
Abstract
This study investigates whether extension of a caregiver-led interactive language program may enhance its effectiveness in supporting communication. Caregiver-led language programs, which focus on establishing responsive interaction patterns to support opportunities for communication between caregivers and young children within natural settings, are frequently used in early childhood intervention services. One example is the Hanen Program It Takes Two to Talk® (ITTT), which involves working in groups with caregivers, with some concurrent individualized support for families. Given the importance of communication, potential strategies to enhance the effectiveness of such programs warrant investigation. Based on a transactional theory of interaction, it can be hypothesized that by directly supporting communication partners to continuously adapt to each others’ behaviours, individualized interventions may further enhance the outcomes of ITTT and, potentially, similar programs. In phase one of this study, 10 caregivers of young children with a range of disability labels completed the ITTT program. Participants were then randomly assigned to a control or experimental group for phase two. In the experimental group, the caregivers were provided with additional individual sessions with a Speech Language Therapist over the subsequent four months. Assessments of caregiver–child interactions were conducted prior to commencing the ITTT program, following the completion of phase one, and again at the completion of phase two. Significant positive changes were found at the completion of phase one for all participants. These findings support the effectiveness of the ITTT program. At the completion of phase two further significant positive changes were found for the experimental group. For the control group there was no further notable change. Although this is a small study, the findings have implications for practice in demonstrating that extending the individualized support provided within such programs may facilitate increased communication, with benefits for caregiver–child interactions and relationships and for child participation more broadly.
Keywords
I Introduction
A social-interactionist approach to language development theorizes the role of the environment and social engagement and emphasizes the role of caregivers (and significant others) in scaffolding a child’s language learning (Bruner, 1983; Chapman et al., 1992; Snow, 1977, 1999). There is growing interest in naturalistic and interactive models of language intervention based on social-interactionist theories of language development as theorists and practitioners move away from conventional didactic and decontextualized methods (Abbeduto et al., 2006; Baxendale et al., 2001).
Research demonstrates that caregiver responsiveness to child communication attempts impacts on child language development (Brady and Warren, 2003; Mahoney and Nam, 2011). Caregiver responsiveness can be understood as the combination of observing, waiting, listening and then responding promptly to a child with warmth, and interest (Girolametto and Weitzman, 2006). For example, a caregiver might smile and acknowledge a child’s communicative attempt and then repeat the approximation to show understanding. Responsive caregiving has been shown to support, extend and enhance child language development in meaningful ways through scaffolding and modelling the child’s communicative exchanges within naturally occurring incidents (Abbeduto et al., 2006; Baxendale et al., 2001; Brady and Warren, 2003; Girolametto et al., 2007).
Caregiver responsiveness has been found to contribute to improved language and literacy development, as well as to skill generalization across multiple contexts (Brady and Warren, 2003; Girolametto et al., 1996; Konza et al., 2010). Increased responsiveness and less directive or controlling approaches on the part of the caregiver have also been associated with increased child initiation and production of communication, as well as child vocabulary growth (Pennington and Noble, 2009; Pennington et al., 2009; van Balkom et al., 2010; Yoder and Warren, 2002). However, some caregivers need information and support to facilitate this responsiveness.
In their review of two decades of research examining the parental model of developmental intervention, Mahoney and Nam (2011) found that caregiver responsiveness was positively associated with language and communication development; however, caregiver directiveness, intrusiveness and hostility were qualities found to hinder child development. Such recognition of the importance of caregiver–child interactions has prompted consideration of how best to assist caregivers in promoting child language development. Consequently, interactive language interventions focus on supporting caregivers in enhancing their communication skills through establishing interaction patterns that support opportunities for communication within natural settings and decrease directive approaches (Pennington and Noble, 2009; Pennington et al., 2009; van Balkom et al., 2010; Yoder and Warren, 2002).
Sameroff’s (1975) transactional theory proposes that child development is dependent upon interactions, and notably the interactions between caregivers and children. When applied to language and communication, a transactional theory of interaction holds that communication partners continuously adapt to each others’ behaviours (Pennington and Noble, 2009; Pennington et al., 2009) and, therefore, that child-language intervention would be more beneficial when focused on both adult and child behaviours. Programs based on transactional theory have been found to be helpful in reducing caregiver directiveness and increasing reciprocity in communicative interaction; for example, turn-taking (Pennington and Noble, 2009). Consequently, a transactional theory of interaction is useful in developing interactive language interventions.
Consistent with this theoretical approach, Hanen Parent Programs (HPPs) aim to provide caregivers with support, education and practical facilitative strategies. These include following the child’s lead, imitating the child’s communicative attempt (for example, gesture, sound or approximation), interpreting and responding to the child’s communicative efforts, and regarding all communicative efforts as meaningful (Baxendale et al., 2001; Carter et al., 2011; Girolametto et al., 2007). As a result, caregivers’ increased responsiveness is hypothesized to motivate children to engage in language-rich social exchanges, thus stimulating early social communication skills, vocabulary and syntax development (Girolametto et al., 2007).
It Takes Two to Talk® (ITTT) is a program for working with caregivers to foster a responsive approach to communication in which caregivers promote interaction, respond to child initiations and follow the child’s lead (Girolametto and Weitzman, 2006; Whittingham et al., 2011). It is one of a suite of programs developed by the Hanen Centre. ITTT is designed to support young children who have been identified as having delayed communication development. The child may also have delays in other aspects of development, including a range of disability diagnoses or impairment labels. Other programs from the Hanen Centre include More Than Words® and TalkAbility™, specifically designed to promote caregiver and child interaction for young children with Autism Spectrum Disorders, whilst Learning Language and Loving it™ and ABC and Beyond™ focus on supporting early childhood educators and other staff to facilitate the communication development of all children within an early education setting.
ITTT is a group intervention program, supplemented with individual sessions that involve coaching and video feedback. It is designed to support caregivers by developing their ability to acknowledge child attempts to communicate, and their confidence in providing opportunities for shared communication to occur in the context of everyday routines and experiences (Girolametto and Weitzman, 2006). This approach is based on transactional theory of interaction; therefore, positive outcomes for child vocabulary growth and active interactions are predicted as a consequence of increased caregiver responsiveness (Whittingham et al., 2011).
Interactive language interventions have been widely used with children who have language delays, but no other diagnoses. However, the effectiveness of such programs have also been investigated in a number of studies with children who have a range of diagnoses. Consequently, in this article we consider research with diverse groups of children, thus addressing both aspects of the research.
Research since the 1980s into the effects of HPPs on caregiver language input and child vocabulary and language development with diverse groups of children (including children labelled as having expressive vocabulary delays, Down syndrome, cerebral palsy, autism, and children without language delay or impairment labels) has provided evidence of increased caregiver responsiveness and decreased caregiver directiveness post-intervention (Girolametto, 1988; Girolametto et al., 1996, 2007; Konza et al., 2010; Leffel and Suskind, 2013; Pennington et al., 2009). The use of HPPs has been found to support caregiver communication methods that have facilitated child communication, resulting in increases in child communicative initiations and interactions and leading to more joint activity around child interests, compared to children in control groups (Girolametto, 1988; Girolametto et al., 1996, 2007; Konza et al., 2010; Pennington et al., 2009). Caregivers who participated in these studies reported increases in child vocabularies overall and the generalization of acquired skills across multiple contexts (Girolametto et al., 1996; Konza et al., 2010). Additionally, children used more multiword combinations and early morphemes, compared to control groups, increasing the structural complexity of their language (Girolametto et al., 1996; Konza et al., 2010). Although standardized testing in some studies has not been consistent with participant reported increases in language development (Girolametto, 1988), caregiver evaluations and focus group discussions reveal an overall high rate of satisfaction with the HPPs (Konza et al., 2010).
In addition to supporting communication between caregivers and their children, research has also identified numerous secondary benefits stemming from participation in HPPs. As child communication capabilities and behaviour are linked, it is unsurprising that caregivers identified positive changes in child behaviour post intervention, and thus decreased caregiver stress (Hancock et al., 2002; Konza et al., 2010; Mason, 2004; Whittingham et al, 2011). For example, a study conducted by Hancock et al. (2002) explored the efficacy of a caregiver intervention program with children labelled with language delays and emergent behaviour concerns. It was hypothesized that by providing caregivers with practical strategies to increase their responsiveness in communicating with their child, child behaviour would improve. After participation in the program, caregivers demonstrated greater responsiveness to their children, positive changes were found in child language and behaviour, and caregivers reported decreased stress levels. Follow-up data collection indicated that these positive changes were maintained six months after completion of the program. Therapist accounts also indicated an increase in caregiver self-confidence and self-esteem and strengthened caregiver–child relationships post intervention, along with strengthened caregiver–therapist relationships, allowing for more effective and positive collaboration during the creation of goals and planning of therapy (Konza et al., 2010).
However, by contrast, in a randomized controlled trial of the efficacy of the More Than Words’ HPP program with young children labelled with autism, Carter et al. (2011) found no major intervention effects. Carter et al. (2011) measured child communication and caregiver responsivity. Results were found to be dependent on child variables upon entering the program. Additionally, even following successful engagement with HPPs, the confidence of caregivers as primary supporters of their child’s communication development may diminish after the completion of the program (Girolametto et al., 1993; Pennington and Noble, 2009; Pennington and Thomson, 2007). Consequently, further research is required using a range of HPPs with diverse child and caregiver groups.
While research predominantly demonstrates positive outcomes of HPPs, HPPs are considered time intensive, requiring twice as much clinician time as traditional, direct intervention programs (Baxendale and Hesketh, 2003). This has been found to impact on caregiver perspectives towards the program, with caregivers indicating that organizing adequate time to complete all of the program’s specific components is a barrier (Pennington et al., 2007; Pennington and Thomson, 2009). This has also evidently affected therapists working with caregivers with the program (Pennington and Thomson, 2009). These concerns are exacerbated by a lack of resources, including accessible transportation, low-quality equipment, and a lack of support by relevant stakeholders (Pennington and Thomson, 2009). As a result, alternative speech and language intervention programs, which use strategies similar to HPPs, have been created to reduce time demands but with the intention of achieving similar outcomes for caregivers and their children (for example, for parent–child interaction therapy, see Falkus et al., 2015; for the Heidelberg parent-based language intervention, see Buschmann et al., 2009).
Aside from criticisms of the time intensive aspects of HPPs, caregiver accounts indicate that HPPs may not be individualized enough to provide optimal outcomes (Girolametto et al., 1993; Pennington and Noble, 2009). For example, caregivers in Girolametto et al.’s (1993) and Pennington and Noble’s (2009) studies indicated that they regarded individualized instruction and home visits as more beneficial than the group activities, due to the usefulness of information provided directly in relation to their own family needs. As a result, Girolametto et al. suggest that more individual sessions may be required to optimize intervention outcomes.
These findings are consistent with anecdotal evidence over the past decade in the early intervention (EI) settings participating in this research. While caregivers report that the foundational knowledge provided in the ITTT group sessions is helpful, they also frequently report that individual sessions are of greatest benefit as they entail an individualized approach specific to the particular child and caregiver. Additionally, EI staff often identify that particular caregivers require additional support to that offered in the ITTT program in order to maintain their confidence in and engagement with the strategies learnt during the program.
Based on a transactional theory of interaction, it can be hypothesized that in directly supporting caregivers in continuously adapting to each others’ behaviours, further individualized sessions would optimize the intervention outcomes. Consequently, this study was designed to investigate whether additional individualized interventions following the completion of the ITTT program, would impact on caregiver–child interactions.
II Method
This research reports a case study that investigated the impact of providing additional support to caregivers following the completion of the standard ITTT program, compared to a control group who participated in the standard program only. This research involved collaboration between university researchers and staff in three EI settings in a large city in New South Wales, Australia. HPPs are used as part of the overall program provided by the EI settings involved. Consequently, a convenience sample was used. Ethical clearance for the study was obtained from the Macquarie University Human Research Ethics Committee and the confidentiality and anonymity of the participants was ensured.
The impetus for this research, as noted above, came from anecdotal evidence gathered over a 10-year period at the EI settings, suggesting that the ITTT program was associated with positive changes in child and caregiver communication and interactions, but that caregivers found the individualization offered through one on one sessions particularly helpful and that increasing this support may hold important possibilities for extending the effects of the program. The design of the study was strongly influenced by the practices within the EI settings. This organic approach offers many benefits, including the rapport already developed between therapists and families, the familiarity of the therapists involved with the training program and assessment measures, and the direct applicability of research to practice. However, there were also some challenges. The decision was made early on in the research to conduct the research process in a manner that caused minimal additional work or disruption to the regular EI settings, including continuing with the assessment tools generally used in each EI setting. This resulted in one mismatch on a measure that was initially intended to be used for the data collection, in that some EI settings used the MacArthur–Bates Communicative Development Inventories (Fenson et al., 2007), while others used the Australian English Developmental Vocabulary Inventory (MARCS Auditory Laboratories, 2004, adapted from Fenson et al., 1993; Manolson, 1992; Weitzman, 1992). Consequently, the child vocabulary scores were not included in the data analysis. These assessments were still completed as part of the intervention process, providing caregivers and EI staff with a comparison of the child’s vocabulary pre and post intervention. However, only the caregiver–child interaction data was analysed.
Participants were obtained from three different EI settings. Consequently, the experience of the ITTT program would have involved some variations dependent on individual therapists running the program at different time points. However, each program was facilitated by a speech-language therapist (SLT) with appropriate certification and previous experience running the ITTT program. Additionally, the second author (who is a certified HPP trainer) audited sessions in each program to ensure program fidelity.
1 Participants
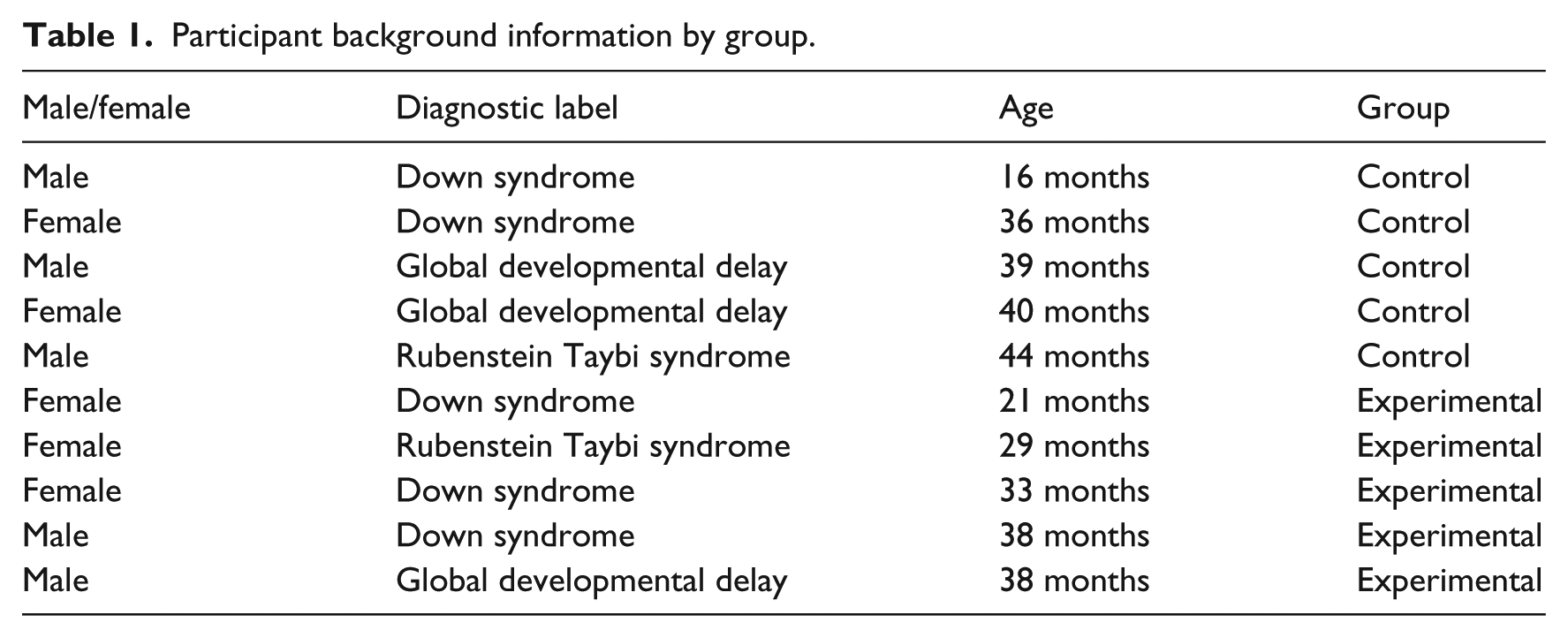
The participant sample of 10 caregivers was obtained from the pool of caregivers participating in the ITTT program. Caregivers who volunteered to participate in the research itself were randomly assigned to either the control or experimental group. Child information for the two groups is provided in Table 1 in ascending age order. The children had a range of diagnostic labels and associated speech and language support needs. None of the children were diagnosed as having major vision impairment and none were hard of hearing. Participants were excluded from the study if the caregivers did not complete the ITTT program (one family moved interstate during the study). Participants were also excluded from the study where assessment data was incomplete. However, these caregivers were not excluded from the HPP itself.
Participant background information by group.
2 Design and procedure
As shown in Figure 1, the study involved two phases. The first phase incorporated a pretest–posttest design with the standard ITTT program implemented in between. ITTT is facilitated by a certified SLT and involves eight group sessions with caregivers of 2.5 hours per session over 10–12 weeks (children are not present in the group sessions), along with four concurrent home visits (one of which is the pre-program visit and baseline assessment) of 1–2 hours per visit during which caregivers interact with their child.
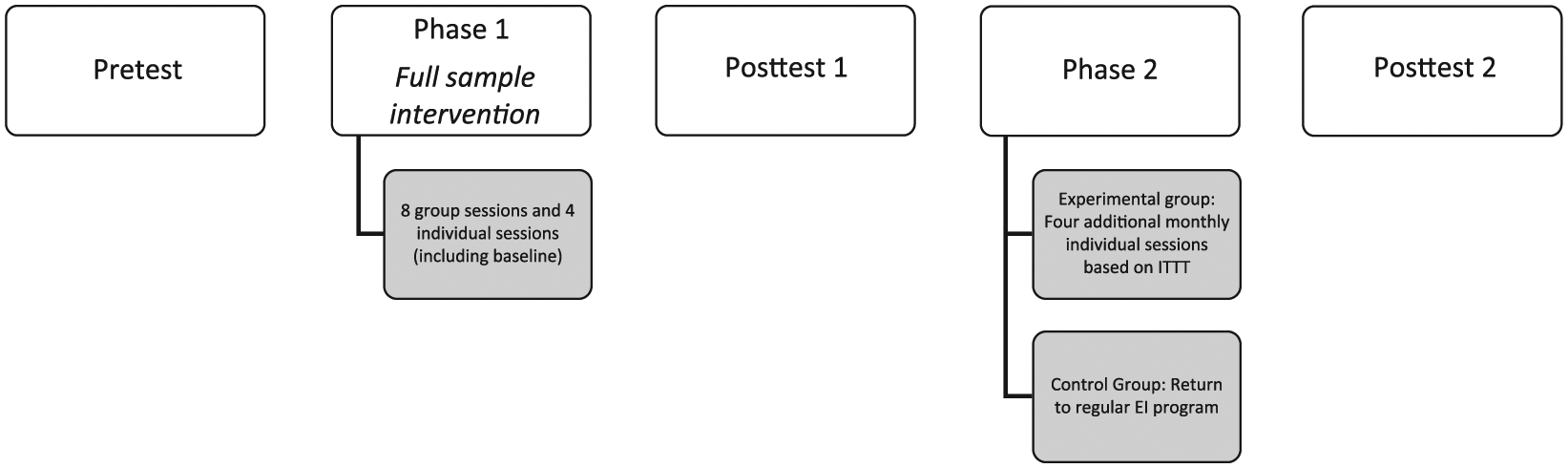
The study design.
Information and practical strategies to promote interaction and communication development were introduced incrementally, supported by the use of video feedback with individual participants during their home visits. Group sessions included group problem solving, role-play, viewing and discussing video footage, and information sharing with the SLTs. Participants (n = 10) were supported to develop individual objectives for their child based on the child’s communication stage and individual needs. Program materials such as caregiver handouts were provided to support the session activities. In addition to the group information sessions, the four individual home visits incorporated the use of videotaping and immediate reflection by the caregiver and SLT. During these individual sessions caregivers were able to trial the use of specific strategies in the context of their home and daily routines whilst examining the outcomes of using these strategies on their child’s communication. Families were encouraged to plan for specific opportunities throughout the day to use identified strategies consistently and employ practical ways to remember how and when a strategy could be used.
For phase two, the participants were randomly assigned to an experimental (n = 5) or control group (n = 5) for follow up EI services. A no-treatment control group was not incorporated into the study in response to ethical concerns about withholding intervention from families. All participants completed the ITTT program, then the control group returned to their regular EI support while the experimental group were provided with four additional individual sessions over a four-month period with a Hanen certified SLT to continue to implement the principles outlined in the ITTT program. The format of four sessions over the following four months was chosen in order to take a staged learning approach (through monthly sessions) over a comparable period of time as phase one. This number of sessions was also considered practical in terms of the time demands on the families and the EI services. The addition of four sessions resulted in a balanced group and individual approach for the experimental group in that they received eight group sessions and eight individual sessions across the two phases of the intervention.
The format of the additional sessions was consistent with individual sessions offered within phase one, utilizing video feedback related to use of identified strategies. All participants (from both groups) completed the final assessment four months after completion of the phase 1 ITTT program. This design enabled consideration of the effects of additional individual sessions with a SLT following on from completion of the standard ITTT program.
3 Measures
Child and caregiver interactions were assessed using the Parent–child interaction checklist (PIC) (Stewart, 2006). This involved videotaping each caregiver engaging in brief interactions with their child, representative of a daily interaction or scenario. For example, sharing a toy, reading a book, completing a daily routine such as washing hands, engaging in a song, or playing a ‘people’ game. (A people game refers to an interactive game or activity caregivers may play with their child such as ‘peek-a-boo’.) Caregiver and child interaction behaviours are rated on the PIC according to a number of descriptors (for example, the caregiver waits to let the child take a turn, the child initiates communication, the caregiver joins in with the child, the child imitates the caregiver, the caregiver expands on the child’s expressive communication). This measure was scored on the basis of video footage by a SLT trained in scoring this task. The SLT was unaware of the purpose of the study or the grouping of the participants. One full set of videos was also scored independently by another trained SLT in order to determine interrater reliability. Reliability was calculated at 67%, and all disagreements of more than 1 point were triple coded by a third SLT, who is trained in scoring the PIC.
In addition to assessment of interactive behaviours, feedback from participants was also gathered. Caregiver evaluations were collected at the completion of phase one for all participants, and at the completion of phase two for participants in the experimental group.
III Results
Phase 1
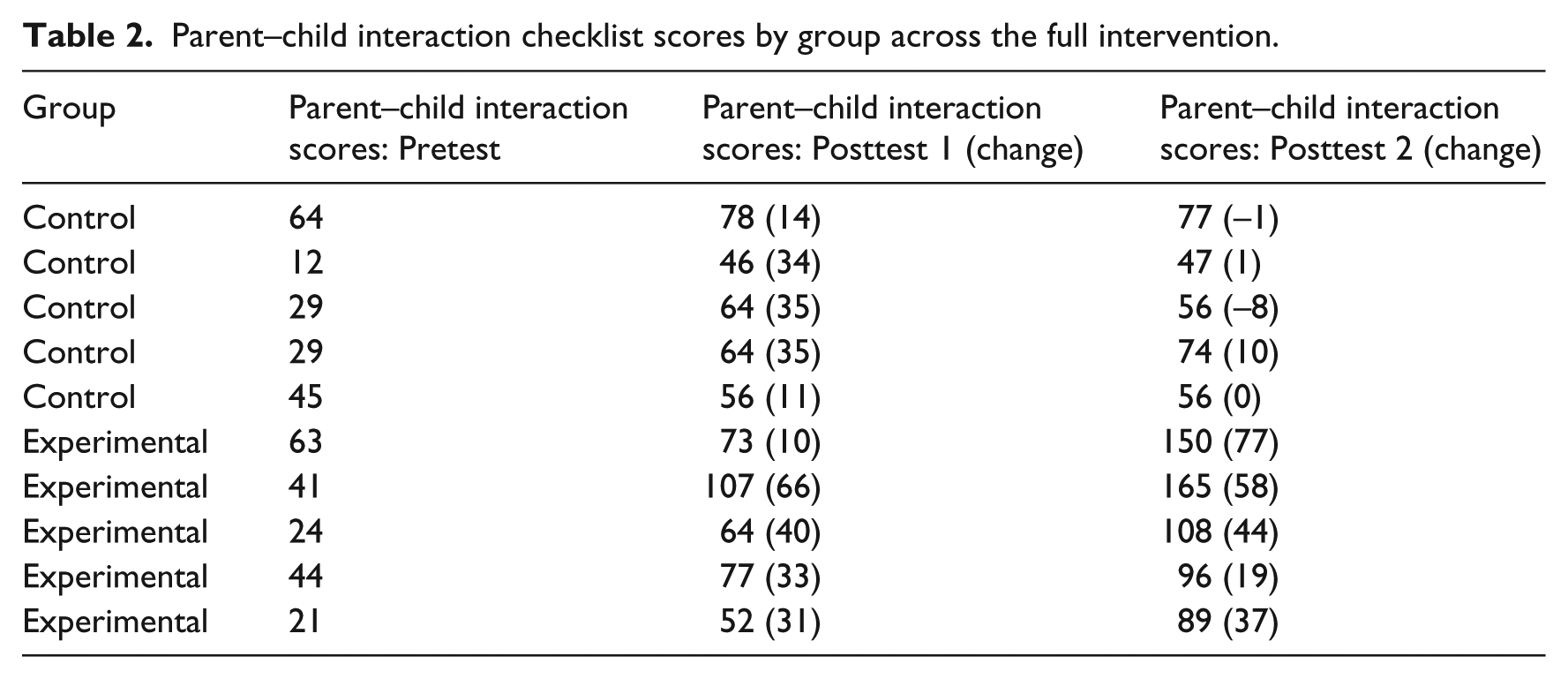
Due to the small sample size and the diversity of the participants, non-parametric statistics were used for analysis of the experimental results. A Wilcoxon Signed-Ranks Test indicated that the posttest 1PIC scores were significantly higher than the pretest PIC scores (Control group Z = −2.015, p < .044; Experimental group Z = −2.402, p < .016) following completion of the standard ITTT program for the full sample (n = 10).The analysis considered the change in scores from pre to post (see Table 2), thus accounting for variation in scores at the outset of the program.
Parent–child interaction checklist scores by group across the full intervention.
Feedback from caregivers after completing phase one (using the standard Hanen parent feedback form) indicated a positive response to the program. For example, one participant commented: ‘This course has helped us incorporate the strategies into many of our daily routines. It is now quite a natural part of our daily interactions.’ Many participants were able to describe specific strategies and their impact on their child’s communication. For example, ‘I speak slowly and stress the words I am trying to get him to say,’ ‘I wait longer and more expectantly’ and ‘He is now spontaneously saying some words.’ Participants commented on the video feedback and individual support received during the training. When asked which aspects of the program they found helpful one participant reported ‘particularly video feedback because although we may feel we’re putting strategies into place, seeing the video reinforces the areas we need to improve.’
Phase 2
The posttest 2 PIC scores (see Table 2) were analysed separately for the control (n = 5) and experimental (n = 5) groups. A Wilcoxon Signed-Ranks Test indicated that the posttest 2 PIC scores were not significantly higher than the posttest 1 scores for the control group (Z = −.106, p < .91) following the return to regular EI without additional ITTT individual sessions. A Wilcoxon Signed-Ranks Test indicated that the posttest 2 PIC scores were significantly higher than the posttest 1 scores for the experimental group (Z = −2.193, p < .028) following the additional ITTT individual sessions. Again, the analysis was concerned with the change in scores following phase 2.
Participants within the experimental group commented on their satisfaction with the continuation of individual support during phase two, noting the benefit of having the opportunity to continue to refine and adapt their approach to interactions and identify new ways to use strategies as their child’s communication developed and they needed a slightly different focus or combination of strategies to continue to support shared communication. Participants reported that the guidance provided in the individual sessions aligned directly with the strategies and activities they were currently engaged in with their child and that the opportunity to practice new or refined strategies immediately, and in the everyday context, during the follow up individual sessions was particularly helpful for further building their communicative responsiveness.
All participants rated their satisfaction with the video feedback sessions (using the standard Hanen parent feedback form) as ‘very helpful’ (5 out of a possible 5). Specifically, participants continued to comment on the use of video review as a powerful tool for reflection. For example, ‘It’s always a great help to watch back on tape how we communicate with our kids’ and ‘watching the video gives me ideas on how to improve my approach’. Participants indicated interest in continuing individual support utilizing video feedback and specific strategies learnt during the ITTT program.
IV Discussion and conclusions
This study was designed to investigate whether an individualized intervention program, following the completion of the ITTT program, would impact on caregiver–child interactions. As hypothesized, the provision of four additional individual sessions was found to further enhance the outcomes of the caregiver-led ITTT intervention. This finding supports the hypothesis put forward by Girolametto et al. (1993) that providing additional individual sessions may be beneficial. The sample size for this study is small, thus the results need to be interpreted with caution. However, there are a number of findings that warrant further investigation in regards to their implications for practice.
As the results indicate, there was a significant increase in PIC scores for the experimental group following the additional ITTT individual sessions. This provides evidence to suggest that the additional individual sessions supported caregivers in maintaining and further developing their communicative behaviours, further reducing caregiver directiveness, increasing child communicative initiations and interactions, leading to more joint activity based on child interests, and facilitating increased reciprocity in communicative interactions. This may be due to the fact that, consistent with a transactional theory of interaction, individual sessions enable the provision of direct support to caregivers in continuously adapting to their child’s particular behaviours in a way that is beyond the scope of group sessions. The one-on-one format lends itself to greater individualization than within a group session. Importantly, the individual sessions involve the immediate application of the strategies between caregiver and child, followed by immediate feedback with the SLT (supported through video feedback), whereas the children are not present within the group sessions.
Additionally, while caregivers often complete an intervention program feeling confident in utilizing specific strategies in interaction with their child, the provision of continued and individualized support creates the opportunity to continue to engage with successful strategies that are appropriate as communication changes over time. In this study we found that caregivers often had a clear goal in mind for a given interaction, but sometimes forgot to use the most fundamental strategy: waiting. The effective and continued use of specific responsive strategies requires continued reflection and adaptation in the moment that interactions occur. Like most behaviour change for adults it can take time for new strategies to feel natural or to be used automatically. The additional individual sessions provided in the experimental condition may have provided the time and opportunity for reinforcement. However, it is also possible that simply continuing intervention for a further four months, in itself, may have contributed to the maintenance of the parents’ changed behaviour, rather than the change being the result of the specific content of the ongoing intervention.
As noted earlier in the article, four monthly individual sessions were chosen in order to engage in staged learning over a period of time comparable to the original ITTT program. The result is a shift towards a more individualized approach overall. The initial program, consisting of eight group sessions plus four individual home visits (including the baseline assessment), is largely a group program, whereas adding an additional four individual sessions, means the division of time between the group and individual sessions is equal. These findings may suggest that the ITTT program could be optimized through stronger emphasis on individualization, with the group component directed at more general foundational skills.
However, while the study’s findings justify consideration of the extension of the individualized aspects of ITTT, they also lend further support to the effectiveness of the program in its standard form. The significant increase in PIC scores for the full group following completion of phase 1 is consistent with previous findings that the ITTT program promotes a more responsive approach to communication in which caregivers facilitate more interaction, respond to child initiations and follow the child’s lead (Girolametto and Weitzman, 2006; Whittingham et al., 2011).
The fact that no significant decrease was found in the PIC scores for the control group four months after completion of the ITTT program (and a return to regular EI), is also noteworthy. While there have been mixed findings regarding the maintenance of intervention effects in previous research, this finding demonstrates maintenance of the behaviours developed through the ITTT program four months after completion for the participants in this study. Further, the findings support the broad applicability of the ITTT program given the range of diagnoses of the participants’ children.
The positive caregiver responses to the intervention reported in this study are consistent with previous research (Pennington and Noble, 2009; Baxendale et al., 2001; Girolametto et al., 1993). Additionally, the participant reports on the particular effectiveness of using video feedback strategies, whereby caregivers and children are videoed interacting together to assist their learning, are consistent with previous research finding that using video modelling in EI has positive caregiver outcomes (Mendelsohn et al., 2007). Further research into the benefits of using video feedback strategies more broadly within EI settings and activities as a method of engaging caregivers actively in their own and their child’s learning may be warranted.
These findings are consistent with a transactional theory of interaction and are relevant to EI practice in that they lend further support to the benefit of caregiver-led language interventions that are aimed at supporting caregivers in developing their knowledge and confidence in using responsive communicative approaches. The findings of this study indicate that additional individual sessions aimed at further developing and maintaining the benefits of the ITTT program may be a useful extension of current practices.
1 Limitations
There are a number of limitations to this study. Firstly, the sample size is small. This considerably limits the generalizability of the findings. Due to the small sample size, the analysis was limited to within-group analysis. Research with a larger sample size enabling between-group comparisons would enable further consideration of the impact of the approach employed in this study. At present the results can be considered to be encouraging rather than conclusive, based on the small sample size. Nonetheless, these findings have implications for further research and support earlier suggestions that additional individual sessions with caregivers may optimize the outcomes of the ITTT program.
While a randomized control design was used for phase two of this study, due to ethical considerations, phase one did not include a control group. Comparison with naturally occurring wait groups may be one way to address these ethical issues whilst providing a no-treatment control group. A within-participants design entailing a wait-time for all participants would be another possible method of addressing this issue. As noted above, while there were important benefits of undertaking this research within existing EI services, including the direct connection between research and practice, the fact that a measure of child language development was not included in the study is a limitation that could be addressed in future research. Additionally, it is important to note that the variability in pretest scores may have limited the change possible for the participants with higher scores. Future research using a matched case design may provide further insight into the precise point at which the intervention is most beneficial.
While caregivers were surveyed at the completion of their participation in this study, caregiver views were not explored deeply. Further research considering caregiver perspectives, particularly regarding the additional individual sessions, is warranted.
2 Conclusion
The present study builds on existing research by providing additional evidence that the ITTT program can foster positive changes in child and adult communication interactions. Moreover, the phase two findings provide promising evidence to suggest that additional individual sessions with a SLT following on from the completion of the ITTT program may enhance the intervention outcomes. Further research is warranted.
Footnotes
Acknowledgements
Our thanks to the children, families and early intervention staff who participated in this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:Partial funding for this research was provided by the Ross Trust and SPOTonDD.