
Abstract
Background
Veno-arterial extracorporeal membrane oxygenation (V-A ECMO) is used for refractory cardiogenic shock, yet optimal weaning strategies and the role of left ventricular (LV) venting remain unclear. The TWEET-1 study was designed as an early feasibility investigation to define processes, timelines, and clinical parameters for future interventional trials evaluating Impella 5.5 for LV venting during V-A ECMO support.
Methods
This prospective, single-center observational study from 2021 to 2025 included patients who received standard-of-care V-A ECMO and Swan-Ganz monitoring. Patients were assigned to the ECPELLA + group (defined as the addition of Impella 5.5 to V-A ECMO to provide left ventricular unloading) when pulmonary artery (PA) diastolic pressure exceeded 20 mm Hg; other individuals served as controls. The primary outcome was survival to discharge. Secondary outcomes included V-A ECMO duration, complications, and SAVE score–adjusted survival.
Results
Among 117 screened patients, 43 were enrolled (25 ECPELLA +, 18 controls). Overall survival to discharge was 53% with no significant difference between groups. ECPELLA + patients had higher pulmonary pressures and longer V-A ECMO support but demonstrated appropriate selection for unloading. Both groups exceeded the SAVE score–predicted survival. Subgroup analysis suggested potential benefit of Impella venting in the most severe patients (SAVE −14 to −10).
Discussion
Hemodynamic-guided LV venting with Impella 5.5 during V-A ECMO was feasible and enabled prompt LV unloading (ECPELLA). While survival to discharge did not differ significantly between groups, patients with higher PA diastolic pressures and SAVE scores below −10 demonstrated a significant reduction in mortality with LV unloading.
Conclusion
Early hemodynamic-guided LV unloading may improve risk-adjusted V-A ECMO outcomes.
Introduction
Veno-arterial extracorporeal membrane oxygenation (V-A ECMO) is widely used for refractory cardiogenic shock, despite a lack of clinical trial evidence.1,2,3 While it is relatively easy to deploy and effective for reversing hemodynamic collapse and metabolic derangements, it may hinder left ventricular (LV) recovery 4 and cause lung injury, 5 access-related complications, 6 and bleeding.7,8 Several studies have identified risk factors, outcome predictors, and risk scores (SAVE and ENCOURAGE). A few small observational studies have described specific strategies for weaning from V-A ECMO.1,2,9–13 However, as of November 2025, detailed weaning strategies after V-A ECMO initiation for refractory cardiogenic shock have not been uniformly adopted.
LV venting is considered standard of care on a case-by-case basis, but limited prospective data on criteria and timing have prevented the establishment of universal guidelines. In severe pulmonary edema, most physicians use surgical or percutaneous LV venting. In addition to upfront LV venting, the Impella device is used as a rescue strategy when V-A ECMO weaning has failed.
Because clinical investigations in V-A ECMO populations are challenging, the primary objective of this observational early feasibility study (TWEET-1) was to define the timeline, clinical data requirements, personnel, and logistics necessary for future interventional or randomized trials. Specifically, we evaluated Impella 5.5 (Abiomed) for LV venting in patients receiving V-A ECMO support (ECPELLA + group) versus conventional V-A ECMO without LV venting (control group) with respect to weaning and survival. The secondary objective was to compare clinical outcomes between groups.
Methods
We screened all V-A ECMO candidates between January 1, 2021, and January 1, 2025. The decision to initiate V-A ECMO was made on a case-by-case basis by our multidisciplinary team, comprising a board-certified critical care physician, cardiothoracic surgeon, interventional cardiologist, and heart failure physician, per our institutional V-A ECMO protocol. All patients were treated according to the current standard of care. To reflect real-world practice, we did not limit inclusion based on the underlying cardiogenic shock etiology, as the specific cause is often defined at the time of or after the decision to cannulate V-A ECMO.
The primary objective of this observational study was to design and collect an extensive prospective dataset to analyze V-A ECMO outcomes at a Platinum-tier Extracorporeal Life Support Organization (ELSO) center, with a particular focus on the effect of early LV venting using the Impella 5.5 before V-A ECMO weaning. The primary endpoint was survival to discharge. Secondary endpoints included duration of V-A ECMO support, length of hospital stay, rates of cardiac recovery (survival free from mechanical circulatory support [MCS]), heart transplantation or inotropic support at 30 days, prevalence of V-A ECMO-driven complications as defined by ELSO, SAVE scores, and survival adjusted to SAVE score (cumulative inotropic dose and inotropic score).
We adopted the ELSO-endorsed SAVE (Survival After Veno-Arterial ECMO) score 12 for V-A ECMO risk stratification. It includes 17 clinical, hemodynamic, and respiratory variables and predicts survival for adult patients undergoing V-A ECMO for refractory cardiogenic shock. 12 Demographic, clinical, and biochemical data needed to calculate individual SAVE scores were available for all patients. SAVE scores were calculated using the online calculator (https://www.elso.org/savescore/index.html).
All patients received a Swan-Ganz catheter at the time of V-A ECMO placement or within 24 h of admission. Pulmonary pressure was continuously monitored. A pulmonary artery (PA) diastolic pressure >20 mm Hg was used as the hemodynamic trigger for escalation to Impella 5.5, selected to prompt LV unloading before the development of pulmonary edema and lung injury as previously described. 10 Time to Impella 5.5 placement was intentionally variable, with escalation initiated once PA diastolic pressure crossed the 20-mm Hg threshold to individualize the decision to each patient’s hemodynamic profile. Once diastolic pulmonary pressure was consistently >20 mm Hg, the patient was implanted with an Impella 5.5 and assigned to the ECPELLA + group. Patients who did not receive Impella 5.5 during V-A ECMO were included in the control group. PA diastolic pressure and insertion time were recorded.
The UTHealth Houston Institutional Research Board approved the study protocol (HSC-MS-21-0286).
Statistical analysis
We compared demographic, clinical, and outcome variables between the ECPELLA + and control groups, which were calculated using the non-parametric Wilcoxon signed-rank tests that do not have assumptions about the distributions of the variable, and chi-square tests were used for categorical variables.
To benchmark survival, we estimated the probability of surviving to discharge using the SAVE score, a logistic regression model with binary survival status at discharge as the dependent variable and the SAVE score as the independent variable. Paired t-tests were used to compare the probability of survival for the different levels of SAVE scores to the corresponding survival probability published by Schmidt M et al. 12 Results are presented in tables with medians and interquartile ranges for the survival probabilities.
All analyses were performed using Stata version 18.0 (College Station, TX), with p-values ≤0.05 considered statistically significant.
Results
TWEET-1 study phases and delayed definition of inclusion & exclusion criteria
To identify strengths and weaknesses after a prolonged enrollment period, the TWEET-1 pilot study concluded on January 1, 2025, before full enrollment was completed. A total of 117 patients were screened, and 43 patients (25 ECPELLA +, 18 controls) were enrolled.
Original and revised inclusion criteria.
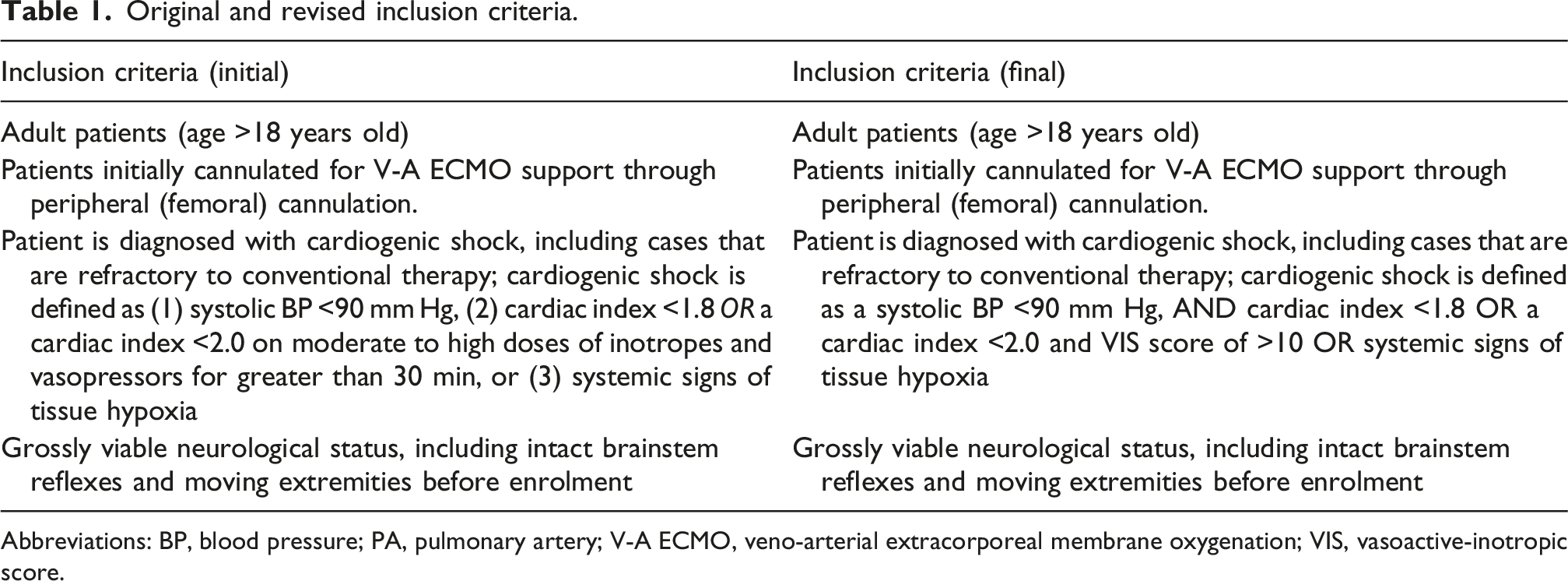
Abbreviations: BP, blood pressure; PA, pulmonary artery; V-A ECMO, veno-arterial extracorporeal membrane oxygenation; VIS, vasoactive-inotropic score.
Original and revised exclusion criteria.
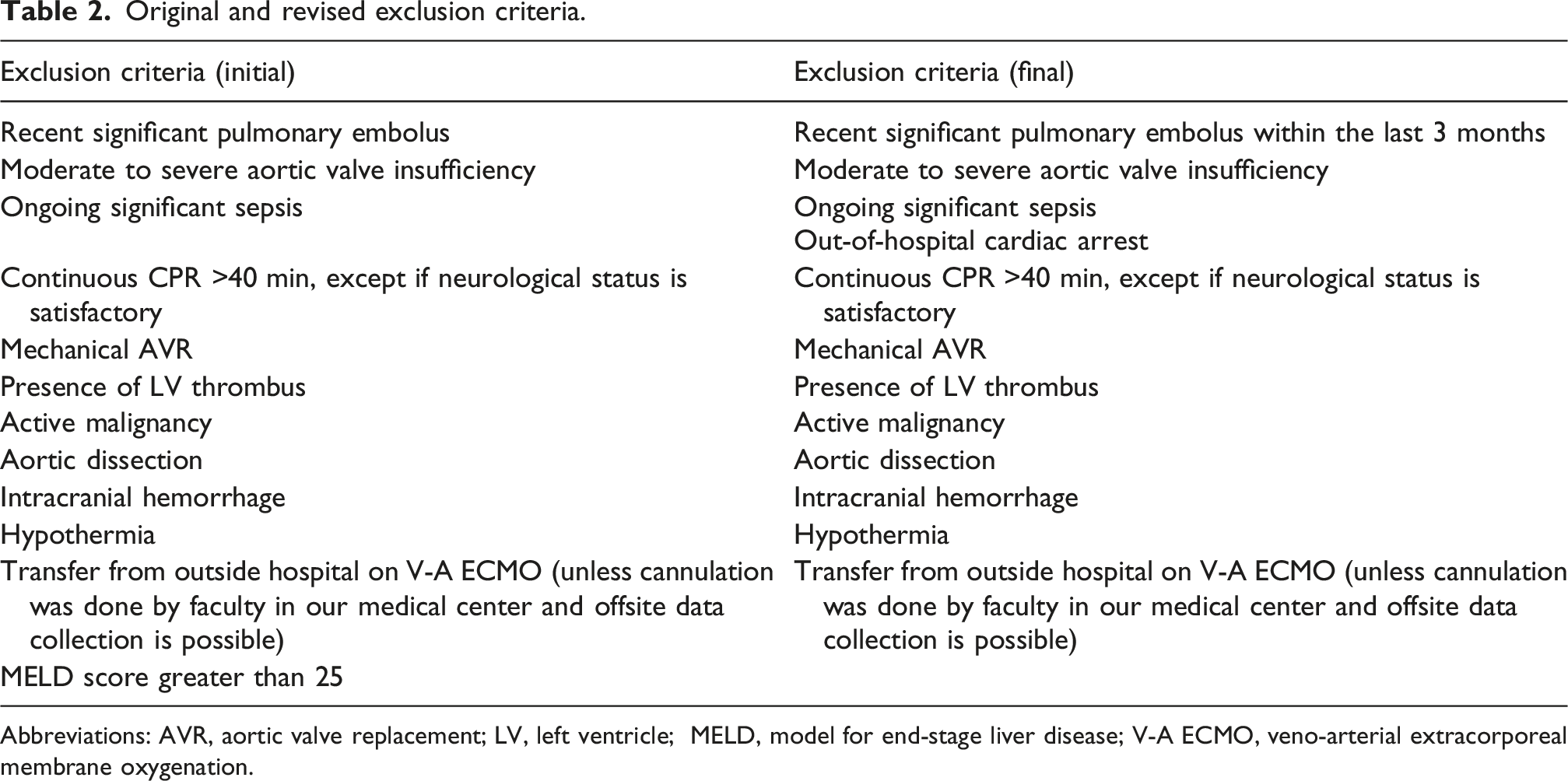
Abbreviations: AVR, aortic valve replacement; LV, left ventricle; MELD, model for end-stage liver disease; V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
Enrollment proceeded in two phases. During Phase 1 (October 2021–January 2023), 24 patients were screened under the original criteria, with three enrolled (88% screen failure). Following IRB approval of a revised protocol with modified exclusion criteria, Phase 2 (February 2023–January 2025) screened 93 patients and enrolled 40 (57% screen failure). The three Phase 1 patients met both original and revised criteria and were retained in the final analysis. Perfusionists were integrated into the data collection workflow to enable real-time prospective data capture during ECMO support, improving data quality and completeness.
Overall patient characteristics and outcomes
Baseline characteristics, primary endpoints, and secondary endpoints for the full TWEET-1 cohort (n = 43).
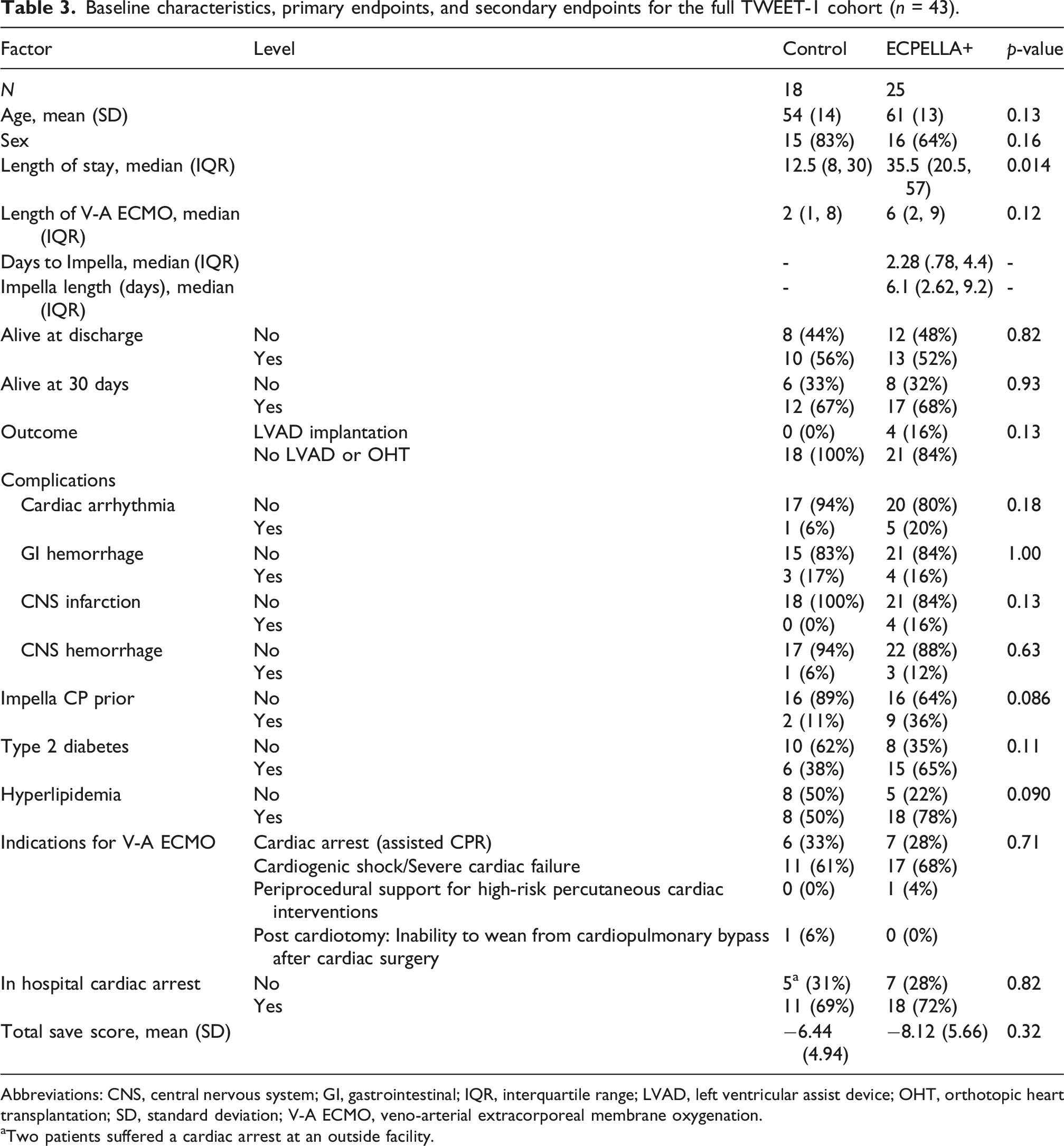
Abbreviations: CNS, central nervous system; GI, gastrointestinal; IQR, interquartile range; LVAD, left ventricular assist device; OHT, orthotopic heart transplantation; SD, standard deviation; V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
aTwo patients suffered a cardiac arrest at an outside facility.
When grouped by underlying etiology, there was no significant difference in indications for V-A ECMO, which included cardiac arrest, cardiogenic shock, acute decompensation, periprocedural support for high-risk interventions, and post-pericardiotomy syndrome. None of the patients in the control group underwent LVAD or transplant during the index hospitalization. In contrast, four patients (4/25, 16%) were transitioned from Impella 5.5 to LVAD as part of our current practice.
A significant fraction of patients (29/43, 67%) had in-hospital cardiac arrest. The rate did not differ between groups (p = 0.82): 18 patients (18/25, 72%) in the ECPELLA + group versus six patients (11/16, 69%) in the control group. Only two patients in the control group had an outside hospital witnessed arrest; all arrests in the ECPELLA + group occurred in-hospital.
Two patients (2/18, 11%) in the control group had Impella CP placed before V-A ECMO. In comparison, 9 patients (9/25, 36%) in the ECPELLA + group initially had an Impella CP that required an upgrade to V-A ECMO and, eventually, Impella 5.5 (p = 0.086).
Demographics, comorbidities, and inotropic score
On univariate analysis, demographic characteristics and comorbidities (sex, BMI, hypertension, diabetes, dyslipidemia) did not differ between groups. Mean SAVE scores were similar (−8.12 ± 5.66 in the ECPELLA + group vs −6.44 ± 4.94 in the control group; p = 0.32).
Length of V-A ECMO support
The median length of stay was longer in the ECPELLA + group (35.5 days, interquartile range [IQR] 20.5–57) than in the control group (12.5 days, IQR 8–30) (p = 0.014). Similarly, the median length of V-A ECMO support was longer in the ECPELLA + group (6 days, IQR 2–9) than in the control group (2 days, IQR 1–8) (p = 0.12). The median time to Impella 5.5 from V-A ECMO implant was 2.28 days (IQR 0.78–4.4). Once implanted, the median length of Impella support was 6.1 days (IQR 2.6–9.2).
Complications during V-A ECMO support
There was no statistical difference between the control and ECPELLA + groups for the four most prevalent complications patients may experience during V-A ECMO support: arrhythmias (control 6% vs ECPELLA + 20%; p = 0.18), gastrointestinal hemorrhage (control 17% vs ECPELLA + 16%; p = 1.00), central nervous system (CNS) infarction (control 0% vs ECPELLA + 16%; p = 0.13), and CNS hemorrhage (control 6% vs ECPELLA + 12%; p = 0.63) (Table 3).
Patients without cardiac arrest (no ECPR): Demographics, comorbidities, and outcomes
Primary and secondary outcomes in patients without cardiac arrest (no ECPR).
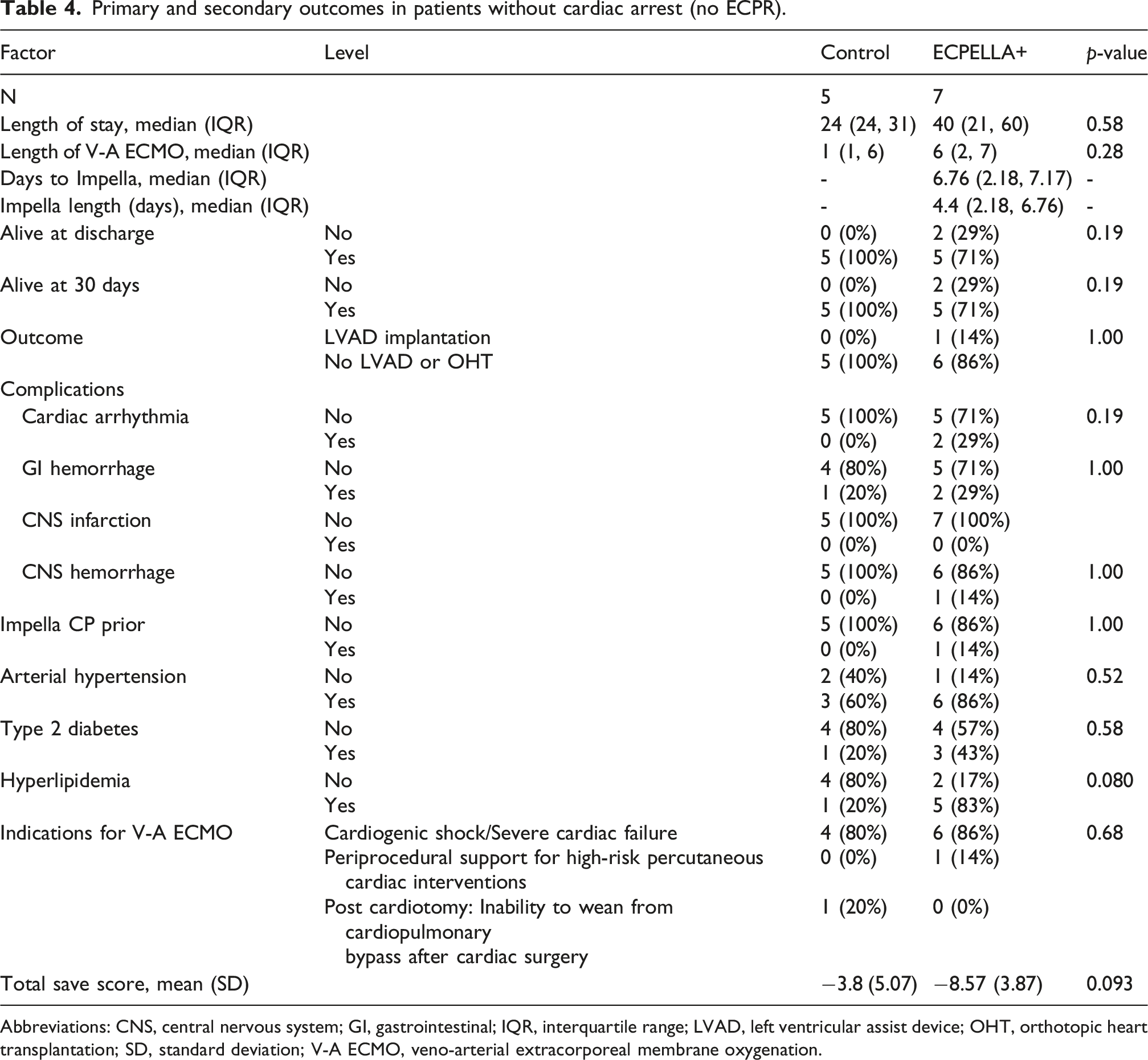
Abbreviations: CNS, central nervous system; GI, gastrointestinal; IQR, interquartile range; LVAD, left ventricular assist device; OHT, orthotopic heart transplantation; SD, standard deviation; V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
When grouped by underlying etiology, there was no significant difference in the indications for V-A ECMO (cardiogenic shock, periprocedural support for high-risk interventions, and post-pericardiotomy syndrome) between the groups. None of the patients in the control group and one patient in the ECPELLA + group underwent LVAD or transplant as part of the index hospitalization. Demographic characteristics and comorbidities (sex, BMI, hypertension, diabetes, dyslipidemia) were also similar. Mean SAVE scores were −8.57 ± 3.87 in the ECPELLA + group versus −3.8 ± 5.07 in the control group (p = 0.093).
Both the median length of stay (40 days, IQR 21–60 vs 24 days, IQR 24–31; p = 0.58) and length of V-A ECMO support (6 days, IQR 2-7 vs 1 day, IQR 1-6; p = 0.28) were longer in the ECPELLA + group than in the control group. The time to Impella 5.5 implantation from V-A ECMO implant was 6.7 days (IQR 2.2–7.2). The median length of Impella 5.5 support was 4.4 days (IQR 2.1–6.7). There was no significant difference between the groups in arrhythmias, gastrointestinal hemorrhage, CNS infarction, or CNS hemorrhage.
Patients with cardiac arrest (ECPR): Demographics, comorbidities, and outcomes
Primary and secondary outcomes in patients with cardiac arrest (received ECPR).
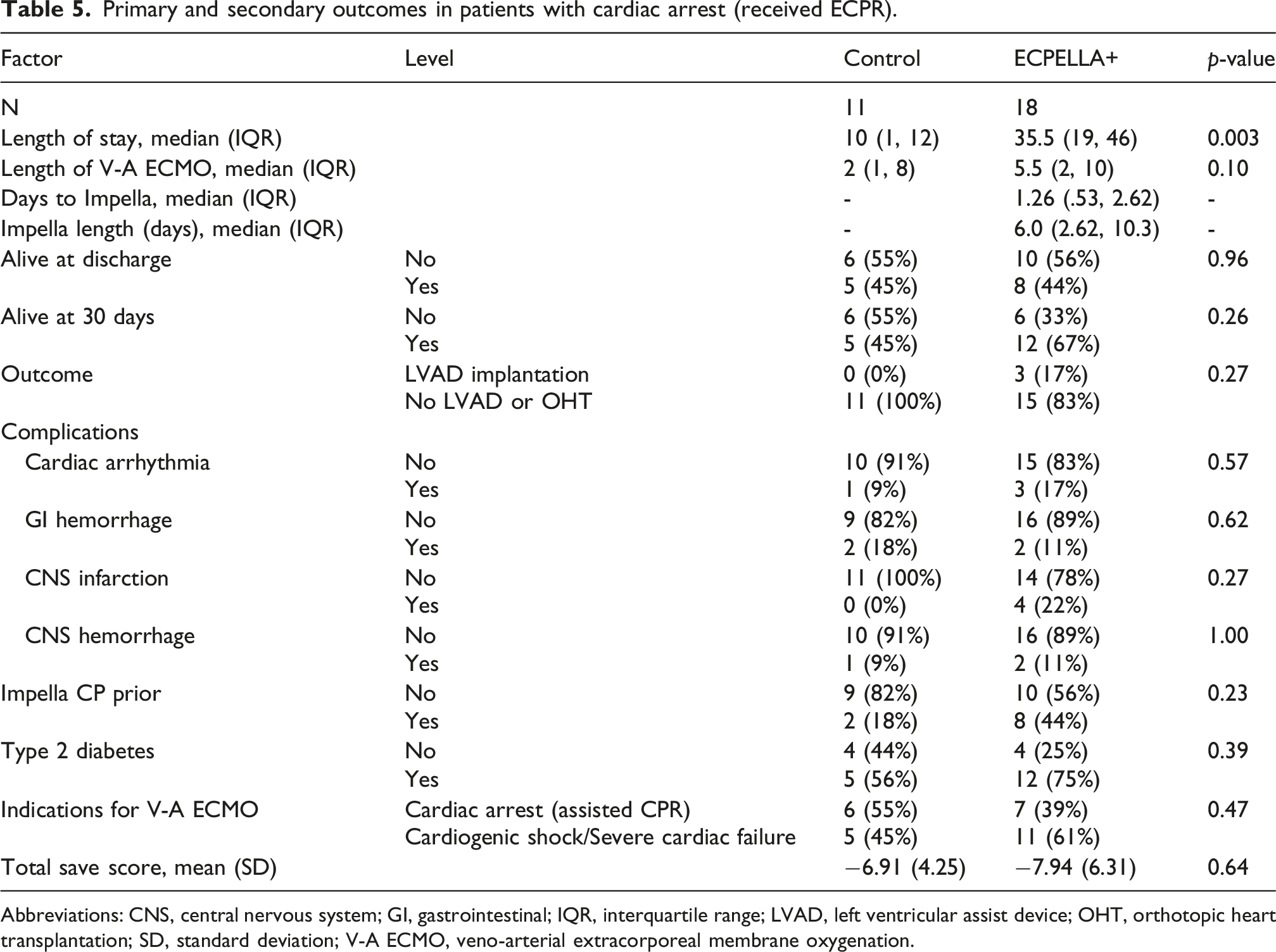
Abbreviations: CNS, central nervous system; GI, gastrointestinal; IQR, interquartile range; LVAD, left ventricular assist device; OHT, orthotopic heart transplantation; SD, standard deviation; V-A ECMO, veno-arterial extracorporeal membrane oxygenation.
Overall, 13 patients survived to hospital discharge (13/29, 45%); eight were in the ECPELLA + group (8/18, 44%) and 5 were in the control group (5/11, 45%). Although survival with ECPELLA + was higher at both 30 days (67% vs 45%, p = 0.26) and at discharge (45% vs 44%, p = 0.96), these differences were not statistically significant. Indications for V-A ECMO—cardiac arrest and cardiogenic shock—were similar between groups (Table 5).
None of the patients in the control group underwent LVAD or transplant during the index hospitalization, whereas 3 patients in the ECPELLA + group (3/18, 17%) were transitioned from Impella 5.5 to LVAD (p = non-significant).
Demographic characteristics and comorbidities (sex, BMI, hypertension, diabetes, dyslipidemia) were similar between groups with similar mean SAVE scores (−7.94 ± 6.31 in the ECPELLA + group vs −6.91 ± 4.25 in the control group; p = 0.64).
The median length of stay was longer in the ECPELLA + group (35.5 days, IQR 19–46) than in the control group (10 days, IQR 1-12) (p = 0.003). Similarly, the median length of V-A ECMO support was longer in the ECPELLA + group (5.5 days, IQR 2-10) than in the control group (2 days, IQR 1-8) (p = 0.10). The median time from ECMO to Impella placement in the ECPELLA + group was 1.26 days (IQR 0.53–2.62), and Impella support lasted a median of 6.0 days (IQR 2.6–10.3).
Rates of arrhythmias, gastrointestinal hemorrhage, CNS infarction, and CNS hemorrhage were similar between groups.
Pulmonary pressure and strategy selection
During enrollment, all patients received a Swan-Ganz at ECMO initiation, causing variation in initial PA pressure timing and patient selection for Impella. Over the full study period, 25 patients were enrolled in the ECPELLA + arm and 18 in the control arm. The mean PA pressure after V-A ECMO and before Impella deployment was 29 ± 12 mm Hg in the ECPELLA + arm versus 18 ± 5 mm Hg in patients who did not receive Impella 5.5 (p < 0.005). This demonstrates the appropriate selection of patients with higher mean PA pressure post V-A ECMO to receive LV venting.
SAVE score-adjusted survival
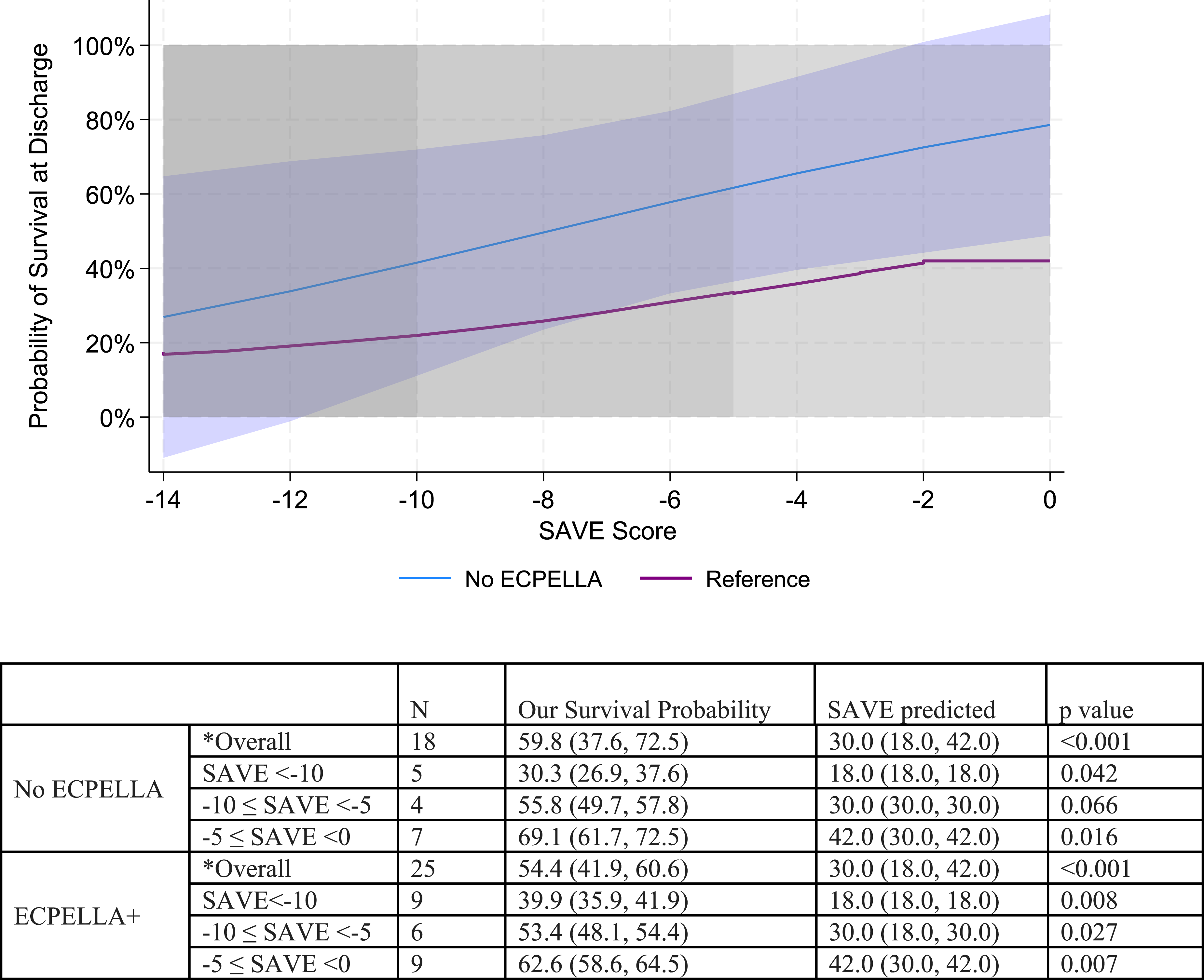
We compared observed survival to discharge with SAVE score-predicted survival. Because of the exploratory design, the current stage of the TWEET registry, SAVE score heterogeneity, and small group sizes, we clustered patients into three SAVE score groups: −14 to −10, −10 to −5, and > −5 (Figure 1). We compared survival to discharge in each observed SAVE score cluster against the predicted survival of patients with similar SAVE scores. Both the ECPELLA + and the control groups significantly outperformed the SAVE score match-predicted survival in all SAVE clusters. However, overall survival to discharge did not differ significantly between the ECPELLA + group (54.4%, confidence interval [CI] 41.9–60.6) and the control group (59.8%, CI 37.6–72.5) (p = 0.42) (Figures 2 and 3). SAVE adjusted survival at discharge in patients with ECPELLA versus SAVE predicted survival (reference). SAVE adjusted survival at discharge: Control versus SAVE predicted survival (reference). SAVE adjusted survival at discharge in patients with ECPELLA versus Control.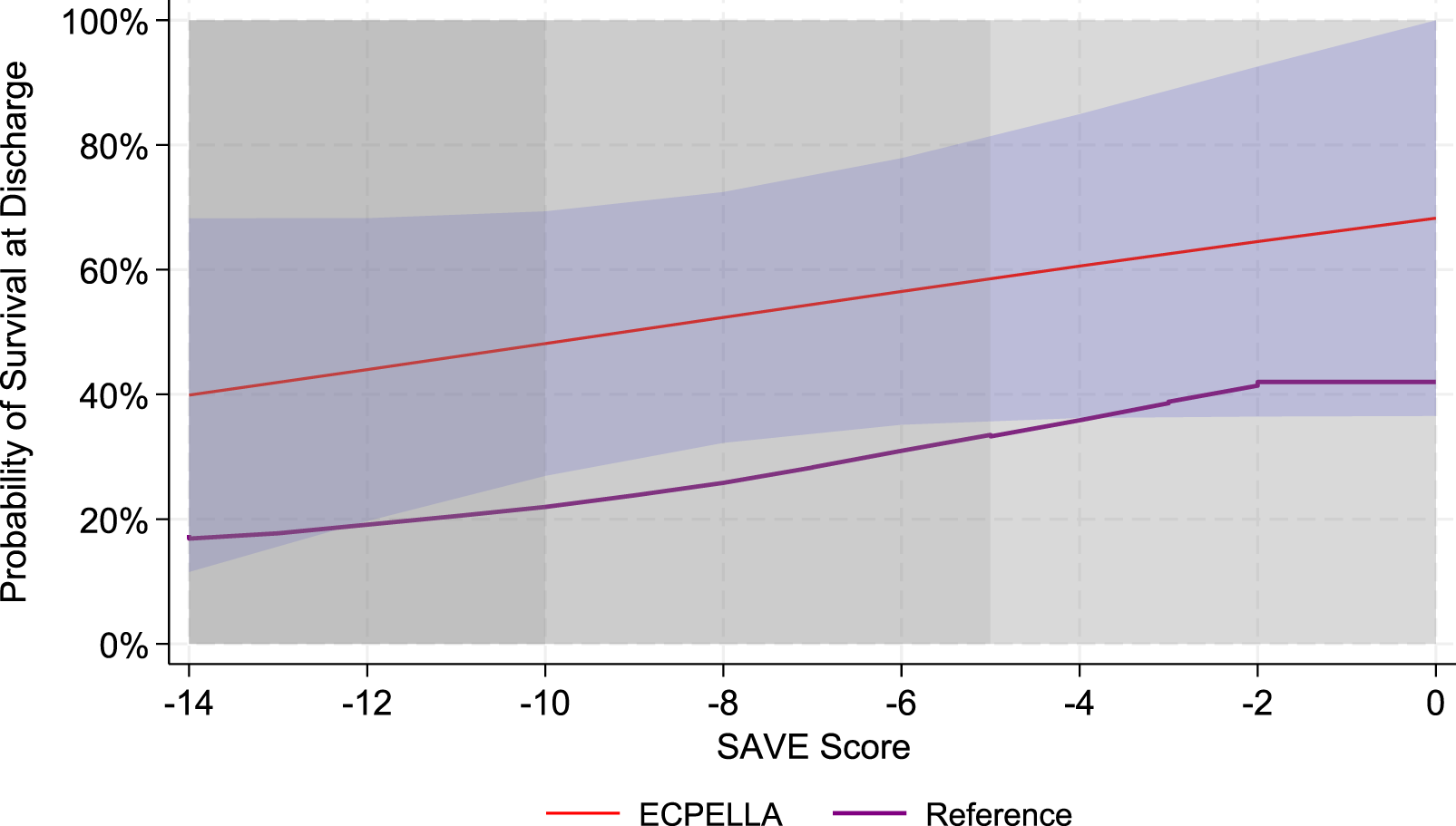
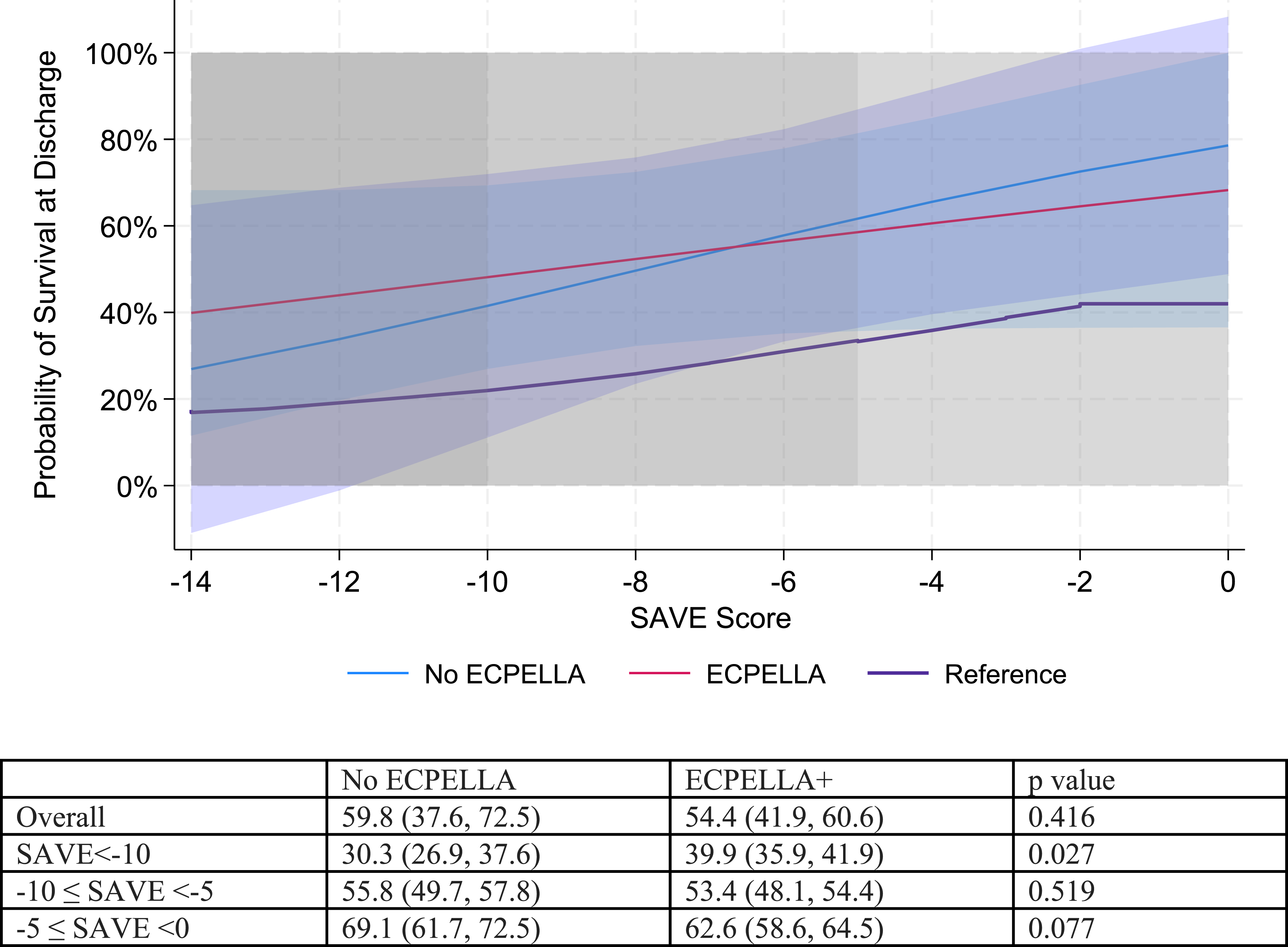
We also compared the survival of ECPELLA + patients with that of control patients across different SAVE score clusters to explore the possible differential impact of LV venting on patients with varying clinical severity grades, as graded by the SAVE score (Figure 3). Interestingly, we observed a significant difference in survival between the ECPELLA + group (39.9%, 95% CI 35.9–41.9) and the control group (30.3%, 95% CI 26.9–37.6) (p = 0.027) among patients with SAVE scores between −14 and −10. No significant difference was seen in the −10 to −5 cluster, whereas patients with SAVE scores greater than −5 (ECPELLA +: 62.6%, 95% CI 58.6–64.5; control: 69.1%, 95% CI 61.7–72.5; p = 0.077) exhibited a non-statistically significant trend towards worse outcomes.
Discussion
This study aimed to clarify the role of LV venting and identify patients who may benefit from full LV unloading after V-A ECMO is initiated for cardiogenic shock. This observational design evaluates a sequential-weaning approach in which early LV venting with an Impella 5.5 provides full unloading, followed by V-A ECMO weaning once metabolic clearance occurs. While limited by a small sample size, our preliminary findings signal that selective use of Impella 5.5 in selected patients on V-A ECMO may improve support and weaning outcomes in cardiogenic shock.
This study and its findings aim to address a growing disconnect between evidence and practice in ECMO and cardiogenic shock management, 15 where the decision to escalate to LV venting frequently relies on center-specific experience rather than objective, patient-level criteria. This pilot investigated whether integrating the overall patient risk profile (SAVE score) with real-time hemodynamic status (PA diastolic pressure) could inform an individualized MCS escalation strategy. Although survival to discharge did not differ significantly between groups, subgroup analyses revealed that patients with higher PA diastolic pressures and SAVE scores below −10 demonstrated significantly greater mortality, suggesting that these combined parameters may identify a hemodynamic phenotype in which LV venting confers benefit.
Patient selection remains critical to the success of MCS. Most patients in this study were enrolled after cardiac arrest. While prompt V-A ECMO deployment can reverse metabolic derangements resulting from cardiogenic shock, it cannot prevent further anoxic brain injury; thus, proper selection criteria are imperative to avoid futile interventions. The enrollment criteria developed during the initial study phase balanced the inclusion of appropriate candidates, including patients with cardiac arrest, while avoiding those with irreversible injury. Additionally, concomitant Swan-Ganz placement at V-A ECMO initiation enabled continuous hemodynamic monitoring and timely device escalation before refractory hypoxia or lung injury developed due to increased afterload, depressed myocardial function, or escalating pressor and inotrope use. While the non-randomized protocol design and well-established V-A ECMO practice in our center may have pre-emptively influenced patient selection, patients with higher mean pulmonary pressure were preferentially assigned to the ECPELLA + group, as initially designed in the current protocol.
The median time from V-A ECMO implantation to Impella placement was 2.28 days. This delay reflected rising pulmonary pressures after V-A ECMO initiation and logistical challenges due to transferring patients on V-A ECMO from outside hospitals. Generally, once patients arrived at our center, Impella 5.5 placement or upgrade occurred within 12 h if their PA diastolic pressure remained consistently above 20 mm Hg. Importantly, although not statistically significant, we observed 11 upgrades from Impella CP to Impella 5.5 (11/43, 25%) due to hemolysis or limited LV unloading, defined as persistent PA diastolic greater than 20 mm Hg.
Although none of the patients in the control group required transition to surgical LVAD or heart transplantation, four ECPELLA + patients were successfully bridged to LVAD. While not statistically significant—likely due to a small sample size—this may explain the longer length of stay in the ECPELLA + group. Nonetheless, the high SAVE-adjusted survival seen in the ECPELLA + group may reflect the ability to fast-track patients from temporary to surgical LVAD while using Impella 5.5 for pre-habilitation 14 during recovery from V-A ECMO.
Several limitations warrant consideration. First, although SAVE score adjustment was performed, this approach does not fully account for time-dependent confounding or treatment indication bias. The small sample size precludes more robust analytical methods such as propensity score matching or marginal structural models, and the non-randomized allocation strategy based on PA diastolic pressure inherently introduces selection bias that cannot be entirely mitigated in an exploratory study of this size. Second, complication rates were low in both the control and ECPELLA + groups; however, the longer duration of ECMO support observed in the ECPELLA + group may bias complication comparisons, and the limited sample size precludes meaningful adjustment for duration of support.
Finally, despite the limited size of the TWEET-1 cohort, the protocol yielded SAVE score-adjusted observed outcomes that significantly outperformed the SAVE-predicted outcome across a wide range of risk profiles (SAVE −14 to 0). Notably, the granular nature of the dataset also suggests a preferential role for ECPELLA + in patients with more compromised clinical conditions (SAVE −14 to −10), who may be candidates for upfront Impella 5.5 deployment. Given its widespread adoption and ELSO endorsement, the SAVE score provides a practical and validated framework for extending these TWEET-1 findings into larger, prospective, multicenter trials. While these results remain hypothesis-generating, the integration of SAVE score and PA diastolic pressure—both well-established parameters within the ECMO community—identified signals that may inform the design of adequately powered randomized trials to establish definitive cutoff values for MCS escalation decisions.
Conclusions
In this limited, prospective, single-center study, a combination of specific patient selection criteria, uniform, continuous hemodynamic monitoring, and hemodynamic-guided LV unloading with the Impella 5.5 outperformed SAVE-predicted survival in patients on V-A ECMO across a wide range of SAVE scores.
Limitations
Given this study’s single-center, exploratory design, conclusions drawn from this relatively small sample size should be confirmed in larger multicenter trials.
We acknowledge that SAVE score adjustment does not fully account for time-dependent confounding or treatment indication bias, and that the small sample size precludes more robust methods such as propensity score matching or marginal structural models.
Complication rates were low in both the control and ECPELLA + groups, and the limited sample size precludes meaningful adjustment for duration of support.
Outcomes presented here are also subject to the initial triage process for offering V-A ECMO to individual patients. This process was performed by an experienced multidisciplinary team at an ELSO Platinum-level center; therefore, outcomes may differ at other centers.
Footnotes
Acknowledgements
The authors would like to thank all clinical personnel of the Heart & Vascular Institute at the Memorial Hermann Texas Medical Center Hospital in Houston for their relentless and devoted assistance in caring for these critically ill patients. The authors also acknowledge Jennifer Peterson, PhD, ELS, and Jessica Moody, PhD, ELS, for their editorial assistance.
Ethical considerations
The UTHealth Houston Institutional Research Board has reviewed and approved the study protocol (HSC-MS-21-0286).
Author contributions
AN, ST, SN, HD, IS, JX, MJ, JP, MP, JW, IG, BK. AN, ST, SN, HD, JW, LJ, KK —Performed the research. AN, JW—Formal Analysis. AN, ST, SN, HD, IS, JX, JP, MP, IG, BK —Investigation. AN,ST, JW—Data Curation. AN,JW, SN, BK—Wrote the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.N. is supported by the National Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI) grant 1R01HL163549-01A1. S.N and A.N. received research grants from Abiomed.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IAS has research-related financial interests in Abiomed.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to patients’ confidentiality but are available from the corresponding author on request.