
Abstract
The goals of the present study were to (1) examine the effects of the multiple opposition phonological approach on improving phoneme production accuracy in children with severe phonological disorders and (2) explore whether the multiple opposition approach is feasible for the telepractice service delivery model. A multiple-baseline, single-participant design replicated across two children, was implemented. Two male children who resided in rural areas of West Texas in the USA participated. One child was 4 years and 10 months old and the other child was 6 years old. Both of the children were diagnosed with phonological disorders without any sensory, motoric, or intellectual disabilities. The children’s articulation was tested using Goldman–Fristoe Articulation Test-2 and probes were administered across the period of the study. The children received a 30-minute phonological intervention via telepractice twice a week for 12 or 16 weeks. An increasing trend for production accuracy for target sounds was observed during intervention for both children. Maintenance also was observed at 2-week and 2-month follow-ups. Standard scores from a standardized articulation test increased during posttest compared to pretest. The multiple opposition phonological approach can lead to improved speech production accuracy in children with severe phonological disorders. Telepractice may be an effective context for a phonological intervention approach as has been found for other domains of speech and language intervention and a useful service delivery model to underserved children with speech disorders who are unable to access a speech pathologist due to various circumstances.
I Introduction
Children with speech sound disorders (SSD) have difficulty developing a phonological system and articulating phonemes correctly relative to chronological age expectations. SSD is a widespread disorder category in preschool and school age children in the USA as well as other countries. According to the US National Institute on Deafness and Other Communication Disorders (NIDCD, 2017), the prevalence of speech sound disorders in young children is 8 to 9% and approximately 5% of children demonstrate noticeable speech difficulties by the first grade. Law et al. (2000) reported that the prevalence of speech delays is highly variable in the UK, ranging from 4.6% to 24.6%. Many young children with SSD show difficulty in reading and spelling tasks as well (Bird, Bishop, and Freeman, 1995; Larrivee and Catts, 1999). Approximately 25% of children with reading disorders have a history of speech sound disorders (Scarborough, 1990; Gallagher et al., 2000; Pennington and Lefly, 2001) and 30% of children with SSD exhibit later reading disorders (Lewis, 1996). In addition, Rice, Hadley and Alexander (1993) noted that children with phonological disorders showed socialization difficulties. A recent report (Hughes, 2014) indicates that children with communication disorders have difficulties with peer relationships because of being bullied. Thus, treating children with SSD is important in order to impact the children’s risk for later language delay as well as associated academic and social difficulties.
During the last several decades, speech-language pathologists (SLPs) have implemented various linguistic-cognitive approaches to SSD interventions. These approaches include minimal pairs (Weiner, 1981), maximum opposition (Gierut, 1989, 1990), empty set (Gierut, 1991), and multiple opposition (Williams, 2000a, 2000b, 2010). Each of these approaches has evidence to support their effectiveness, however the multiple opposition approach was developed specifically to address extensive phoneme collapses which are common for children with severe phonological disorders. Phoneme collapses are a consequence of a limited sound inventory in which the child produces one sound for multiple adult target sounds resulting in a one-to-many phoneme correspondence between the child and adult sound systems. This results in severely reduced intelligibility. Using the multiple opposition approach, several target sounds are treated from across the rule set, or phoneme collapse, with the assumption that the frame of learning the child needs to achieve is increased and greater system-wide generalization will be obtained (Williams, 2006a). For example, when a child produces [d] for the target sounds /t, s, k, ʃ/ in the words such as ‘tip’, ‘sip’, ‘kip’, and ‘ship’, all of the target words are produced as a homonym [dɪp]. The multiple opposition approach targets all four error sounds from the phoneme collapse at the same time to increase the frame of learning. Consequently, speech intelligibility may increase more effectively as compared to other phonological approaches in children with severe phonological disorders. Compared to the multiple opposition approach, other cognitive-linguistic approaches may take longer to treat all of these target sounds because they typically select one target sound at a time. In spite of the proposed effectiveness of the multiple opposition approach, the effectiveness of the multiple opposition phonological approach has not been investigated widely. A very limited evidence base for multiple opposition intervention is currently available (Allen, 2013; Williams, 2000a, 2000b). Thus, further studies are warranted to evaluate if the multiple opposition approach is effective for children with severe phonological disorders.
A second critical dimension of service delivery is the setting for intervention. Telehealth is a growing new area of service delivery within our profession and is the provision of health services using communication technologies. It allows health care specialists, including SLPs, to consult and deliver assessment and treatment services in real-time across a geographic distance. The American Speech-Language-Hearing Association (ASHA) has adopted the term telepractice to indicate that telecommunication is used in various health care settings, such as medical, as well as educational settings. The importance of the telepractice service delivery model has increased because it may be a solution for the shortage of SLP service providers in schools in the USA (Mashima and Doarn, 2008). It is well documented that a substantially large number of children who need speech and language services are currently underserved due to the critical shortage of certified SLPs in public school settings in the USA (American Speech-Language-Hearing Association, 2016; Edgar and Rosa-Lugo, 2007). Given the fact that children with speech and language impairment constitute a major proportion of SLP practice (Theodoros, 2011), the shortage of school SLPs became a significant concern in the USA. These shortages may be exacerbated in rural areas (American Speech-Language-Hearing Association, 2016; Mashima and Doarn, 2008).
While a significant number of physicians have used telecommunication technology to provide medical services and a larger volume of evidence of telemedicine research is available (Ekeland et al., 2010), the volume of telepractice research involving children with speech-language disorders is very limited. Mashima and Doarn (2008) conducted a systematic review, reporting that out of 40 telepractice studies for speech-language assessment and intervention, most studies were limited to case studies. Furthermore, the majority of the studies included in their review dealt with various types of adult populations. Only one study (Waite et al., 2006) was an experimental study with children. Reynolds et al. (2009) also conducted a systematic review of telepractice for speech-language pathology and found that out of a total of 62 studies, 28 articles were sufficiently detailed to be reviewed whereas the remaining studies were non-analytic studies such as case-reports. Among the 28 studies, only five telepractice studies were evaluated as having reliable and valid data, all of which were limited to adult participants. These two systematic reviews indicate that it is critical to establish treatment effects of telepractice for children with speech and language impairment in order to evaluate whether intervention via telepractice is feasible with these children.
Recently, additional studies have been conducted to examine the efficacy of speech-language assessment and intervention via telepractice. The majority of these studies were still mainly conducted with adult populations; only a few telepractice intervention studies involving children with speech-language impairment are available (Constantinescu et al., 2014; Gabel et al., 2013; Grogan-Johnson et al., 2010, 2011, 2013; Lee et al., 2017; Wilson et al., 2004). Among these studies, only two studies (Grogan-Johnson et al., 2011, 2013) investigated the efficacy of speech intervention via telepractice for children with SSD. These two studies were based on the same dataset.
Grogan-Johnson et al. (2011, 2013) examined the effect of speech intervention via telepractice with 13 children with SSD. Seven children received speech therapy via telepractice and six children received the same therapy using the face-to-face conventional method. The authors found that children in both service delivery models made statistically significant improvement in speech sound production based on the Goldman–Fristoe Test of Articulation-2 (Goldman and Fristoe, 2000); there was no significant difference in the posttest between the two groups. In addition, production accuracy of a small number of target sounds per child was qualitatively compared between the pretests and posttests. Descriptive results indicated that production accuracy was improved in posttreatment evaluation (e.g. 80% during baseline improved to 100% posttest). The study only targeted one or two error sounds per child based on the adoption of a traditional articulation approach targeting individual phonemes. Thus, further studies are needed to validate the treatment efficacy of speech intervention via telepractice as well as investigating whether contemporary phonological approaches via telepractice lead to improvement in children with severe phonological disorders.
The purpose of the current study was twofold. A primary goal was to examine the effects of the multiple opposition phonological approach (Williams, 2000a, 2000b) on phoneme production accuracy in children with severe phonological disorders. A second goal was to explore whether this phonological approach is feasible to implement via the telepractice service delivery model. The evidence base for the multiple opposition phonological approach as well as telepractice need to be enhanced in support of SLP decision making for intervention efficacy. The findings of the study can also provide evidence to evaluate telepractice use for children in rural areas. Telepractice has been proposed as a useful model for underserved children in the USA; however, limited studies via telepractice have been conducted with children residing in rural areas.
II Method
1 Participants
As a preliminary study, three children were initially recruited from rural areas of West Texas, USA. One child was withdrawn from the study due to an internet connection difficulty during telepractice intervention. Thus, two children completed the study.
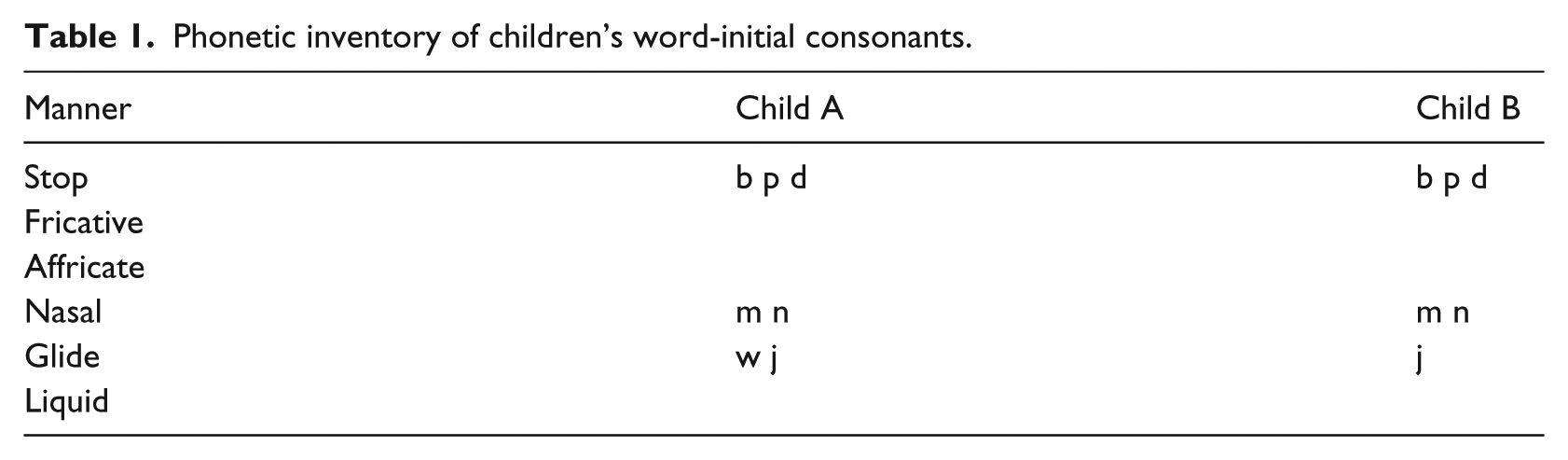
Child A was a 4-year, 10-month-old male when the pretest was conducted. The child was monolingual English-speaking with limited exposure to other languages (e.g. Spanish), residing in a small town in rural Texas, a 1.5-hour drive from a major city where intervention service would be available. The child was initially evaluated by early childhood intervention (ECI) and had received speech therapy in his town. While participating in this study, he was brought to a large city in West Texas and received speech-language services once a week for 2.5 hours in a group setting. Based on his clinic records, the child passed a hearing screening at 20 dB hearing level (HL) for each ear at 500, 1,000, 2,000, and 4,000 Hz, and an oral-motor examination was unremarkable. The child did not demonstrate any language difficulties, but showed below average articulation and phonology skills. The Clinical Evaluation of Language Fundamentals Preschool – Second Edition (CELF Preschool-2; Semel et al., 2004) revealed that the standard scores of CELF Preschool-2 (112) were within the range of 85 to 115. Standard scores of anywhere between this range is considered within normal limits. The Goldman–Fristoe Test of Articulation-2 (GFTA-2; Goldman and Fristoe, 2000) score was 2 standard deviations below the mean for his chronological age. A percentile rank of 6 indicated that he performed as well as or better than 6% of his chronological age matched peers. The child’s overall intelligibility for connected speech was highly unintelligible. The level of intelligibility was 1 based on 1 to 6 scales (Fudala, 2000). The consonant phonetic inventory of Child A is shown in Table 1. An error analysis indicated that he demonstrated a limited sound system with extensive phoneme collapses word-initially (see Figure 1). Specifically, he had complementary phoneme collapses:
1:15 phoneme collapse for non-labial and predominantly non-continuant obstruents and clusters to [d];
1:5 phoneme collapse for labial obstruents and clusters to [b];
1:8 phoneme collapse of voiceless continuants to null (Ø);
1:2 phoneme collapse of voiced continuants to [w].
Phonetic inventory of children’s word-initial consonants.

Phoneme collapse patterns in Child A.
Child B was a 6-year-old male who also resided in a small town in West Texas, located 2 hours driving distance from the major city in the area. His primary language was English and he was not exposed to other languages. Child B was diagnosed with a speech sound disorder by a local speech-language pathologist when he was 3 years of age. Since then, he had received speech intervention for 2.5 years, but little progress was observed. During the study, he did not receive speech intervention at his local school due to his speech-language pathologist being on maternity leave. He passed an oral-motor examination and a hearing screening at 20 dB HL for each ear at 500, 1,000, 2,000, and 4,000 Hz. CELF Preschool -2 and GFTA-2 indicated that the standard scores of CELF Preschool-2 (110) were within normal limits; however, those of GFTA-2 (60) were 2 standard deviations below the mean, indicating that he performed below the average. A percentile rank score indicated that he performed below 1% of his same aged peers. Similar to Child A, Child B’s overall intelligibility for connected speech was highly unintelligible. The level of intelligibility is 1 based on 1 to 6 scales (Fudala, 2000). Table 1 shows his consonant phonetic inventory in word-initial position. An error analysis indicated that his sound system was very limited in that only bilabial stops, nasals, and glide /j/ were correctly produced in word initial position, which resulted in extensive phoneme collapses (see Figure 2). Specifically, he had complementary phoneme collapses based on the major class distinction of obstruents and sonorants;
1:22 phoneme collapse of non-labial obstruents and clusters to [d];
1:5 phoneme collapse of labial obstruents and clusters to [b];
1:4 phoneme collapse of sonorants to null (Ø).

Phoneme collapse patterns in Child B.
2 Study design and goal selections
The current study used a multiple baseline single-participant experimental design across behaviors replicated in two participants. A single-participant design with replication across children is commonly used to demonstrate effectiveness of behavioral interventions (Richards et al., 1999). As Kratochwill et al. (2010) suggested, the current study included three experimental behaviors (three groups of target sounds) for each participant in order to demonstrate an intervention effect. A group of target sounds were selected based on the child’s phoneme collapse patterns. For Child A, word initials /k, dʒ/ were treated first (Phase I) followed by word initials /tʃ, t/ (Phase II) and then initials /f, s/ (Phase III). For Child B, word initials /k, dʒ, tr/ were treated first (Phase I). Then, initials /s, g, kl/ (Phase II) and /tʃ, t, sl/ (Phase III) followed, respectively.
Baseline condition probe assessment consisted of 30 words that have the target sound in word initial position (5 words for each target sound; six targets) for Child A, and 45 words for Child B (5 words for each target sound; nine targets). Five baseline pretreatment probes were established for each child. For experimental condition probe assessments, three monosyllable words per each target sound were randomly selected to measure treatment effects on treated sounds and to monitor untreated sounds. A total of 18 probes for Child A and 24 probes for Child B were used. Because the words were not targeted during intervention, these probes were used as a measure of generalization to untreated words. The probes were administered via direct imitation without feedback at the end of every other session (once a week) during the last five minutes of intervention. The direct imitation technique is commonly used in the speech pathology profession where the child is asked to repeat what he or she hears (Hegde and Gierut, 1979). To avoid possible threats to internal validity in multiple probe design, the order of these experimental condition probes was randomized.
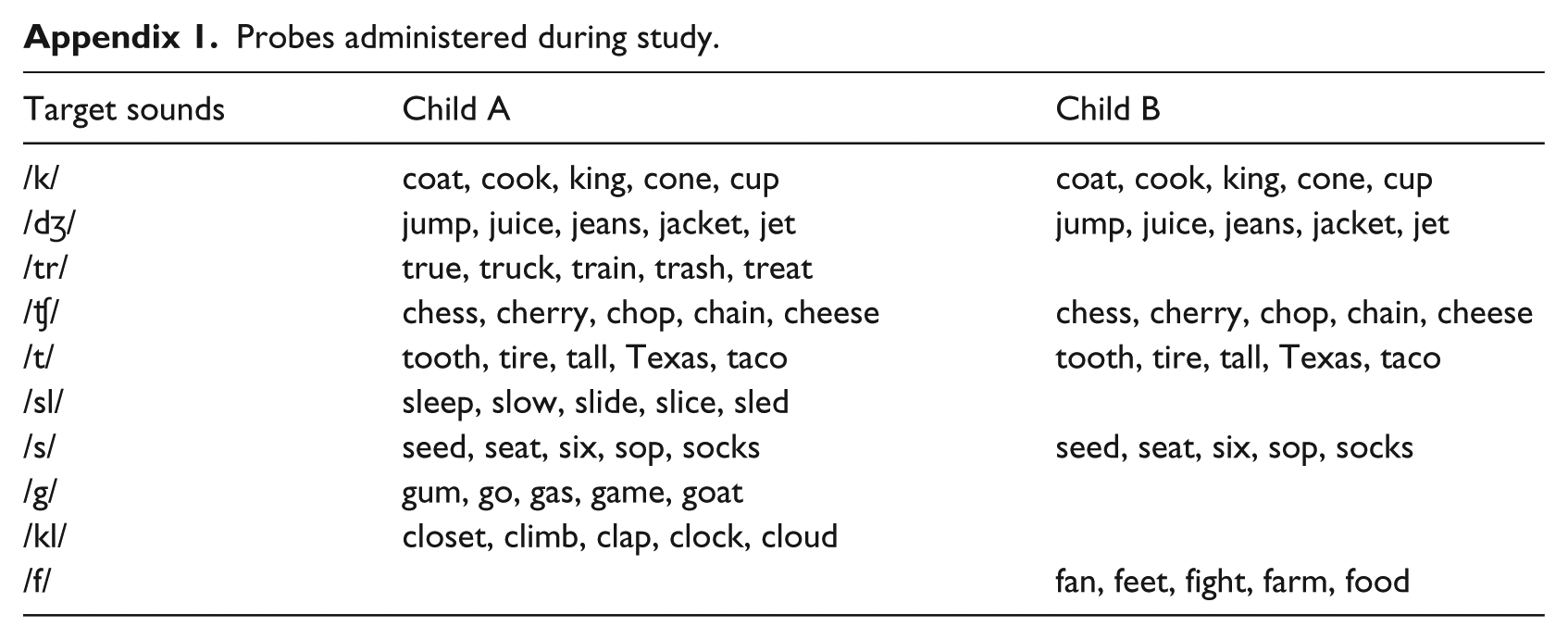
Following five baseline probes, the first target group was treated and the remaining target groups were untreated. Treatment of the second target group began four to five weeks after the first target group was treated. Each target group was treated until at least a target sound of a target group reached 100% accuracy. After the end of the treatment period, the 30- or 45-word probes were re-administered at 2-week and 2-month follow-ups to evaluate maintenance of any gains made in intervention. The GFTA-2 was also re-administered 2 months after the intervention was completed. Appendix 1 provides an example of the probes used during baseline, experimental condition, and maintenance condition. The child’s productions elicited using probes were identified as ‘correct’ or ‘incorrect’ by an SLP graduate student who was blind to the study goals as well as participants. Another SLP graduate student with no knowledge of the study or participants transcribed 10% of the production independently. Transcription reliability between the two transcribers was 83.5% for Child A and 86.2% for Child B. This level of agreement was similar to previous studies in that SLP students participated as raters for the speech intervention study (e.g. McAllister Byun and Hitchcock, 2012). All disagreements were discussed and the raters resolved discrepancies.
3 Treatment procedures via telepractice
Treatment was provided by a SLP intern supervised by a certified SLP. The clinician implemented telepractice intervention at the Telepractice Research Lab at a university in Texas. The children received intervention at each participant’s home. Before intervention, primary caregivers received intensive training in a face-to-face training session on how to use the telepractice platform, how to assist the child during intervention, and basic troubleshooting. Then, the clinician and caregiver had an online practice session to resolve any technical difficulties. Once the caregivers felt confident using telepractice procedures, intervention via telepractice began. Two training sessions (one face-to-face and one online) were sufficient for both caregivers. The telepractice platform selected for the current study was Presencelearning.com; this platform is available online at http://www.presencelearning.com (accessed January 2018). The platform allows dynamic interaction between a clinician and a client using various games and manipulative hands-on activities. Primary caregivers logged into a telepractice platform for her child using a computer and assisted the child during intervention. Treatment sessions were scheduled twice a week for 30 min. each. Since Child A did not attend a school, treatment was provided during daytime whereas Child B received intervention after school.
All treatment materials were made using the Sound Contrast In Phonology (SCIP; Williams, 2006b) software. This program was useful to generate sets of contrastive word pairs for each group of target sounds. Three sets of contrastive word pairs for each phoneme collapse pattern were used during intervention. Examples of the contrastive word sets for Child A consisted of ‘Day, K, J’ for Phase I, ‘Dew, Chew, Two’ for Phase II, and ‘Dye, Sigh, Fie’ for Phase III. Examples of the contrastive word sets for Child B was composed of ‘Day, K, J, Tray’ for Phase I, ‘Dew, Sue, Goo, Clue’ for Phase II, and ‘Dew, Two, Chew, Slew’ for Phase III. It is important to treat across error patterns instead of training each error in isolation using a multiple opposition approach (Williams, 2000a). Thus, the treated sounds were always presented in the contrastive words with the error production in order to help the children develop phonemic contrasts and support reorganization of their phonological system.
During intervention, a first goal was to ensure the child’s receptive understanding of each target word. Once the child was able to identify each target word by circling the corresponding picture using a mouse, or pointing to the computer screen (as indicated by the caregiver), the intervention focused on the difference between the contrastive pairs, which were presented on the screen. For example, when the child produced a homonym for the contrasting pairs, the clinician gave feedback with an emphasis on the difference between the two words (e.g. ‘the two words you said sound the same’ or ‘make each word sound different’). Various contrasting activities were utilized during intervention. For most sessions, the children either imitated or spontaneously produced the contrasting pairs. A total of 24 treatment sessions (12 weeks) for Child A and 32 sessions (16 weeks) for Child B were provided by the time the study was completed. Telepractice sessions were recorded using Camtasia software.
III Results
1 Child A
Figure 3 shows Child A’s production accuracy of each target sound of each target group. The top panel shows production accuracy for target group 1 (/k, dʒ/), the middle panel is production accuracy for target group 2 (/ʧ, t/), and the bottom panel shows production accuracy of target group 3 (/f, s/). Five baseline probes for each target group were obtained. Baseline results indicated that Child A produced all target sounds with 0% accuracy except for two target sounds. During the second baseline probe, Child A correctly produced /k/ and /dʒ/ once, resulting in 20% accuracy for target group 1 (1 correct out of 5 probes each). Beyond the probes, Child A produced all target initial sounds /k, dʒ, tʃ, t, f, s/ with 0% accuracy. Once solid baseline data were obtained, the initials /k, dʒ/ were treated during the Phase I experimental condition. Child A correctly produced /k/ once during probes 7 and 9 whereas the other target sound /dʒ/ was not produced correctly at all during this experimental condition. While target group 1 was treated, only the /t/ sound of target group 2 was produced with 33% accuracy (1 correct out of 3 probes) during probe 7 and all target sounds of target group 3 were produced with 0% accuracy.

Percentage of correct production of probes in Child A.
After target group 1 was treated for four weeks, target group 2 was treated simultaneously with target group 1 during the Phase 2 experimental condition. A dramatic increase was observed for target sound /k/ during probe 11 and 12 where it was produced with 100% accuracy (3 correct out of 3 probes); however, the target /dʒ/ sound was still produced with 0% accuracy. Correct productions of target group 2 sounds were also observed once these sounds were treated. During probes 11 and 12, /t/ was produced with 66% accuracy whereas /ʧ/ was produced with 33% accuracy. During probe 13, the target /ʧ/ sound was produced with 100% accuracy and the target /t/ was produced with 100% accuracy during probe 14. Untreated target group 3, on the other hand, was produced with 0% accuracy during the Phase II experimental condition except for probe 13 where /s/ was produced with 33% accuracy.
The Phase III experimental condition began when production accuracy for target group 2 reached 100% accuracy. Within a week, both target sounds of target group 3 were produced with 100% accuracy. Although a regression for production accuracy of /s/ was observed during probes 16 and 17, production accuracy for the /f/ sound maintained 100% accuracy during the Phase III experimental condition. The two untreated target group 1 and 2 sounds were also maintained with over 50% accuracy although production accuracy of the /dʒ/ sound remained 0% until the end of intervention.
A 2-week maintenance probe revealed that Child A produced /k/ and /f/ with 100% accuracy, and /t/ and /dʒ/ with 80% accuracy. The /s/ and /tʃ/ phonemes were produced with 60% accuracy. A 2-month follow-up probe, however, showed an improvement in the two affricate sounds. The child produced all sounds with 100% accuracy except for dʒ/ and/s/. The /s/ sound was produced with only 60% accuracy. The GFTA-2 was re-administered at 2-month follow-up. The standard scores indicated that his productions were 1.5 standard deviations below the mean expected for his chronological age. Most singleton consonants were produced correctly except for /r, s, ɵ, ð/ at word initial position. /r/ was produced as /w/, inter-dental fricatives were produced as either /t/ or /f/ and /s/ was dentalized. Most errors occurred in consonant clusters, showing a consonant cluster deletion process (e.g. /bl/ → [b]) or substitution process for all consonant clusters including /r/ (i.e. /br, dr, fr, gr, kr, tr/). All /r/ clusters were produced with /w/. Only two consonant clusters such as /kw/ and /sp/ were produced correctly. The /dr/ and /tr/ clusters were produced as /dʒ, tʃ /, respectively. The overall intelligibility for his connected speech during the maintenance session was greatly improved. Based on a 1 to 6 scale (Fudala, 2000), his overall intelligibility was 2, that is, his speech was intelligible, although there were noticeable errors.
2 Child B
Figure 4 shows Child B’s production accuracy of each target sound of each target group. The top panel shows production accuracy for target group 1 (/k, dʒ, tr/), the middle panel is production accuracy for target group 2 (/s, g, kl/) and the bottom panel shows production accuracy of target group 3 (/ʧ, t, sl/). As in Child A, five baseline probes for each target group were obtained and showed that all target sounds were produced with 0% accuracy. The initial /k, dʒ, tr/ sounds were treated during Phase I experimental condition. During five weeks, none of target group 1 sounds were produced with 100% accuracy. Child A produced /k/ with 33% accuracy and /tr/ with 66% accuracy during probe 8 and 9. However, the /dʒ/ sound was not produced correctly at all during this period. While target group 1was treated, target group 2 was produced with 0% accuracy whereas the /t/ sound for target group 3 was produced with 66% accuracy during probe 6 and 33% accuracy during probe 8–11.
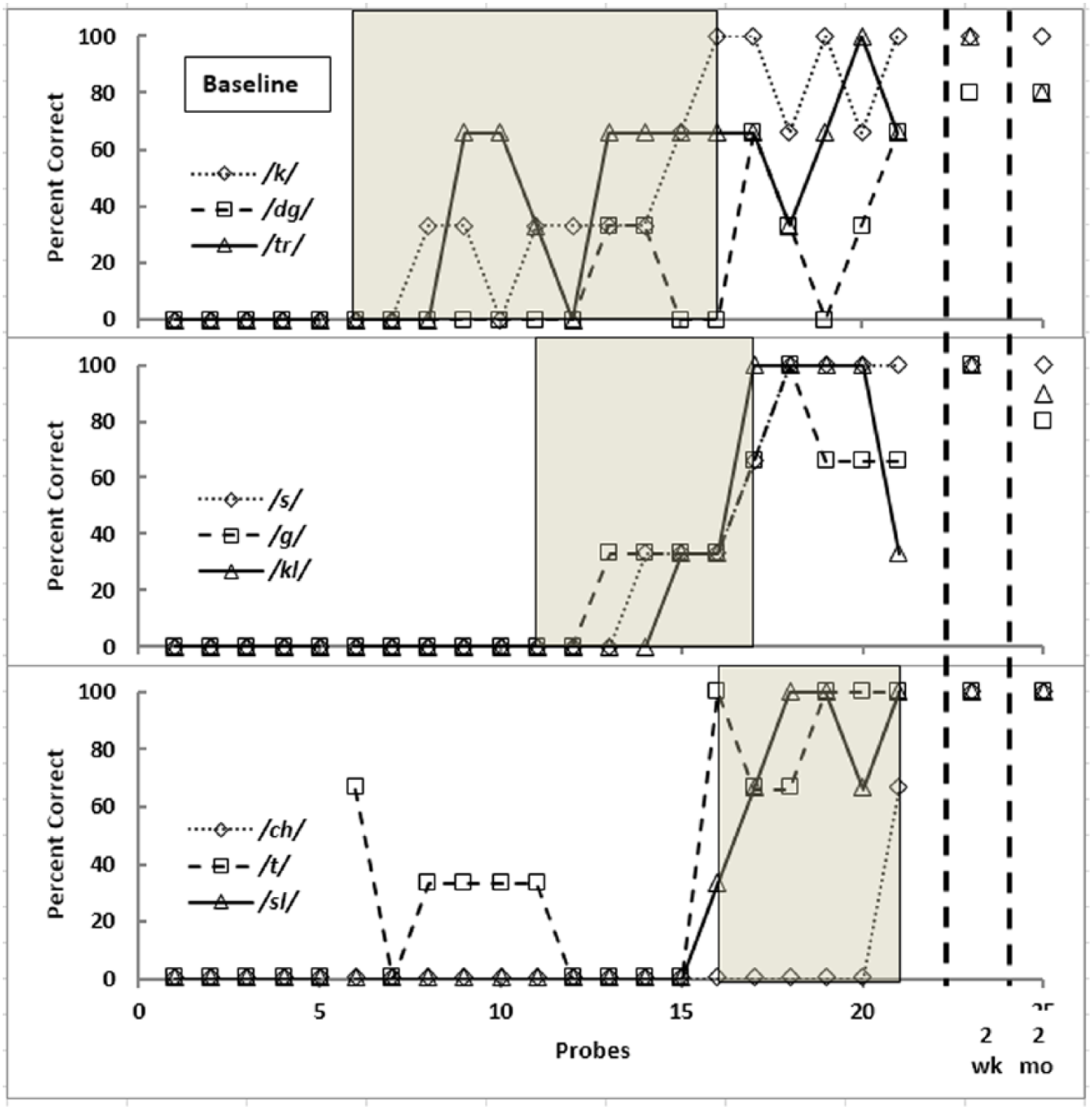
Percentage of correct production of probes in Child B.
After target group 1 was treated for five weeks, the Phase II experimental condition began by treating target group 2 simultaneously with target group 1. While the production accuracy of target group 1 was similar to Phase I, sounds for target group 2 gradually increased in accuracy. The /s/, /g/, and /kl/ sounds were produced with 33% accuracy during this phase. A dramatic improvement in production accuracy for all three target sounds of target group 2 was observed during probe 17. An interesting observation was that /t/ for target group 3 was no longer produced accurately at all whereas this sound was produced with 33% accuracy during Phase I.
The Phase III experimental condition began when production accuracy of one target sound (/k/) of target group 1 reached 100% accuracy. Once the Phase III experimental condition started, a dramatic increase for /t/ was observed; however, Child B had difficulty in producing /ʧ/ until the end of treatment. During the last probe, however, he was able to produce /ʧ/ with 66% accuracy whereas the other target sounds for target group 3 were produced with 100% accuracy.
A 2-week postmaintenance probe revealed that Child B produced /k, dʒ, tr/ with 97% accuracy, /s, g, kl/ with 100% accuracy, and /tʃ, t, sl/ with 100% accuracy. All sounds except for /dʒ/ were produced with 100% accuracy (5 correct out of 5 probes). The phoneme /dʒ/ was produced with 80% accuracy. A 2-month follow-up probe showed the child produced all target sounds with over 80% accuracy. The GFTA-2 was re-administered at 2-month follow-up. His production was within normal range. The standard scores were within 1 standard deviation below the mean. Most singleton consonants were produced correctly except for /r/ and /z/. The phoneme /r/ was produced as /w/ whereas /z/ was distorted. Other major errors occurred in consonant clusters including /r/ such as /br, dr, fr, gr, kr, tr/. All /r/ clusters were produced with /w/. Finally, the /st/ consonant cluster was produced as /s/. Similar to Child A, the overall intelligibility for Child B’s connected speech during the maintenance session was greatly improved. Based on a 1 to 6 scale (Fudala, 2000), his overall intelligibility was 2, that is, his speech was intelligible, although there were noticeable errors.
IV Discussion
The findings of the current study suggest that the multiple opposition phonological approach can be an effective treatment approach for children with severe phonological disorders. The two child participants demonstrated multiple phoneme errors. However, after receiving intervention using the multiple phonological approach, both children demonstrated great improvement on their production accuracy for target sounds during posttreatment probes. Thus, the current study provides additional support for findings in the current literature on the efficacy of the multiple opposition phonological approach (Allen, 2013; Williams, 2000a, 2000b, 2006).
Generalization effects were also observed in the two child participants. The GFTA-2 results at 2-month follow-up revealed that most singleton consonants except for a few were produced correctly although they were not targeted during intervention. For example, during pretest using the GFTA-2, Child A correctly produced only /b, p, d, m, n, w, j/ at word initial position. During posttest, his phonemic inventory at word initial position was expanded to /b, p, d, t, g, k, m, n, f, s, z, ʃ, h, ʧ, l, w, j/. Beside the target sounds /t, k, ʧ, dʒ, f, s/, untreated sounds /g, z, ʃ, h, l/ were also produced correctly based on GFTA-2 results. However, a generalization effect was not apparent in consonant clusters. Only two consonant clusters such as /kw/ and /sp/ were produced correctly at word initial position whereas other consonant clusters tested on the GFTA-2 were produced with sound deletions and/or substitutions. These findings suggest that consonant clusters may still need to be targeted to improve accuracy for this child. It may not be plausible to find a generalization effect for consonant clusters without direct treatment.
Child B also showed similar generalization effects. Child B correctly produced only /b, p, d, m, n, j/ correctly at word initial position during pretest. During posttest, his phonemic inventory at word initial position was expanded to /b, p, d, t, g, k, m, n, f, s, z, ʃ, h, ʧ, l, w, j/. Beside the target sounds /t, k, ʧ, dʒ, s, g/, untreated sounds /ʃ, h, l, w, ɵ, ð, v/ were produced correctly based on GFTA-2 results. A generalization effect also appeared for consonant clusters. Besides the treated consonant clusters /tr, kl, sl/, all other /l/ consonant clusters such as /bl, fl, gl, pl/ were correctly produced at word initial position. In addition, consonant clusters /kw, sw/ and /sp/ were also correctly produced.
These findings suggest that a multiple opposition phonological approach may enhance reorganization of the phonological system in children. Williams (2006a) noted that phoneme collapses in children provide an opportunity to understand what the child knows about the sound system. When multiple phonemes are collapsed, the child’s phonological system is smaller than the adult system and limited evidence of sound contrasts are observed (Grunwell, 1997). For these children, a phonological approach may be helpful instead of a traditional articulation approach because the multiple opposition phonological approach focuses on system-wide change and generalization, resulting in system reorganization. In particular, the multiple opposition approach which targets several sounds simultaneously may be a more effective way to treat children with phonological disorders because, as Ingram (1983) suggested, ‘children acquire several sounds simultaneously, not one at a time’ (p. 386). Crosbie et al. (2005) also made a similar claim that phonological contrast therapy leads to significant changes in a child’s phonological system although their argument was driven by examining the minimal pair approach (Weiner, 1981). Since limited evidence of the multiple opposition approach is available currently, further studies including a larger number of participants are warranted to validate these findings.
1 Evidence base of telepractice for speech intervention
The second focus of the current study was to examine treatment efficacy via telepractice for children with phonological disorders. The majority of telepractice studies have been limited to adult populations. Only a few studies are currently available investigating interventions for children with speech sound disorders. Thus, the current study provides additional evidence to the existing literature on speech intervention via telepractice for children with speech sound disorders. Similar to previous studies (Grogan-Johnson et al., 2011, 2013), we found that telepractice was an effective service delivery model for these two children with speech sound disorders. Unlike Grogan-Johnson, the current study adopted a phonological approach. Thus, telepractice may not be limited by type of speech intervention. Either articulation or phonological approaches may be appropriate for the telepractice service delivery model. However, it is not certain whether an articulation or a phonological approach is more effective via telepractice. Further studies are warranted to investigate this issue.
2 Study limitations
Although the present study adopted the overall principle of the multiple opposition approach (i.e. more than one contrasting sound was targeted during intervention), the study protocol did not strictly follow other aspects of the multiple opposition approach. The multiple opposition phonological approach protocol suggests that up to four target sounds should be selected simultaneously. In contrast, the present study procedures included only two (Child A) or three (Child B) target sounds based on phoneme collapse patterns of each participant because a multiple baseline approach where three target groups should be targeted was selected. Thus, if an SLP selects target sounds for either Child A or B using multiple oppositions, the number of target sounds that are treated during a session may be different from the current study. Furthermore, the way to select target sounds for the current study also might be different from the conventional way to select target sounds in that consonant clusters were not selected for Child A. The present study targeted only middle developing sounds (i.e. Shriberg, 1993), especially for Child A due to his young chronological age, resulting in exclusion of later developing sounds such as consonant clusters and /r/, /ɵ/, /ð/ phonemes. The author previously employed the multiple opposition approach for another young child who was similar to Child A and found that the young child had a difficult time developing a consonant cluster whereas other singleton consonants were acquired during intervention. Thus, the target selection was based on the clinician’s clinical judgement. Thus, these late developing sounds might be included for this child if the protocol for the multiple opposition approach is implemented.
In addition, the present clinical protocol adopted both a time-based and a criterion-based shift of target group sounds which may be different from the other studies evaluating a multiple baseline design. However, some previous studies (e.g. Preston et al., 2013) also targeted more than one sound during intervention when a multiple baseline design was adopted. The main reason for uses of both time-based and criterion-based shifts was that the production accuracy of target sounds did not reach the criteria during the extended time period of the intervention in either child. For example, Child B showed only 33% accuracy for /k/ and 66% for /tr/ during five weeks or 10 sessions. Even /ʤ/ was produced with 0% accuracy across this period. It was difficult for both child and clinician to continue to treat the same target sounds without improvement. Thus, in order to avoid frustration in a child client, a new target group was introduced after 4 or 5 weeks of treatment. Preston et al. (2013) noted that they discontinued treating a target sound if 0% improvement was observed after six consecutive sessions. Further studies may need to anticipate this lack of improvement as an important factor and modify their protocol.
Clinical evidence for the multiple opposition phonological approach showed a rapid increase of production accuracy in children who were studied. For example, Williams (2000a) found that percent correct of /s/ and /ʃ/ increased from 10% to 90% within less than 2 weeks once a multiple opposition approach was implemented twice a week. Dramatic improvement was also observed in the current study; however, it happened during Phase III for both of these children. In particular, during Phase I, it was difficult to observe a rapid improvement in production accuracy of targeted sounds. Our findings may be attributed to clinician factors. The clinician in the current study was an SLP intern trained in multiple opposition procedures. If an experienced SLP had delivered the intervention using the multiple opposition approach, progress might have been quicker than in the current study. Further studies may need to investigate clinician factors in intervention progress.
One last issue is evaluation of limitations of the telepractice service delivery model. It is commonly suggested that technology such as internet speech intervention via telepractice is a critical issue for delivering services. The current study originally included three participants; but one participant dropped out due to limited internet connection capacities in the child’s home. One of the primary purposes for adopting telepractice methods is to provide high quality services to under-represented populations in rural areas of the USA. Such a purpose may not be fulfilled if technical issues cannot be resolved successfully.
Footnotes
Appendix
Probes administered during study.
| Target sounds | Child A | Child B |
|---|---|---|
| /k/ | coat, cook, king, cone, cup | coat, cook, king, cone, cup |
| /dʒ/ | jump, juice, jeans, jacket, jet | jump, juice, jeans, jacket, jet |
| /tr/ | true, truck, train, trash, treat | |
| /ʧ/ | chess, cherry, chop, chain, cheese | chess, cherry, chop, chain, cheese |
| /t/ | tooth, tire, tall, Texas, taco | tooth, tire, tall, Texas, taco |
| /sl/ | sleep, slow, slide, slice, sled | |
| /s/ | seed, seat, six, sop, socks | seed, seat, six, sop, socks |
| /g/ | gum, go, gas, game, goat | |
| /kl/ | closet, climb, clap, clock, cloud | |
| /f/ | fan, feet, fight, farm, food |
Acknowledgements
The author deeply appreciated the two children and their families who participated in this study. Without their help and patience this project would not have been successfully completed. The author also appreciated Lynn A Williams, Barbara L Davis, Melissa Jakubowitz, and Sherry Sancibrian for their input and helpful comments when this study was conducted and the manuscript was prepared.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the South Plains Foundation Grant, Lubbock, TX.