
Abstract
Background:
Cost-effectiveness analysis (CEA) is often misperceived to be a cost-cutting exercise. The intention of CEA is not to identify and implement cheap technologies, but rather those which offer maximum health gain, subject to available funds. Such analysis is crucial for decision making in health care, as tight budget constraints mean spending in one area of healthcare displaces spending elsewhere. Therefore in order to achieve the greatest health gain for the overall population, treatments must be selected which provide the greatest health gain within the available funds.
Summary:
The relevance of CEA in health care systems is explained, using varicose vein treatment in the UK NHS as an example. Treatment for varicose veins is often not commissioned to at a local level, most likely because it is misperceived to be a cosmetic problem. However, this view does not take into account the impact of quality of life. CEA balances costs against a quantitative measure of health related quality of life, and could therefore be used to determine whether it is cost-effective to provide varicose vein treatment. The current literature on the cost-effectiveness of varicose vein treatment is reviewed, and an overview of cost-effectiveness principles is provided. Concepts such as economic modelling, incremental cost-effectiveness ratios (ICERs), net monetary benefit (NMB) and sensitivity analysis are explained, using examples relevant to varicose veins where appropriate.
Conclusion:
This article explains how, far from cutting costs and sacrificing patient health, CEA provides a useful tool to maximise the health of the population in the face of ever tightening budget constraints. CEA could be used to compare the cost-effectiveness of the various treatment options for varicose veins, and efficiencies realised.
Keywords
Introduction
Contrary to common belief, health economics is not about saving money. Health economics, or more specifically cost-effectiveness analysis (CEA), does not advocate implementation of the cheapest treatments, but rather those that offer maximum benefit for the available funding. Even the cheapest of treatments cannot offer good value for money if it offers little health gain. The overall objective of CEA is to identify the optimal allocation of resources within health care – the allocation of resource which maximizes population health, subject to prevailing budget constraints. Optimal allocation of resources is essential because, when faced with a budget constraint, spending in one area of health care displaces spending elsewhere. In other words, provision of treatment to one patient has an opportunity cost: treatment for another patient must be foregone, and their health sacrificed. Therefore it is vital that the most cost-effective treatments are identified, through CEA, as this allows us to achieve the highest level of population health possible within our constraints. CEA is therefore used to inform decision-making in health care, to assess whether a new technology represents sufficient value for money to be implemented. 1
This article will explain the relevance of CEA in health-care systems, using varicose vein treatment in the UK National Health Service (NHS) as an example. An overview of cost-effectiveness principles is provided, with a view to demonstrate how decision analysis is conducted in the context of health care. Further information on the different types of economic evaluation can be found elsewhere. 1
The NHS and varicose veins
In order to maximize population health subject to financial constraints, health-care services must only provide treatments which are cost-effective. In the UK, the National Institute for Health and Clinical Excellence (NICE) is charged with producing evidence-based guidance for the NHS. NICE's clinical guidelines, public health programme and technology appraisals all include economic assessments, and should only recommend cost-effective practice.
At present, no published guidance is available in which the cost-effectiveness of the different treatment options for varicose veins is compared (although a guideline is in development for this disease area at the moment 2 ). In the absence of such guidance, interventional treatments for varicose veins are often not commissioned at a local level, most likely because this condition is misperceived to be a cosmetic problem. However, this view does not take into account the impact of this condition on quality of life, and it overlooks the implications of the disease worsening. A CEA of varicose vein treatments could determine whether or not it is cost-effective to intervene in these patients, and identify specifically which of the available treatments represents the best value for NHS money.
At present there are only two3,4 published studies which use decision analysis to assess the cost-effectiveness of different treatments for varicose veins from a UK perspective. Michaels et al. 3 compared surgery, liquid sclerotherapy and conservative care in various groups with differing stages of disease, and found surgery to be the most cost-effective option. However as endovenous techniques (specifically endothermal treatments and foam sclerotherapy) have increased in popularity since the time of publication, this analysis is no longer complete. The second evaluation, carried out by Gohel et al., 4 found day case surgery, endothermal laser ablation (local anaesthetic) and radiofrequency ablation (local anaesthetic) to be cost-effective, in comparison to foam sclerotherapy, endothermal laser ablation (general anaesthetic), radiofrequency ablation (general anaesthetic), inpatient surgery and conservative care. However, the analysis was subject to several limitations. In addition to these two published analyses, there is also an ongoing Health Technology Assessment (HTA) to investigate the cost-effectiveness of minimally invasive techniques; 5 the HTA project is still being revised, and no further comment can be made here. Finally, as mentioned previously, a clinical guideline for treatment of varicose veins is currently in development. The guideline will be published by NICE later in 2013. 2
None of the aforementioned CEAs comprehensively answer the question of who to treat and when. To answer such a question would require data on natural progression of the disease and the effectiveness of each treatment at each level of severity of varicose veins, and such data may not yet exist. Recent data emerging from the Bonn Vein study and Edinburgh Vein study (for example, Refs.6,7) could prove useful in determining long-term aggregate outcomes.
Health economic principles
All of the aforementioned analyses involve decision modelling, where a mathematical model is built to evaluate the costs and outcomes which are expected to arise as a result of a particular intervention or treatment strategy. Decision models replicate the pathway a patient would be expected to take through a particular disease, including natural progression of the disease and the effect of any intervention, based on clinical trial data. For example, a varicose veins model would look at the expected health gain from treatment, taking into account possible adverse events associated with treatment and the possibility of recurrence further down the line. If long-term natural progression data were available, the model could also approximate the health gain of an individual who was not treated, in comparison to a patient who was. As with many types of analysis, there are drawbacks and limitations to modelling; assumptions and simplifications are necessary and define the boundaries of the model. It is not possible to take into account every single clinical eventuality in the model; decision analysis requires a balance between clinical accuracy and computational burden. Approaches to modelling and the associated limitations are discussed elsewhere. 8
NICE requires all such CEAs to be conducted in accordance with its ‘reference case’. 9 Among other things, this means all decision analyses must be conducted from the perspective of the NHS and personal social services (meaning only direct costs faced by these institutions should be included) and the analysis is typically conducted over a lifetime horizon or at least a long enough horizon such that all important effects on costs and health are included. For the varicose veins example, costs from an NHS and PSS perspective would include the cost of treatment (including staff costs, scans, instruments, disposables and overheads associated with treatment rooms, etc.), specialist appointments and treatment of recurrent varicose veins. Costs incurred by the patient and productivity costs associated with the patient absenting from work would be excluded from the analysis, as these are not costs to the NHS.
For this type of analysis, health gain must be quantified. The health outcome recommended by the NICE reference case is the quality-adjusted life-year (QALY). A QALY is a measure of a person's length of life, weighted by a valuation of their health related quality of life. The weight is called a utility value, and is a measurement of the preference for a particular health state. Utility scores are usually measured between 0 (death) and 1 (perfect health). Scores lower than 0, representing a quality of life considered to be worse than death, are possible but would be unlikely to arise when considering varicose veins. Equivalently QALYs can be represented graphically, as demonstrated in Figure 1. Figure 1 shows the course of an individual's utility level over time in two scenarios: no treatment and treatment. The number of QALYs in each scenario is equal to the area under each curve, with the difference (the lighter shaded region) representing QALY gain.
Graphical representation of the quality-adjusted life-year (QALY)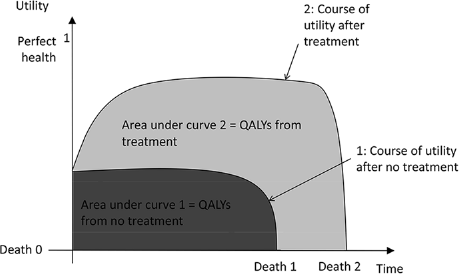
There are several methods of measuring utility, but the preferred method for NICE CEAs is the EQ–5D questionnaire. The NHS patient reported outcome measures 10 (PROMs) data include EQ–5D scores for patients undergoing varicose vein treatment; the preoperative utility score is 0.746, with an increase in utility of 0.093 post-treatment. If this improvement was sustained over 10 years, this would represent a gain of 0.93 QALYs per patient associated with intervention.
Clinical data must be incorporated in to the analysis. The clinical data are used to inform the probabilities of various clinical events taking place, for example the possibility of successful varicose vein treatment, or the chance of experiencing recurrent reflux after treatment. These data are usually taken from a combination of randomized trials and observational studies; often relative treatment effects obtained from randomized trials are applied to baseline probabilities obtained from observational studies. The model compiles the inputs (the unit costs, utility scores and clinical data) and calculates the expected total cost of each strategy, as well as the expected health gain (QALYs).
Having built a model to calculate the expected costs and health gain associated with a treatment, we need to decide whether the treatment represents good value for money. Assessing value for money is simple if, for example, treatment A is both more effective and less costly than treatment B, but often the more expensive treatment is also the more effective one, and a decision rule is needed. There are two main methods commonly used to guide decision-making: incremental cost-effectiveness ratios (ICERs) and net health benefit (NHB). Both methods are outlined below.
An ICER is the ratio of additional cost to additional health benefit. Consider two interventions: X and Y Let C represent mean cost, and Q mean QALYs. Suppose the incremental cost between X any Y is C x –CY = £2000, and the incremental benefit is Q x – QY = 0.2. The ICER will be ICER XY = £2000/0.2 = £10,000 per QALY for X compared with Y.
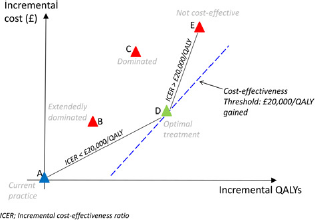
An intervention which is dominated is more costly and less effective than a competing alternative. Dominance is demonstrated graphically in Figures 2 and 3; the North West quadrant of Figure 2 illustrates dominance when only considering two interventions, and option C in Figure 3 is an example of a dominated intervention when considering multiple competing alternatives. Dominated options would not normally be implemented, and must be removed when calculating ICERs in order to allow calculation in comparison to the next best alternative. If dominated (or extendedly dominated) options are not removed, the ICERs will be underestimated. An option is said to be ‘extendedly dominated’ if a mixed strategy (a strategy of a combination of two competing interventions) would provide the same (or greater) level of health benefit at a lower cost. In Figure 3, a mixed strategy of interventions A and D could sit anywhere along the line that joins these points on the graph. There are points on the line which dominate option B, providing greater health benefit at a lower cost, thus B is extendedly dominated. The need to remove all dominated and extendedly dominated options represents a drawback of ICERs, as when considering a large number of alternatives identification of dominated and extendedly dominated strategies can be complex.
Rules when comparing only 2 options. Reproduced with permissions from © 2013 The American College of Physicians. Rules when comparing multiple options. Reproduced with permissions from © 2013 The American College of Physicians.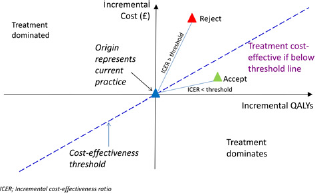
ICERs are more useful than average ratios (total costs divided by total QALYs), yet an ICER is still merely a summary of cost-effectiveness; it does not provide enough information to inform a policy decision. The decision of whether to choose X or Y depends on whether we deem the extra £10,000 for an additional QALY to be good value for money. Answers to this question of what is/is not cost-effective can only be determined relative to a cost-effectiveness threshold.
The cost-effectiveness threshold is the maximum amount of money which can be spent per QALY in order for an intervention to be cost-effective. In theory the threshold is dependent on the NHS budget. Assuming the threshold is set correctly, the budget would run out at the point that it has provided every intervention below the threshold, without investing in any interventions which lie above the threshold. Currently in the UK, NICE asserts that there is no absolute threshold level. Guidance states that interventions with a cost per QALY less than £20,000 are likely to be implemented, whereas an intervention with a cost between £20,000 and £30,000 per QALY can be justified only by making reference to additional factors such as level of innovation. 11 In the case of our example, a cost-effectiveness threshold of £20,000 per QALY gained would indicate that we do deem the extra £10,000 per QALY gained to be good value for money: option X is the cost-effective strategy. If we were comparing multiple ICERs, we would select the intervention with the highest ICER under the threshold, as this would offer the greatest health gain while remaining below the maximum amount which can be spent for an additional QALY. Figures 2 and 3 provide a graphical summary of this decision rule.
Interventions with ICERs above the cost-effectiveness threshold should not be implemented, as health-care budget constraints mean that the opportunity cost of these interventions is greater than the benefit they produce. For example, if a treatment with an ICER of £40,000 (double the cost-effectiveness threshold level in the UK) was implemented, then for every 10 QALYs gained, 20 would be lost from services displaced by this intervention. Clearly the use of decision rules is vital in CEA, and this example shows why the cost-effectiveness threshold must be adhered to.
NHB and net monetary benefit (NMB) are alternative representations of the same decision rule as with the ICER approach, and have been employed to overcome the problems associated with ICERs.
8
The net benefit approach provides an explicit valuation of the outcome of an intervention, by using the threshold value to convert between health outcome and monetary value. Net benefit is the benefit of the intervention, less the opportunity cost of the resource used:

k represents the threshold value, and is used here to translate costs into QALYs, or health benefits into monetary terms. Option X is chosen if kQx – Cx > kQY – CY. The NMB and NHB of options X, Y, Z are calculated in Table 1.
Calculation of net benefit

QALY, quality-adjusted life-year; NMB, net monetary benefit; NHB, net health benefit
Option X yields the highest net benefit and is therefore the most cost-effective (note this is the same conclusion as when using the ICER application of the decision rule). An advantage of this approach is that it does not require the elimination of dominated or extendedly dominated strategies but it still gives the same optimal strategy.
However, the conclusions drawn here do not take uncertainty into account. As mentioned previously, economic models are built upon assumptions, and uncertainty often clouds parameter estimates. For example, it is unlikely that we will ever be sure precisely what the reflux recurrence rate is postsurgery Sensitivity analyses are therefore often undertaken to test the robustness of a model. This involves varying key parameters (for example, the probability of experiencing recurrent reflux), and relaxing key assumptions, in order to investigate the impact of these changes on the model results. Probabilistic sensitivity analysis is particularly useful, in which inputs (the costs, probabilities and utilities) are randomly drawn from carefully selected distributions, and mean results taken over a large number (for example 10,000) of model simulations. In the context of varicose veins, substantial uncertainty surrounds the cost of the various interventions, thus cost inputs would be key variables to undergo sensitivity analysis in a CEA.
Results of CEA ought to be interpreted carefully, and it should be noted that results based on expected outcomes are not always suitable to generalize to all individuals. For example, in the context of varicose vein treatment, there exists a large proportion of individuals for whom one or more of the available treatments are not suitable; within this population, a CEA of all available treatments may be of limited relevance.
Implications and conclusion
The implication of CEA within health care is a means to identify those treatments which represent good value for money, and ultimately the ability to improve population health. In many publically funded health-care systems, new technologies and drugs have to be proven to be cost-effective before widespread implementation; NICE's technology appraisals are one example of this. For varicose veins, if intervention was proven to be cost-effective, it may no longer be considered efficient to ration treatment. A CEA suitable for such decision-making in the NHS would necessarily be based on the NICE reference case, and include all relevant comparators, including surgery, endovenous techniques and conservative care. ICERs or NMB could then be used to compare the cost-effectiveness of the various treatment options to each other, and cost-effective practice could be implemented. To conclude, far from cutting costs and sacrificing patient health, CEA provides a useful tool to maximize the health of the population in the face of ever tightening budget constraints.
Footnotes
The authors have no conflicts of interest to declare.