
Abstract
This pilot study explored the potential for Project ASPIRE to effect behavior change in a sample of 11 parents of children with hearing loss who were from typically underserved populations, such as families from backgrounds of low socioeconomic status or families who speak English as a second language. The study consisted of one education session, five 16-hour home audio environment recordings, and four linguistic feedback reviews. The educational session focused on child language development and early language environment enrichment strategies. Parents received ‘quantitative linguistic feedback’ on the home audio recordings to further support behavior change through increased awareness of linguistic behaviors. The audio recordings were completed with the Language ENvironment Analysis system. This system measured parental linguistic behavior (adult word count or AWC), child linguistic behavior (child vocalization count or CVC), and child–parent interactive linguistic behavior (conversational turn count or CTC). Post-intervention both CTC and CVC had increased significantly compared to pre-intervention recording counts (p < 0.01; p < 0.05). Increase in AWC trended towards significance between pre- and post-intervention recordings (p < 0.1). These preliminary findings support ‘quantitative linguistic feedback’ as a viable behavior change strategy for enriching children’s early language environments through parental linguistic behaviors.
I Introduction
For children with hearing loss, early auditory access – through cochlear implantation or hearing aids – is a vital first step in the development of successful listening, spoken language, and literacy skills. However, providing such access is not sufficient to ensure attainment of communication and literacy goals. Rather, mastery of these capabilities depends on successful habilitation of a child’s developing brain to learn, reproduce, and, ultimately, understand oral and written words (Sach et al., 2003). Socioeconomic status (SES) has been established as an important determinant of these outcomes in the field of pediatric cochlear implantation. With respect to both rates of implantation and post-implantation language outcomes, significant inequities between lower-SES children with cochlear implants and their more affluent counterparts have been well documented (Connor and Zwolan, 2004; Geers and Brenner, 2003; Hodges et al., 1994, 1999; Hoff, 2002; Hyde and Power, 2006; Luetje and Jackson, 1997; Niparko et al., 2010; Sorkin and Zwolan, 2008; Tobey et al., 2003). Confronting these inequities is an essential step in the effort to help all children with hearing loss to reach their greatest potential within the world of listening and spoken language.
Despite routine newborn hearing screenings and efforts to provide timely intervention, many children with hearing loss in the USA do not experience equal access to care, intervention, or follow-up services. Socioeconomic, minority status, and non-English native language may prevent children from receiving the types of services and health care that they need to reach optimal developmental outcomes (Chin et al., 2009; Flores, 2009; Flores and Tomany-Koman, 2008). Yet even when children from low-SES or underserved populations have access to hearing technology, habilitation outcome disparities still persist. In a recent study, Chang et al. (2010) offered important insights into the approach necessary to achieve equal implantation rates and post-implantation outcomes among children with hearing loss. In a retrospective cohort study of 133 pediatric patients undergoing unilateral cochlear implantation, Chang et al. (2010) found that in a state with adequate Medicaid reimbursement, implantation rates were equal between higher-SES and lower-SES cohorts; still, a significant difference was noted in post-implantation markers. Children from lower-SES families had higher rates of complications, missed follow-up appointments with increased frequency, and were less likely to undergo a subsequent bilateral implantation (Chang et al., 2010). As this study shows, disparities in the intensive post-implantation habilitation process leave lower-SES families most vulnerable to diminished outcomes even when children have early auditory access.
Addressing the disparity in habilitation outcomes means not only ensuring that all children have access to timely hearing technology intervention, but also that these children experience the enriched environment that best supports their subsequent listening and language development following device activation. A recent national survey has shown that pediatric hearing loss professionals overwhelmingly identified increasing parental involvement as the most effective strategy for reducing post-activation outcome disparities (Kirkham et al., 2009). This survey further supports the existing multi-disciplinary body of evidence that shows the potential effectiveness of targeting parental involvement and knowledge during the habilitation process in order to improve child language outcomes (DesJardin and Eisenberg, 2007; Spencer, 2004; Zaidman-Zait, 2007; Zaidman-Zait and Young, 2008). Targeting parental involvement may be an effective method for improving the outcomes of children with hearing loss because of the critical role parent involvement plays in the development of children’s spoken language and reading skills (Niparko et al., 2010). Parents extend the benefits of therapy beyond the therapy session by assuring rehabilitation adherence through the consistent use of the hearing aid or cochlear implant and being essential language models during their children’s critical language learning period.
Parents are responsible for creating and maintaining the early language environment during the critical language learning period in the first years of life. Due to the all-encompassing nature of the early language environment and its intractable impact on listening and spoken language development, parent enrichment of the language environment is a crucial component of achieving successful habilitation outcomes. Compelling evidence from both child development and hearing loss literature demonstrates that linguistic environments are predictive of a child’s language development trajectory (Bus et al., 1995; Bornstein et al., 1998; Hall et al., 1987; Landry et al., 2000; Pan et al., 2005; Rowe, 2008; Weizman and Snow, 2001). The impact of the early language milieu on future learning was confirmed by Hart and Risley’s landmark study, which demonstrated a correlation between the number of words a typically-developing child is exposed to before age three and his or her later IQ and academic success (1995). Differences in income may not wholly explain these disparities because maternal language input and the home literacy environment mediate the association between SES and a child’s language development (Bornstein et al., 1998; Bus et al., 1995; Forget-Dubois et al., 2009; Foster et al., 2005; Hall et al., 1987; Hoff, 2003; Landry et al., 2000; Pan et al., 2005; Raviv et al., 2004; Rowe, 2008; Weizman and Snow, 2001). The significant inequities in home language environments – including lower quantity of talk and gesture, smaller mean length utterances, poorer syntactic complexity, decreased use of open-ended questions and greater use of directives – provide insight into the differences in early language environments that may lead to the disparities seen in children’s academic trajectories (Bornstein et al., 1998; Hammer and Weiss, 1999; Hart and Risley, 1995; Hoff, 2003; Hoff-Ginsberg, 1991; Rodriguez et al., 2009; Rowe et al., 2005; Walker et al., 1994). The quantity and quality of the types of language input described above decreases as a function of decreasing SES, resulting in a significant maternal-related SES language gradient where mothers from more affluent backgrounds provide a more enriched early language environment on average than mothers from less affluent backgrounds (Hoff, 2003; Huttenlocher et al., 2002).
While there exists an extensive body of evidence identifying and describing the unique role of parents in their children’s linguistic development, few evidence-based behavioral interventions have been developed specifically targeting parents, and even fewer interventions directly target lower-SES families (Baxendale and Hesketh, 2003). Improving the linguistic outcomes for currently underserved children with hearing loss, many of whom are low-SES, through parent-directed interventions that enrich typically austere home language environments would target one of the most significant factors affecting the habilitation process and, ultimately, children’s language development. Project ASPIRE (Achieving Superior Parental Involvement for Rehabilitative Excellence) is a behavior-change intervention seeking to address habilitation outcomes by supporting parent creation and maintenance of a developmentally supportive language learning environment for their children with hearing loss. The foundational behavior-change strategy of the Project ASPIRE intervention combines an education session and ongoing ‘quantitative linguistic feedback’ to motivate an increase in parental language input and parent–child interaction.
The full Project ASPIRE program is conceptualized as a 10-module Early Intervention (EI) curriculum intended for implementation by a developmental therapist-hearing or speech pathologist in the traditional, one-on-one EI therapy session. The Project ASPIRE curriculum will provide parents with critical knowledge and skills to help their children with hearing loss reach their fullest linguistic potential. Prior to launching a full program study, it was important to assess the feasibility of utilizing the home visit format as a vehicle for the Project ASPIRE curriculum and quantitative linguistic feedback as a method of increasing parental linguistic input when working with underserved and lower-SES populations. For the pilot study, the educational component was limited to a prototype of the first of 10 modules (education and quantitative linguistic feedback) as a one-time home visit intervention, followed by three quantitative linguistic feedback sessions. This design explores the feasibility and potential efficacy of utilizing quantitative linguistic feedback in combination with a home-visiting education session to increase parental linguistic input and parent–child interactions in low-SES and underserved populations.
II Method
The study protocol was approved by the University of Chicago Institutional Review Board. Families were compensated US$100 for their participation.
1 Study participants
Project ASPIRE is being developed to target a variety of underserved populations, which are not always identifiable solely by SES markers. Families who speak English as a second language were included in this initial proof of concept study in order to explore the program’s potential application to diverse populations in need of increased habilitation support (Flores, 2009; Flores and Tomany-Koman, 2008).
Eleven families, recruited from the principle investigator’s (author DS) pediatric hearing loss clinic, participated in the pilot study. To determine eligibility, parents were asked to fill out a short demographics questionnaire concerning their child’s medical history and family characteristics. Inclusion criteria were the following: 1) low-SES status (determined through enrollment in Medicaid and/or low maternal educational status), or English as a second language (ESL); 2) English or Spanish as the primary spoken language in the household; and 3) family communication approach that included spoken language.
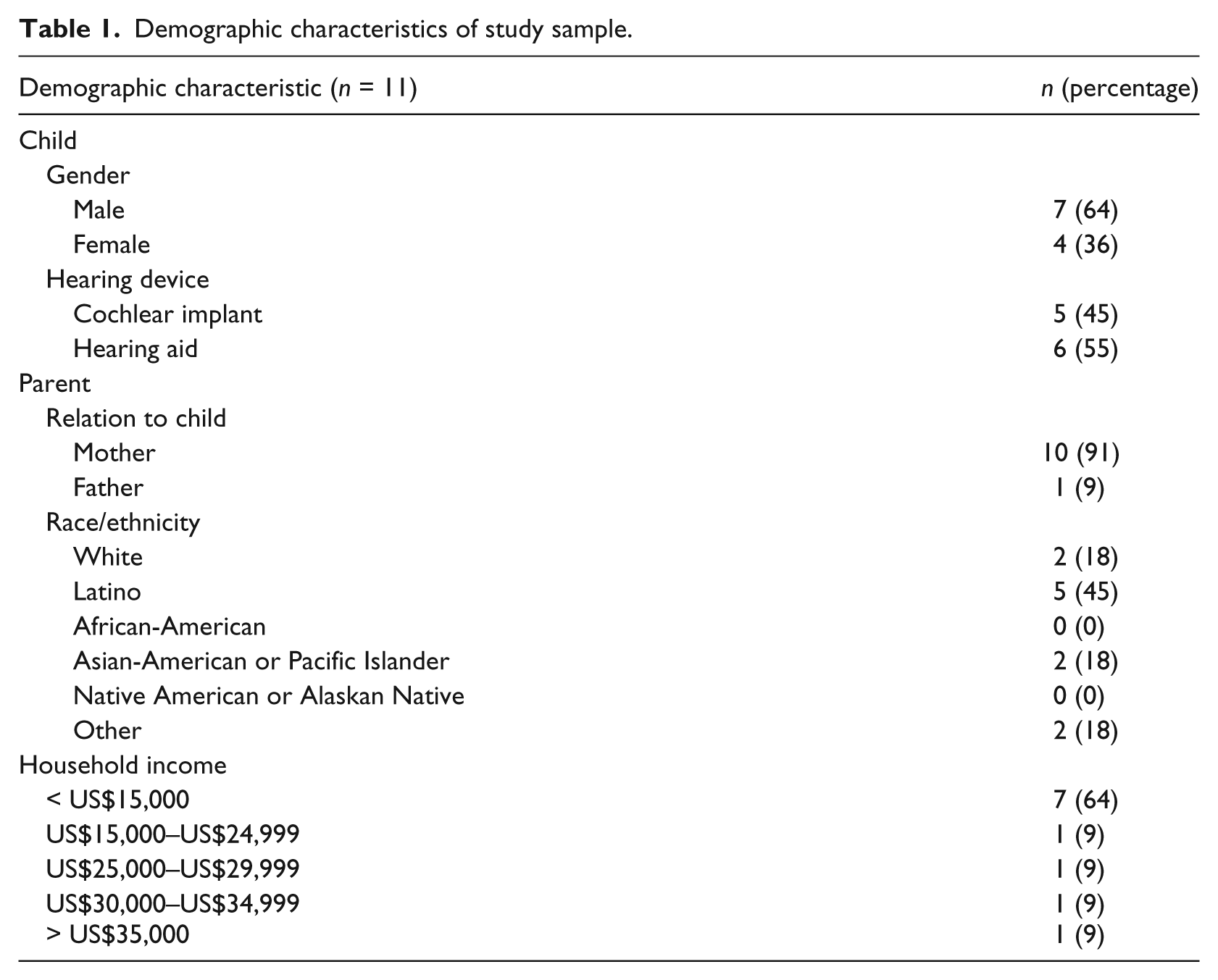
The demographics of the ASPIRE cohort are outlined in Table 1. Mothers made up most of the studied sample (n = 10), with only one father included in the study. The group was nearly evenly divided between participants with hearing aids (n = 6) and cochlear implants (n = 5). The majority of participants were from underrepresented minority groups; nearly half of the total cohort was Hispanic (n = 5). Household income for families in the study varied, but 7 families in the sample earned under US$15,000 per year. The average age at which the children were diagnosed with hearing loss was 23.8 months (range of 0 to 72 months); the average age at which the children began participation in Project ASPIRE was 32.5 months (range of 5 to 72 months).
Demographic characteristics of study sample.
2 Intervention
a Project ASPIRE education
The prototype educational module utilized in the study introduced parents to the idea that parent language input is pivotal to children’s language development and that receiving linguistic feedback could help parents monitor and augment their language environment. Using a standardized 60-minute PowerPoint presentation, the deaf educator in this study (author LR) made home visits to families to present the interactive module. The core concepts of the educational module included talking to children more often, using words and gestures to have conversations with children, and engaging in joint attention activities. A Spanish version was developed and a Spanish language translator was available for home visits for Spanish-speaking families. The PowerPoint presentation acted as a semi-structured script that allowed for standardization of presented information in a format that preserved the module’s fidelity while allowing for adaptation to families with differing levels of need, education, and skill.
b Quantitative linguistic feedback
Quantitative linguistic feedback is a behavior change strategy developed to give parents and care givers access to frequent, accurate information about their language behaviors (Suskind et al., 2013). The Language ENvironment Analysis system (LENA) system, consisting of a small recording device and accompanying computer software, was used to gather the audio environment data necessary for creating the personalized quantitative linguistic feedback charts that were given to parents. The small LENA recording device is worn by the child for up to 16 hours, giving researchers and parents unprecedented insight into the home language environment. While the LENA device is capable of providing actual audio files, which would allow transcription and ultimately qualitative analysis, audio recordings were deleted to protect family privacy per Institutional Review Board protocol. Therefore, only quantitative data were downloaded and processed.
LENA processing software applies research-supported algorithms to the audio recordings to determine adult word count (AWC), conversational turn count (CTC), and child vocalization count (CVC). AWC refers to the number of words adults say in close proximity to the child wearing the device, CTC refers to the number of child–parent vocal interactions within a specified time frame, and CVC refers to the number of times the child wearing the device vocalizes (Gilkerson and Richards, 2008; Greenwood, 2011). The LENA also has the ability to distinguish distant sound and electronic sound (i.e. television).
3 Procedure
The protocol for this study began with two separate 16-hour LENA recordings to provide a baseline of the family’s language environment for comparison. For each recording, parents filled out a ‘recording day information sheet’ to note child nap times and recording start and stop times. After the completion of these baseline recordings, a deaf educator (author LR) conducted the 60-minute educational home visit that included a review of the educational module and a discussion of the parents’ quantitative linguistic feedback from their baseline LENA results. Parents, through collaborative discussion with the deaf educator, applied the educational information and linguistic feedback to determine realistic goals for their next LENA recording session.
Following the one-time intervention home visit, parents completed three post-intervention recordings to assess parental linguistic behavior change. Parents continued to receive quantitative linguistic feedback via phone sessions with LR after each follow-up recording was processed. The ongoing linguistic feedback formed the basis for discussion of parental linguistic goal setting, including AWC goals and CTC goals, and for increasing parents’ quantitative language parameters.
4 Data processing
Research assistants extracted data from the recorder in raw form using the LENA software on a dedicated study computer. All data were then processed into counts by the LENA Advanced Data EXtractor (ADEX) software, and the audio recordings were discarded. Language-related outcomes were assessed on three main measures: AWC, CTC, ad CVC. In addition, the total television time was recorded and analysed. A computer script was written to filter naps and other extended periods during which direct interaction between parent and children was unlikely. Naptime and parent–child interaction start and end time parameters were set using the information parents provided in their initial surveys and on their daily recording time sheets. Once filtered, all counts were standardized by total relevant interaction time and are here expressed as words-per-hour (wph), turns-per-hour (tph), or vocalizations-per-hour (vph). Script outputs were assessed and merged with parent time sheet and demographic file data to reconcile data inconsistencies (e.g. when parent-recorded and LENA-recorded dates did not align).
5 Analysis and statistics
In total, five 16-hour sessions were recorded and downloaded for each participant: two pre-and three post-intervention recordings. To control for the Hawthorne effect (i.e. observer effect), the first baseline LENA recording was not included in analysis and post-intervention parameters were compared to the second baseline recording only. An entire sample baseline series was generated from this data. Post-intervention scores were generated by averaging the data from the three post-intervention recordings. AWC, CVC, ad CTC were analysed using two-tailed paired t-test for difference, comparing averaged pre- and post-intervention scores, in STATA 11 (College Station, TX; 2009).
III Results
At baseline for AWC, the cohort averaged 1,319 (SD = 363) wph. After the Project ASPIRE prototype module intervention, the average AWC increased to 1,575 (SD = 538) wph. The change in AWC post-intervention approaches significance with an increase of approximately 20% above baseline measures (p < 0.1). The average AWC per hour for each recording is depicted in Figure 1.

Average adult word count in words per hour.
CTC had a pre-intervention average baseline of 32 tph (SD = 14). This measure showed an average increase to 49 tph (SD = 25) after the intervention, a significant increase of 53% from baseline (p < 0.01). The average CTC per hour for each recording and post-intervention recording average is depicted in Figure 2.

Conversational turn count in turns per hour.
The pre-intervention average baseline for CVC was 124 vph (SD = 63). Following the intervention, CVC average increased to 177 vph (SD = 93), a significant increase of 43% from baseline (p < 0.05). The average CVC per hour for each of the three post-intervention recordings is displayed in Figure 3.

Child vocalization count in turns per hour.
IV Discussion
While disparity-related discussions often focus on unequal access to medical and educational interventions, a fundamental and often overlooked issue in low-income populations is that of the early language environments. While undoubtedly obtaining auditory access through cochlear implants or hearing aids is a critical first step, it is a child’s early language environment that plays a critical role in his or her language and cognitive trajectories. The pervasive disparities in habilitation related to SES require targeted, inclusive, and culturally-sensitive interventions.
The results of this proof of concept study support the potential efficacy of a home visiting approach that combines education with evidence-based behavior change mechanisms to enrich the early language environments of children with hearing loss who may otherwise experience less than optimal habilitation outcomes.
The significant increase in CTC and CVC suggests that the Project ASPIRE intervention influenced a rich, nuanced component of the habilitation process: parent–child linguistic interaction. The change in parent linguistic input, as evidenced by the increase in CTC post-intervention, reflects how often parents spoke directly to or in response to their children with hearing loss. As such, the CTC increase seen in this study may be understood as a substantial enrichment of parent–child verbal interaction following intervention. The accompanying significant increase in child vocalizations post-intervention provides further insight into the level of vocal engagement during the recording day. CTC and CVC, when compared to AWC, offer a more meaningful picture of the children’s home language experiences because they measure parent–child vocal interactions and child vocalizations rather than just simply adult speech. AWC, which trended towards significance, must be interpreted carefully as it has the potential to be artificially elevated throughout the day due to changes in the number of adults in the child’s immediate area. The impact that parent–child conversations may have on childhood language development and school readiness has been documented in the early childhood literature (VanDam et al., 2012).
The signficant increases in CTC and CVC documented in this study support the existing multidisciplinary evidence and professional belief that a parent-focused approach has great potential to effect positive change in the home language environments of children within the low-SES and underserved patient population and may, in turn, affect child language behaviors (Kirkham et al., 2009).
1 Limitations and next steps
Several limitations in this study must be addressed. First, the sample size of 11 participants from a single academic medical center requires recognition of the potentially limited generalizability of the significant results obtained. Additionally, in this pilot no control group was present to reduce the possibility of confounding factors that might explain the significant increase in language output that was observed. In future studies, the inclusion of child developmental measures administered pre-and post-intervention may provide a more accurate picture of Project ASPIRE’s impact. For example, it is unclear if the natural aging of children during the length of the study might account for increase in speech production in children or parent. Similarly, the differing lengths of time between patients’ receipt of hearing aids or cochlear implants and their participation in ASPIRE may affect the rate of their language development. A randomized controlled trial of a larger sample size is a clear next step in this investigation and will be conducted upon completion and final testing of the 10 Project ASPIRE educational modules.
An additional limitation is the possibility of a Hawthorne bias because families were observed and recorded during five discrete periods of time during which they were aware that they were being recorded. While the first recorded session was discarded in an attempt to eliminate the session most likely to be affected, this is an imperfect control. Ultimately, a long-term longitudinal assessment using a compilation of quantitative and qualitative measures of parent and, most importantly, child language outcomes will be the most effective way of assessing the intervention’s success.
Finally, with only 11 participants in the sample, this pilot study did not have adequate power to detect a more subtle increase in AWC, which showed a 20% increase from baseline measures. A future study with a larger sample size is needed to properly evaluate the intervention’s effect on AWC.
2 Conclusion
Combining education and linguistic feedback, Project ASPIRE is a unique, multifaceted intervention designed to provide low-income or underserved parents with the critical knowledge and skills necessary to best help their children to navigate the post-implantation process and reach their spoken language potential. The behavior change centerpiece of Project ASPIRE is the concept of quantitative linguistic feedback. Rather than creating a knowledge transfer curriculum that views education alone as the central method for achieving increased parental language production, the curriculum is built upon the understanding that incorporation of formalized techniques from the behavior change literature is imperative. From an understanding of the importance of a child’s home language environment, Project ASPIRE was developed to focus on improving a child’s home language environment as a means to improving child language outcomes. The first step in developing this approach is to demonstrate that parental linguistic behavior is, in fact, amenable to a direct intervention through linguistic feedback. This study is offered as a critical piece of evidence supporting the underlying theory upon which Project ASPIRE has been created. With this support of concept, the next stages of project development may be undertaken with confidence in the potential for success of a truly parent-inclusive, accessible, and culturally sensitive language intervention.
The 10 modules of Project ASPIRE currently in development offer a new approach to confronting the pervasive disparities in the field of Pediatric Cochlear Implantation. With a combination of education and linguistic feedback, the Project ASPIRE curriculum seeks to fill a void within the current resource structure available to children with hearing loss and to their families. With this pilot study as a proof of concept, the development of Project ASPIRE will continue with reason to believe in the power of a parent-inclusive approach to help families that are confronting the complex challenges of hearing loss to succeed in the world of listening and spoken language.
Footnotes
Author Note
Partial preliminary results included in this article were presented at the American Society of Pediatric Otolaryngology (ASPO) Scientific Program, Combined Otolaryngological Spring Meetings (COSM) in 2010, Presentation Session 2.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.