
Abstract
Romantic relationships and socioeconomic resources are both well-established predictors of health and wellbeing, yet their effects have not often been examined simultaneously as primary predictors. This study investigated the relative contributions of relationship quality and socioeconomic status (SES) to life satisfaction, physical health, and mental health across two national contexts that differ in social structure and welfare systems. Demographically stratified national samples from the United States (n = 1,004) and Spain (n = 969) completed measures of relationship satisfaction, perceived partner responsiveness, and multiple SES indicators. Linear regression analyses showed that higher levels of relationship satisfaction and perceived partner responsiveness were robustly associated with greater life satisfaction, better physical health, and fewer mental health symptoms in both countries, even after accounting for SES. Subjective SES also predicted all outcomes in both countries, above and beyond the effects of relationship quality. However, objective SES indicators showed country-specific patterns: education consistently predicted outcomes in the U.S. but not in Spain, and income predicted some outcomes in the U.S., but effects were weaker and less consistent than for education. Together, these findings show that relationship quality is a robust predictor of health and wellbeing across contexts, whereas the impact of socioeconomic status seems to depend on the broader structural environments.
Keywords
A large body of research demonstrates that both romantic relationships and socioeconomic resources are central to health and wellbeing. High-quality, supportive relationships are associated with better physical and mental health, lower mortality risk, and greater life satisfaction (Cohen, 2004; Holt-Lunstad et al., 2010; Robles et al., 2014), while higher socioeconomic status (SES) is also associated with better psychological wellbeing and reduced risk of physical illness and premature death (Chen & Miller, 2007; Lorant et al., 2003; Tan, Kraus, Carpenter, & Adler, 2020). Despite these well-established associations, the two literatures have largely developed in parallel rather than in an integrated manner. Although many relationship studies include SES as a covariate, fewer treat both domains as primary, independent predictors, and relationship processes are often absent from broader research on the social determinants of health. As a result, relatively few studies have directly examined their simultaneous contributions, leaving open questions about their relative importance and whether the benefits of satisfying relationships persist once socioeconomic resources are taken into account. The present study addresses this gap by simultaneously examining relationship quality and SES as predictors of health and wellbeing, using demographically stratified national samples from Spain and the United States to test whether these associations generalize across distinct sociocultural contexts.
Social relationships play a pivotal role in determining health outcomes. Meta-analytic reviews have found that individuals with strong and supportive relationships report better subjective health (r = .16) and lower mortality risk (r = .11), effects comparable to those of many health behaviors such as exercise or diet (Holt-Lunstad et al., 2010; Robles et al., 2014). At the physiological level, a large body of evidence indicates that greater relationship quality is linked to more adaptive physiological functioning, including lower systemic inflammation, enhanced autonomic regulation, attenuated cardiovascular reactivity, and faster recovery from illness (Donoho et al., 2015; Kulik & Mahler, 2006; Shrout et al., 2021; Skiba et al., 2023).
The impact of relationships extends even more strongly to mental health and psychological wellbeing. Individuals in more satisfying marriages report higher overall life satisfaction and greater daily wellbeing, as well as lower depression and anxiety (Carr et al., 2014; Postler et al., 2022; Rehman et al., 2008). Meta-analyses confirm robust associations, with marital quality reliably associated with lower depression (r = .37 - .42; Whisman, 2001), greater psychological wellbeing (r = .25 - 37; Proulx et al., 2007), and greater life satisfaction (r = .46; Aksu et al., 2023). Together, this evidence underscores the broad health and wellbeing benefits of high-quality romantic relationships.
Importantly, most of this evidence relies on broad indicators of relationship quality, such as relationship satisfaction or marital quality, which capture individuals’ global evaluations of their relationship. Although these measures are robust predictors of health, they provide limited insight into the interpersonal processes through which these effects emerge. One process that has been identified as a central mechanism linking close relationships to both psychological and physiological outcomes is perceived partner responsiveness (PPR), which is the extent to which individuals feel understood, validated, and cared for by their partner (Reis et al., 2004; Selcuk et al., 2016, 2017). Higher perceived responsiveness is associated with greater daily positive affect, lower stress reactivity, and better long-term mental and physical health, in part because it fosters feelings of security and belonging that support adaptive emotional and physiological regulation (Alonso-Ferres et al., 2020; Slatcher & Selcuk, 2017).
Accordingly, the present study focuses on two complementary indicators of relationship quality: relationship satisfaction and perceived partner responsiveness. Relationship satisfaction reflects individuals’ global evaluations of their relationship, whereas perceived responsiveness captures a key interpersonal process underlying these evaluations. Together, these constructs provide a more comprehensive assessment of how close relationships contribute to health.
Importantly, these relational processes do not operate in isolation but are embedded within broader social contexts that also shape health and wellbeing. In this regard, a parallel body of research has established the critical role of SES in shaping health. Both objective indicators (income, education) and subjective perceptions of social standing predict health outcomes across the lifespan. Meta-analyses demonstrate that lower SES is associated with higher levels of inflammation (r = .12 - .15; Muscatell et al., 2020), hypertension (r = .05 - .19; Leng et al., 2015), and poorer general physical health (r = .11; Cundiff & Matthews, 2017). SES disparities also extend to psychological outcomes, with higher SES linked to greater subjective wellbeing (r = .16 - .22; Tan, Kraus, Carpenter, & Adler, 2020), and lower incidence of depression (Lorant et al., 2003).
Despite strong evidence in both domains, important questions remain about how relationship quality and socioeconomic status jointly shape health. Although some studies include SES as a control variable when examining relationship processes, relatively few have directly tested whether relationship quality predicts health above and beyond SES or compared the relative strength of these domains within the same models. As a result, it remains unclear whether the benefits of high-quality relationships reflect independent effects or are partly explained by socioeconomic differences (Robles et al., 2014). Conversely, research examining the impact of SES on health seldom considers the quality of romantic relationships (Umberson et al., 2010). Integrating these lines of work is also theoretically important, as recent models emphasize that understanding how relationships shape health requires attention to the broader sociocultural and structural contexts in which they occur (Shrout et al., 2024; Slatcher & Selcuk, 2017). A small number of recent studies have begun to bridge this divide, suggesting that relationship processes may mitigate socioeconomic disadvantage and that relational advantages may persist across socioeconomic strata (Mäki et al., 2025; Tan, Kraus, Impett, & Keltner, 2020). Yet, this small body of research focuses primarily on moderation rather than examining whether relationship quality and SES independently contribute to health and wellbeing. Overall, the siloed approach to examining these two important determinants of health leaves open a critical question: are the health benefits of romantic relationships robust after accounting for socioeconomic resources, or do they reflect confounding by SES? Clarifying this issue is especially important in light of growing policy attention to social connection and poverty as determinants of health (e.g., Murthy, 2023; OECD, 2023a).
Cross-national comparisons provide an additional opportunity to test the generalizability of these effects. Macro-level contexts such as healthcare systems, income inequality, and labor markets may shape the extent to which socioeconomic resources translate into health outcomes. Spain and the United States offer a particularly informative contrast. Both countries are high-income democracies with pronounced income inequality, but they differ markedly in healthcare provision. In the U.S., access to healthcare and related benefits is often tied to employment and education, whereas Spain provides universal healthcare with relatively low and standardized costs (OECD, 2023b). These structural differences suggest that the health advantages of higher SES may be amplified in the U.S. but attenuated in Spain, where access to basic healthcare is not dependent on socioeconomic resources. Comparing these contexts makes it possible to test whether the links between relationship quality, socioeconomic resources, and wellbeing reflect general processes or vary with the broader structural conditions that shape daily life.
The present study addresses this gap by examining the relative contributions of romantic relationship quality and socioeconomic resources to health and wellbeing in large national samples from Spain and the United States recruited using demographic quotas. Specifically, we examine whether relationship satisfaction (a global evaluation) and perceived partner responsiveness (a core interpersonal process) predict life satisfaction, physical health, and mental health symptoms above and beyond income, education, and subjective SES, and whether these associations differ across national contexts. Based on prior research linking high-quality romantic relationships to better health and wellbeing, we hypothesized that higher relationship satisfaction and greater perceived partner responsiveness would be associated with greater life satisfaction, better physical health, and fewer mental health symptoms. We also expected socioeconomic resources (income, education, and subjective SES) to be positively associated with health and wellbeing outcomes. However, given limited prior work directly comparing these domains, we did not make a priori predictions about whether relationship quality or socioeconomic resources would emerge as stronger predictors of health and wellbeing. We also did not make a priori hypotheses about how the relative strength of these associations would differ across countries.
Method
Transparency and Openness
Below we describe how we determined our sample size, all data exclusions, and all measures relevant to the current study. This study was preregistered: the preregistration is available at https://aspredicted.org/czjv-bn3m.pdf. Research materials, analysis code, and data are available at https://osf.io/h8be2. This study was approved by the Institutional Review Boards at the University of Texas at Austin and the University of Granada.
Procedure and Participants
Participants in the United States (n = 1,004) were recruited via the research panel provider Dynata during April and May 2024. Dynata maintains a large panel of individuals who have previously registered to participate in survey research and who receive invitations to studies based on demographic eligibility criteria. Panel members are recruited through a variety of online channels (e.g., websites, mobile applications, and digital advertising) and are compensated through the panel provider’s incentive system. The sample was stratified using quotas based on gender, race, and age to mirror the distribution of the U.S. population. Eligibility requirements included being at least 18 years old and being part of a romantic relationship that was at least 6 months in duration. Participants were compensated the equivalent of $7.50 through the panel provider’s incentive system.
Demographics of U.S. Sample
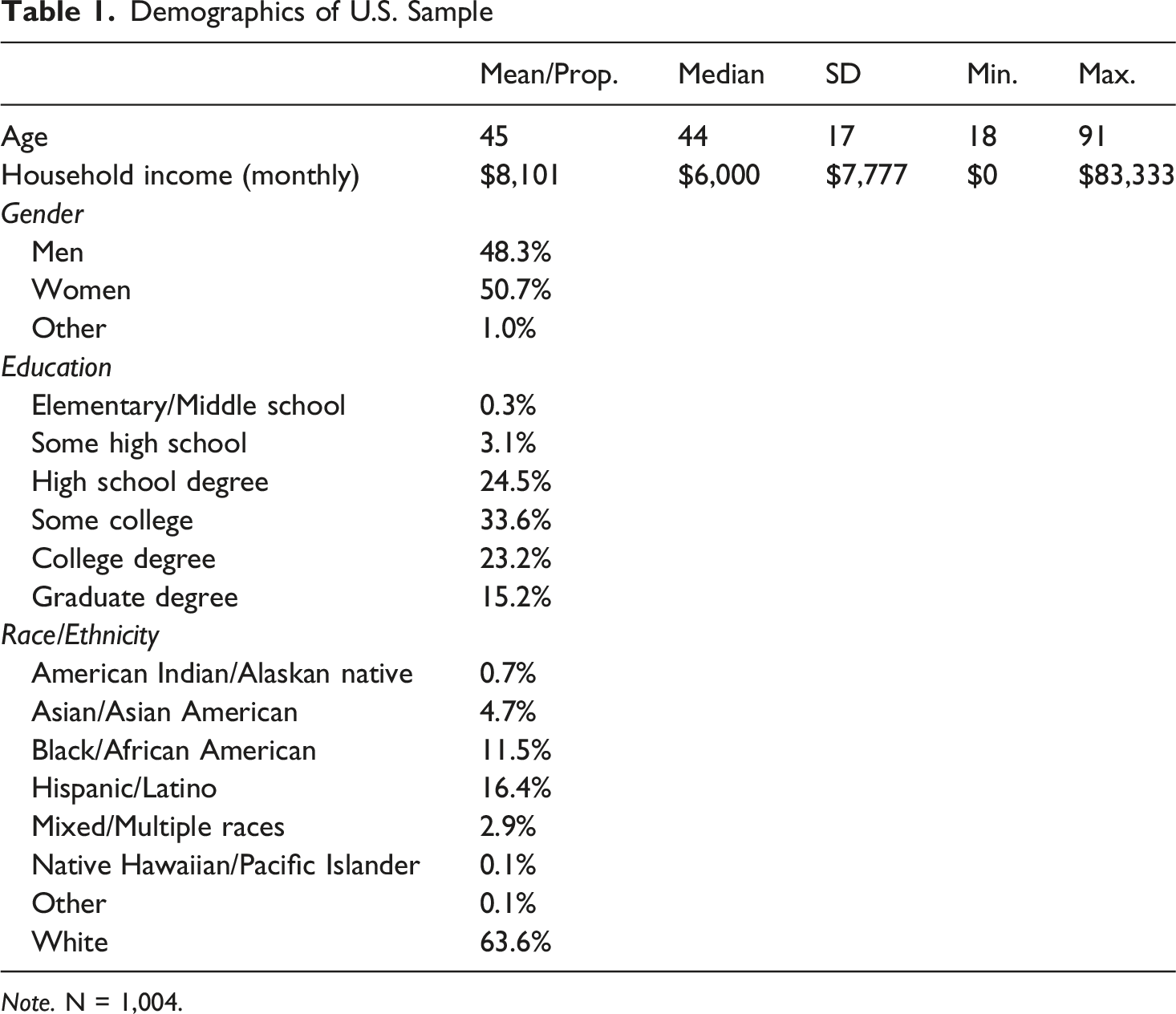
Note. N = 1,004.
Participants in Spain (n = 969) were recruited via the research panel provider NetQuest during May and June 2023. NetQuest maintains a large panel of individuals in Spain who have registered to participate in survey research and who are invited to studies based on demographic eligibility criteria. Panel members are typically recruited through online advertising and partner websites and receive compensation through the panel provider’s incentive system. The sample was stratified using quotas based on gender, age, social class, and region of residence to mirror the distribution of the Spanish population. Eligibility requirements for the survey included being at least 18 years old, and only those who were part of a romantic relationship were included in the analytic sample. Upon completion, participants were compensated through the panel provider’s inventive system.
Demographics of Spain Sample
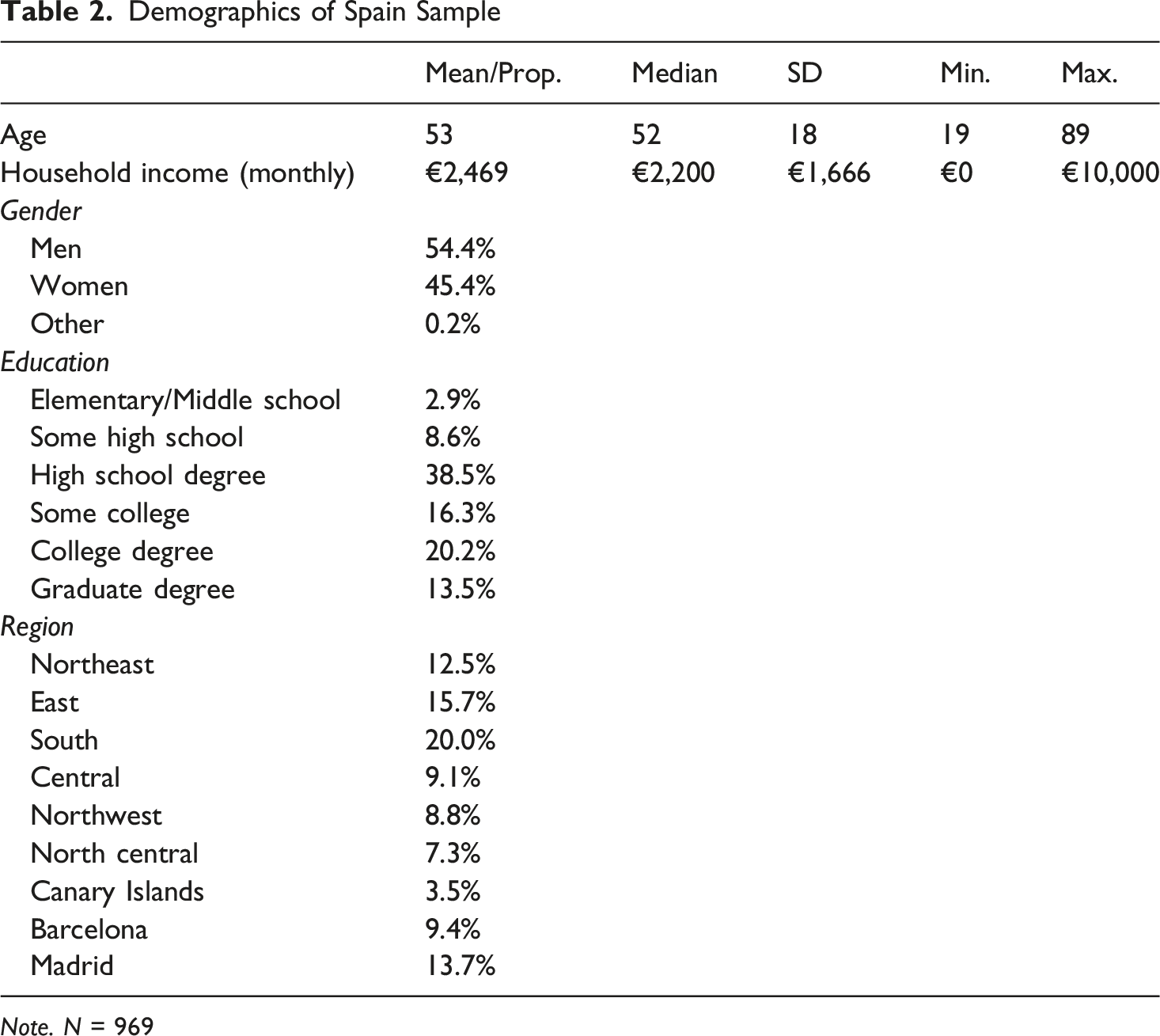
Note. N = 969
Measures
Analytic Plan
A series of linear regression models were used to examine the associations between relationship quality (relationship satisfaction and perceived partner responsiveness), socioeconomic status (income, education, and subjective social class) and the three indicators of health and wellbeing: life satisfaction, mental health symptoms, and physical health. The three socioeconomic indicators were only modestly correlated (all rs < .30) so they were entered into the same model simultaneously. However, the two relationship quality indicators were highly correlated (r = .84) so they were tested in separate models. We first examined the main effects of relationship quality and socioeconomic status on the DVs. Next, we tested whether country was a significant moderator of the associations between the IVs and DVs by adding interaction terms between country and each predictor. Finally, for significant interaction terms, we examined the simple slopes by country to understand the nature of the association between relationship quality, socioeconomic status, and health/wellbeing within each country.
Results
Descriptive Statistics
Means, SDs, and Inter-correlations for all Variables
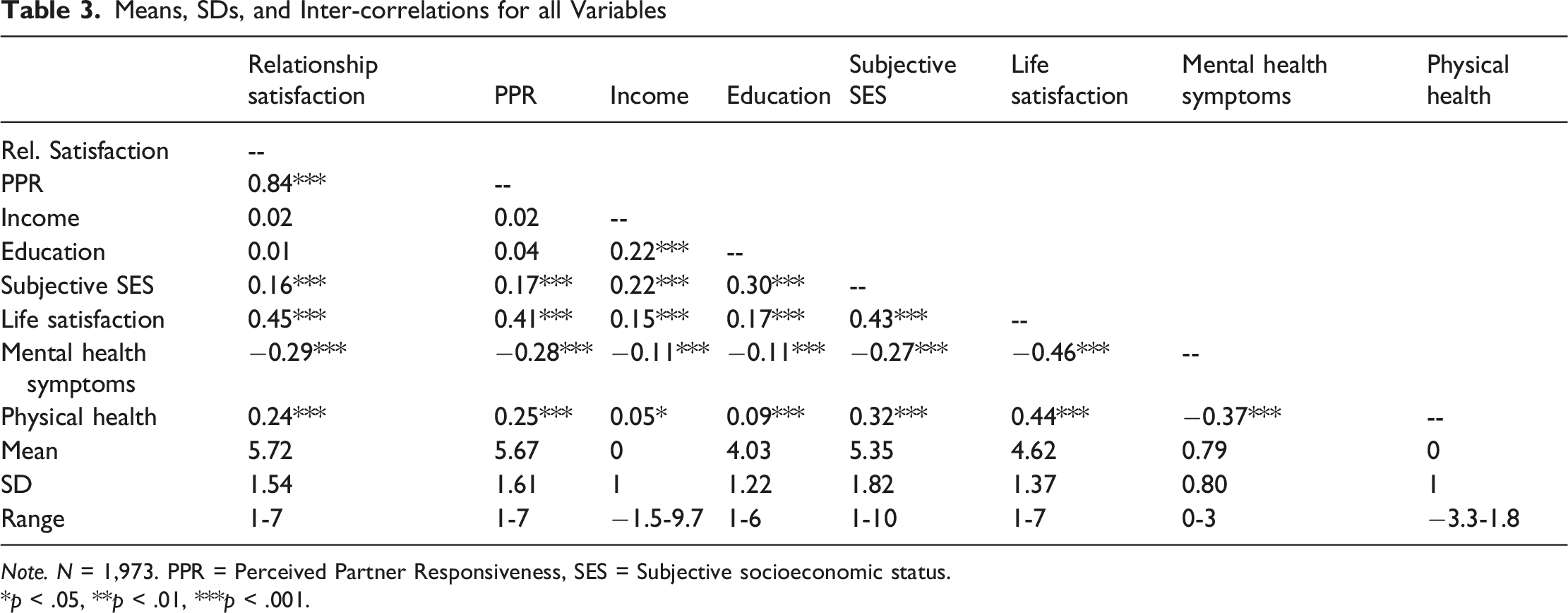
Note. N = 1,973. PPR = Perceived Partner Responsiveness, SES = Subjective socioeconomic status.
*p < .05, **p < .01, ***p < .001.
Results for Life Satisfaction
Regression Models With Relationship Satisfaction and Socioeconomic Status
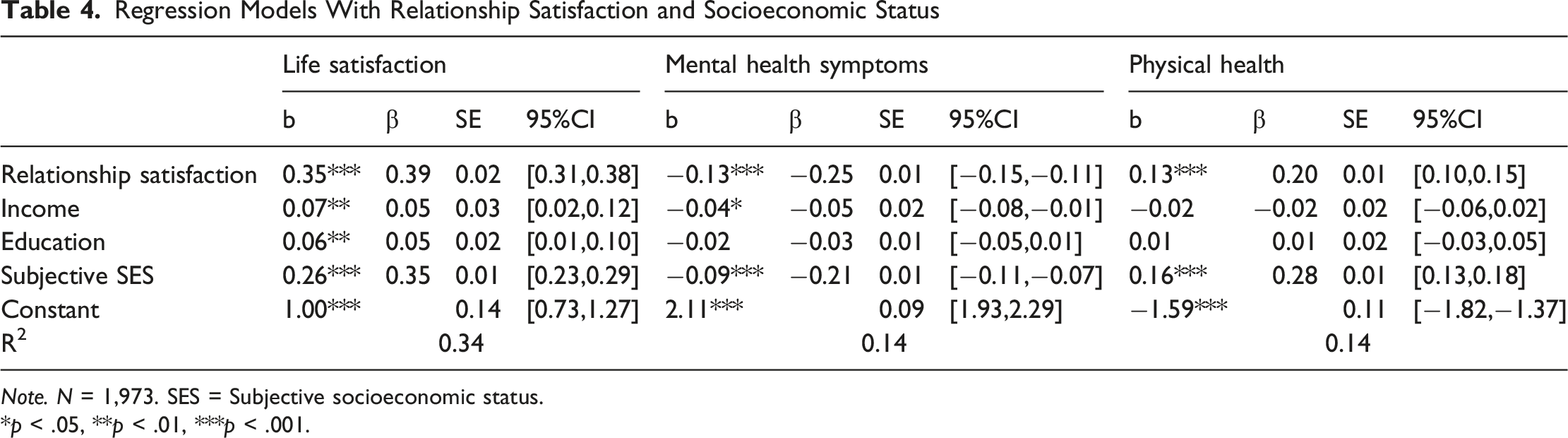
Note. N = 1,973. SES = Subjective socioeconomic status.
*p < .05, **p < .01, ***p < .001.
Regression Models With Country as a Moderator of Relationship Satisfaction and Socioeconomic Status
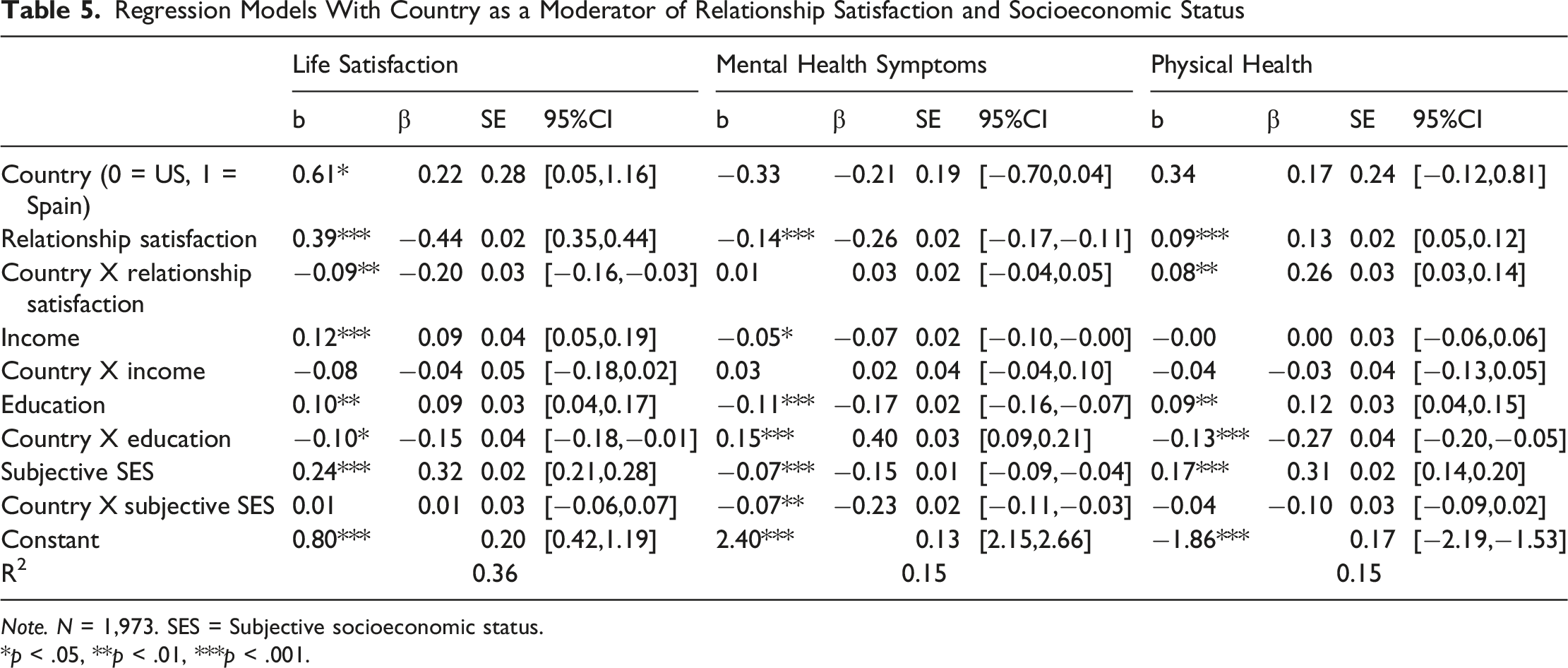
Note. N = 1,973. SES = Subjective socioeconomic status.
*p < .05, **p < .01, ***p < .001.
Regression Models With Perceived Partner Responsiveness and Socioeconomic Status
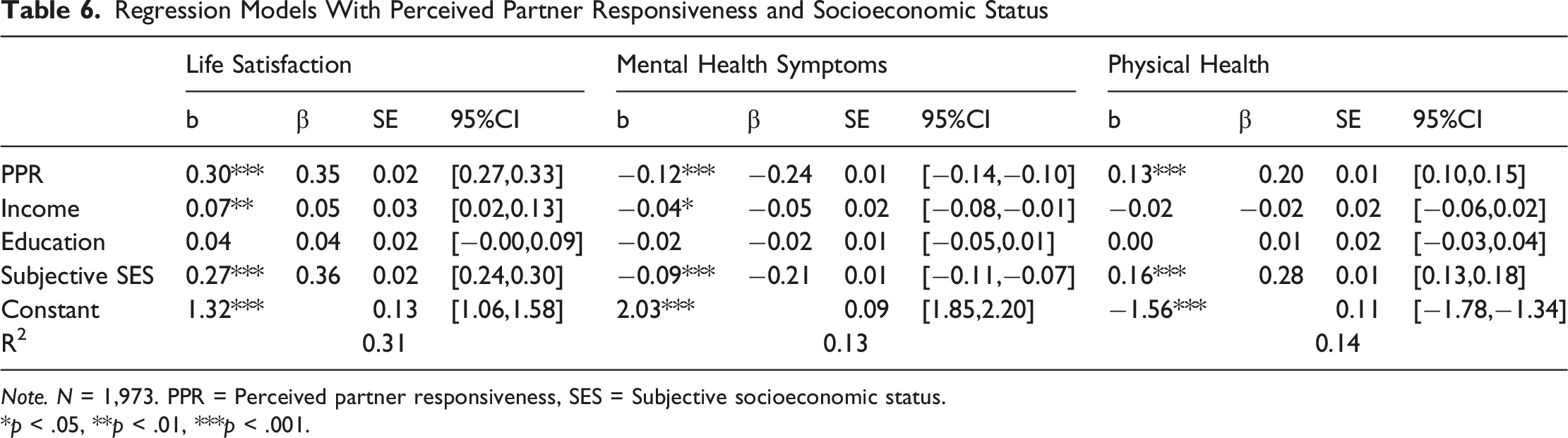
Note. N = 1,973. PPR = Perceived partner responsiveness, SES = Subjective socioeconomic status.
*p < .05, **p < .01, ***p < .001.
Regression Models With Country as a Moderator of Perceived Partner Responsiveness and Socioeconomic Status
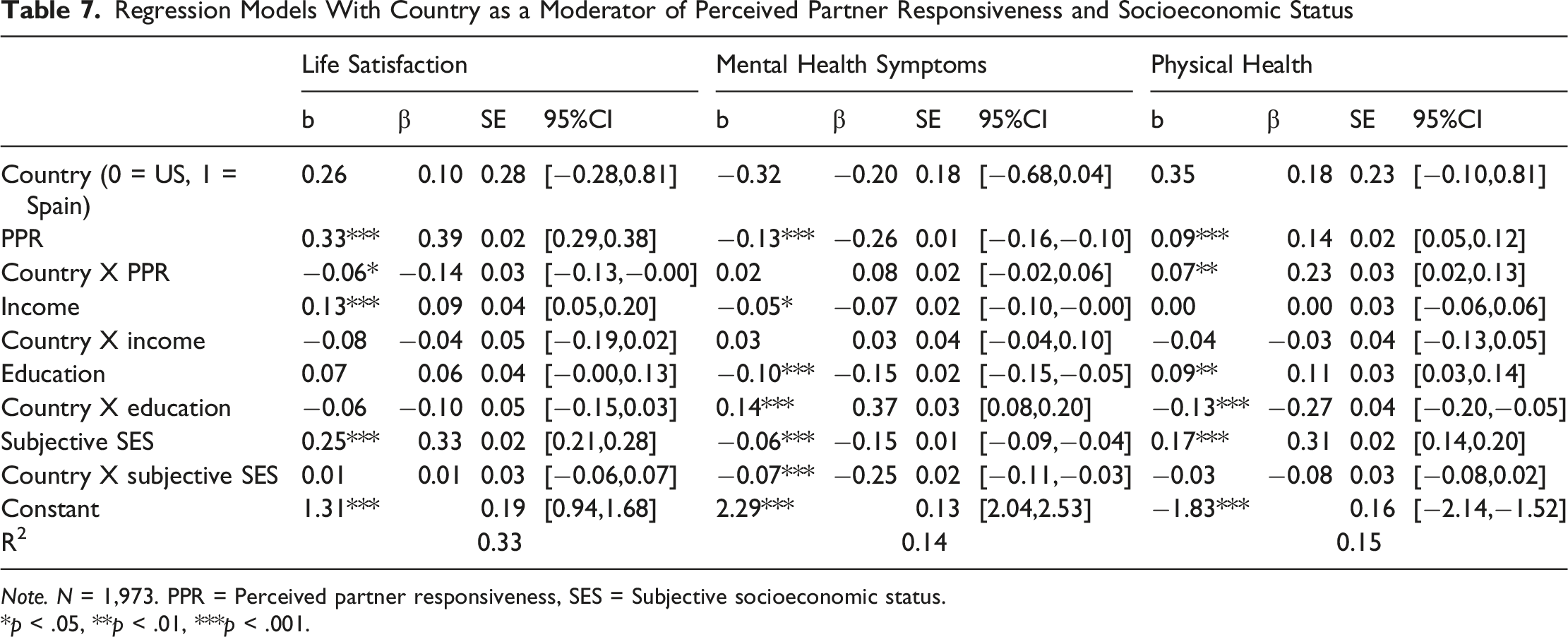
Note. N = 1,973. PPR = Perceived partner responsiveness, SES = Subjective socioeconomic status.
*p < .05, **p < .01, ***p < .001.
Results for Mental Health Symptoms
Results for Physical Health
Robustness Check
Supplementary analyses including age and gender as covariates yielded substantively identical results. The pattern and significance of both the main effects and country moderation effects remained unchanged when these variables were included in the models. Full results for these models are reported in Tables S1–S4 in the online supplement.
Discussion
The present study examined the relative contributions of romantic relationships and socioeconomic resources to health and wellbeing in large national samples from Spain and the United States recruited using demographic quotas. Across both countries, we found robust evidence that relationship quality (indexed by relationship satisfaction and perceived partner responsiveness) was significantly associated with higher life satisfaction, better physical health, and fewer mental health symptoms. Importantly, these associations held even when socioeconomic indicators were included in the models, underscoring that the health benefits of high-quality romantic relationships operate above and beyond socioeconomic resources. At the same time, socioeconomic status, particularly subjective SES, emerged as an independent and consistent predictor of health and wellbeing. Finally, objective SES indicators such as education showed stronger associations in the U.S. than in Spain, highlighting the role of macro-level structural factors in shaping the SES-health link.
These findings reinforce a large body of evidence linking relationship quality to health. Prior research has consistently shown that supportive relationships predict better physical health outcomes, lower risk of morbidity and mortality, and enhanced psychological wellbeing (e.g., Cohen, 2004; Holt-Lunstad et al., 2010; Proulx et al., 2007; Robles et al., 2014). Perceived partner responsiveness in particular has been identified as a robust predictor of both daily affect and long-term health (Selcuk et al., 2016, 2017), and our results confirm its central role in large national samples drawn from two distinct cultural contexts. By demonstrating that these associations remain significant after accounting for both objective and subjective SES, the present study strengthens the case that satisfying close relationships constitute an independent social determinant of health.
At the same time, our findings highlight the parallel and powerful role of socioeconomic resources. Consistent with prior meta-analytic evidence, higher subjective SES predicted greater life satisfaction and better mental and physical health (Cundiff & Matthews, 2017; Muscatell et al., 2020; Tan, Kraus, Carpenter, & Adler, 2020). Importantly, subjective SES has been argued to capture not only material resources but also relative social standing, perceived control, and psychosocial stress, which may explain its robust associations with wellbeing across both Spain and the U.S. (Adler et al., 2000; Navarro-Carrillo et al., 2020). In contrast, objective SES indicators revealed cross-national differences: education was a strong predictor of life satisfaction, physical health, and mental health in the U.S., but showed little to no association in Spain.
One plausible explanation for these cross-country differences lies in macro-level structural contexts. In the U.S., education and employment are strongly tied to access to healthcare and health insurance, retirement benefits, and job stability, all of which contribute to health disparities (Montez & Friedman, 2015; Ross & Mirowsky, 2010). People with lower levels of education are more likely to hold part-time or precarious jobs that lack benefits, leaving them vulnerable to gaps in healthcare coverage and financial stress. By contrast, in Spain healthcare is provided universally, with relatively low and uniform costs across the population (OECD, 2023b). This system may attenuate the health advantages of higher education, producing weaker associations between objective SES and health outcomes. Importantly, however, life satisfaction is not fully explained by healthcare access alone, which may explain why some education effects were observed for wellbeing in the U.S. but not Spain. Notably, subjective perceptions of SES remain highly relevant in both contexts, pointing to the psychological and social dimensions of social stratification that operate above and beyond objective resources. Furthermore, cultural factors may interact with these structural differences: in more individualistic contexts like the U.S., education and employment may carry additional social and psychological value, whereas in more collectivist contexts such as Spain, social integration and relational support may play a larger role in wellbeing outcomes.
Taken together, these results underscore that romantic relationships and socioeconomic resources represent partially independent pathways to health and wellbeing. Romantic relationships likely exert effects through psychological and biological mechanisms, including stress buffering, reduced allostatic load, enhanced immune functioning, and increased engagement in health-promoting behaviors (Robles & Kiecolt-Glaser, 2003; Uchino, 2006). Socioeconomic resources, in contrast, influence health through access to material resources, healthcare, occupational opportunities, and reduced exposure to chronic stressors such as financial strain and neighborhood disadvantage (Chen & Miller, 2012; Matthews & Gallo, 2011). Our findings suggest that both pathways are important and that policies or interventions targeting only one domain are unlikely to fully close gaps in health and wellbeing.
Several limitations warrant consideration. First, the data are cross-sectional, preventing conclusions about causal direction. Although longitudinal evidence supports bidirectional associations between relationships, SES, and health (e.g., Gallo & Matthews, 2003; Umberson et al., 2010), future studies should use longitudinal and experimental designs to more clearly identify causal mechanisms. Second, several constructs were measured with single items, particularly the relationship quality indicators. While single-item measures were used to reduce fatigue and minimize participant attrition (Bolger et al., 2003), and have demonstrated reliability and predictive validity in large-scale surveys (Niehuis et al., 2024), multi-item measures may enhance robustness of the results. Third, all measures were self-reported, which may introduce bias due to shared method variance or cultural differences in response styles. Fourth, while our cross-national design strengthens generalizability, comparable demographic information was not collected across both samples; specifically, sexual orientation, relationship status, relationship duration, cohabitation status, and race/ethnicity were not assessed in the Spanish sample, and disability status was not assessed in either sample, precluding our ability to fully characterize and compare the demographic composition of the two sample. Finally, the cross-national design cannot isolate specific macro-level mechanisms underlying observed differences. For example, we have hypothesized that healthcare access likely explains weaker education effects in Spain, but other cultural or institutional differences across countries may also play a role.
Despite these limitations, the present study contributes to ongoing debates about the determinants of health and wellbeing. By showing that close relationships predict health outcomes above and beyond socioeconomic resources, our findings align with recent calls to prioritize social connection as a public health issue (Murthy, 2023). At the same time, cross-national differences in the strength of SES effects underscore the importance of structural contexts in shaping health disparities. Future research should investigate mechanisms underlying these associations, examine additional countries with different welfare and healthcare systems, and test whether interventions targeting both relationship quality and socioeconomic resources can produce synergistic benefits for population health. Additionally, identifying the conditions under which relational and socioeconomic resources interact could inform more targeted interventions, particularly for populations at elevated risk due to economic disadvantage or social isolation.
In sum, this study demonstrates that both romantic relationships and socioeconomic resources are vital predictors of health and wellbeing. High-quality relationships confer benefits across physical, psychological, and subjective wellbeing domains, even after accounting for socioeconomic resources, while subjective SES remains a powerful and consistent predictor. Cross-national comparisons between Spain and the United States further reveal that structural contexts, such as healthcare systems, may shape the extent to which socioeconomic resources translate into health. These findings highlight the need for integrated approaches that address both interpersonal and structural determinants in order to improve health and wellbeing at the population level.
Supplemental material
Supplemental material - Romantic Relationships and Socioeconomic Status as Independent Predictors of Health and Wellbeing: Evidence from the United States and Spain
Supplemental material for Romantic Relationships and Socioeconomic Status as Independent Predictors of Health and Wellbeing: Evidence from the United States and Spain by Inmaculada Valor-Segura, María Alonso-Ferres, and Hannah C. Williamson in Journal of Social and Personal Relationships.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Texas Global Faculty Research Seed Grant and a Fulbright Scholar Award awarded to Hannah Williamson, and grant P2CHD042849 awarded to the Population Research Center at the University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Data collection in Spain was supported by the financing provided by the Spanish Ministry of Economy, Industry and Competitiveness [Ref. PID2020-114464RB-I00 (MINECO/AEI/FEDER/UE)] and preparation of this manuscript was supported by the Plan Propio de Investigación y Transferencia of the University of Granada (Ref. PP2025.PP.22) awarded to Inmaculada Valor-Segura. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Fulbright Program, the Government of the United States, or the Fulbright Spain Commission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data, materials, and analysis code are available at https://osf.io/h8be2. This study was preregistered: the preregistration is available at ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.