
Abstract
The aims of this small-scale study were to explore the feasibility and outcomes of a parent-implemented intervention for two-year-olds at risk of language difficulties, and to explore the implications for the public health model of speech and language therapy (SLT). This adds to limited research into targeted SLT public health interventions. It is the first study to investigate early language intervention delivered by trained therapy assistants (TAs) rather than clinicians. Nine children aged between 26 and 31 months took part. Seven (78%) completed the six-session intervention. The outcome measure was the Words subscale of the Language Use Inventory. The gross motor subscale of the Ages and Stages Questionnaire was used as a control measure. Children’s skills were assessed twice before intervention and once afterwards. At baseline, six participants had expressive language delay and no wider speech, language and communication needs (SLCNs). Five of this subgroup showed language use skills within the typical range following intervention. At baseline, three participants had expressive language delay and previously undetected receptive language and/or social interaction difficulties. None of this sub-group showed improved age-adjusted language use skills following intervention. All nine participants had gross motor skills in the typical range at each time point. These exploratory findings suggest this targeted intervention is feasible. This study presents no evidence of short-term impact of this intervention for two-year-olds with expressive language delay and wider SLCNs. These findings suggest this targeted language intervention for two-year-olds may be associated with accelerated language development for some two-year-olds at risk of language difficulties because of expressive language delay; and may help identify two-year-olds with previously undetected wider SLCNs, and therefore facilitate early access to specialist support. We highlight limitations in the study size, design and outcome measures, and identify how these preliminary findings can inform future research.
Keywords
I Introduction
Expressive language delay is relatively common. 10% to 20% of children do not meet the typical milestones of using at least 50 single words and combining words into phrases by their second birthday (Reilly et al., 2007; Zubrick et al., 2007). Many children make progress after an early delay; up to 70% of two-year-olds with expressive language delay have skills within the typical range when reassessed at age 4 (Reilly et al., 2010). However, language difficulties which persist until school entry tend not to resolve, and may then be diagnosed as language disorder (McKean et al., 2017), which is associated with long-term social, emotional and academic difficulties (Norbury and Sonuga-Barke, 2017). While some risk factors for persistence of language difficulties are known, accurate prediction of long-term outcome is difficult. Many individuals move back and forth during the preschool years across arbitrary thresholds to define the presence or absence of language delay, and individual prognosis at age 2 is inaccurate (Bishop et al., 2016).
In addition, language delay may be a signal of a need for timely additional support, regardless of long-term prognosis. The presence of language delay may elicit changes in parent behaviour that in turn reduce children’s language-learning opportunities, such as increased parental directiveness or reduced responsiveness (Blackwell et al., 2015). Furthermore, language delay which appears to resolve by school-age may nevertheless present wider developmental risks. In the short term, two-year-olds with language delay have lower school readiness skills at age 5 than their peers (Hammer et al., 2017). In the longer term, the group of two-year-olds with language delay whose language skills move into the typical range by school-age nevertheless show lower literacy and language skills throughout childhood than their peers with typical early development (Rescorla, 2009). In short, language delay is a risk for long-term language and wider developmental difficulties.
Parent-implemented therapy can effectively improve language outcomes for two-year-olds with expressive language delay when delivered over 9 to 22 hours of therapy time by a qualified clinician. Effective intervention involves coaching parents to improve children’s language-learning opportunities in everyday conversation through the use of interaction-building and language-modelling strategies, such as following the child’s focus of interest and responsively modelling spoken language at the appropriate developmental level (Cable and Domsch, 2011; Roberts and Kaiser, 2011).
While intervention can be effective, there is a substantial social gradient in the prevalence and persistence of language delay, and in access to speech and language therapy (SLT). Children from more socially disadvantaged groups are more likely to have early language delay (Morgan et al., 2015a), and those difficulties are more likely to persist until school age. Recent population-based studies show that 18% to 23% of 5 year olds from the most socially disadvantaged quintile of the population have significant language difficulties, compared to 3% to 10% of the most advantaged quintile (Law et al., 2017a). Furthermore, children from more socially disadvantaged backgrounds with language delay are less likely to access SLT than their peers with similar speech, language and communication needs (SLCNs) (Morgan et al., 2015b). Some parents from socially disadvantaged groups report they do not know about the existence of SLT services (Roulstone et al., 2015), or find them difficult to access (Lees et al., 2011).
In response to this, some children’s SLT services have adopted a public health model of service provision. The public health model differs from the traditional medical model by including three tiers of service: (1) primary preventative or universal services for all children; (2) secondary preventative or targeted services for groups of children at increased risk of SLCNs; and (3) specialist services for children with identified SLCNs (Law et al., 2013). The model is intended to provide a continuum of services based on the continuum of long-term risk, with the overall aim of reducing the prevalence of long-term SLCNs (Law et al., 2017a). The model entails a need to provide targeted interventions - often of lower intensity and duration than specialist interventions - for children at risk of long-term SLCNs but who, based on their current speech, language and communication skills, might not be offered access to therapy within a medical model (Law et al., 2017c). These targeted services are often offered in innovative locations or formats to facilitate access to services (Smith et al., 2017).
Low intensity targeted intervention for children with language delay is feasible, acceptable to parents (Sheehan et al., 2009), and is a plausible mechanism to elicit change. Parents of two-year-olds with language delay can learn a new language-promoting strategy and consistently use it in play after as little as a one-hour teaching workshop and a one-hour therapy session (Roberts et al., 2014). However, only one published study has evaluated the impact of targeted public health SLT intervention. A cluster randomized trial of a targeted low intensity 12-hour group intervention for 18 month olds with expressive language delay detected no effect on children’s language or behaviour outcomes at ages 2 and 3 (Wake et al., 2011). The authors suggest this may be because 18 months is too young to accurately identify children with expressive language delay. Limited engagement in the intervention may have also contributed to the lack of effect; 43% of parents attended fewer than four of the six-session intervention, and 27% did not attend any sessions. In short, further research into targeted interventions used in practice is needed to inform the development of the public health SLT model.
In this article, we explore a targeted intervention for two-year-olds with language delay; we refer to this group of children as being ‘at risk of language difficulties’. As noted, some children in this group are likely to show signs of language disorder in later life, while some are likely to have less severe language difficulties which nonetheless impact on later development. As targeted public health interventions are intended to provide support for both these sub-groups, we use the term ‘at risk of language difficulties’.
II Method
The aims of this small-scale preliminary study were to explore the feasibility and individual outcomes of a low intensity parent-implemented language intervention offered as a targeted service for two-year-olds at risk of language difficulties, and to explore the implications of the study for the public health model. Ethical approval for the study was gained from the Health Regulation Authority (NHS IRAS no. 206352) and the local NHS Trust Research and Development department.
1 Intervention
The Nottinghamshire Children and Families Partnership Sure Start Children’s Centres service in Nottinghamshire, UK, offers a parent-implemented SLT service for two-year-olds at risk of language difficulties, known as Home Talk.
Home Talk is offered for children aged between 24 and 30 months at the point of referral with a parent-reported expressive vocabulary of between 11 and 30 single words and no known wider SLCNs. Children judged to be at highest risk of long-term language difficulties because of wider SLCNs (e.g. receptive language difficulties) and those with the most severe expressive delay (expressive vocabulary of fewer than 10 words) are eligible for a specialist SLT service rather than Home Talk. Children are referred to Home Talk following a universal developmental review between 24 and 30 months of age by health visitors or health visitor assistants, as part of the Healthy Child Programme (Department of Health, 2009). Health visitor teams are trained by the local SLT service in the use of a locally devised language assessment (based on observation and parent report) as part of this 2 year developmental review.
Home Talk consists of up to six therapy sessions with the child and parent(s) lasting around one hour each, delivered over around 6 to 12 weeks, by a therapy assistant (TA). We consider that Home Talk is a low intensity intervention as therapy time is less than specialist interventions known to be effective (at least 9 hours of therapy time) (Roberts and Kaiser, 2011). Sessions are delivered at home to facilitate access to the service, and to help parents embed changes into their home learning environment and routine. Therapy aims are to coach parents to provide optimal language-learning opportunities through (1) developing their use of interaction-supporting and language-modelling strategies; (2) providing a supportive environment for language learning, for example, by limiting use of dummies and background noise such as television; and (3) regular use of language-rich activities such as book sharing and one-to-one play times. Individualized therapy goals related to these areas are agreed between the TA and parent(s). The intervention also provides opportunity for further assessment of the child’s speech, language and communication skills. For example, TAs typically assess the child’s receptive language skills through play-based key word assessment, which has been shown to be a valid measure of receptive language (Frizelle et al., 2017).
TAs have at least a Level 3 qualification in early years or child development (UK Government, 2018), training in motivational interviewing, and enhanced training in language development, including Let’s Interact: An adaptation of Learning Language and Loving It™: The Hanen Program® for Early Childhood Educators/Teachers (McDonald et al., 2015; Weitzman and Greenberg, 2002). During the period of the study, the TAs and supervising SLTs completed an on-line training seminar in coaching parents in supporting early language development (The Hanen Centre, 2017). TAs have clinical supervision with an early years Speech and Language Therapist every six weeks. At the start of the study, the TAs who delivered the intervention (authors DH, SC, and CW) had relevant Level 4, 5 and 6 qualifications, respectively, and had between 4 and 6 years’ experience delivering this intervention. The supervising Speech and Language Therapists (authors DM and SG) had 7 and 31 years’ experience in children’s SLT, respectively.
Home Talk uses a range of tools and resources to engage parents in therapy and support learning. Dunst and Trivette’s meta-analysis of adult learning methods identified six effective adult learning methods, and showed that learning outcomes are improved when more of these methods are used (Dunst and Trivette, 2009). Table 1 describes these learning methods, and the tools and resources used in Home Talk that correspond with each. These tools are used flexibly for each family.
Adult learning methods, tools and resources used in Home Talk intervention.
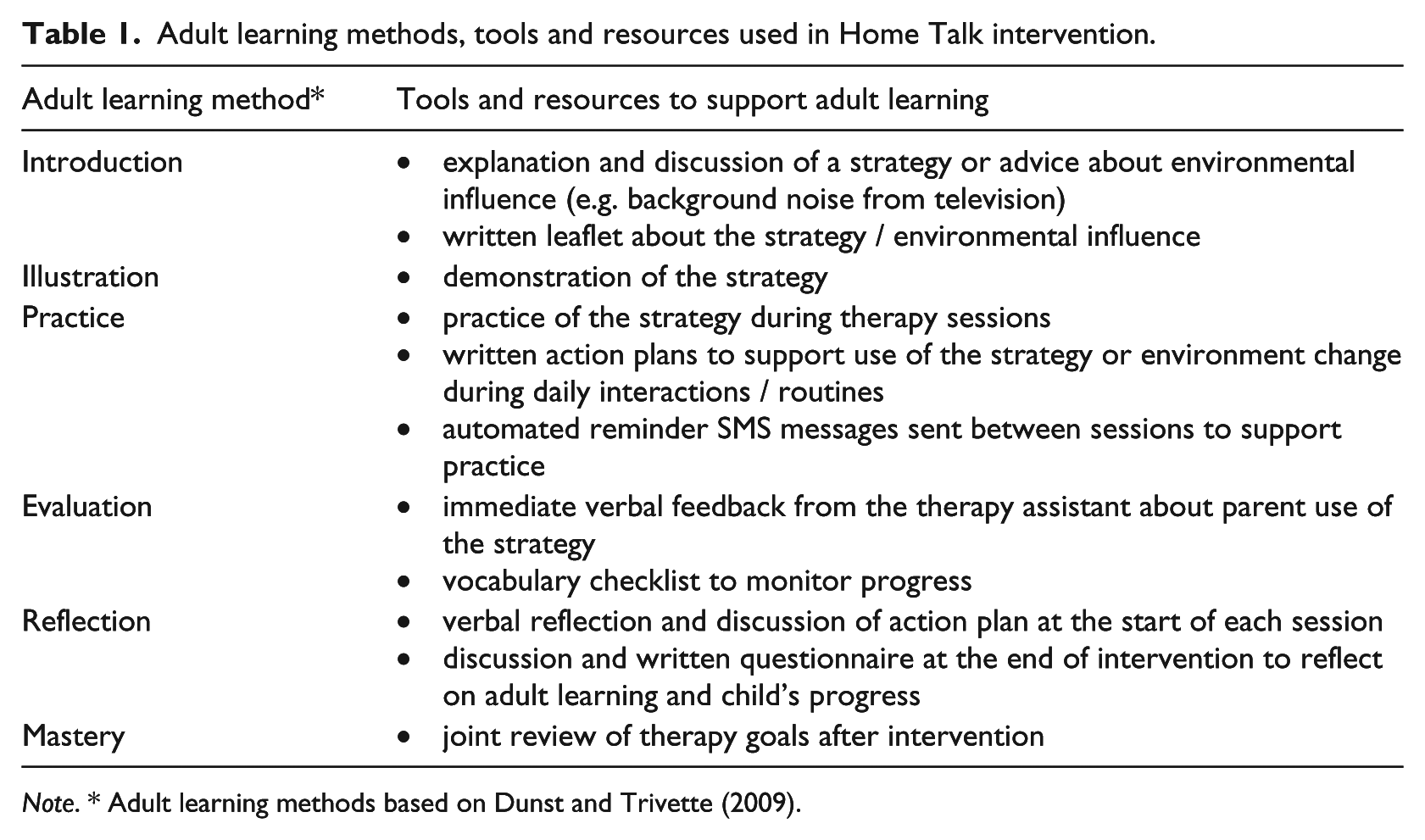
Note. * Adult learning methods based on Dunst and Trivette (2009).
2 Study design
The study was a multiple baseline case series. Case series studies do not test the efficacy of an intervention, and their results are not intended to be generalizable to the population. However, they provide opportunity to develop theory and models of intervention and, when they include elements of experimental control such as a multiple baseline, can contribute to the evidence base, especially, as here, where evidence is limited (Vance and Clegg, 2012).
Outcomes measures were parent-report measures, a valid and reliable assessment method in two-year-olds which shows strong agreement with direct assessment methods, especially for expressive skills (Miller et al., 2017). The primary outcome measure was the Words subscale of the Language Use Inventory (LUI), a standardized parent-report measure of a child’s language use skills with strong psychometric properties (O’Neill, 2009; Pesco and O’Neill, 2012). Parents complete the LUI Words 28-item checklist by identifying word types their child uses from a list of categories (e.g. body parts, food, clothing), and how their child uses words to ask for help. The Gross Motor subscale of the Ages and Stages Questionnaire, 3rd edition (ASQ-3; Squires and Bricker, 2009) was used as a control measure, as we did not predict any change in age-adjusted gross motor skills following intervention. The ASQ-3 is a standardized parent-report measure with moderate to strong psychometric properties (Velikonja et al., 2017) which is routinely used in the UK to screen for developmental delay in two-year-olds (Department of Health, 2009). Following administration rules, the age-appropriate version of the ASQ-3 was used at each time point (24, 27, 30 or 33 month version). Feasibility of the intervention was assessed using evaluation of attendance at therapy sessions.
3 Participants
Children referred to the intervention from their 2 year developmental review who met referral criteria for the service (as described in the Intervention section) in three districts in Nottinghamshire were eligible to participate in this study. Families could choose to take part in the intervention without participating in this study. Children whose main language was not English were not invited to participate, as the primary outcome measure is not standardized for this population. Parents gave written informed consent to take part in the study at the point of referral. Consent was reconfirmed at the first phone contact with the research team and re-recorded in writing. Recruitment ran from July 2016 to January 2017. 24 families returned written consent to take part. It was not possible to contact six participants for data collection, and one was excluded as intervention was started in error before baseline data collection. Of the 17 remaining participants, two declined the intervention, one did not start the intervention during the study period due to administrative error, and one postponed the intervention due to illness. Of the remaining 13 participants, four had made progress during the baseline period, and then showed single word vocabulary within the typical range and use of at least two-word phrases at first contact with the local SLT team. These families took part in a different low intensity intervention so were not included in this study.
Nine families (6 boys; 3 girls) took part in the intervention and were included in the study. Children’s median age when they started intervention was 29 months (range: 26 to 31 months). All participants were monolingual English speakers. The Index of Deprivation Affecting Children (IDACI) was used to measure participants’ socio-economic background (Department for Communities and Local Government, 2015). A higher IDACI score indicates a higher level of deprivation. The national median score is 0.148 (range: 0.004 to 0.916), compared to our sample median of 0.216 (range: 0.092 to 0.365). Seven participants (78%) scored above the national median.
4 Procedure
The existing routine waiting time for intervention was used as a baseline period. Outcome measures were completed in phone interviews with parents / carers by a member of the SLT team who was not involved in the child’s care (authors DM or JY). The assessor was not blinded to the time point of the assessment. Data were collected at three time points. The two baseline time points were Time 1: as soon as possible after referral to the intervention; and Time 2: 8 weeks after Time 1. The outcome time point was Time 3: 18 weeks after Time 2. There was some variation in timing of assessments relative to intervention because of differences in local waiting list times. The median time between Time 2 and the start of therapy was 27 days (range: 6 to 68 days). The median total duration of intervention sessions was 360 minutes (range: 160 to 390 minutes). For the 8 participants who had completed therapy by Time 3, the median time between the end of therapy and Time 3 was 40 days (range: 18 to 70 days), and the median duration of therapy (time between the start of the first session and the final therapy session) was 63 days (range: 37 to 84 days).
III Results
1 Feasibility
As shown in Table 2, seven of nine families (78%) attended all six home sessions during the study period. One family (ID 111) completed three therapy sessions and the parent then agreed with the worker to stop the intervention as she thought she had learnt enough new language-modelling strategies to support her child’s language development. One had completed five sessions of the six-session intervention at the follow-up assessment for this study, as some therapy sessions had been cancelled and missed by the family.
Therapy input, individual outcomes and clinical assessments.

2 Language outcomes
We identified two groups of children based on their SLCNs before intervention. Group A consisted of six children at risk of language difficulties because of expressive language delay. Group B comprised three children at risk because of expressive language delay and other co-occurring SLCNs. Table 2 describes clinical assessments, therapy input, and individual outcomes for each participant. For children who scored the maximum raw score on the LUI Words measure at Time 3, we report the range of corresponding percentile scores, following the LUI manual (e.g. ⩾ 49th percentile if the maximum raw score corresponded to between the 49th and 99th percentile for that age/sex).
To evaluate outcomes after intervention, we used an arbitrary cut-off of ⩽ 20th percentile on the LUI Words measure to define the presence of delayed language use skills. As this targeted intervention was intended for at-risk children, we used a more inclusive cut-off than typically used in studies of similar specialist level interventions, which often use the 16th (–1 SD) or ⩽ 10th percentile as an arbitrary cut-off (e.g. Buschmann, 2009; Roberts and Kaiser, 2015).
Five of six participants (87%) in Group A showed age-adjusted language use skills within the typical range following intervention. Notably, the language skills of one of these five (ID 111) moved close to the 20th percentile cut-off before the start of intervention and the parent and practitioner agreed to reduce the number of intervention visits. The sixth participant in Group A (ID 102) showed persistently delayed language use skills following intervention. Participant 102 had inconsistent attendance at therapy sessions, had not fully completed the intervention by Time 3, and was referred for further specialist SLT for severe expressive language delay.
Group B consisted of three participants who had expressive language delay and wider SLCNs. Clinical assessments showed that all three had previously undetected receptive language difficulties (one key word level of comprehension), and one had previously unidentified social interaction difficulties, i.e. high risks for language difficulties. These participants showed no change in their age-adjusted language use skills following intervention, remaining at the 1st percentile. None met criteria for this targeted intervention because of undetected SLCNs at the point of referral, but would have been eligible for local specialist SLT at that point. All three were referred on to specialist SLT following intervention.
No participant scored below the age-adjusted cut-off on the ASQ-3 assessment at any assessment point, demonstrating that all participants had gross motor skills within the typical range at each time point. This suggests that improvements in parent-reported language use skills were not due to changes in parents’ ability to observe and report on their child’s behaviour or development, or due to accelerated developmental progress in all areas.
IV Discussion
Current UK Government policy focuses on the importance of early language intervention from the age of two (Department for Education, 2017; Early Intervention Foundation, 2018). This exploratory study extends previous early language intervention research in two important ways. First, it is the first study to explore a parent-implemented language intervention for two-year-olds led by a therapy assistant rather than by a clinician. Second, it adds to the limited research into early language interventions at the targeted level of the public health model of SLT. We stress that this case series is not intended to test the efficacy of this targeted intervention, but to explore its feasibility, to inform the development of the public health model of SLT, and to highlight where further more robust research studies are needed. We highlight four findings from this exploratory study, and their possible implications for the public health model.
First, this study suggests that low intensity targeted parent-implemented intervention delivered at home by a therapy assistant for two-year-olds at risk of language difficulties is feasible. Participation in the intervention (78% completion of the six-session intervention) was higher than that reported in the only other published study of targeted early language intervention, in which 57% of parents attended at least five of six group sessions for 18 month olds at risk of language difficulties (Wake et al., 2011). It is possible that the home-based location, one-to-one nature of the intervention, or age of children at referral influenced participation rates compared to Wake et al., (2011). Wider research into home-based early interventions has identified features which influence feasibility and participation, such as the structure of the intervention, learning methods used, and the dispositions and personal qualities of the home visitor (Korfmacher et al., 2008). As one of the aims of the public health model of SLT is to increase equity and ease of access to intervention, further qualitative research into the factors that influence feasibility and participation in public health SLT services is clearly needed to inform the development of services being used in practice within this model.
Second, this study suggests this parent-implemented intervention may be associated with accelerated language skills for some two-year-olds at risk of language difficulties because of expressive language delay. 87% of a relatively socially disadvantaged sample of two-year-olds with expressive language delay and no wider SLCNs who accessed this intervention – the at-risk group for whom the intervention was intended – showed age-adjusted language use skills within the typical range following intervention. The presence of one participant in this at-risk group who made no gains in age-adjusted language use skills following intervention is consistent with existing intervention research. While a systematic review shows that therapist-led higher intensity interventions for this client group have moderate to large effect sizes at the group level, every study which reports data at the individual level includes some participants who made no significant gains or no gains at all following intervention (Cable and Domsch, 2011). In short, these indicative findings suggest this model of intervention is a plausible candidate for further efficacy studies.
Third, individual outcomes suggest that targeted intervention may have an important role to play in identifying children at high risk of language difficulties, including those with previously undetected wider SLCNs, and may facilitate early access to the long-term specialist support they are likely to need. For three participants with expressive language delay, participation in this targeted intervention led to detection of previously unidentified additional SLCNs, receptive language delay and / or social interaction difficulties, which substantially increase the risk of persistent language difficulties (Paul and Roth, 2011). This study provides no evidence of short-term impact of this low intensity intervention on the language skills of this subgroup of two-year-olds at high risk of long-term language difficulties. This is consistent with wider evidence that these individuals need high intensity specialist intervention designed to meet those needs (Roberts and Kaiser, 2015). We note that the targeted intervention examined in this study was not designed for this sub-group of two-year-olds, and was offered because their wider SLCNs were not known at the point of referral.
Fourth, this study demonstrates the need for ongoing surveillance of development and flexibility of provision for two-year-olds identified as being at risk of language difficulties. The aim of the public health approach is to provide a continuum of services which correspond to a continuum of need, so individuals can ‘step up’ and ‘step down’ between levels of services as needed (Law et al., 2017b), as was observed in this study for four participants who were referred on for further specialist intervention. The clinical outcomes for one participant (ID 111), whose language skills moved close to our arbitrary cut-off during the baseline period and took part in a reduced intervention, suggest that flexibility within the targeted level may also be an important feature of the model. A potential benefit of this flexibility of targeted provision is that it may mitigate the risk of over-provision within the public health SLT model (Law et al., 2017b), in that an individual’s progress both before and during intervention may inform a decision to change the type or dosage of intervention, or not to offer intervention.
1 Implications for research
These preliminary findings suggest that low intensity TA-delivered targeted intervention supervised by an SLT should be evaluated in efficacy studies, such as experimental group studies comparing outcomes of assistant-delivered, clinician-delivered intervention and/or a control condition, and in studies examining the impact of treatment intensity on outcomes. Qualitative research which explores the key features of this type of parent-implemented interventions is also needed to inform the provision of acceptable interventions. In short, further research is needed to identify if this model of intervention is effective for two-year-olds at risk of language difficulties and, if so, for which individuals it should be recommended, and what the key features of intervention delivery should be. Given the limits of current evidence and the prioritization of this model of intervention in the UK (Early Intervention Foundation, 2018), this should be a high priority for the SLT profession.
2 Limitations
This exploratory study has at least four important limitations in its design. First, the case series design, while strengthened by the use of a multiple baseline and a control measure, does not rule out alternative explanations of the observed changes in age-adjusted language use skills (e.g. accelerated language development unrelated to intervention). Second, because the sample was self-selecting, participants may be more highly motivated and engaged in therapy than other parents/carers who access this intervention. Third, we did not monitor fidelity of implementation of the intervention, either in terms of what intervention content was delivered by TAs for each participant, what learning tools, resources and methods were used, or how it was implemented by parents. Fourth, we did not measure long-term impact of the intervention. Limitations of the outcome measures should also be noted. First, while this exploratory study includes a relatively socially disadvantaged sample, IDACI measures deprivation of a geographical area and is not a direct measure of deprivation or socio-economic status at the individual level. Second, the main language outcome measure is not standardized for the UK population and is not a comprehensive assessment of all aspects of language development. This measure was chosen as a feasible option for use in this clinical research study due to resource limitations; where resources allow, a direct standardized assessment of children’s language development would be preferable. Given these limitations, we caution again against extrapolating these findings until further more rigorous studies into this type of intervention are completed, and caution against applying these findings to different service models (e.g. intervention delivered by TAs with lower levels of qualification, training or supervision).
V Conclusions
This study suggests that low intensity parent-implemented language intervention for two-year-olds at risk of language difficulties, in which sessions are delivered at home by a highly trained therapy assistant with clinical supervision, is feasible. It presents novel preliminary evidence that the most appropriate use of this intervention in public health SLT may be for two-year-olds at risk of language difficulties because of expressive language delay and no wider SLCNs. It suggests that targeted intervention may help identify two-year-olds who have previously undetected wider SLCNs, and therefore facilitate access to specialist SLT for children who otherwise may not have their needs identified or supported. This study reinforces wider evidence that two-year-olds with expressive language delay and co-occurring receptive language delay and / or social interaction difficulties need long-term specialist intervention specifically designed to address their needs. The study provides indicative evidence that provision of targeted intervention should be based on ongoing surveillance of needs and risks, and that flexibility within the targeted level for the public health model may help tailor intervention to individuals’ needs and mitigate the risk of overprovision. We stress that these findings are preliminary and that further robust research is needed before these findings should be extrapolated.
Footnotes
Declaration of conflicting interest
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors are employed by an organization that delivers the intervention studied in this article. The intervention was devised and developed by author SG.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.