
Abstract
Objectives: The nutcracker syndrome (NS) may lead to insufficient perirenal collaterals as well as incompetence of the left ovarian vein with consecutive ovarian vein insufficiency.
Methods: A female patient with NS and severe genital varicosis was treated with dilation of the renal vein and coiling of a left perirenal collateral vein feeding an insufficient left ovarian vein (LOV) with pelvic vein varicosity.
Results: In re-evaluation 18 month later with left renal vein (LRV) and LOV phlebography, a widely patent LRV was found. The embolized LRV to LOV collateral was occluded. However, left hypogastric phlebography showed incompetent branches of the left hypogastric vein feeding the genital varicose veins. These were successfully embolized with coils and the genital varicosity decreased on follow-up.
Conclusions: In our patient a combined therapeutic approach with balloon dilation of the NS and embolization of the genital varicose veins by left hypogastric vein coil was performed.
Keywords
Introduction
In nutcracker syndrome (NS), the impingement of the left renal vein (LRV) between the superior mesenteric artery (SMA) and the abdominal aorta (AA) can lead to an inappropriate drainage of the left renal vein (LRV).1,2,3 The consecutive LRV hypertension may cause left flank pain and haematuria, in some cases pelviureteral varices can occur. Varicoceles maybe seen in male patients. In women the clinical presentation is known as ‘pelvic congestion syndrome’, characterized by symptoms of dysmenorrhoea, dyspareunia, post-coital ache, lower abdominal pain, dysuria and emotional disturbances due to renal-to-left ovarian vein (LOV) reflux leading to LOV insufficiency (LOVI) with pelvic, vulvar, gluteal or thigh varices.4,3
Vulvar varices and perivulvar veins are common though often unrecognized and pelvic pain is a common complaint, sometimes without an obvious cause. In some cases pelvic pain is clearly associated with venous pathology. The NS may lead to insufficient perirenal collaterals as well as incompetence of the left OV with consecutive LOVI. To establish the diagnosis, the communication from the atypical varicose veins in the legs to the OVs must be shown and incompetence of one or both OVs must be demonstrated. Treatment requires elimination of the retrograde flow in the OVs. This can be by either surgical ligation and removal or obliteration with coils and sclerosant. Having removed the cause and relieved the pelvic symptoms, the leg veins can then be successfully treated. 5
Our patient was suffering from genital varicosity with a NS and an incompetent perirenal collateral vein (CV) supplying an insufficient and distally dilated LOV. In addition, an incompetent left hypogastric vein branch feeding the prominent vulvar varices was found. We present this unusual case of NS and genital varicosity to demonstrate a combined therapeutic approach with balloon dilation of the NS to reduce venous hypertension in the RV and resolve the perirenal to LOV reflux on the one hand and finally to treat the genital varicose veins by coil embolization of peripheral left hypogastric vein branches on the other.
Case report
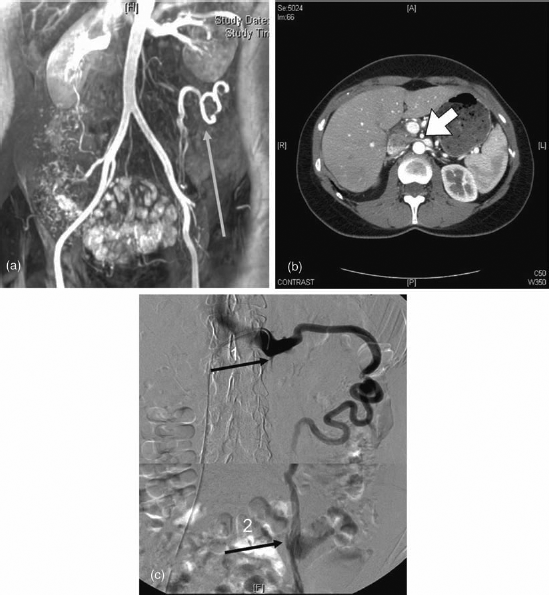
A 46-year-old woman complained of severe and symptomatic vulvar varicosis especially after prolonged standing, in warm environment she suffered from heaviness and swelling of her legs and protruding varicose veins in the genital region. After physical exercise she noted transient haematuria. On physical examination there were prominent genital varicose veins, particularly on the left side of the labium majus and clitoris (Figure 1). Duplex ultrasound of the legs showed a normal deep and superficial venous system. Magnetic resonance venography showed a hypoplastic origin of the LOV and dilated and tortuous perirenal collateral of 7 mm in diameter connecting to the mid LOV (Figure 2a). The distal part of the LOV was found to be markedly dilated with backflow towards the left varicose pelvic veins. Computed tomography clearly disclosed a compression of the LRV between the SMA and the AA as well as a praestenotic dilation of the renal vein representing a NS (Figure 2b). Thus the severe vulvar varicosis was thought to be due to the abnormal backflow from the perirenal to LOV secondary to LRV caused by the NS. The laboratory tests including platelet count, haemoglobin and creatinine were within normal limits.
A photo of left vulva and clitoris with oedema and large varicose veins (a) Magnetic resonance imaging angiography with early contrast enhancement of the left ovarian vein collateral (dart) and (b) computer tomography showing the impingement of the left renal vein between the superior mesenteric artery and the abdominal aorta (dart, nutcracker syndrome) (c) In the phlebography low attenuation of the renal vein is shown (dart 1 sufficient ostium) with filling of the renal vein but reflux of the collateral ovarian vein till the connection with the mid left ovarian vein (dart 2)
Therapeutic concept
Based on the above hypothesis we planned a threefold therapeutic concept: (1) to lower the left renal vein pressure and improving blood flow towards the inferior vena cava (IVC) by balloon dilation of the stenosed LRV. (2) Treatment of the pelvic and genital varicosity by embolization of the perirenal to LOV collateral. (3) We planned to additionally obliterate the genital varicous veins by foam sclerotherapy.
To verify the impeded venous outflow of the LRV across the stenosis to the IVC and effectiveness of balloon dilation pressure gradients before and after the procedure were measured.
Therapeutic methods
Under sterile conditions and local anaesthesia the right femoral vein was punctured, a F7 curved guiding catheter with side port (Cordis Vista britetip Introducing Guide) was advanced to the ostium of the LRV. Using a 0035′ Terumo curved gude wire (Terumo Corporation Tokyo, Japan) a F4 renal Soft Vu Renal catheter (Angiographic Catheter Angio-dynamics, Queensbury NY, USA) was placed into the LRV. Phlebography with ultravist 300 (Bayer, Zürich, Switzerland) revealed the ostium of a competent proximal LOV and marked reflux into a collateral perirenal vein connecting to a mid-left OV, filling dilated pelvic veins (Figure 2c). Via the renal catheter we then measured pressures in the LRV (8 mmHg) and the pressure of the IVC was taken by means of the 7F guiding catheter (4 mmHg). Since the gradient of 4 mmHg was thought to be significant
6
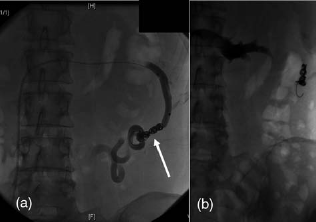
the renal catheter was exchanged for a 6 mm/40 mm balloon catheter (Admirale Xtreme PTA Balloon Catheter, Invatec S.p.A, Roncadelle, Italy) and the stenosis close to the ostium of the LRV was dilated. The neck of the balloon during the inflation showed a definite stenosis at the ostium of the left renal vein which was completely opened at 6 bar balloon pressure (Figures 3a and b). Control pressure measurements of the LRV via the lumen of the balloon catheter and the 7F guiding catheter showed complete resolution of the gradient. Even after temporary occlusion of the CV with a balloon catheter (Pacific Xtreme PTA Balloon Catheter Invatec) guided over a 0018′ guide wire (Pointer Nitinol Guidewire Angiotech PBN Medicals, Stenlose, Denmark) repeated measurement of the LRV and ICV in retraction technic trough the 7F guiding catheter showed again no significant gradient (2 mmHg). The definitive coiling with 5 Tru Fill Pushable Coils 7 mm diameter (Codeman and Shurtleff Inc., Johnson & Johnson, MA, USA) showed a sufficient occlusion (Figures 4a and b).
(a) In the phlebography the neck of the balloon shows the stenosis of the renal vein followed by (b) dilation of the stenosis with the balloon (a) During the phlebography, after temporary occlusion of the left ovarian vein collateral with a balloon, repeated measures of the left renal vein and inferior vena cava pressure gradient were performed (b) followed by occlusion of the left ovarian vein collateral with coils (dart)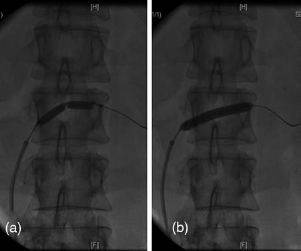
Follow up
On duplex sonography six and 12 months after the intervention renal vein flow was normal. To accelerate the regression of the genital varicosis after occlusion of the supposed feeding vein three sessions of percutaneous foam sclerosing therapy of the labial varices were performed (polidocanol 1%, 5 mL). The size of the genital varicose veins moderately decreased with the patient having less pain. Because of the insufficient regression of the genital varicosis on follow up 18 months after the intervention a control phlebography of the RV and occluded perirenal to LOV collateral was performed via right femoral vein approach using again a 7F curved guiding catheter (Cordis Vista britetip Introducing Guide Johnson & Johnson, Waterloo, Belgium) and a selective 5F cobra catheter (COOK, Bjaeverskov, Denmark) the renal vein viewed in several projections showed a widely patent lumen and no recurrence of the stenosis (only fluoroscopy without documentation). In addition the embolized renal to LOV collateral was found to be completely occluded on valsava manoeuvre. To investigate the status of the LOV distally to the embolized collateral the ostium of the LOV was catheterized with a micro catheter (Progreat Micro catheter system 2,7F Terumo Corporation Tokyo, Japan) which was advanced distally of the former connection of the embolized perirenal collateral. Phlebography showed only a mildly dilated distal LOV with moderate varicosity of pelvic veins, but no reflux into any prepubical or genital varices. (Figure 5a). Therefore a different source of the genital varicosis had to be searched for. Right OV phlebography did not show any abnormal reflux and a vein of normal calibre. However, on left pelvic phlebography using a 5F Cobra catheter (COOK, Bjaeverskov, Denmark) in crossover technique two markedly dilated branches of the left hypogastric vein showing massive reflux to the lower pelvic region with a filling of varicose veins leading to the genital respectively vulvar area were demonstrated (Figure 5b).
(a) Embolized left ovarian vein collateral and mildly dilated distal LOV with moderately dilated pelvic veins are shown (b) The collateral branches of the hypogastric vein that show reflux toward vulvar veins, (c) coiled hypogastric branches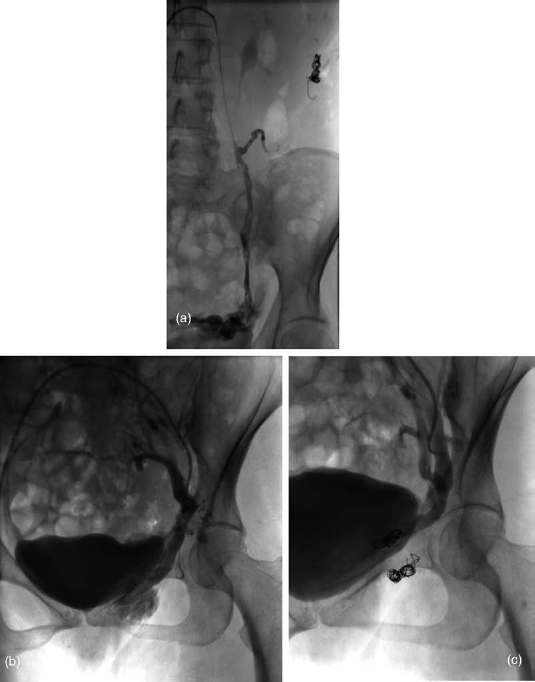
Using a coaxial technique each of the two branches was accessed with micro catheter (Progreat Micro catheter system 2,7F Terumo Corporation) and were embolized with each five 10 mm True Fill Coils (Codeman and Shurtleff Inc., Johnson and Johnson, MA, USA) Occlusion with cessation of reflux was achieved immediately on control phlebography (Figure 5c). Twelve months following this second embolization procedure the genital varices have markedly decreased with complete relief of the patients symptoms.
Discussion
Although often asymptomatic, the NS may be associated with symptoms of pelvic venous congestion or peripheral and pelviureteral varices through massive gonadal reflux. Since de Scheper's 7 publication in 1972 progress in the therapy of this syndrome has been made.
The treatment of NS is controversial. Many treatment options have been applied (nephrectomy, medial nephropexy, renal vein bypass, transposition of the LRV, autotransplantation, endovascular stents). 4 The use of balloon dilation and stents with regard to arterial renovascular disease is common in venous disease.1,2 In our patient we postulated non-elastic adhesions creating the stenosis of the LRV. Similar adhesions can be found in May-Thurner syndrome due to chronic pulsatile mechanic irritation of the impinged vein.8,9 Thus, the arterial pulsation (SMA and AA) might cause chronic trauma to the LRV, resulting in accumulation of collagen and elastin and formation of intimal fibrosis and adhesions. After angioplasty by balloon dilation a probatory occlusion of the perirenal collateral with a balloon was performed to investigate the renocaval gradient. In case of an embolization of the OV (perirenal collateral in this case) the renocaval gradient should not rise and should be still sufficient to sustain the venous flow in the RV. This procedure was important to assure the renal flow with no danger of a possible renal venous stasis after the embolization. The renocaval gradient was 2 mmHg. According to Nishimura, 6 regarding a 3 mmHg pressure gradient as cut-off value indicating renal hypertension, our gradient of 2 mmHg can be considered as normal. In this consequence there is a normal unimpeded flow of the LRV to the IVC. There was no reason to implant stents in the LRV ostium, consequently avoiding possible complications. As a matter of fact the blood flow in the LRV was high enough to support the formation of a sufficient LRV flow. Duplex ultrasound control six and 12 months after intervention showed a normal flow in the LRV. Because the genital varicosis did not regress adequately the patient was again evaluated 18 months later with LRV and LOV phlebography. No recurrence of the stenosis but a widely patent LRV was found. In addition, the embolized LRV to LOV collateral was found to be occluded. On selective catheterization of the distal LOV no connection to the genital varicosity could be demonstrated. However, left hypogastric phlebography showed two incompetent branches of the left hypogastric vein feeding the genital variose veins. These were successfully embolized with coils and the genital varicosity decreased with resolution of the patient's symptoms on follow up.
In our patient a dual therapeutic approach with (1) Balloon dilation of the LRV to reduce venous hypertension in the RV and resolve the perirenal to LOV reflux and (2) Treatment of the genital varicose veins by left hypogastric vein coil embolization was chosen. In the literature endovascular stenting is described as an effective procedure to treat the NS with low incidence of peri- and postoperative complications such as stent migration into the right atrium, stent protrusion into the IVC and stent migration into the hilar left renal vein. 10 The treatment of NS is controversial. Conservative treatment has been proposed for cases with mild haematuria, while endovascular or surgical 4 treatment is indicated when clinical symptoms arise as massive haematuria and pain. Our patient received only a dilation of the LRV without stenting. Avoiding the stent the intention was to minimize the risks of implantation of a stent, as the risk of perforation, migration, recurrent obstruction over time or bleeding.
Further experience and long-term studies have to confirm successful improvement of the LRV blood flow in NS in well selected cases by only performing dilation of the LRV and occlusion of the OV without placing a stent into the LRV.
Footnotes
Acknowledgements
We are thankful to all the colleagues who participated in developing the manuscript. There are no conflicts of interest.