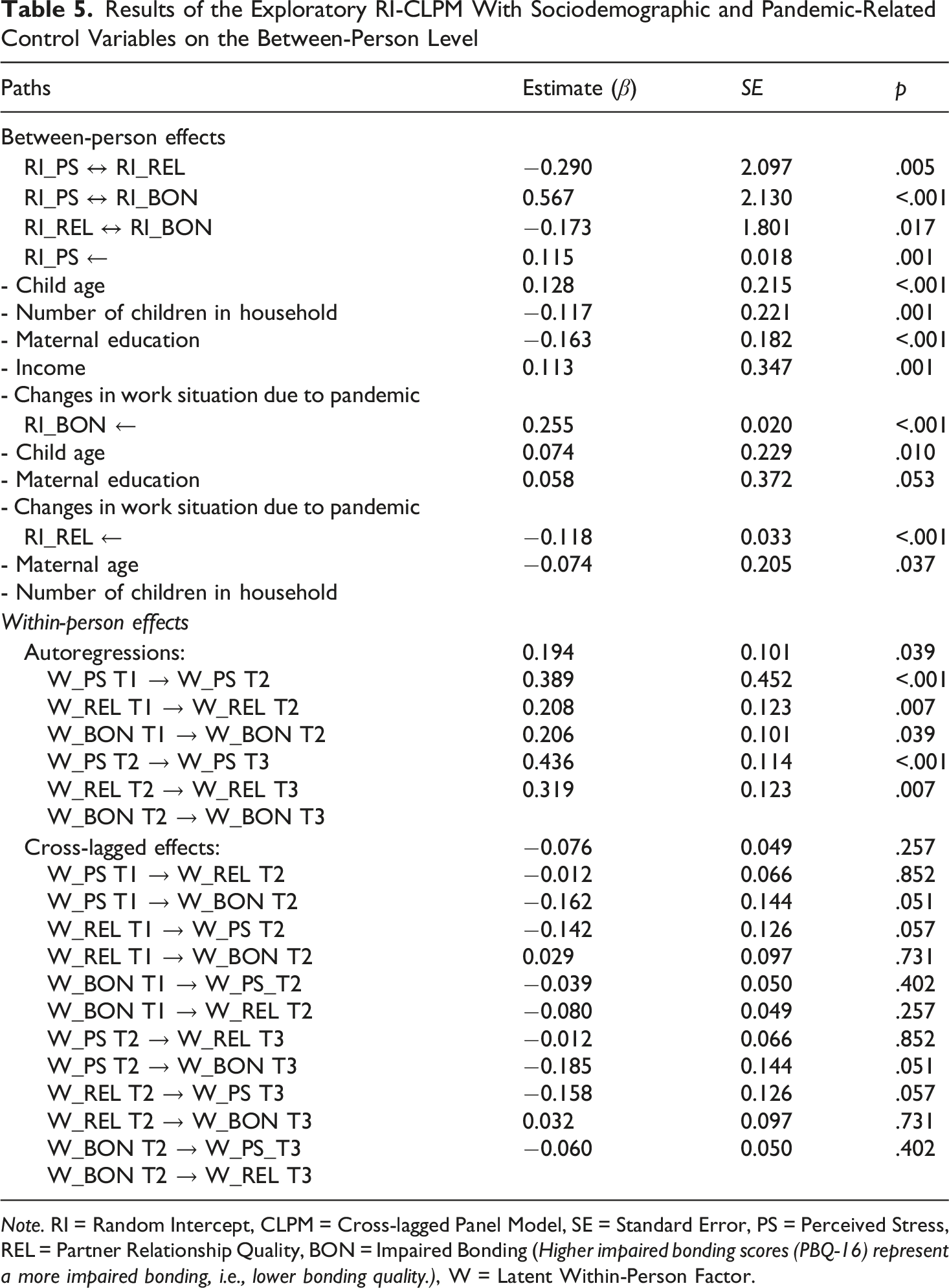
Note. RI = Random Intercept, CLPM = Cross-lagged Panel Model, SE = Standard Error, PS = Perceived Stress, REL = Partner Relationship Quality, BON = Impaired Bonding (Higher impaired bonding scores (PBQ-16) represent a more impaired bonding, i.e., lower bonding quality.), W = Latent Within-Person Factor.
Discussion
This study examined the dynamic longitudinal reciprocal relations between perceived stress, relationship quality with the partner, and impaired mother-to-child bonding in mothers with children between 0–3 years of age during the COVID-19 pandemic from May 2020 to May 2022. By applying an RI-CLPM, effects at the between- and within-person level could be separated, allowing the disentanglement of stable interindividual differences from dynamic intraindividual processes and thus providing a more precise understanding of the associations under investigation.
A significant link between all three random intercepts – describing stable between-person traits – was revealed: While perceived stress and impaired bonding were positively linked, relationship quality with the partner was negatively associated with both perceived stress and impaired bonding. At the within-person level, intraindividual increases in relationship quality predicted subsequent decreases in perceived stress. Further, trend-level evidence points to decreasing impaired bonding following increases in perceived relationship quality with the partner.
The results regarding the random intercepts indicate that mothers who, on average, experience a lower relationship quality with their partner also tended to report higher perceived stress and impaired bonding, and mothers with generally higher perceived stress typically reported more impaired bonding. Notably, these effects remained significant and almost equal in size when controlling for sociodemographic or pandemic-related factors. These results are in line with previous studies that identified associations between perceived stress, partner relationship quality, and maternal bonding before (Martin & Brock, 2023; Tolja et al., 2020) and during the COVID-19 pandemic (Mousavi et al., 2021; Overall et al., 2022; Pietromonaco & Overall, 2022; Power et al., 2024; Xie et al., 2022). Importantly, the correlations between random intercepts do not imply a temporal direction; rather, they suggest that enduring individual differences in one construct are associated with enduring individual differences in the other, possibly due to reciprocal long-term influences or shared underlying factors. While all random intercepts were significantly correlated, the correlation between those of perceived stress and impaired bonding was particularly large. At the same time, perceived stress and impaired bonding were not connected via cross-lagged paths at a within-person level. This suggests that their link is mainly rooted in the association of their stable, trait-like components, rather than in intraindividual changes, potentially reflecting enduring personal or contextual factors that influence both perceived stress and bonding.
At the within-person level, intraindividual fluctuations in mothers’ perceived relationship quality with the partner predicted fluctuations in perceived stress: On the one hand, the direction of effects indicates that increases in relationship quality predicted decreased perceived stress, suggesting a protective effect of high-quality partner relationships during the COVID-19 pandemic. On the other hand, the results can also be interpreted in reverse with intraindividual decreases in perceived relationship quality (relative to the mothers’ own typical average) being associated with subsequent increases in perceived stress. These results are in line with previous studies identifying a link between intraindividual changes in partner relationship quality and stress: In a pre-pandemic study, greater fluctuations in partner relationship quality over time were associated with poorer individual well-being (i.e., increased psychological distress and reduced life satisfaction), but not vice versa (Whitton et al., 2014). Similarly, findings from a traditional CLPM in a sample of pregnant women during the COVID-19 pandemic showed that maternal perceived partner relationship quality predicted later symptoms of depression and anxiety, whereas the reverse effects were not significant (Xie et al., 2022).
Furthermore, Pauly et al. (2022) found that changes in perceived stress and relationship quality from pre-to during the pandemic were significantly correlated with each other. However, several previous studies only investigated effects of fluctuating stress on the partner relationship without considering reciprocal effects (Rusu et al., 2020; Tepeli Temiz & Bilican, 2024). Our results, framed within a reciprocal-effects model, show that intraindividual fluctuations in relationship quality influenced subsequent perceived stress, but not the other way around. By accounting for participants’ stable levels, these findings provide important new insights into the dynamic processes unfolding during the COVID-19 pandemic. It must be noted that this effect was only marginal in the exploratory RI-CLPM that included sociodemographic control variables (p = .051). Importantly, the effect sizes remained similar in magnitude, suggesting that the shift in statistical significance was likely due to the influence of the control variables on the estimation and standard errors of the within-person paths. This is consistent with the notion that statistical significance is sensitive to model complexity, whereas the underlying substantive process appears robust. At the same time, caution is warranted, as the effect narrowly failed to reach the conventional significance threshold, raising the possibility that it may be sample-specific or less stable than suggested. Future studies are therefore needed to corroborate the robustness of these findings.
Further, the results indicated a potential effect such that when mothers reported higher (or lower) partner relationship quality than usual, this tended to predict subsequent decreases (or increases) in impaired bonding. This potential effect was only marginal (p = .055), underscoring the need for further replication in future studies. Nevertheless, this finding is in line with previous studies that found positive longitudinal associations between partner relationship quality – particularly regarding partner support – and maternal bonding, with subsequent effects on infant and child development (Cuijlits et al., 2019; de Waal et al., 2023).
These results underscore that, for mothers, the relationship with the partner functioned as a resilience or risk factor during the pandemic, not only at a stable between-person level but also in terms of within-person dynamics. In particular, fluctuations in the perceived security and quality of the relationship appear to be crucial for maternal stress levels and, potentially, for maternal bonding. In line with this, previous studies emphasize the relevance of considering both general levels and dynamic changes in couple relationship functioning during the pandemic: While couples with a generally better dyadic coping have been found to report fewer fights and less disagreement during the pandemic, initially stronger dyadic coping did not buffer against increases in conflict (Lee et al., 2022). Hence, challenges posed by the COVID-19 pandemic often increased the risk for elevated conflict even for couples with previously high relationship quality (Lee et al., 2022). Because of the distinctive difficulties presented by the pandemic, such as limited access to childcare and social support systems or changes in one’s job/financial situation, parents frequently struggled to cope with internal and external stressors as a couple (Lin et al., 2025), potentially even if their coping mechanisms had been effective in the past. This underscores the need for multifaceted support for families during crises like the COVID-19 pandemic, including structural (e.g. financial support in case of reduced income) and psychological support.
The latter is supported by results from the exploratory model in which sociodemographic and pandemic-related variables were included. The exploratory model highlights that stable individual differences in perceived stress, relationship quality with the partner, and bonding were partly shaped by demographic and pandemic-related factors (see Table 5). For perceived stress, older child age, more children in the household, and changes in the work situation due to the pandemic were associated with greater stress, whereas higher maternal education and higher income were linked to lower stress, which is in line with similar studies during the pandemic (Brown et al., 2020; Cusinato et al., 2020). For impaired bonding, older child age and higher maternal education were linked to more impaired bonding, with work changes showing only a marginal effect. However, an important limitation must be noted: the PBQ-16 was validated for children aged 0–1 year. Thus, the association with child age potentially reflects reduced validity of the PBQ-16 for older children, rather than a genuine age effect on bonding. In contrast, the association between higher maternal education and more impaired postpartum bonding appears more robust, as similar findings have been reported in previous studies as well (Dubber et al., 2015; Lehnig et al., 2019; Mazúchová et al., 2021). Finally, perceived relationship quality with the partner was negatively predicted by maternal age and the number of children in the household, indicating that older mothers and larger families reported lower relationship quality. This is in line with previous research showing that older parental age is associated with reduced relationship quality with the partner - an effect that may be partly explained by the general decline in partner relationship quality over the course of long-term relationships (Jadva et al., 2022; van Laningham et al., 2001). Likewise, a higher number of children in the household has repeatedly been linked to lower partner relationship quality, likely due to increased parenting demands, elevated stress, and diminished opportunities for couple interaction (Ahlborg et al., 2009; Saheba & Mansuri, 2020). Taken together, family structure, educational background, and economic stability appear to shape the baseline levels from which intraindividual fluctuations unfold, underscoring the importance of considering these contextual factors when interpreting stress and relational dynamics during the COVID-19 pandemic.
Overall, this study’s results suggest that couple-centered approaches strengthening the relationship with the partner are promising for preventing high maternal stress, and possibly also impaired bonding, with potential positive long-term effects for family well-being. Previous studies have demonstrated positive effects of couple-based prevention and intervention programs on the partner relationship, but also on individual and family well-being (Bradbury & Bodenmann, 2020; Kanter & Schramm, 2018; Kysely et al., 2021; Lavner et al., 2020). Based on this study’s findings in a relatively low-risk community sample with comparatively high socioeconomic status, the observed effects underscore the importance of a public health approach to relationship-focused support. It is therefore highly plausible that easily accessible large-scale interventions aimed at strengthening partner relationships may be even more critical in the general population, particularly among families with lower socioeconomic resources. First evidence for the effectiveness of brief online programs targeting different aspects of relationship quality and functioning with the partner (e.g., closeness, conflict) during the COVID-19 pandemic underscores possibilities for cost-effective, low-threshold programs during such crises (Prime et al., 2024; Rodriguez et al., 2021; Tsai et al., 2020).
In terms of strengths and limitations, to the best of the authors’ knowledge, this was the first study to examine longitudinal reciprocal effects among perceived stress, perceived relationship quality with the partner, and impaired bonding in mothers during the COVID-19 pandemic. In addition, the large sample size and longitudinal design enabled the use of advanced statistical modeling separating between-person differences and within-person processes. Regarding limitations, the high dropout rate in this study must be considered. However, comprehensive attrition analyses and robustness checks indicated very few significant differences with negligible to small effect sizes regarding the main variables and sociodemographics, suggesting that dropout is unlikely to have introduced bias into our results. Model indices further indicated near-perfect fit, raising over-fitting concerns and calling for replication with lower dropout rates or more parsimonious models. Another limitation of this study is that it was conducted in a relatively low-risk sample with predominantly higher socioeconomic status, which may restrict the generalizability of the findings to more socioeconomically diverse populations. Moreover, we did not collect data on participants’ ethnicity, which represents an additional limitation and potential source of bias. In addition, the measure used to assess maternal bonding (PBQ-16) has not been validated for toddlers and preschool-aged children and should therefore be regarded as a proxy to assess the mother-child relationship; however, child age was included as a control variable in an exploratory model, which did not alter the main results. Furthermore, this study relied exclusively on maternal reports, as only a very small number of fathers or other primary caregivers participated in the survey. This reliance on a single informant may have introduced a single-informant bias into our results. Future studies would benefit from recruiting more fathers and other caregivers, as well as including further data sources, such as observations of parent-child or parental interaction, and ecological momentary assessments.
Conclusion
This study’s results underscore the interrelation of maternal perceived stress, perceived relationship quality with the partner, and mother-to-child bonding, and highlight the dynamic relevance of the relationship quality with the partner as a risk or resilience factor for maternal stress and, potentially, for bonding during the COVID-19 pandemic. These processes, however, do not occur in isolation: Sociodemographic factors such as maternal education, income, family size, and pandemic-related work changes significantly shaped baseline levels of stress and relational functioning. Consequently, support services should focus on strengthening the relationship with the partner early and tailor interventions to families’ structural contexts to mitigate stress, promote bonding, and prevent long-term adverse effects on maternal and child well-being.
Footnotes
Acknowledgements
We would like to thank all volunteers who participated in the online survey and all colleagues who contributed to this study.
Ethical Considerations
The study was approved by the ethics committee of the medical faculty, Ruprecht-Karls-University, Heidelberg, in agreement with the Ludwig Maximilian University, Munich (vote: S-446/2017). Written informed consent was obtained from participants to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Mannheim’s Graduate School of Economic and Social Sciences, Center for Doctoral Studies in Social and Behavioral Sciences (CDSS).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets, analysis scripts, and study materials are openly available in the PsychArchives repository at https://doi.org/10.23668/psycharchives.22158, ![]() and https://doi.org/10.23668/psycharchives.22159, Woll and Stürmlinger (2026).
and https://doi.org/10.23668/psycharchives.22159, Woll and Stürmlinger (2026).