
Abstract
This study explored the feasibility of training school teaching assistants to provide the treatment, Dynamic Temporal and Tactile Cueing to treat childhood apraxia of speech (CAS, also known as developmental verbal dyspraxia). The study used a single case experimental design across behaviours and a qualitative evaluation of teaching assistant experiences using interviews. Two student-teaching assistant dyads participated. One child was aged 6;2 (6 years 2 months) and the other 5;6 at the time of the study. Both participants had speech characteristics consistent with the features outlined in the 2007 Technical Report on CAS from the American Speech and Language Hearing Association (ASHA). These included lengthened and disrupted coarticulatory transitions between sounds and syllables, inappropriate prosody and inconsistent errors on consonants and vowels. Treatment outcomes were measured using visual analysis and calculations of total-change improvement rate difference (TC-IRD) and composite IRD (C-IRD) based on percent of phonemes correct. Fidelity to the treatment protocol was measured using a Fidelity Score. Visual analysis of both child participant’s data showed an upward trend for all treatment and similar words and a flatter trajectory for control words. Both child participants had a TC-IRD score of 100% for all treatment words. One child also had a TC-IRD score of 100% for their similar words and a TC-score of 25% for their control words. The second child had a TC-score of 67% for similar and control words. Both teaching assistants had a Fidelity Score of over 90%. Both teaching assistants reported positive experiences in conducting the program. Training teaching assistants may be an effective means of providing treatment to children with CAS while they are at school. Training teaching assistants also helps to improve their capacity which may have positive implications in their interactions with other children with speech sound disorders.
I Introduction
Childhood apraxia of speech (CAS, also known as developmental verbal dyspraxia) is a speech motor planning disorder that can severely affect a child’s ability to produce intelligible speech. While some believe it can be difficult to diagnose due to the potential overlap with symptoms of other speech sound disorders such as a phonological disorder (Terband and Maassen, 2010), recent computational models of speech production (Terband et al., 2011) suggest that CAS may result from a systemic level difficulty in the speech production mechanism. This difficulty comprises of an impairment in feedback and feedforward commands which results in an over reliance on the impaired feedback mechanisms. Consequently, motor plans are either not developed, are difficult to store or recall or are poor quality. This leads to difficulties such as disordered coarticulation, distortions and inconsistency.
These characteristics are highlighted in the American Speech and Language Hearing Association (ASHA) CAS technical report as the main features of CAS (American Speech-Language-Hearing Association, 2007). In this report, CAS is characterized by difficulties with transitioning across sounds and syllables, disordered or unusual prosody, and inconsistent production of consonants and vowels (American Speech-Language-Hearing Association, 2007). These features have been used for diagnosis or description of CAS in most, if not all, reported studies of CAS over the past 20 years. Children with CAS often require extensive speech therapy and CAS can persist throughout an individual’s life (ASHA, 2007). A longitudinal study of 10 children from preschool to school age, found that children with CAS exhibited more severe and persistent errors in speech, language and spelling than either children with other speech difficulties or children with other speech difficulties and a concomitant language disorder (Lewis et al., 2004).
Given the severity and persistence of CAS, the need for effective speech-language pathology intervention is high. There has been a significant increase in the number of treatment studies over the past 10 years however currently only one single randomized control trial has examined the comparative effectiveness of CAS treatments (Morgan et al., 2018). However, recent single subject experimental studies have illustrated the effectiveness of motor-based intervention strategies for CAS (Maas et al., 2014). These studies are grounded in the principles of motor learning (PML), and suggest that effective treatment outcomes for children with CAS can be achieved with intensive and regular treatment sessions (Maas et al., 2014).
In practice, the degree to which clinicians can deliver this intensive level of service provision for children with CAS has not been well researched. However, more general research into the extent of service delivery for children with speech sound disorders (SSD) (including articulation and phonological disorders, CAS and dysarthria) suggests that service provision can be limited (McLeod et al., 2013). For example, McLeod and colleagues (2013) reported that in Australian schools, a significant percentage of preschool aged children with SSD had not had any contact with a speech and language practitioner (SLP; McLeod et al., 2013). School-based SLPs in the USA experience larger caseloads than considered manageable by the American Speech and Hearing Association (Katz et al., 2010). and caseload size and years of practice have been found to influence the level of SLP service delivery in schools rather than student characteristics or severity (Brandel and Loeb, 2011). Therefore, despite research suggesting that intensive treatment is effective for children with CAS, it is possible that children with CAS are not receiving sufficient intervention to improve their speech in an effective and efficient manner.
A shortage of funded speech-language pathology positions has been reported by SLPs in both Canada and Australia as the main barrier to service delivery across a wide range of speech-language pathology practice (Lim et al., 2017). In the same study, training of parents, teaching assistants and caregivers was reported to be the main strategy that SLPs used to overcome these service delivery barriers. Despite this reported use of teaching assistants 1 to aid in the treatment of children with speech and language difficulties in schools, there is very little research into the effectiveness of using teaching assistants in the treatment of children with speech difficulties.
Some research has been conducted into the effectiveness of training educators both in schools (i.e. trained teachers) and in early years programs (i.e. childcare workers) to improve the oral language and early literacy skills of children (Rezzonico et al., 2015; Tyler et al., 2014; Wasik and Hindman, 2011) and other areas such as the use of visual supports in the classroom (Wellington and Stackhouse, 2011). However, there is very little research into the effectiveness of training teaching assistants, teacher’s aides or therapy assistants in the treatment of children with SSD using a ‘pull-out’ service delivery model, let alone specifically with children who have CAS. Mecrow et al. (2010), in their study on the effectiveness of using specialized teaching assistants to perform speech and language therapy with 35 children, showed improvements in their target outcomes. However, no distinction was made between language outcomes versus speech outcomes and therefore it is difficult to determine if the use of therapy assistants was equally effective for speech and language goals. Gardner (2006) explored how teaching assistants and SLP students might be trained to adjust their responses to children’s speech attempts in therapy to shift a child closer to an accurate production but the study did not elaborate if this training had any overall impact on the accuracy of speech outcomes of the children. Another study has also shown that using a school based ‘pull out’ method and delivering targeted language therapy by SLPs or teaching assistants can have a more efficacious effect on the expressive language skills of students than a consultative therapy model (McCartney et al., 2011). However, no studies to date have focused specifically on children with CAS and there is no detailed diagnostic information provided for the children’s speech difficulties, so we might assume that more common conditions such as articulation or phonological disorders were the primary diagnoses.
Dynamic Temporal and Tactile Cueing (DTTC) is a treatment approach that uses the PML and relies on the clinician guiding a client through a hierarchy of motor-based cues to achieve accuracy in target words. (e.g. Maas and Farinella, 2012; Strand and Skinder, 1999; Strand et al., 2006;). In all but one of the existing DTTC studies, clinicians delivered intervention with a relatively high frequency of treatment. The exception to clinician treatment is a recent study which explored the effectiveness of training parents to deliver DTTC at home which showed positive change for only one of the children (Lim et al., 2019). That study highlighted the barriers to parent-implemented speech therapy for these children including the difficulties parents encounter in managing behavioural challenges of their children and difficulty finding the time to carry out the programme. Lim et al. (2019)’s findings about parent delivery of DTTC confirmed the findings of Thomas et al. (2017) which indicated that a parent delivered home therapy program for CAS was often logistically difficult for parents to carry out and that it often placed a large amount of stress on the family so that many parents did not enjoy being the therapist (Thomas et al., 2017).
Therefore, given the difficulties of using parents as agents of therapy and the limited research into the effectiveness of using teaching assistants to deliver a school-based therapy programme for children with CAS, there exists a gap between research and clinical practice. This study attempts to fill this gap by exploring the effectiveness of training teaching assistants in a school setting to deliver a motor-based treatment programme, DTTC, to children with CAS. The study aims to answer the following questions:
Will DTTC school-based treatment program delivered by school teaching assistants lead to increased percentage of phonemes correct in words targeted in therapy (i.e. target words)?
Will teaching assistants be able to achieve good fidelity with the treatment and be able to conduct the required number of sessions?
What are the teaching assistant experiences when delivering DTTC?
II Method
The study uses a single case experimental design across behaviours and a qualitative evaluation of teaching assistant experiences using teaching assistant interviews. The research was approved by The University of Sydney Human Research Ethics Committee (2014/924).
1 Participants
Two children participated in the study. Both children had a history of speech delay and met the study’s criteria for a diagnosis of CAS (see below). Their first language was English and they both successfully completed a hearing screen (American Speech-Language-Hearing Association, 2015) They did not have an Autism Spectrum Disorder or any other diagnosed developmental syndromes. Both teaching assistants passed a hearing screen, spoke English as their first language and did not have any speech difficulties.
Child participants were recruited after being referred by their teachers. As there is no current standardized test for CAS, it is commonly diagnosed by experienced clinicians using perceptual judgements based on a group of core features (see Appendix 1). (Shriberg et al., 2011). ASHA (2007) in their technical report outlined three characteristics of CAS including inconsistent errors on consonant and vowels, lengthened and disrupted coarticulatory transitions between sounds and syllables and inappropriate prosody (see Appendix 1). Murray et al. (2015) in their study identifying objective measures to differentiate CAS from other speech disorders found the following features to be most discriminative: syllable segregation, lexical stress matches, percentage phoneme correct and decreased accuracy in a diadochokinesis (DDK) task. They did not find that the feature of inconsistency had significant discriminative value. This research was used to develop the eligibility criteria for a CAS diagnosis in the present study. CAS was diagnosed when the following characteristics were present in at least 2 of the assessment tasks:
lengthened and disrupted coarticulatory transitions between sounds and syllables;
inappropriate prosody, especially in the realization of lexical or phrasal stress;
slow or disrupted diadochokinesis (DDK);
at least one additional feature outlined in Appendix 1.
The Dynamic Evaluation of Motor Speech Skills (DEMSS) (Strand and McCauley, 2018) was used as part of the pre-assessment battery. The DEMSS has been found to have good reliability and validity in differentially diagnosing CAS (Strand et al., 2013). Both children obtained scores on this test that indicated a likelihood of CAS.
Both children lived in a single community in Northern Canada although they went to different schools. Brian was 6;2 (6 years 2 months) at the start of the study and Nicholas was 5;6. The two teaching assistants, Sarah and Pamela, also lived in the same community and had experience in working with children with speech and language difficulties. Sarah was in her 30s and Pamela was in her 50s. Sarah had been working in the role for 2 years and Pamela over 30 years. Neither teaching assistant had any formal training in the area beyond school sponsored seminars and on-the-job training by school SLPs. All names are pseudonyms.
2 Pre-study assessments
The pre-study assessments included the Goldman Fristoe Test of Articulation 2 (Goldman and Fristoe, 2000); the Inconsistency subtest of the Diagnostic Evaluation of Articulation and Phonology (DEAP) (Dodd et al., 2002); the oro-motor screen of the DEAP (including DDK) (Dodd et al., 2002); the Dynamic Evaluation of Motor Speech Skills (Strand and McCauley, 2018), the Test of Polysyllable Words (Gozzard et al., 2006); and the Reynell Developmental Scales 3 (Edwards et al., 1997). All authors agreed on the diagnosis of CAS and the eligibility of both participants. Appendix 2 shows the pre-test performance of the participants. Pre-treatment assessments for both participants were conducted at the clinic or at school.
3 Study design and treatment protocol
The single case experimental component was made up of six different phases; baseline, teaching assistant training, treatment phase 1, withdrawal or break phase, treatment phase 2 and a maintenance phase (see Figure 1). Each treatment phase targeted 6 different target words, giving a total of 12 target words across the two phases of treatment. Target words were selected based on the child’s phonemic repertoire and the gaps in their abilities as determined by the pre-assessment tests. Control words also reflected these gaps in speech skills however they were not targeted in therapy and were not expected to change.

Planned study design from commencement to completion.
a Probe data collection
Probe data collection occurred each week of the study and was collected at the clinic, at school, at day care or at home prior to any therapy on that day. The exception to this was that there was only one probe session conducted across the first two teaching assistant training weeks due to the availability of the child participants. Probe items were individualized for the child but largely the same across the entire study period from baseline to maintenance. The exception to this was that after the initial three baseline sessions, Nicholas’ speech goals were slightly changed and his probe words were subsequently altered. This was because he was able to say some of the words that were initially going to be targeted in therapy. Consequently, analysis of Nicholas’ baseline probes only included data from Baseline week 4 onwards. Both participants’ probe data consisted of 14 control words, 6 phase one target words, 6 phase two target words and 8 words with similar features to the target words but were not targeted in any treatment phase.
Two local speakers not connected to the study were video recorded saying the probe items, one speaker for each child. All probe word video recordings were presented in a power point presentation accompanied by a picture of the word. Each slide consisted of one probe word with both picture and video. Probe words were randomly presented in each probe session. The child was seated in front of a laptop and the first author changed the slides of each probe after the child tried to say the word. The child wore over the ear headphones with an attached microphone (Sennheiser PC) that was placed approximately 5cm from the child’s mouth. The first author played the video recording on each slide and the child was told to look at the video and repeat what was said. The child was video and audio recorded and at the end of the probe session, the author and the child played a game as a reward.
b Teaching assistant training sessions
Four weekly teaching assistant training sessions were completed at school with each lasting 1–1.5 hours. These teaching assistant training sessions followed a staged model of self-directed learning (Grow, 1991) where the teaching assistant was supported through a learning process to become more independent in their use of DTTC. The teaching assistant was initially provided with information on CAS and DTTC and then DTTC was demonstrated with opportunities for the teaching assistant to practise the strategies initially through role play with the first author and then later through practising with the child. The teaching assistants were shown how to use the individual cues in the hierarchy. They were also trained in how to determine accuracy of production. They were told to see a child’s production as accurate if ‘the whole word sounded correct’. Feedback was provided to the teaching assistant through the use of videos (online coaching) and offline coaching. Within this training structure, some flexibility was allowed to cater to the learning needs of the teaching assistant. The structure of the training sessions was as follows:
Week 1: Building knowledge. Information on CAS using videos
Week 2: Building knowledge. Information on DTTC using videos and demonstration
Week 3: Building capacity. Role playing and practice
Week 4: Building capacity. Practice.
Teaching assistants were provided with a DTTC teaching assistant manual that contained information on CAS, DTTC and the treatment protocol at the end of the training phase. They were also provided with access to the videos used in the training. These videos included videos of their role playing, of the first author practising with the child and of their own interactions with their student. The manual and treatment protocol are available from the first author.
Although not part of the treatment phases, due to the need for both demonstration of DTTC and the teaching assistant to practice the strategies, the child participants did receive a small amount of therapy during the teaching assistant training phase. This therapy was limited to the teaching assistant training sessions (once a week prior to formal commencement of teaching assistant led therapy).
c DTTC treatment protocol
DTTC relies on a hierarchy of cues that help support the child to successfully say the targeted word (Strand et al., 2006). Appendix 3 shows an outline of the cueing hierarchy used in the study. If a child is not able to say a target word accurately or respond to the cue provided, the teaching assistant was required to move down the hierarchy and provide a more detailed cue (e.g. moving from direct imitation to saying the word at the same time as the teaching assistant). The reverse then occurred if the child was able to respond to a cue with an accurate production. In this situation, they would move up the hierarchy and be provided with a cue that was less supportive or detailed.
A DTTC board game was provided to each teaching assistant to facilitate adherence to the cueing hierarchy during the intervention sessions. The game provided the teaching assistant with instructions of what to do following the child’s response. Teaching assistants were also told to ask the child to repeat a target word three times if they gave a correct response to a cue. If a child made two consecutive errors at one level of cueing on the hierarchy, they were allowed another attempt at saying the word using the next cue down the hierarchy before the teaching assistant moved onto another target word. Each target word and associated picture were placed on a card that the teaching assistant used in the intervention when working with the individual target words. The same picture was used in the PowerPoint of the probe words.
Cards were shuffled at the start of an intervention session and then presented in that order during that session until the allocated time expired. This allowed for the random practice of the words between sessions but still encouraged blocked practice of the words during the session. Other features of the PML such as reducing feedback frequency and a large number of practice trials were not emphasized to ensure the protocol was as simple as possible for the teaching assistants. Teaching assistants were given a timer that they set for 15 minutes and asked to get as many attempts as possible during this time. They were also provided with some short, non-therapy games that they could play with at the end of the session to help keep the child motivated.
d Treatment and maintenance phases
There were two treatment phases, each of 5 weeks duration They were separated by a break or withdrawal phase of 2–3 weeks. During the two treatment phases, teaching assistants were asked to provide treatment for 15 minutes twice a day (Brian) or once a day (Nicholas) depending on whether they were attending school for the full day or only half a day. Teaching assistants were provided with an audio recorder so they could record the treatment sessions. Regular in-person or via social media messaging contact was made between the first author and the teaching assistants throughout the study. The teaching assistants were able to contact the first author during the break period if they wanted. A four-week maintenance phase followed the second (final) treatment phase.
At the conclusion of the second treatment phase teaching assistants were interviewed about their experiences in carrying out the DTTC treatment program using a semi-structured interview protocol. Teaching assistants were also given the opportunity at the completion of the interview to provide further comments. These semi-structured interviews were audio recorded and transcribed by the first author. The interviews were listened to up to four times to check the accuracy of the transcription and the transcriptions were then checked with the teaching assistants who were able to make any changes. Neither teaching assistant made any changes.
4 Outcome measures
a Child measures
All words were calculated for percent phonemes correct (PPC) and an overall PPC score for each group of probe words (control, target 1 and 2, and similar) was obtained for each probe session. Visual analysis was conducted to determine treatment effects and an improvement rate difference (IRD) score was used to calculate an effect size. The IRD reflects the number of improved data points between baseline or non treatment phases and treatment phases (Rakap, 2015). A small or questionable change is reflected in an IRD of 50% or less while a moderate effect has an IRD above 50% to 70%. An IRD of greater than 70% indicates a large effect size (Parker et al., 2009). Two IRD scores were calculated – an IRD across all the study phases that measured the IRD for each intervention phase versus neighbouring non-intervention phases (Composite IRD or C-IRD) and an IRD that compared the baseline phase with the maintenance phase to provide a pre-post measure of changes in PPC (total change IRD or TC-IRD). Therefore, the TC-IRD score is a measure of the difference in the child’s abilities after intervention versus before intervention whereas the C-IRD score is a measure of change throughout the study period and may reflect more fluctuations in the child’s abilities across the study period. Both scores have been used in an attempt to obtain a richer analysis of the dynamic process of therapy. It is hypothesized that treated words will have higher TC-IRD and C-IRD scores than the other groups of words and that due to generalization effects, similar words will have higher scores than control words.
Probe data was transcribed by the first author, another experienced speech-language pathologist, and a trained speech-language pathology intern. Inter and intra rater reliability was measured on 20% of the probe data. The mean intra-rater reliability was 92 (SD 3.80, range 85–100) and the mean inter-rater reliability was 89 (SD 4.77, range 80–100).
b Teaching assistant measures
The teaching assistant’s ability to carry out treatment was determined by the total number of school-based sessions that the teaching assistant conducted. The number of practice trials of target words said in each session was also calculated. The teaching assistant’s fidelity or compliance in using the DTTC treatment protocol was measured by determining how many behaviours the teaching assistant exhibited on an eleven item checklist (for a copy of the fidelity checklist, see Appendix 4). The checklist was completed by the first author based on audio recordings of therapy sessions. Teaching assistants were scored as YES if they used a behaviour that was part of the DTTC protocol (e.g. moving down the hierarchy when the child’s response was judged incorrect) or NO if an appropriate behaviour was absent. A fidelity score (FS) was obtained by dividing the number of YES behaviours by the total number of YES and NO behaviours.
The teaching assistant interviews were analysed qualitatively by the first author using qualitative content analysis (Graneheim and Lundman, 2004). Each idea that was expressed by the teaching assistants was noted and similar ideas were grouped together and then coded as themes. These themes were then compared across both teaching assistants to determine any similarities or differences in the content of the themes that were expressed. The second author then reviewed the transcripts and themes to ensure that there were no misinterpretations or omissions.
III Results
1 Child outcomes
a Brian
A visual analysis of Brian’s PPC across the study period (Figure 2) showed that there is a steady improvement in his PPC scores for his target and similar words. His C-IRD scores for phase 1 target words were 53% across the whole study (see Figure 3). The C-IRD score of 39% for his phase 2 target words was in the not effective range (under 50%) although it was higher than his similar and control word C-IRD scores. However, his TC-IRD scores phase 1 and 2 target words and similar words was 100% while his TC-IRD score for his control words was 25% which indicated a treatment effect for target and similar words (see Figure 4).

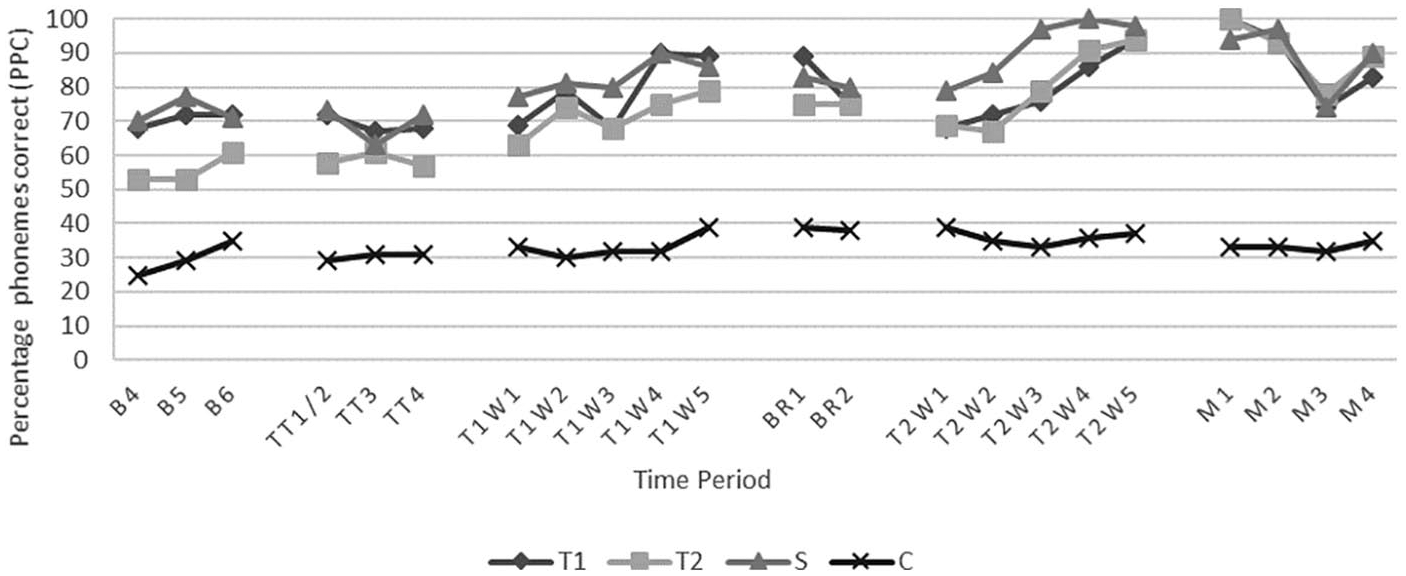
Brain: Percentage phonemes correct across time periods.
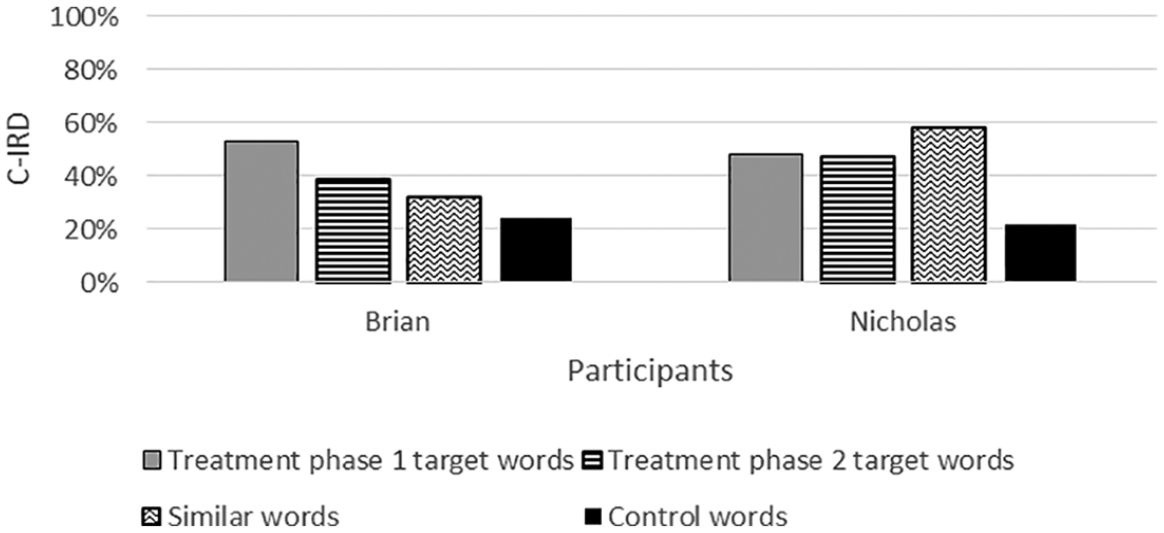
Composite Improvement Rate Difference (IRD) for each group of probe words across participants.
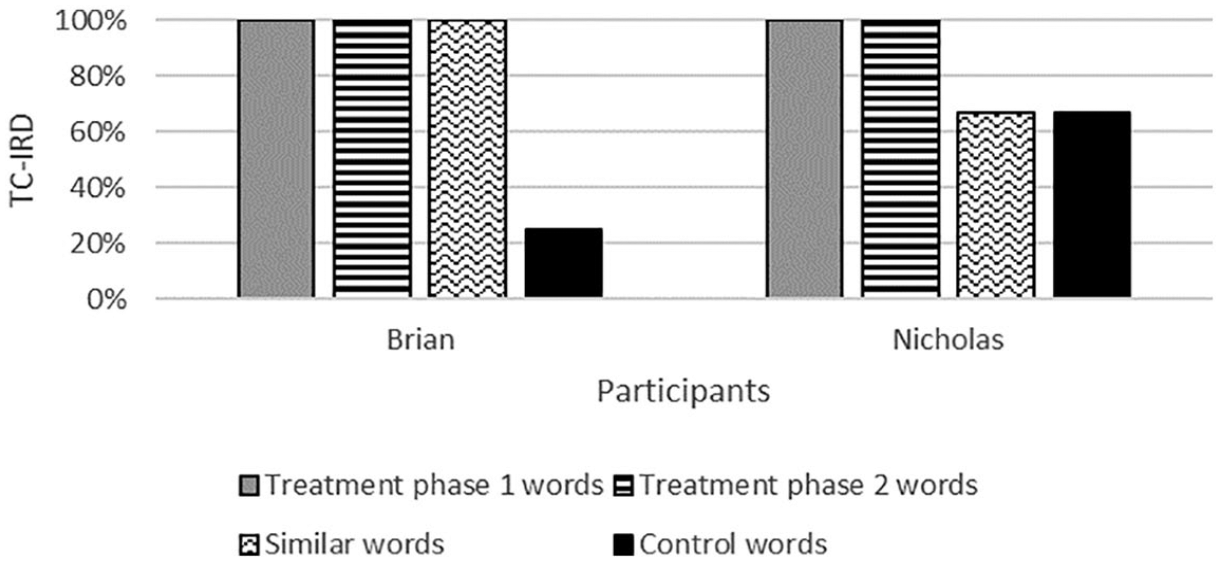
Total change Improvement Rate Difference (IRD) for each group of probe words across participants.
b Nicholas
A visual analysis of Nicholas’ data (Figure 5) indicated that there is an upward trend for his phase 1 and phase 2 target words and similar words. Although his control words also increased, their trajectory was more stable and flat after the initial improvement in the teaching assistant training and treatment phase 1 part of the study. His C-IRD scores for phase 1 target words was 48% and 47 % for phase 2 target words (see Figure 3). His C-IRD for the control words was 22%. His production of similar words had a C-IRD of 58 %. All target words achieved a TC-IRD of 100% and his similar words and control words had a TC-IRD of 67% (see Figure 4).
Nicholas: Percentage phonemes correct across time periods.
2 Teaching assistant outcomes
a Sarah
Teaching assistant outcomes for both teaching assistants are summarized in Table 1. Sarah completed 35 sessions out of a possible 100 sessions (16 for phase 1 target words, 19 for phase 2 target words). Reasons for not conducting sessions included student and teaching assistant absences, class special events and holidays. She had 90% fidelity. During the sessions, Sarah elicited an average of 91 practice trials of treatment words per session (range: 78 –131).
Tutor outcome measures.

b Pamela
Pamela completed 33 sessions out of a possible 50 sessions (19 for phase 1 target words, 14 for phase 2 target words). Reasons for not conducting sessions included student and teaching assistant absences and holidays. She had 93% fidelity. She elicited an average of 47 practice trials of treatment words per session (range: 16 to 76).
3 Themes from semi-structured interviews
There were 6 themes that were identified from interviews with both teaching assistants. Although both teaching assistants expressed some similar ideas within the themes, there were differences in what they thought about the relevant themes.
a Child’s response
Both teaching assistants felt that the program was helpful for the children. Sarah felt that the program ‘worked really well’ for Brian and she particularly noted that when he had been at school for consecutive days, ‘his ability to speak and want to speak out loud was greater than when he was absent for days in a row’. Pamela also felt that the program was ‘definitely useful’ for Nicholas and that he ‘got better at it’.
b Format of the program
Both teaching assistants commented on the format of the program and were mostly positive about the nature of DTTC. Both teaching assistants remarked that the program was clear and well outlined. Sarah for instance said:
It seemed well thought out. The step by step, it made it. You had a clear goal and a clear way to get to the goal. And there was no abstract to it.
Pamela also found that ‘the format of it I really liked because I know what to do next.’ They both liked the cueing hierarchy and felt that it provided some degree of independence for their students even when they were struggling with achieving good accuracy. As Pamela said:
They feel that they can even if they haven’t got the word right, but they can like independently, if they’ve got it right together they can say it together correctly, it’s still a step.
This idea was echoed by Sarah who felt that the cues provided a means of achieving some success even with challenging words. She described how Brian was ‘in the beginning very quiet and shut off and if he couldn’t say it, he didn’t want to say it but then near the end, it was like, “Ok, I made a mistake on that but that’s not the word, it’s this” and that he became “a lot more open and vocal”.’ Sarah felt that the cues ‘[made him] feel like you go with it until [he felt] like [he] succeeded it in some way’.
Both Sarah and Pamela felt that the program was flexible. Pamela also felt the program easy to implement as part of her workday and although she only conducted the program once a day because Nicholas was only at school in the afternoon, she felt that she could easily have implemented it twice a day.
The teaching assistants also provided some individual reflections. Pamela said that she felt the program was an efficient use of her time and that she could achieve quite a few practice trials in a 15-minute session. Sarah felt that Brian’s words could have been a little bit more challenging as she felt that she was often providing cueing beyond the direct imitation step (e.g. delayed imitation) and she was concerned that Brian was not getting as much practice responding to the lower level cues (e.g. tactile and gestural cue). Pamela also said that she liked the visual nature of the game board.
c Extended use
Both teaching assistants liked DTTC sufficiently that they found that they were using it (albeit more informally without the game board) with other children and were planning on continuing to use it with other children. Sarah also detailed how she would also use some of the cueing with Brian in class with other words. Her use of it was modelled to his class teacher who was also using some of the cueing with him (e.g. getting him to say a word simultaneously with her). She elaborated on this when she said:
In class yeah, he seemed to look more at you. And like if you weren’t letting him just get away with not saying a word. He’d have to look at you, to mouth the word or whatever and he seemed to get more connected with myself and with [teacher name]. Cause she would make him say the word too. It wasn’t just ‘we know what you want, so just go get it’.
Pamela elaborated on how using it with other children also proved beneficial:
I’ve actually used it with some of the other kids, not the chart per se, but the technique of you know the copy, you know, say it after me. Some really good things and made a difference in some other kids on them picking up stuff quickly so that was really, really. I was excited.
Both teaching assistants said that they would repeat the study again if possible.
d Lessons learnt
Both teaching assistants appreciated the stepped nature of the cueing and felt that learning DTTC helped them to learn more about how to help their student articulate targeted sounds more. They found that DTTC allowed them to break down where their student was having difficulty with the target word. For instance, Sarah felt that DTTC allowed her to know ‘more of the hierarchy of the steps instead of going straight from one of them to giving him the word or feeding him a sound or whatever, to step down slower’. Pamela found that she felt DTTC allowed her to understand better what difficulty Nicholas was having and therefore was more able to help him. She described it this way:
it gave other ways for me to back up and I liked that. I liked that it gave me levels to do because not everyone gets the copy one right away . . . Its when they can’t even copy that, now where do I . . . So it gave me some other ways of looking at it . . . well, here’s some other things we can try.
Pamela elaborated more than Sarah on what she had learnt and reflected more on her own growth throughout the study. She found it was ‘easier as I went along because I was definitely more used to the whole process’. She felt she was able to make better judgement calls about when Nicholas was correct in his productions as the study progressed. Pamela ultimately felt DTTC was another ‘tool in [her] toolbox’ that she could use with other children that she saw.
e How teaching assistants felt
Although both teaching assistants talked about liking the program, their emotional responses to the program, at least initially, were quite different. Sarah reported confidence in using DTTC and did not indicate that this wavered at any point during the study. Pamela on the other hand, felt a certain degree of anxiety initially about ‘going to screw them up for life if I do something a little bit differently’. She did not feel confident going into the study. Nonetheless these feelings shifted and by the end of the study she was no longer anxious, felt more confident using the program and was less concerned about making a mistake. She said:
once I got over the nervousness and got more comfortable with it, definitely was much easier to do.
f Barriers
The only barrier that Sarah encountered was Brian’s attendance at school which was inconsistent at times. Pamela felt her initial difficulties in judging a word as correct or incorrect was a barrier. She also outlined initial difficulty in getting into the flow of the cueing as a barrier but also went on to say that once she got more practised, this ceased to be an issue.
You know, so I think that was probably the hardest part of it was just getting to the point where I felt comfortable with the flow of up and down and kind of going and then the second thing is also my problem, getting past the point, you know, even if I’m not sure what it was, if I’m right or wrong, it’s not going to hurt them if we back up when we should have gone ahead one, so realizing that it’s not the end of the world if I make the mistakes with that.
IV Discussion
DTTC, when provided by a trained teaching assistant, was effective in changing the speech accuracy of both children in this study. Both children showed a large treatment effect when comparing their scores at the end of the study to the start of the study (TC-IRD = 100%). Across the study, a steady change in PPC scores for target words was maintained to the end of data collection. This steady change across the entire study period was also reflected in a visual analysis of their PPC scores suggesting that the TC-IRD scores may be a more accurate reflection of longer term therapeutic change than the C-IRD scores. Brian’s lack of effective change in control words indicated that this change is related to the use of DTTC teaching assistant-led therapy and not normal maturation and the equally high effect size for his similar words reflected generalization to untreated but similar words. Nicholas also had generalization of the treatment effect to similar words. While Nicholas’ results showed an effective change across pre and post intervention for his control words (TC-IRD = 67%), this is likely a result of the initial improvements that he had in production of his control words during the early part of the study that plateaued rather than continuing to increase across the rest of the study. The fact that as the study progressed and the target and similar words continued to progress along an upward trajectory where the control words did not, may indicate that it was the treatment and not normal maturation that influenced the accuracy of the treatment and similar words. These results demonstrate that it is possible to train teaching assistants to deliver a DTTC based treatment programme in schools to children with CAS and that gains made in such treatment can be maintained for some time after the treatment is completed. Furthermore, a teaching assistant led treatment program can lead to improved results not just for treated words but also for similar untreated words.
The study provided additional evidence for the effectiveness of DTTC as a treatment protocol for children with CAS. However, unlike some of the previous research into using DTTC to treat CAS (Edeal and Gildersleeve-Neumann, 2011; Maas and Farinella, 2012; Maas et al., 2014), this study demonstrates that it is possible to train others besides clinicians to use DTTC effectively. This has particular utility for clinicians who may be in a position to train others such as teaching assistants or therapy aides to deliver DTTC therapy. Despite the nuanced nature of DTTC of moving up and down a hierarchy in response to child attempts, this study shows that a DTTC approach to therapy has the potential to be learnt and successfully used by teaching assistants. This supports the Gardner (2006) results where teaching assistants were able to learn how to change their responses to their student’s speech attempts to facilitate more accurate and independent speech production. The teaching assistants in our study reported an overall positive experience in using DTTC with their students. They found the process easy to follow and once they became more practised in using the cueing themselves, they found it easy to move up and down the hierarchy and even started to use DTTC with other children on their caseload. Teaching assistants here had fidelity scores which reflect this confidence. The reported experiences of the teaching assistants in the current study shows that even if there is initial trepidation and uncertainty about how to do DTTC, with practice and support, teaching assistants can become comfortable in using DTTC with minimal barriers.
There may be a range of reasons why teaching assistants could be better agents of therapy than other people in a child’s life (e.g. parents). Teaching assistants are paid to work with children and therefore time management difficulties that parents have reported in parent-led studies (Lim et al., 2019; Thomas et al., 2017) are not a concern for teaching assistants. Also, teaching assistants may already have prior experience in working with children in a structured setting as was the case for the two teaching assistants in this study. This prior experience may explain why they were able to achieve such high levels of fidelity.
Despite the success of this study, it is important to be aware of its limitations. Foremost, this study was a single case design with two participants and therefore the results need to be replicated in a larger study to provide confidence that they are applicable to the general CAS population. For instance, the teaching assistants here had prior experience in working with children with speech disorders and therefore had a certain capacity prior to the study. It is uncertain if the same positive results could be achieved if the program was carried out by teaching assistants that had less overall experience either as teaching assistants or in working with children with speech disorders. The teaching assistants in this study also had the aid of the DTTC game board which provided them with visual reminders of when to move up and down the hierarchy accurately. Teaching assistants were given specific criteria as to when to suspend cueing on a word and move onto the next word. Therefore, while non-clinicians can be taught how to use DTTC, they may still need to rely on additional supports to help them maintain fidelity with the treatment protocol. A more complete use of the PML in the treatment protocol was also not feasible and this could be explored further in future research. Furthermore, despite the encouraging results in relation to the maintenance of speech accuracy, longer term maintenance of treatment effect for more than 4 weeks has not been determined. Additionally, the results of this study reflect success in training teaching assistants to use DTTC to treat a select group of target words, which in this case words were single syllable. It is unclear if target selection has an impact on the effectiveness of a teaching assistant led DTTC treatment program. Finally, the results in this study do not reflect any functional changes in the participants’ speech such as their intelligibility or ability to communicate more effectively with peers. Future studies should include examination of this as it would add further depth to our understanding of the impact of the approach.
DTTC can be taught to other non-speech-language pathologist child professionals successfully and a teaching assistant implemented DTTC program in schools has the potential to have a positive impact on the speech of children with CAS. Perhaps this study also highlights that the process of therapy is often nuanced and multifaceted, and as we train others to carry out therapy programs, we should also be aware of their own learning needs and capacity to conduct therapy with children. We may add another tool to someone’s tool box, but we do still need to make sure they are supported in using it.
Supplemental Material
Desktop – Supplemental material for ‘Another tool in my toolbox’: Training school teaching assistants to use dynamic temporal and tactile cueing with children with childhood apraxia of speech
Supplemental material, Desktop for ‘Another tool in my toolbox’: Training school teaching assistants to use dynamic temporal and tactile cueing with children with childhood apraxia of speech by Jacqueline Lim, Patricia McCabe and Alison Purcell in Child Language Teaching and Therapy
Footnotes
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.