
Abstract
Profound hearing loss can have serious and irreversible consequences for oral language development in children, affecting spoken and written language acquisition. Auditory-verbal therapy has been widely applied to children with hearing loss with promising results, mainly in developed countries where cochlear implants are available. An evaluation was done of auditory perception in 25 children 5 to 8 years of age, with profound hearing loss, users of 4- or 5-channel hearing aids, and enrolled in a personalized auditory-verbal therapy program. Regarding initial auditory perception skills, children performed better on the Noises and Sounds block than on the Language block. By subscales, top performance was observed for auditory analysis (Noises and Sounds) and auditory recognition (Language). A series of t-tests showed that significant improvement after Auditory-verbal therapy occurred in global scores for Noises and Sounds and for Language blocks, regardless of sex, urban or rural community origin, nuclear or extended family. The study provides evidence of deficiencies in auditory in children with profound bilateral hearing loss and how this might improve after receiving Auditory-verbal therapy. Nevertheless, the descriptive study design prevents conclusions regarding the effectiveness of the therapy. Subsequent research must take into account intrinsic and environmental factors that might play a mediating role in the benefits of Auditory-verbal therapy for auditory perception.
Keywords
I Introduction
Up to 5.3% of the world’s population presents with hearing loss and 9% of it are children (World Health Organization, 2017b). In México, 19.2% of the population with a hearing loss is not older than 9 years, and up to 28.9% are 14 years or younger. It has been estimated that in Mexico 13.4% of children aged 0–14 years have a hearing loss (INEGI, 2015).
Hearing loss in children from 0 to 14 years old (i.e. a hearing loss greater than 30 dB in the better hearing ear) has been linked to lifelong deficits in speech and spoken language acquisition, poor academic performance, personal-social maladjustments, and emotional difficulties (Cunningham et al., 2003; World Health Organization, 2017a). Research on the impact of hearing loss has shown that, if appropriate early auditory exposure and auditory brain development are not experienced, the results are linguistic and communication deficits which may be lifelong (Dornan, 2010). Children born with limited auditory function cannot adequately develop spoken language capacities and this, directly or indirectly, may compromise their functionality and social integration, as well as their cognitive development. Thus, timely diagnosis is clearly needed to begin appropriate treatment as soon as possible (Nikolopoulos, 2015). It has been argued in that spoken language-deprivation highly compromise spoken language development in children with hearing loss by altering in crucial early stages white matter microstructure, especially in the left dorsal arcuate fasciculus (AF) pathway (Cheng et al., 2019) and this may lead to psychiatric symptomatology, for instance, spoken language dysfluency, knowledge deficits, and disruptions in thinking, mood, and/or behaviour (Hall et al., 2017). Fortunately, during the last decades, the negative impact of early hearing loss has been reduced through significant technological developments such as hearing screening of new-borns, new objective diagnostic tests, use of digital hearing aids and cochlear implants. Furthermore, emerging neuroscience research is supporting the rationale for the combination of early diagnosis and fitting of hearing technology with early auditory brain stimulation, resulting in maturation of the auditory neural system, a precondition for development of listening and spoken language (Dornan, 2010).
Hearing aids will compensate sensory function but need to be accompanied by auditory-verbal training to help with learning and interpreting sounds, understanding and contextualizing their meanings, and other abilities promoting assertiveness in the spoken language learning process (Garrett and Baquedano-López, 2002). Habilitating the physiological capacity to perceive sounds is a necessary precondition, but is not sufficient alone for spoken language development and, in this case, improvements in the auditory perception would be beneficial. Auditory perception is the ability to identify, segment and isolate the sound elements in the environment, interpreting sounds, and associating them with information stored in the memory. The sounds stimulus is transformed into a coherent mental representation with meaning that favours cognitive and intellectual development. This is one of the biophysical reasons for the efficiency and superiority of auditory communication by speech. If fully functional, it naturally leads to the development of the individual’s capacities for spoken language (Nippold, 2014). However, in case of early and long deprivation of auditory stimulation, the corresponding brain pathways (i.e. from the receptors in the organ of Corti of the inner ear (cochlear hair cells) to the central nervous system, carried by the vestibulocochlear nerve (CN VIII) until the primary auditory cortex) might not organize and mature properly.
One consequence, might be that integration of auditory and visual information may be deficient even after hearing is habilitated (Gilley et al., 2008, 2010). It is advisable that audiologic intervention in children, by cochlear implants or hearing aids, be accompanied by auditory-verbal training to improve the cognitive sound assignment process (Ingvalson et al., 2014; Paatsch, 2005). This condition has demanded the development of training approaches in delivering auditory brain stimulation and developing listening and spoken language, such as auditory-verbal therapy (AVT). It must be pointed out that learning and using sign language, although compatible, does not seem favourable for children with hearing loss learning spoken language. For instance, Geers and colleagues (Geers et al., 2017) found that children without early sign language exposure achieved better speech recognition skills, had better age-appropriate spoken language, produced more intelligible speech and exhibited a significant advantage in spoken language and reading in comparison to children exposed to sign language.
AVT is a logopedic therapeutic approach emphasizing audition for the development of the auditory skills needed for spoken language acquisition, focusing on developing listening and spoken language through audition, using parents as the child’s natural spoken language teachers, with the aim of full inclusion in the mainstream. AVT relies on ten core principles related to early diagnosis, use of an appropriate state-of-the-art hearing technology and commitment of parents to be guided and coached to create an environment where the child can learn to listen, process verbal language and speak (Dornan, 2010; Maggio-De-Maggi, 2004).
Although the effect of AVT on auditory perception has been reported before, to the best of our knowledge, it has not been exclusively applied in children with no cochlear implants. Fairgray and colleagues (Fairgray et al., 2010) evaluated the effect of AVT on speech and spoken language, speech perception in noise, and reading in 7 children. Five participants had profound, bilateral sensorineural hearing loss and used 1 or 2 cochlear implants, the remaining 2 had moderate-to-severe and severe-to-profound hearing loss, respectively, and used hearing aids. Sahli and colleagues (Sahli and Belgin, 2011) examined the development of auditory perception performances of 15 children who received AVT after cochlear implantation. Both studies report improvements in auditory perception performances following AVT.
AVT interventions have been implemented in the treatment of children with hearing loss in various contexts and evidence-based practice outcomes suggest it is a promising approach (Eriks-Brophy, 2004; Rhoades, 2006); yet, further evidence from samples of children with no cochlear implants is required. In Mexico, continuous efforts have been made by the public health system and non-governmental associations to provide infants with the necessary treatment but limited financial resources, private and public, result in most children with profound hearing loss receiving a hearing aid rather than a cochlear implant. This circumstance, although not ideal, provides the opportunity to perform a study with the following objectives: (1) to analyse the auditory perception profile in a sample of Mexican children with profound hearing loss and who are only provided with hearing aids, and (2) to observe any possible improvements in their auditory perception following auditory verbal therapy.
II Method
1 Design and participants
The Research and Ethics committee of the School of Medicine, of the Autonomous University of Yucatan, provided authorization and ethical approval for this descriptive study. All children received treatment at AYPRODA (Asociación Yucateca Pro Deficiente Auditivo / Yucatecan Association Pro-Hearing Impaired), the only non-profit civil society in the community working on prevention, detection, oral-only treatment, and consultancy for deafness and hearing impairment. It offers services to all in need regardless of residence, availability of medical insurance and socioeconomic status.
Inclusion criteria were: (1) diagnosis of profound bilateral sensorineural hearing loss as recorded in clinical files, (2) 5 to 8 years of age, (3) bilateral use of hearing aids that were properly functioning, (4) a status of ‘active patient’ in the association (no more than two weeks since last visit), (5) no ear infection present during the time of intervention neither over the two weeks prior to initial assessment, (6) without any prior knowledge of sign language or intention to learn it during the time of intervention. An initial review of clinical records found 29 children meeting these criteria. In a meeting with their parents/tutors AVT was offered to all children, regardless of acceptance to be part of the study. Inclusion in the study required the child’s agreement and at least one parent/tutor informed consent signing with no economic compensation involved. None of the parents/tutors presented hearing loss. Initially, all 29 children were signed up for the study but 3 could not initiate AVT due to difficulties to attend with the required frequency. For a first meeting with each family of the remaining 26 children the purpose was to establish rapport with the child and to ask parents/tutors to complete a brief socio-demographic interview (Appendix 1 in supplemental material) on behalf of their child. A total of 22 weekly meetings were then scheduled, 20 for AVT and another two to assess the child’s auditory perception capacity before and after AVT.
All participants had in common that they were first assessed and treated for hearing loss in AYPRODA, and no speech/spoken language intervention had ever been received previous to their participation in the study. They did not present any physical and/or mental disability. All cases of hearing loss were static, as they had no syndromic origin they could not possibly progress into anacusis. Hearing loss type and level were measured in AYPRODA by a certified audiologist, who was also responsible for fitting and placing the hearing aids of 4 or 5 channels to all children. Parents were instructed to make the child wear the hearing aids daily and at all moments, except during bathing and sleeping; yet, compliance to this instruction was not strictly monitored. All children are raised in monolingual Mexican Spanish families and due to their hearing disability they are still in the process of spoken language acquisition.
All children had hearing loss from birth, but specific etiology could not be identified for any of the participants. It must be mentioned that a genetic test did not find the GJB2 and GJB6 genes to be present; neither the hearing loss could be attributed directly or indirectly to any comorbid condition.
2 Auditory verbal therapy (AVT)
Following Pollack et al. (1997), a personalized AVT plan was designed based on each child’s deficiencies taking into consideration the initial results from the Auditory Perception Test (Gotzens-Busquets and Marro-Cosialls, 2001). Children did not receive sign language input during the intervention. AVT consists of twice weekly 60-minute sessions for ten weeks for a total of twenty sessions. In this study, sessions were once a week, given that most families live outside the city, lack private transportation and depend on the free transport service provided by their local government accessible once a week. In each session, individual work was done with the child using cognitive-behavioural techniques such as sound and word examples, association of the mental representation of an image with each sound or word, and its conceptual representation and socialization in daily life. All sessions took place in AYPRODA’s location with a single psychologist certified as an Auditory-verbal therapist. Appendix 2 in supplemental material presents the program for the twenty sessions and a pair of examples of individual sessions. Tasks and times were arranged according to the child’s needs and advances.
3 Auditory perception
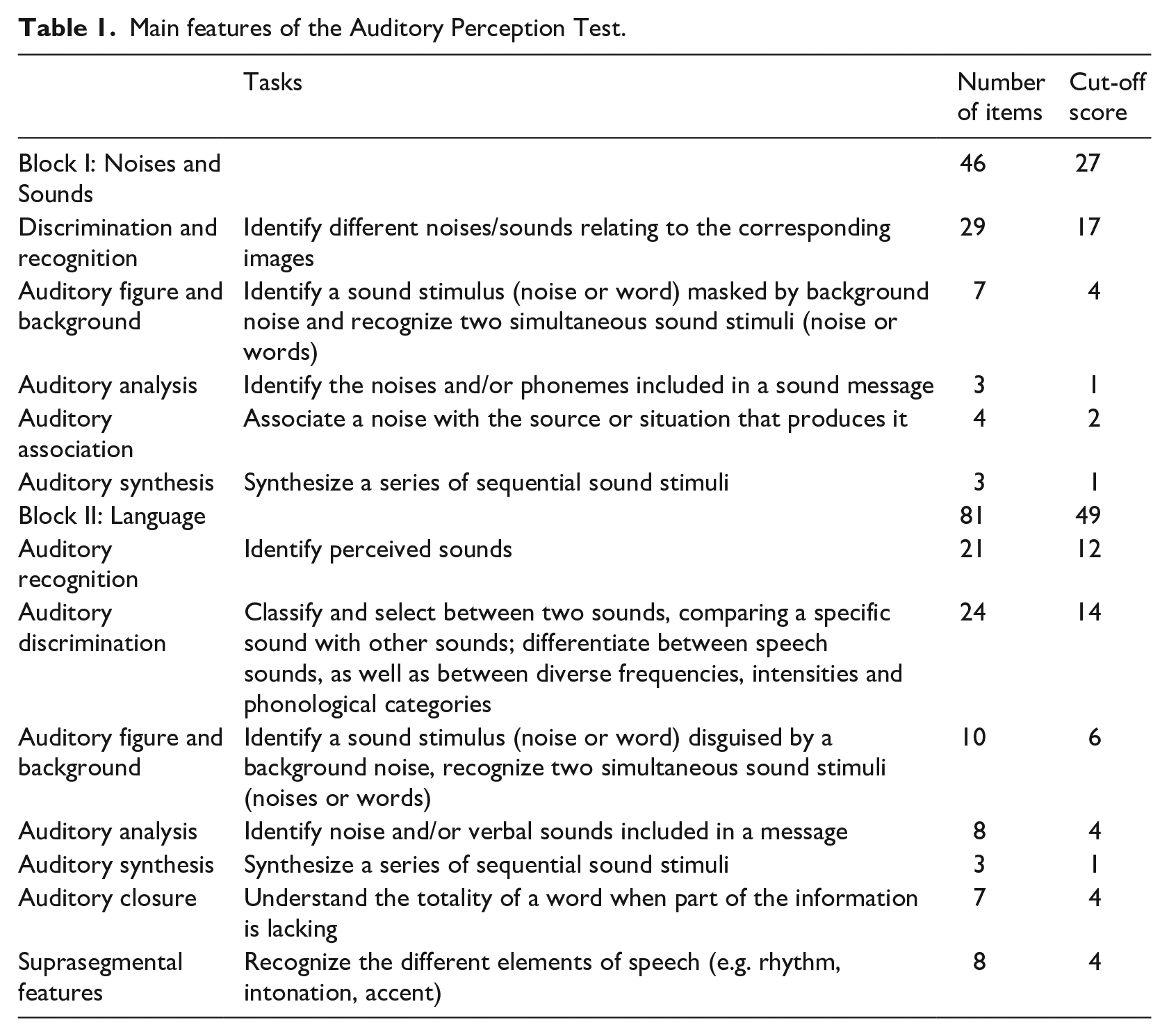
A specific test developed in Spanish by Gotzens-Busquets and Marro-Cosialls (2001) was used to assess auditory perception. This test includes a series of tasks to analyse independently the skills related to the perception of linguistic and not-linguistic sounds. It has a total of 127 items, all to be scored as correct or incorrect, distributed in two blocks: (1) Noises and Sounds and (2) Language. As the number of items in subscales ranged from 3 to 29 and percentages would be presented along with scores (means and standard deviations), authors agreed that 60.0% or less of total items answered correctly would be considered low performance whereas 60.1% or more of total items would be considered good performance. That is, a subscale with only 3 items, would classify a score of 2 out 3 (66.6%) correct answers as good performance, and of 1 out of 3 (33.3%) as low performance. The rationale was to set the cut-off score above chance (50.0%) for the subscales with an even number of items, while being conservative considering the disadvantageous clinical profile of the children (i.e. profound bilateral hearing loss, with no cochlear implants, not having ever received AVT) and setting a cut-off criterion that could be used in subsequent studies with different samples. Table 1 summarizes the tasks of the two blocks and their corresponding subscales along with their number of items and cut-off points.
Main features of the Auditory Perception Test.
4 Statistical analysis
Percentages of children scoring below the cut-off and mean scores calculated for the individual subscales and overall blocks served to analyse the auditory perception profile of children in both conditions (before and after completing AVT). T-tests for independent samples explored the differences by sex. Comparisons (before and after completing AVT) of percentages with chi-square tests and of mean scores with a series of t-tests for related samples explored possible improvements in auditory perception. A significance value of .05 was adjusted for Bonferroni correction to a value of .004, considering a total of 12 subscales comparisons. SPSS v.20 was the software package for all statistical analyses.
III Results
After presenting some features of the sample, results are reported following the order from Section II.4. Regardless of having begun AVT, 1case dropped-out after the second session. The final sample included 25 children (52% girls and 48% boys), most from urban communities (64%) and nuclear families (68%). All were in school: 3 (12%) in preschool and 22 (88%) in elementary school. Age at diagnosis ranged from 2 to 7 years (2 years 8 months to 7 years 0 months) with an average of 4.65 (SD±1.49) years. Age at initial assessment ranged from 5 to 8 years (5 years 2 months to 8 years 4 months) with an average of 7.32 (SD±0.86) years. Time since diagnosis ranged from 0.83 to 5.50 years (10 months to 5 years 6 months) with an average of 2.67 (SD ±1.46) years. No significant differences by sex were found for any of these three variables. Data is presented in Appendix 3 in supplemental material.
As a standard procedure, the hearing response of every child attending AYPRODA is tested at the levels of 1, 2, 4 and 8 kHz by a certified audiologist. The audiometric threshold for the participating children was obtained from their clinical records. Considering the four responses for each level, hearing capacity in each ear ranged from under 90 db to under 120 db. Threshold under 90 db was the most common for both, right (n = 19) and left ear (n = 18). For the right ear 2 cases were under 100 db and 4 cases under 120 db. For the left ear 4 cases were under 100 db and 3 cases under 120 db. Although levels show profound hearing loss for both ears, 7 children had a milder hearing loss in the right ear, 7 children had a milder hearing loss in the left ear, and 11 were even.
It can be observed (Table 2) that overall, the children performed better on the Noises and Sounds section (64% scoring above the cut-off) than on the Language section (48% scoring above the cut-off). In two of the five Noises and Sounds subscales, more than half the children scored below the cut-off before AVT (range 64%–76%), but less than a fifth did so after AVT for all subscales (range 0%–16%). In the Language section, more than half (range 68%–100%) the children scored below the cut-off in three of the seven subscales before AVT, which decreased notably (range 52%–72%) after AVT. The Auditory Figure and Background, and Suprasegmental Features subscales, both of the Language block, were the most difficult for the children; all (100%) scored below the cut-off in before AVT. Improvements after AVT were observed with below cut-off percentages dropping to 64% (Auditory Figure and Background) and 72% (Suprasegmental Features). Auditory Analysis, also of the Language section, was the third most difficult subscale with 68% scoring below the cut-off before AVT and 52% after. The most challenging subscales in the Noises and Sounds section were Auditory Figure and Background (76% below cut-off) and Auditory Synthesis (64% below cut-off). After AVT these percentages dropped to 16% and 12%, respectively. Before AVT, in the Noises and Sounds block, the children did best in the Auditory Recognition subscale (0% below cut-off), followed by the Auditory Analysis subscale (4% below cut-off). After AVT, all the children were able to correctly answer these subscales.
Comparison of Auditory Perception Test results before and after auditory verbal therapy (n = 25).
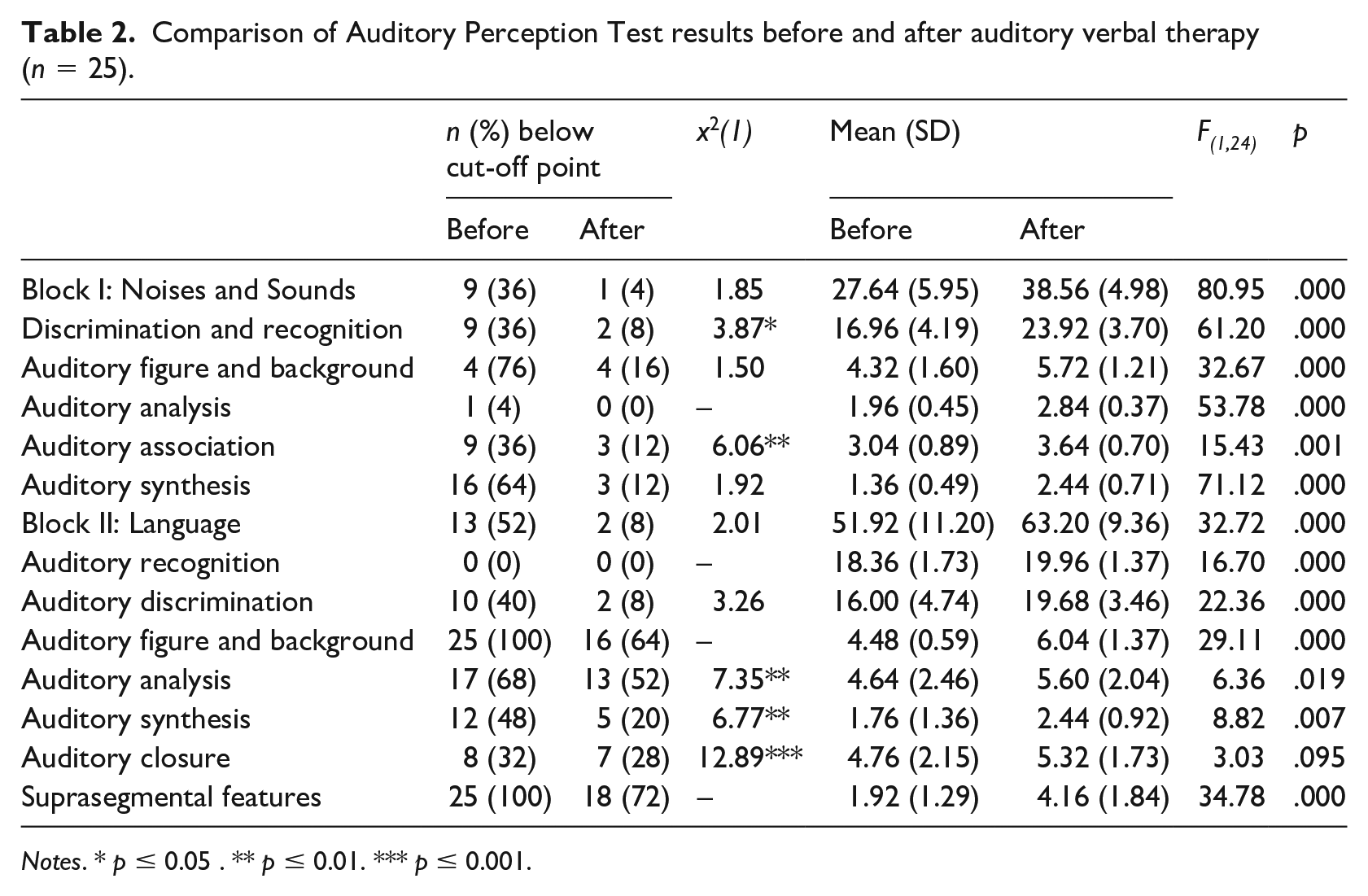
Notes. * p ≤ 0.05 . ** p ≤ 0.01. *** p ≤ 0.001.
Before AVT, the boys scored significantly higher than the girls only in Noises and Sounds block (t(23) = 2.11, p = .05) and its Auditory Association subscale (t(23) = 2.19, p = .04). Improvement was observed in both groups; yet, boys still scored significantly higher than girls after AVT: Noises and Sounds (t(23) = 2.40, p = .03), and Auditory Association (t(23) = 2.80, p = .01). The girls initially scored significantly higher than the boys in the Auditory Recognition subscale (t(23) = −2.05, p = .05), though this discrepancy disappeared after AVT. Figure 1 presents graphically the individual scores by block. Appendix 4 in supplemental material presents the individual scores for subscales and blocks before and after AVT. Appendix 5 in supplemental material presents graphically scores before and after AVT per child.
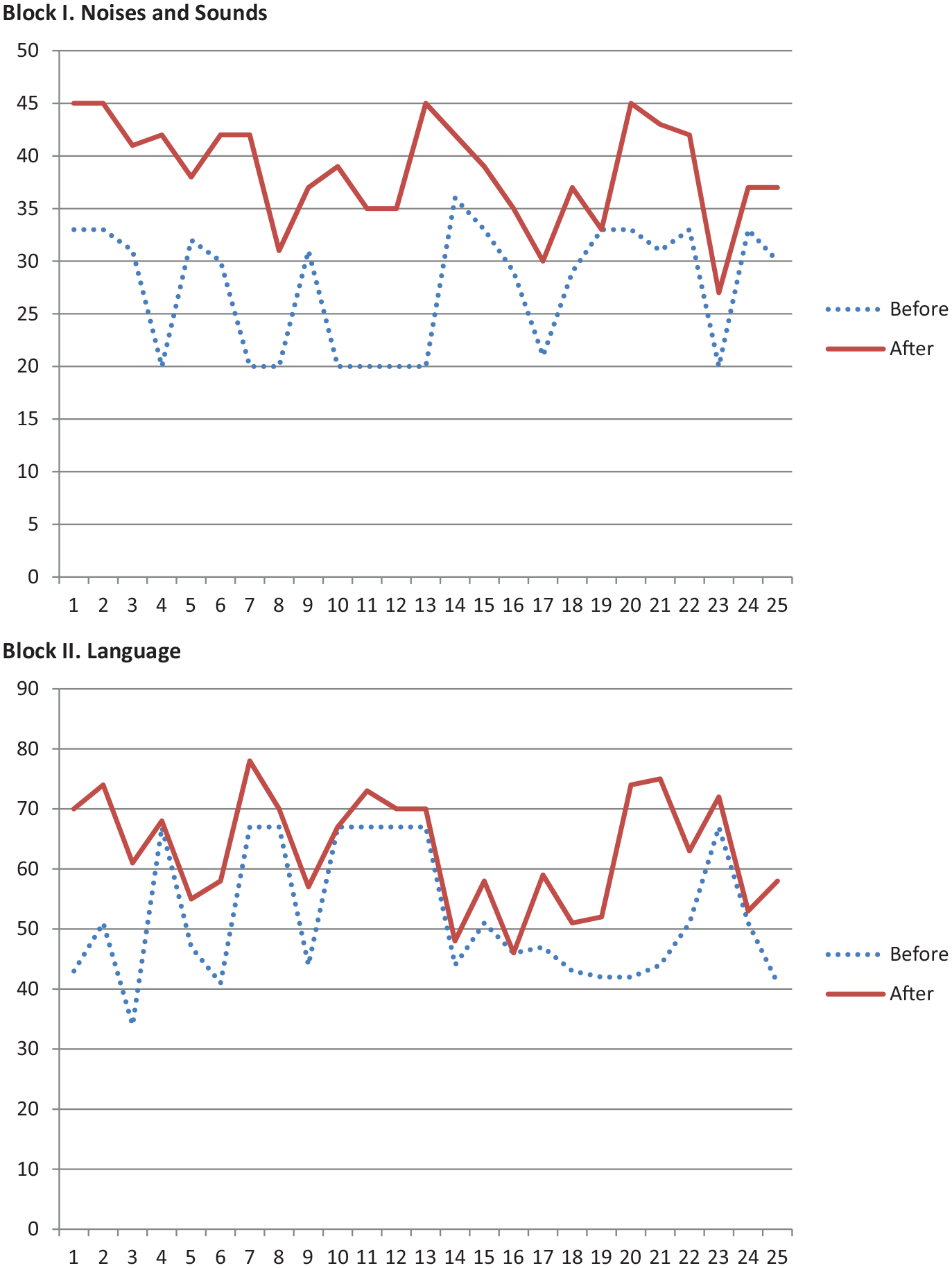
Individual scores before and after auditory-verbal therapy (AVT).
A series of t-tests showed that significant improvement (p ⩽ 0.05) after AVT occurred in global scores for Noises and Sounds and for Language blocks, regardless of sex, urban or rural community origin, nuclear or extended family. Nevertheless, in regard to current school grade, the 3 pre-schooled children showed no significant improvement in either block. Bivariate Pearson correlations showed that age at diagnosis and age before AVT were not significantly related to the global scores of either block.
Though not always at a significant level, comparison of before and after AVT outcomes suggests AVT might help improving auditory perception. Statistically significant changes were observed only in the Discrimination and Recognition and Auditory Association subscales (Noises and Sounds block), and the Auditory Analysis, Auditory Synthesis, and Auditory Closure subscales (Language block). Case distribution sometimes precluded application of the x2 test, even so, the percentage of below cut-off scores still declined. T-tests showed that all but one subscale (Auditory Closure) exhibited significant improvements after AVT, particularly in the Noises and Sounds block.
IV Discussion
Although cochlear implants would be highly recommended for children with hearing loss, in developing countries such as Mexico, financial constraints and cultural conditions frequently make this technology inaccessible (Gerner de Garcia et al., 2011). Prevailing conditions in Mexico mean implants are not a viable treatment option for a large majority of the population, and therefore treatment models need to be developed and updated in accordance with the population’s possibilities (Madriz, 2000). Under these circumstances, the present study aimed at analysing auditory perception in a sample of Mexican children with profound hearing loss using hearing aids and possible improvements after receiving auditory verbal therapy.
Hearing loss in newborns is likely to stay unnoticed by lay hearing parents, as babies instinctively produce cooing and babbling sounds. Language, by signed or spoken words, will continue to develop; yet, children with hearing loss will not show progress in their spoken language. If not detected, spoken language delay may be prolonged and by the time schooling starts, children may already show a significant underdevelopment. Language, spoken and/or signed, is vital for the child’s integral growth, facilitating learning and social interaction.
Profound bilateral hearing loss can have negative impacts on quality of life, especially when it begins in early childhood. If therapeutic measures are not initiated in the neonatal or nursing stage a child’s developmental and learning processes can be compromised (Johnson et al., 2016).Absence of a hearing loss diagnosis during neonatal screening is one of the main causes delaying the timely treatment that can limit the consequences of hearing loss (Thompson et al., 2001). The present study is a good example of this since average age at diagnosis was four years, that is, the age at which it became obvious to adults that the child could not hear properly. Even after diagnosis, it took an average of two more years before the child was fitted with hearing aids and provided with AVT; that is, an average of six years between birth and treatment. These are vital years in a child’s spoken language development, and the loss of this extremely important stimulation can pose serious challenges to full integration into society (Nicholas and Geers, 2007). It is worth to mention that in addition to receiving attention at AYPRODA, the studied children regularly attended public schools not provided with programs for students with disabilities and applying the same type of teaching techniques to all students. In terms of development, this can be favourable for children with hearing loss because it provides stimulation and generates no stigmas or differences as they coexist with other children who can collaborate with them in adapting to their social surroundings. Research indicates that children with hearing loss in inclusive settings face great difficulties in communicating, initiating/entering, and maintaining interactions with hearing peers. Yet, interactions with peers provide opportunities to practise competencies for establishing interpersonal relationships, thus specific programs to help them develop friendships and prevent isolation must be implemented in mainstream schools (Batten et al., 2014; Xie et al., 2014).
Regarding initial auditory perception skills, children performed better on the Noises and Sounds block than on the Language block. Noises and Sounds tasks, representing the skills to differentiate timbre, intensity and duration, continuity and impact of the stimulus, are simpler, demanding the child only to perceive and discriminate a stimulus (e.g. raise his hand when perceiving a particular sound). Language tasks, focused on the system of signs used to communicate orally, are more complex, they require not only to perceive and discriminate but also to interpret and answer (e.g. the child is presented the audio of a dog barking and is expected to hear it, understand it and point out of a series of images the one that represents it while at the same time say in words what he hears, ‘a dog is barking’).
By subscales, top performance was observed for auditory analysis (Noises and Sounds), that is the ability to identify the noises and/or phonemes included in a sound message, and auditory recognition (Language), that evaluates the sound qualities and onomatopoeias and the auditory recognition at the level of word, phrase and speech. This might be due to both being simple tasks that demand only perception and identification. On the other hand, auditory figure and background (in both, Noises and Sounds and Language blocks), were the subscales the children had more difficulties with. Auditory figure from language assesses the child’s ability to identify sounds masked by noise or other simultaneous stimuli and to differentiate two sounds that occur simultaneously, while auditory figure from noises and sounds, though similar to the one from language, it only identifies sounds but not their intensity. Also, auditory synthesis (Noises and Sounds), requiring the identification of what is occurring in a particular scene/situation by what is heard, and suprasegmental features (Language), that is, discrimination by the intonation the intention of the speaker, e.g. questioning, being happy, were also difficult scales. These subscales present more complex tasks requiring active attention and memory to identify morphemes and phonemes, to repeat them accurately and/or integrate the information in temporal sequences.
Though not the primary focus of this study, the results showed similar participation rates and profiles in boys and girls. Some differences were observed in the initial test of audio-verbal abilities, with boys scoring higher in the Noises and Sounds section and girls in Auditory Recognition. These differences were not present in the final test scores, suggesting that both sexes responded satisfactorily to AVT. This differs from previous studies in other contexts showing that women perform better than men in auditory and verbal abilities for biological and cultural reasons (Jacobsen et al., 2017; McFadden, 2011; Strelnikov et al., 2009).
Research has evidenced a positive effect of AVT for improving auditory perception in children with hearing impairments (Brennan-Jones et al., 2014; Dornan et al., 2009; Kaipa and Danser, 2016; Rhoades, 2006). Here, AVT was applied to a group of children characterized not only by a profound bilateral hearing loss but also by using hearing aids in default of cochlear implants. Auditory perception improved most notably in the Discrimination and Recognition, and Auditory Association subscales of the Noises and Sounds section, which has been reported elsewhere (Reetzke et al., 2016). It also improved in the Auditory Analysis, Auditory Synthesis and Auditory Closure subscales of the Language section, again, these results are similar to those of previous studies (Dijk et al., 2016; Richards and Goswami, 2015). These results suggest AVT might help improve auditory perception in these children; yet, due to the study design limitations (lack of control group, non-randomization, poor control of background variables, no follow-up) no conclusions can be drawn in regard to the effectiveness of this therapy. Differences in the auditory perception of these children previous to receiving AVT and also in their level of improvement after AVT might be attributed to the interaction of various intrinsic (e.g. intelligence level, motivation to learn, level of cognitive development, self-confidence, audiometric threshold, learning style) and environmental (e.g. expertise of the therapist, child-therapist rapport, family functionality and commitment to therapy, daily stimulation of spoken language at home and at school, type of schooling (regular vs. special needs), optimal functioning and daily use of hearing aids) factors. These variables must be considered for subsequent designs aiming at testing the effectiveness of AVT with an experimental design. The lack of well-controlled studies addressing the effectiveness of AVT has been acknowledged (Brennan-Jones et al., 2014; Dornan et al., 2009; Kaipa and Danser, 2016; Rhoades, 2006); this calls for more rigorous experimental designs that might be possible through multi-centre research. Furthermore, collaborative research might open an opportunity for offering auditory verbal therapy to children with profound bilateral hearing loss from diverse locations and backgrounds who, due to economic constraints, are unlikely to receive cochlear implants timely.
V Conclusions
The implementation of AVT in children with hearing loss should be considered to improve their auditory perception. Future studies are needed to analyse the effectiveness of AVT and explore the relationship between the different dimensions of auditory perception.
Supplemental Material
6_Estrella_et_al._AVT_-_Appendix_1 – Supplemental material for Auditory perception of Mexican children with profound bilateral hearing loss receiving auditory verbal therapy
Supplemental material, 6_Estrella_et_al._AVT_-_Appendix_1 for Auditory perception of Mexican children with profound bilateral hearing loss receiving auditory verbal therapy by Damaris F Estrella-Castillo, Héctor Rubio-Zapata and Lizzette Gómez-de-Regil in Child Language Teaching and Therapy
Footnotes
Acknowledgements
The authors thanks AYPRODA (Asociación Yucateca Pro Deficiente Auditivo / Yucatecan Association Pro-Hearing Impaired), Yucatan, Mexico, for all the facilities and support, and to all those families that kindly agreed to participate.
Contribution of authors
All authors contributed to the concept and design of the work, to the acquisition, analysis and interpretation of data. All authors drafted the article and revised it critically, and take public responsibility for its content.
Declaration of conflicting interests
The Authors declare that there is no conflict of interest
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.