
Abstract
While little is known about why children make speech errors, it has been hypothesized that cognitive-linguistic factors may underlie phonological speech sound disorders. This study compared the phonological short-term and phonological working memory abilities (using immediate memory tasks) and receptive vocabulary size of 14 monolingual preschool children with phonological delay with individually matched peers with typical speech development. The immediate memory tasks examined forward recall of familiar words (pointing response), reverse recall of familiar words (pointing response), and reverse recall of digits (spoken response). The results indicated that children with typical speech development had larger receptive vocabularies and performed significantly better than children with phonological delay on all immediate memory tasks. Qualitative error analyses revealed that while the two groups made similar errors on the forward memory task, children with phonological delayed performed differently on reverse recall of spoken digits. These findings suggest a link between immediate memory and delayed phonological development.
Keywords
I Introduction
While much is known about the types of speech errors children make when learning to talk, little is known about why they make the errors they do. Consequently, it is difficult to answer parents when they question why their child’s speech is not developing normally. Two simplistic explanations are that the child’s speech sound disorder (SSD) is due to ‘listening’ problems or oro-motor difficulties. However, the nature of childhood SSD of unknown origin is far more heterogeneous than these two explanations suggest. There is a need, then, to investigate the underlying nature of the speech difficulties.
Stackhouse and Wells (1997) modelled the speech processing chain from sensation to motor output, identifying component skills underpinning speech development. Dodd (1995/2005) compared the speech processing abilities of five SSD subgroups according to the nature of their speech errors. The subgroups identified were:
articulation disorder, i.e. mislearnt motor program for speech sounds, e.g. lisp;
phonological delay, i.e. use of error patterns typical of children of a younger chronological age such as in English, ‘fronting’, ‘stopping’, ‘cluster reduction’;
consistent phonological disorder, e.g. atypical error patterns in English such as ‘initial consonant deletion’, ‘backing’, ‘intrusive consonants;
inconsistent phonological disorder, e.g. show at least 40% variability; and
childhood apraxia of speech (comprising < 1% of children presenting with SSD of unknown origin).
Both research approaches indicate that children with SSD have different underlying deficits, ability profiles, and intervention needs.
The term ‘phonologically delayed’ is sometimes used generically for any child making speech errors (e.g. Lewis et al 2006). In this article, phonological delay (PD) specifically refers to Dodd’s (1995/2005) subgroup of children whose speech is characterized by consistently used error patterns typical of children of a younger chronological age, according to standardized assessment. The term ‘error pattern’ rather than ‘phonological process’, is used throughout the article to reflect common definitions of ‘process’ as an error pattern (e.g. Bowen’s website) and to explicitly reject the assumptions of innateness and motor output constraints implied by the term ‘phonological process’ (Grunwell, 1982).
Research indicates that children with PD have age appropriate phonological awareness and reading ability (Harris et al., 2011), rule abstraction and cognitive flexibility (Preston et al., 2013), auditory-visual speech perception and oro-motor skills (Dodd and McIntosh, 2008). In contrast, children who consistently use atypical error patterns do poorly on measures of phonological awareness, literacy, rule abstraction, cognitive flexibility and aspects of auditory-visual speech perception (Dodd, 2014). Suggested explanations for delayed development have included the language-learning environment and a history of fluctuating hearing loss (Dodd, 2011). Other studies have suggested that specific cognitive-linguistic processes such as phonological short-term memory (pSTM) and phonological working memory (pWM) may play a role in phonological development (Adams and Gathercole, 2000), and that children with SSD demonstrate poorer pSTM abilities than their peers with typically developing speech (TDS; e.g. Eaton, 2014). To our knowledge, no studies have investigated pSTM and pWM in children only making typical but delayed errors.
1 Phonological short-term memory and speech development
Phonological short-term memory is the ability to retain (‘hold’) verbal information briefly (Archibald and Gathercole, 2006). pSTM tasks (e.g. serial recall of words, letter, numbers) have high storage and low processing demands. Evidence supports the role of pSTM in new word learning and speech development in general (Baddeley et al., 1998). According to the Baddeley and Hitch (1974) working memory model, the phonological loop supports pSTM ability. Moreover, the phonological loop, which consists of a rapid-decaying phonological short-term store and a subvocal rehearsal mechanism, is intrinsically involved in learning the phonological forms of words and the rules that govern how lexical and sublexical units can be combined. Gathercole and Adams (1993) argue that ‘phonological memory skills are intimately linked with aspects of speech production in early childhood’ (p. 777), with short-term memory deficits leading to difficulties establishing accurate phonological representations, and therefore speech output errors. If Gathercole’s phonological loop hypothesis is correct, then children with PD should have reduced pSTM abilities and reduced long-term representations (receptive vocabulary).
Alternatively, the phonological loop may be part of the speech production system (Keren-Portnoy et al., 2010). Keren-Portney et al. (2010) argue that the phonological loop serves both receptive and productive functions, and develops along with a child’s ability to segment speech into syllables; categorize speech sounds; and plan and execute spoken words. According to Keren-Portney et al. (2010), speech production practice drives phonological loop (pSTM) development, rather than pSTM ability underlying speech development.
2 Phonological working memory and speech development
Working memory (WM), the ability to temporarily store and mentally manipulate information, allows humans to: (1) consider alternatives, (2) incorporate new information and mentally update knowledge, (3) derive general principles, (4) identify relationships between ideas, and (5) perform critical reasoning (Diamond, 2013). Working memory is also an ‘updating’ system. True WM tasks involve both a ‘holding’ component and, most importantly, a significant ‘manipulation’ component, and include tasks such as repeating digits in reverse order (Diamond, 2013).
Baddeley (1986) argues that pWM tasks (i.e. tasks that involve simultaneously storing and processing verbal information), tap both the phonological loop (for ‘holding’ verbal information) and the central executive. The central executive is purportedly responsible for a range of cognitive processes including selective attention and inhibition, cognitive shift, and activation of long-term memory (Archibald and Gathercole, 2006). pWM, may be implicated in speech development by updating phonological representations of words that allow a child to move from immature patterns to more adult-like speech. Specifically, pWM may be involved in temporarily storing and manipulating sounds while a child tries to correct error sounds (Eaton, 2014).
3 pSTM, pWM and children with SSD
Conventional pSTM assessment involves serial recall of sentence, digit, and random word list recall tasks (Couture and McCauley, 2000). Studies since 2000 (Couture and McCauley, 2000; Linassi et al., 2005) report mixed results in pSTM on word recall list and/or digit span tasks. Both studies investigated pSTM (phonological loop) in school-aged children (5;0–7;11) with phonologically-based SSD of varying severity. Couture and McCauley (2000) reported that the SSD group were sensitive to word length and phonological similarity effects but performed more poorly than controls on an unrelated word recall task. Linassi et al. (2005) reported no difference in pSTM ability regardless of SSD severity on a digits reverse task, unfortunately no control group was included in the study design, making results difficult to interpret.
More recently, the development of nonword repetition (NWR) tasks has changed the focus of pSTM assessment from serial recall tasks to the spoken repetition of nonwords, which also tap the ‘phonological loop’ (or pSTM) of the working memory model (Baddeley and Hitch, 1974). Farquharson (2012) tested school-aged children with persistent SSD (i.e. speech errors beyond eight years of age) on receptive and expressive pSTM and pWM tasks, including a nonword repetition task. Results indicated a specific phonological loop deficit. Eaton (2014) compared 20 four and five year-old children with phonologically-based SSD with 45 children with TDS. Children with phonologically-based SSD performed more poorly on a conventional forward digit span task and the nonword repetition task. Unfortunately, NWR tasks findings are difficult to interpret with children with SSD because of the potential for speech output errors to confound the results (Wells, 1995), as well as the complex nature of NWR tasks, which aside from measuring pSTM also tap phonological encoding, speech perception, and oro-motor planning abilities.
Recently, Eaton (2014) investigated pWM (Baddeley’s ‘executive component’) in preschool children with phonologically-based SSD. She reported no significant difference in performance between children with SSD and TDS controls on three pWM tasks. Low scores across the pWM tasks by all the children with TDS and SSD, however, may have obscured potential group differences. Overall, few studies have investigated immediate memory in children with SSD, and even fewer with groups of preschool children with phonologically-based SSD, even though this is the most common subtype of childhood SSD of unknown origin, which peaks during the key speech development period (three to six years of age) (Broomfield and Dodd, 2004).
4 Vocabulary development and children with SSD
There is general agreement that children with SSD have receptive vocabulary deficits (Foy and Mann, 2012). One hypothesis is that children with larger vocabularies have more adult-like phonological representations (Mody, 2003) While numerous studies (e.g. Lewis et al, 2011; Foy and Mann, 2012) have investigated receptive vocabulary in children of varying ages and severity, few studies have investigated vocabulary skills in children making typical versus atypical errors.
Preston and Edwards (2010) measured the phonological awareness and receptive vocabulary abilities of 43 children aged four to five years with typical and atypical speech errors. Results revealed that children with atypical speech errors had poorer receptive vocabularies than children with typical (but delayed) speech errors. Conversely, Dodd and McCormack (1995) compared preschool-aged children with inconsistent, typical (but delayed) and atypical (disordered) errors on a range of measures, including receptive vocabulary. Children with inconsistent errors performed more poorly on receptive vocabulary than the other three groups although the delayed group had reduced age-equivalent scores. Further investigation of the vocabulary skills of children with varying SSD subtypes is required.
5 Study aims, hypotheses, and research questions
In this study, we sought to explore potential cognitive-linguistic factors underlying delayed phonological development by investigating immediate memory and receptive vocabulary skills of monolingual preschool children with PD and TDS. Our aim was to profile pSTM and pWM abilities to determine whether these skills differ between children with PD and children with TDS.
Based on prior research, we hypothesized that children with PD would have pSTM deficits. Moreover, these pSTM/‘holding’ deficits would lead to children with PD having impaired pWM performance, because of the pWM demands of ‘holding’ words before manipulating their order. It was also hypothesized that children with PD would make different types of errors from children with TDS on pWM tasks due to deficits in short-term storage (‘holding’). Reduced receptive vocabulary was hypothesized for children with PD. Four questions were asked:
Do children with phonological delay demonstrate poorer phonological short-term memory than their typically speech developing peers?
Do children with phonological delay demonstrate poorer phonological working memory than their typically speech developing peers?
Are there differences in the types of errors made on phonological short-term memory and phonological working memory pointing tasks by children with typical speech development and children with phonological delay?
Do children with phonological delay demonstrate reduced receptive vocabulary scores compared to their peers with typically developing speech?
II Method
1 Participants
Following approval from the University of Melbourne, Human Research Ethics Committee and the National University of Singapore, Institutional Review Board, children with typical speech and speech impairments were recruited from Singaporean expatriate communities. Parents volunteered for their children to participate in the study after reading advertisements in preschool newsletters, attending parent talks or hearing about the study via word-of-mouth.
The inclusion criteria for all participants were:
monolingual English speaker;
passed a pure tone audiometric hearing screening on day of screening assessment;
standard scores > 85 on the total receptive language score of the Clinical Evaluation of Language Fundamentals Preschool 2: Australia and New Zealand (CELF-P2; Wigg et al., 2006);
an inconsistency score of less than 50% on the Diagnostic Evaluation of Articulation and Phonology (DEAP; Dodd et al., 2002);
standard score of 8 or higher on the DEAP Oro-motor Assessment; and
a complete phonetic inventory for chronological age according to DEAP norms.
Children were excluded if they had a diagnosis of Attention Deficit Disorder / Attention Deficit Hyperactivity Disorder, Autism Spectrum Disorder, cerebral palsy, Down syndrome, hearing impairment, or more than four ear infections requiring antibiotics and/or grommets between 18 months and 4 years. Children born premature (< 36 weeks gestation), of low birth weight (< 2.5 kg); or, bi/multilingual/colloquial Singapore English (CSE) speakers were also excluded. TDS participants had to obtain a percentage consonants correct (PCC), percentage vowels correct (PVC) and single versus connected speech agreement standard score of 8 or above on the DEAP Phonology subtest; produce no or only age appropriate speech sound errors (i.e. no atypical errors) as measured by the DEAP phonology subtest; and never received speech therapy. To receive a phonological delay (PD) differential diagnosis and be included in the study, each speech impaired child also needed to:
obtain a PCC standard score of 7 or below on the DEAP Phonology subtest;
present with delayed speech error patterns (i.e. error patterns used by more than 10% of children in a younger age group), which occurred at least five times across different lexical items on the DEAP Phonology subtest; and
present with no more than four atypical speech errors on the DEAP Phonology subtest.
One hundred and twelve children were volunteered, and 65 met the eligibility criteria, including 50 TDS and 15 PD. Fourteen of the fifteen PD participants completed all the required assessment tasks and were included in this study. Fourteen age- and gender-matched children were then selected from the pool of 50 eligible TDS participants. The mean age of the 14 PD participants was 4 years 4 months (range = 42 months to 71 months; SD = 8.2 months), and included 11 males and 3 females, while the mean age of the 14 TDS participants was also 4 years 4 months (range = 44 months – 68 months; SD = 7.5 months) with an identical boy:girl ratio. The mean PCC of the children with PD was 72.6% (45.4–85.1%; SD 11.7), and the mean PCC of the children with TDS was 93.4% (range = 85–100%; SD 4.8). Thirteen of the 14 children with PD had never received speech therapy, while one child had undergone an initial assessment and two hours of therapy. All the participants resided in Singapore in intact family units and attended a minimum of three half days a week of formal preschool. Parents came from a range of backgrounds: 42.9% Australia; 23.2% United Kingdom; 17.9% New Zealand; 7% North America; 3.6% South Africa; 3.6% India; and 1.8% from Singapore. All children were from middle to high SES (socioeconomic status), based on fathers’ employment and mothers’ education. All mothers of the children with TDS held a University qualification, as did 13/14 (92.9%) mothers of children with PD.
2 Procedure
Study participants were part of a larger project investigating the broader cognitive and executive functioning profile of children with SSD. This article reports only the pSTM and pWM abilities, receptive language and speech assessment results of children with PD and their matched TDS peers. First, a parent-screening telephone interview was completed to exclude children who failed to meet inclusion criteria and to determine the parent’s impression of their child’s overall speech (e.g. difficult to understand or typical for age). Thirteen children were excluded during this screening process. Ninety-nine eligible children then participated in a 45-minute individual, home-based speech and receptive language assessment. The DEAP screener, DEAP phonology subtest, the PPVT-4 (Dunn and Dunn, 2007) and the CELF-P2’s three receptive language subtests were administered. Four children were excluded for a CELF-P score below 85. The DEAP quantitative and qualitative analyses were used to differentially diagnose the children into (1) typical speech; (2) phonological delay; (3) phonological disorder; (4) inconsistent disorder; or (5) articulation disorder. Fifty children with TDS and 15 children with PD were identified. These 65 eligible children were offered an assessment of pSTM and pWM abilities. Sixty-four parents consented.
Over two further 45 minute sessions, 64 children completed the immediate memory tasks, interspersed with other assessment tasks for the larger study. Children completed a pointing forward memory task first, followed by a reverse memory-pointing task in one session. In a separate, counterbalanced session, children completed a spoken digits reversed task. One third of the participants were video recorded and rescored by the first author. The data were also inspected and discussed with a speech-language therapist with expertise in memory research
a Phonological short-term memory
To accurately measure pSTM, a non-speech response task is needed, given that children with PD have reduced intelligibility that may cause examiner scoring errors. As no standardized pSTM assessments were suitable because of speech output requirements, a pointing span task (Items Forward) was constructed. The examiner first showed the child 10 black and white line drawings of common, monosyllabic nouns (selected from animal, clothing, household items and transport categories from an early child visual dictionary; different initial sound) naming each picture and encouraging the child to repeat the word. Next, the examiner explained she would say some words and the child’s task was to point to the pictures in the same order as the examiner. The first trial page (measuring 295 mm × 210 mm, i.e. A4 size) was presented, covered by an A4 sheet of black cardboard; the examiner spoke the trial sequence at one word per second; then removed the cardboard and the child pointed to the pictures. Four practice trials and up to 25 test trials followed the same procedure. The number of items to be sequentially recalled increased from two to eight incrementally. For each trial, once the spoken list was presented, children saw a picture grid of 2–8 target pictures and 0–4 foils. Picture size (4 mm × 40 mm) and position were held constant across all trial items. Testing ceased after six consecutive errors (for test format, see Appendix 1).
b Phonological working memory
Two pWM tasks were completed: (1) a pointing response task (Items Reversed), and (2) a spoken response task (Numbers Reversed). Both tasks included a ‘holding’ and ‘manipulating’ component (Diamond, 2013).
Items reversed (pointing): Difficulties measuring and scoring children with reduced speech intelligibility led to a second classic pointing task being constructed. The Items Reversed task has a similar format to the Items Forward task except for a new set of 10 familiar words, and the child pointing to the test pictures in reverse order. Again, the child was shown 10 black and white fine-line drawings, was told their names, and encouraged to repeat them. Then, the examiner explained she would say some words and the child’s task was to point to named pictures in backwards order. Practice items ensured the child understood the task. Testing began once children demonstrated they understood ‘backwards’. Items were spoken at one word per second, initial trials having two items, increasing to six. Removal of the black cardboard revealed a picture grid (2–8 target pictures, and 0–4 foils), signalled the child to point to the named pictures in reverse order. Testing ended after six consecutive incorrect responses. The Reverse Items format appears in Appendix 1.
Numbers reversed: The standardized Numbers Reversed subtest from Woodcock–Johnson III Tests of Cognitive Abilities (WJ-III) (Woodcock et al., 2007) was administered to measure spoken pWM. The examiner told the child she would say some numbers and his or her task was to remember the numbers and repeat them aloud in backwards order. Initially, the child had to remember and manipulate two numbers, and after a block of 5 trials, the number increased to 3, then after blocks of 4 trials, to 4, 5, and finally 6 items. The Woodcock–Johnson III manual instructions, cut-off, and scoring rules were followed.
3 Data analysis
Matched-pair t-tests were used to answer three research questions. An error analysis, identifying the type and number of errors according to group (TDS versus PD) across the three immediate memory tasks, were also completed. Bonferroni adjustments were not made for a number of reasons: (1) the robust study design of carefully matched pairs; (2) specific testing of separate, unrelated hypotheses; and (3) to avoid inflating type II errors (see Perneger, 1998).
III Results
Table 1 provides descriptive statistics for the speech and language measures for the children with TDS and PD. Table 2 provides descriptive statistics for the immediate memory tasks for the children with TDS and PD.
Descriptive statistics for all speech and language assessment measures.
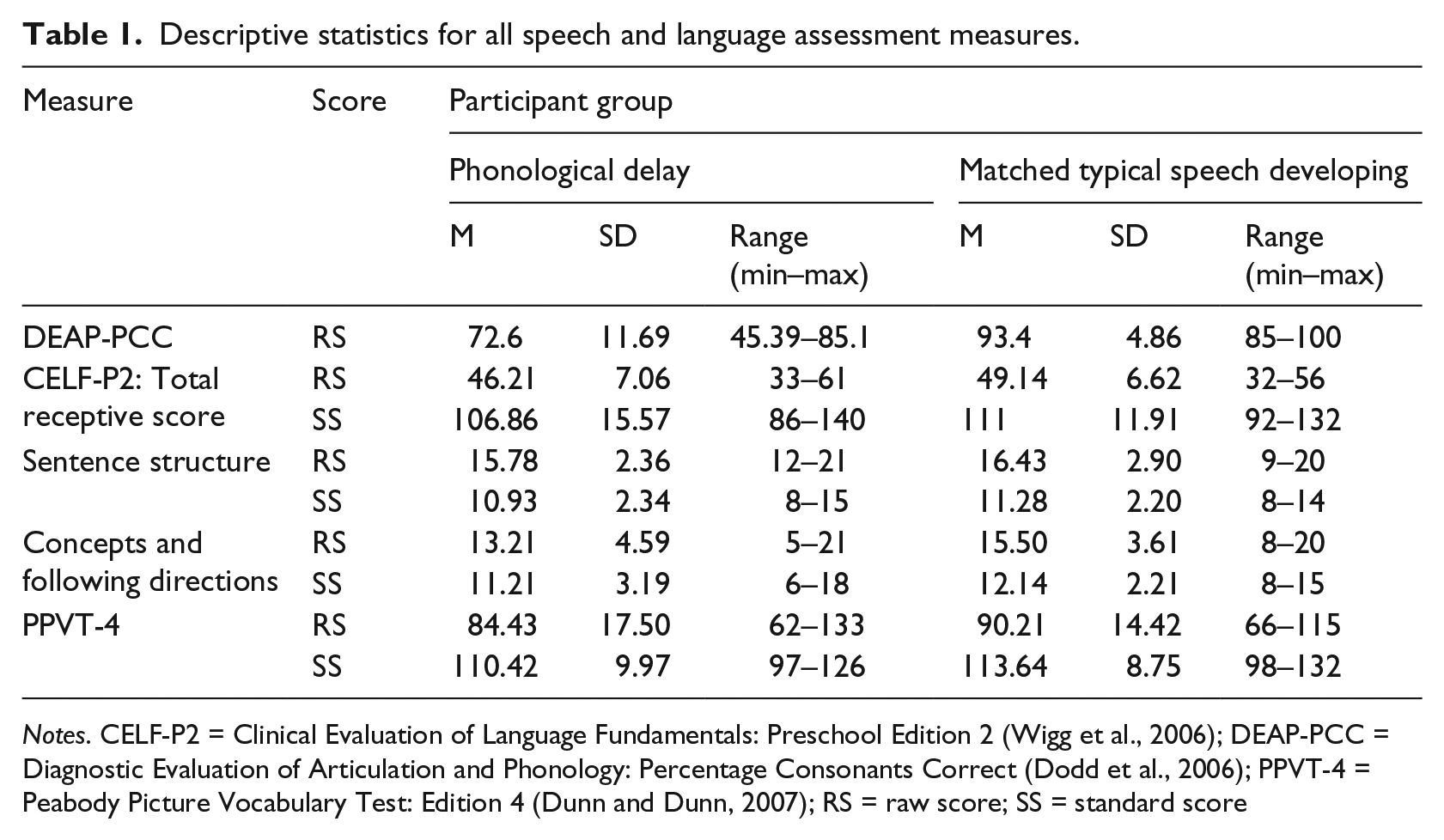
Notes. CELF-P2 = Clinical Evaluation of Language Fundamentals: Preschool Edition 2 (Wigg et al., 2006); DEAP-PCC = Diagnostic Evaluation of Articulation and Phonology: Percentage Consonants Correct (Dodd et al., 2006); PPVT-4 = Peabody Picture Vocabulary Test: Edition 4 (Dunn and Dunn, 2007); RS = raw score; SS = standard score
Descriptive statistics for immediate memory assessment measures.
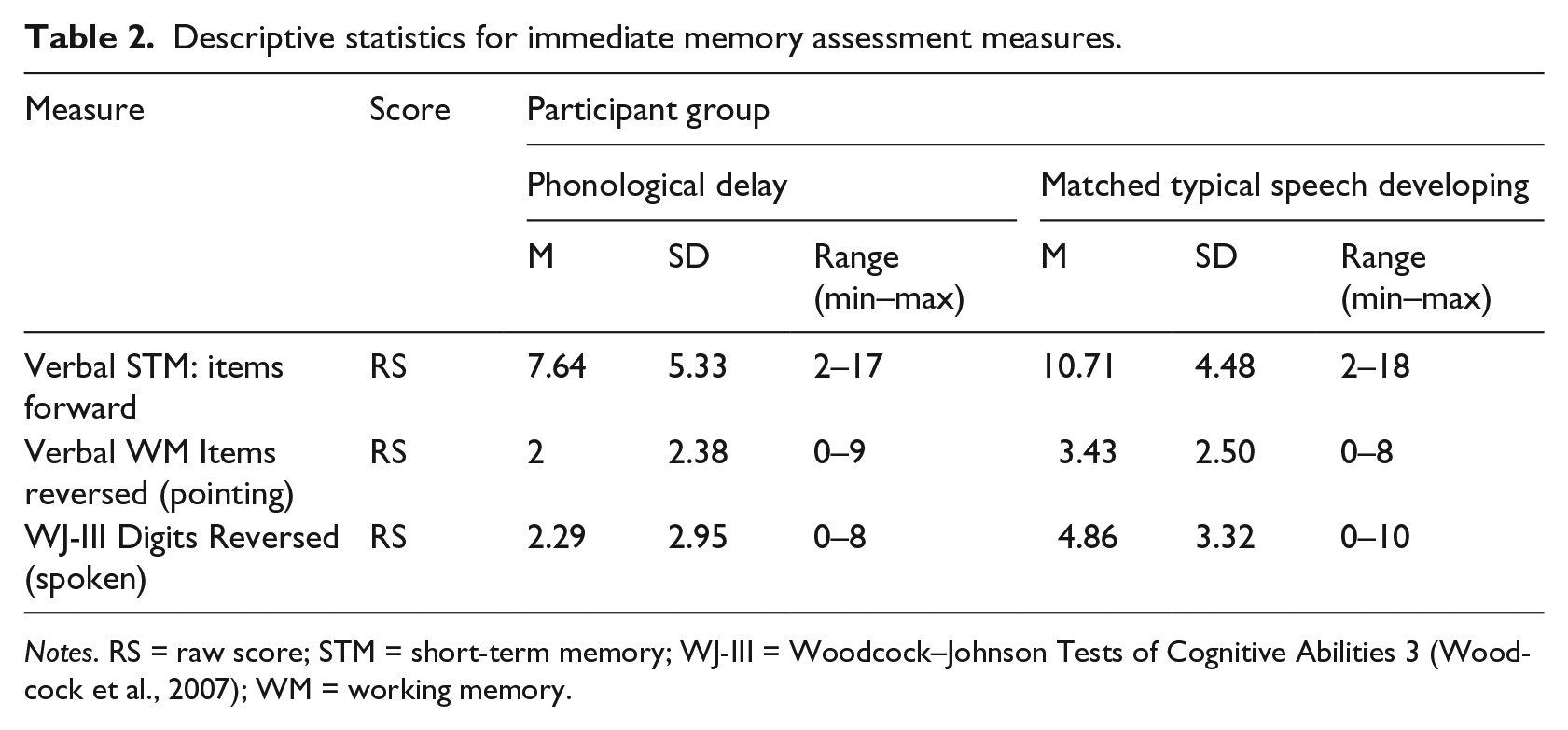
Notes. RS = raw score; STM = short-term memory; WJ-III = Woodcock–Johnson Tests of Cognitive Abilities 3 (Woodcock et al., 2007); WM = working memory.
1 Do children with PD demonstrate poorer phonological short-term memory than their peers with TDS?
A one-tailed matched samples t-test compared the average difference in forward items (pointing) scores in children with TDS and children with PD. There was a significant difference in the average difference in scores for children with TDS and children with PD (t(13) = 1.89, p = 0.04). The results suggest that children with TDS have better forward memory abilities than children with PD.
2 Do children with PD demonstrate poorer phonological working memory than their peers with TDS?
Two one-tailed matched samples t-tests were conducted to compare the average differences of the two phonological working memory scores in children with TDS and children with PD. There was a significant difference in the average difference in Items Reversed (pointing) scores for children with TDS and children with PD (t(13) = 2.59, p = 0.011). There was also a significant difference in the average difference in Numbers Reversed (spoken) scores for children with TDS and children with PD (t(13) = 2.665, p = .0095). This result was not surprising given the dependence of working memory on the ‘holding’ component (STM).
Next, the average difference between pSTM (forward pointing) and pWM (reverse pointing) was calculated as a measure of ‘manipulating ability.’ On average, children with TDS were able to hold 4 items in pSTM and manipulate 2.3 items in working memory (1.64 difference), while children with PD could hold 3.4 items in STM and manipulate 1.8 (1.57 difference). A matched pairs t-test revealed that the average difference in scores was not significant (t = –.179, df = 13, p = .861 two-tailed), suggesting the ‘manipulating ability’ of children with PD was similar to that of the children with TDS. The significantly reduced score on the pointing pWM task may have been due to ‘holding deficits’ rather than deficits manipulating auditory units in working memory. Combined results suggest that while the children with PD appeared to have poorer working memory abilities than the children with TDS, this was because of the STM deficits and not because of difficulties manipulating information.
3 Are there qualitative differences in the types of errors made by children with TDS and those with PD on working memory tasks that require a pointing response versus a spoken response?
Qualitative error analyses of the two reverse memory tasks revealed a difference between children with TDS and those with PD on the spoken digits reverse task but not the pointing reverse task. On the pointing task, both groups of children mostly made ‘no response’ errors, followed by ‘partial reversals’, ‘forwards’, and ‘incomplete’ errors. ‘No response’ errors were given most often when the number of items was above the child’s span threshold, whereas ‘partial reversals’, where at least one item appeared along with other required items in the correct position, occurred when the child could ‘hold’ the number of items in STM but could not complete the full manipulation of items. On the spoken digits reverse task, children with PD made predominately ‘forwards’ errors (51%), followed by ‘partial responses’ (20%) and ‘incorrect items’ (11%), whereas children with TDS had a more even spread of errors, with the ‘forwards’ and ‘partial errors’ evenly matched. Figures 1 and 2 provide a summary of percentage errors types by speech group. These results may indicate that children with PD may be impulsive (i.e. could not inhibit a forwards imitation response) on spoken tasks when over- learned, automatic words are used.

Percentage error types by speech group: Items reversed (pointing).

Percentage error types by speech group: Digits reversed (spoken).
4 Do children with PD demonstrate reduced receptive vocabulary stores compared to their peers with TDS?
A one-tailed matched samples t-test was conducted to compare the average difference in receptive vocabulary scores in children with TDS and children with PD. There was a significant difference in the average difference in scores for children with TDS and children with PD (t(13) = 1.89, p = 0.04). These results suggest that children with TDS have larger receptive vocabularies than children with PD.
IV Discussion
Previous research (e.g. Eaton, 2014) has implicated pSTM and pWM as predictors of speech errors in a group of children with undifferentiated phonologically-based SSD. This study compared the pSTM and pWM abilities and receptive vocabulary size of monolingual preschool children with phonological delay with individually matched peers with typical speech development. The immediate memory tasks examined forward recall of familiar words (pointing response); reverse recall of familiar words (pointing response) and reverse recall of digits (spoken response). The results indicated that children with TDS had larger receptive vocabularies and performed significantly better than children with PD on all tasks. Qualitative error analyses revealed that while children with TDS and PD made similar errors on pointing tasks, children with PD performed differently on reverse recall of spoken digits. These findings suggest that children with PD have reduced pSTM and pWM abilities, compared to their peers with TDS.
When children were asked to point to items in sequential order, children with PD performed more poorly than their peers with TDS. This result is consistent with the results reported by Eaton (2014), Farquharson (2012), and Linassi et al. (2005), who used a combination of NWR and conventional recall tasks with children with a range of SSDs (e.g. phonologically-based; undifferentiated speech and language disorders; persistent speech disorder). This evidence suggests that preschool-aged children with PD have difficulties ‘holding’ phonological information in short-term memory.
Children also completed two reverse memory tasks to determine if there were any ‘manipulating’ ability differences between children with TDS and children with PD. In both tasks, children with PD performed significantly worse than their matched peers with TDS. However, given that the group of children with PD demonstrated reduced pSTM performance, this result was not surprising, since pWM requires both ‘holding’ (pSTM) and ‘manipulating abilities’. To address ‘manipulating ability’, the difference between pSTM span and pWM span was calculated. There was no difference between PDs and TDS when only ‘manipulating’ was considered. This result is consistent with Eaton (2014) who reported no difference in pWM between preschool-aged children with typical and phonologically-based SSD. This study’s findings suggest that while children with PD may appear to perform poorly on pWM tasks, this is probably due to pSTM deficits rather than difficulties manipulating verbal information per se.
Qualitative analyses revealed that children with TDS and children with PD made similar types of errors on the pointing tasks but not the spoken digits reversed task. On the digits reversed task, children with PD were more likely than children with TDS to give a forwards response (instead of inversing items) or include incorrect items whereas children with TDS were more likely than children with PD to give a partial reversal (i.e. inverse at least two numbers) or not respond. The types of errors children with PD made suggests an impulsive response pattern, which may be implicated in SSD. Specifically, children with PD may struggle to inhibit early mental word templates, making it difficult to transition to more adult-like speech.
Treatment studies (e.g. Cummings and Barlow, 2011) have demonstrated that using non-words over known-words in therapy leads to greater improvement perhaps, because children with SSD do not have to inhibit ‘old’ forms. However, Eaton (2014) who directly investigated inhibition in children with phonologically-based SSD, reported no difference in inhibition between controls and a SSD group. This may have been because the assessment tasks measured lexical–semantic inhibitory control and not phonological inhibitory control. Further investigation is required to understand the role of inhibition control in SSD.
pSTM and vocabulary size are reportedly associated (e.g. Gathercole and Baddeley, 1989; Gathercole, et al., 1999). Dodd and colleagues (2005) reported no difference in the vocabulary size of children with PD compared to children with TDS. In this study, the PPVT-4 scores for the children with PD while in the average range were significantly lower than their matched peers with TDS. In this study vocabulary size variation was not attributable to differences in maternal education, as is typically the case (e.g. Eaton, 2014). The results provide further support for a link between PD and vocabulary size.
Unfortunately, it is impossible to determine whether the immediate memory and vocabulary deficits identified in the children with PD are the cause or the effect of delayed error patterns. Therefore, there are a number of possible explanations for the poor performance by the children with PD on the pSTM, pWM, and vocabulary tasks. First, pSTM deficits may lead to problems with vocabulary and speech development. Children who are slow to acquire an adult-like phonological system may have pSTM deficits that prevents them from ‘holding’ sufficient information in the phonological loop. The pSTM deficits then lead to pWM difficulties, as the child has a limited amount of information to manipulate in the formation of robust templates. If inaccurate phonological representations were stored in long-term memory, planning word production would include those inaccuracies. Alternatively, reduced vocabulary may lead to pSTM deficits and speech problems. Specifically, children with PD experience delayed early word acquisition, with fewer phonological representations of words than their peers. Remembering unfamiliar words might be more difficult than familiar words reflected by poorer pSTM. Delayed speech errors may reflect the smaller database (fewer mentally represented words) from which they work out their language’s phonological constraints. Finally, perhaps speech errors lead to pSTM deficits and reduced vocabulary. For example, a child hears a word said correctly, but then repeats it incorrectly via the phonological loop. Incorrect sound sequences are analysed and form incorrect templates, that are then inaccurately stored in long-term memory. There are, then, at least three ways in which pSTM might impact speech acquisition, with pSTM deficits either causally or consequentially related to PD.
V Conclusions
This study is the first to investigate pSTM and pWM in a differentiated subgroup of preschool children with phonological delay (i.e. typical but delayed error patterns only). Results indicate that PD is more than ‘surface error’ deep, with children with PD presenting with cognitive-linguistic deficits in pSTM, pWM, and receptive vocabulary. In light of building evidence, current assessment protocols for children with PD may need to incorporate immediate memory assessment. Finally, research profiling the pSTM and pWM abilities of children who make atypical phonological errors (i.e. children with phonological disorder), and inconsistent errors, is now required to determine whether pSTM deficits are implicated in all phonologically-based SSDs or only phonological delay.
Footnotes
Appendix 1
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.