
Abstract
Compression therapy is considered to be the most important conservative treatment of venous leg ulcers. Until a few years ago, compression bandages were regarded as first-line therapy of venous leg ulcers. However, to date medical compression stockings are the first choice of treatment. With respect to compression therapy of venous leg ulcers the following statements are widely accepted:
Compression improves the healing of ulcers when compared with no compression; Multicomponent compression systems are more effective than single-component compression systems; High compression is more effective than lower compression; Medical compression stockings are more effective than compression with short stretch bandages.
Healed venous leg ulcers show a high relapse rate without ongoing treatment. The use of medical stockings significantly reduces the amount of recurrent ulcers. Furthermore, the relapse rate of venous leg ulcers can be significantly reduced by a combination of compression therapy and surgery of varicose veins compared with compression therapy alone.
Introduction
Compression therapy is regarded as the basis of therapy in phlebology The efficacy of compression therapy on venous leg ulcers can clearly be defined by explicit established endpoints: healing rate, time to complete healing and – less frequent – the reduction of wound surface within a defined period.
At the stage of healed venous ulcers (C5), the relapse rate or the time to first relapse are generally determined to evaluate treatment efficacy. 1 Less commonly, the improvement of symptoms and signs is used. 2 At lower stages of chronic venous insufficiency (C1–4) the evaluation of treatment efficacy often draws on the investigation of weaker parameters such as pruritus, pain, discomfort or general leg disorders. However, more objective parameters like venous pressure in the ankle region, plethysmographic measurements, sonographic measurements of the vein cross-section or measurements of leg circumferences and leg volume are available. 3
Healed venous ulcer (C5)
Healed venous leg ulcers show a high relapse rate without ongoing treatment. The use of medical stockings significantly reduces the amount of recurrent ulcers. 4 Compression pressures of 25–35 mmHg show significantly lower relapse rates than compression pressures of 18–24 mmHg. However, the compliance of patients with medical stockings is better with lower compression pressures. 5 Furthermore, the relapse rate of venous leg ulcers can be significantly reduced by a combination of compression therapy and surgery of varicose veins compared with compression therapy alone. 6
Active venous ulcer (C6)
Compression therapy is considered to be the most important conservative form for treatment of venous leg ulcers. Up until a few years ago, compression bandages were regarded as first-line therapy of venous leg ulcers. However, to date medical compression stockings (MCSs) are the first choice of treatment. This is based on higher healing rates and reduced time to healing on the one hand, and on a better wearing comfort contributing to patient compliance on the other hand.4,7,8 Improved healing of venous ulcers with MCSs is probably related to their ability to better uphold the aimed compression pressure.
9
However, in clinical practice the measured compression pressure under MCSs also differs from the desired range in 32% of the cases.
10
The efficacy of compression therapy on the healing of venous leg ulcers is substantially better demonstrated in randomized controlled trials than the effect of often cost-intensive local wound therapy with various topical wound dressings. With respect to compression therapy of venous leg ulcers the following statements are widely accepted:4,7
Compression improves the healing of ulcers when compared with no compression; Multicomponent compression systems are more effective than single-component compression systems; High compression is more effective than lower compression; MCS are more effective than compression with short stretch bandages.
Types of compression stockings for venous leg ulcers
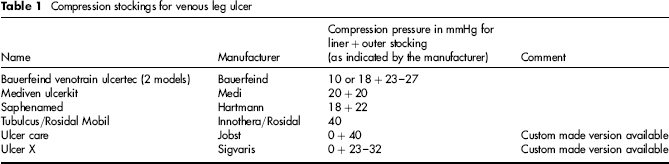
MCSs for venous leg ulcers are usually double-layer compression systems (Table 1). The Rosidal® mobil (Fa. Lohmann & Rauscher, Neuwied, Germany; previous Tubulcus, Fa. Innothera) is the only one-layer system, consisting of a circular compression stocking, which is pulled over a stocking aid ranging up to the knee. All other compression systems for venous leg ulcers consist of a light compression liner stocking and a stronger outer compression stocking. Generally, the light compression liner stocking can easily be pulled over the wound dressing. In addition it helps the outer compression stocking to slide on easier. Both compression stockings together lead to the desired compression pressure, which corresponds to compression ranging from 23 to 40 mmHg (Table 1) for most compression systems. Simultaneously, the double-layer system provides a higher stiffness, which increases the working pressure under mobility. Some outer compression stockings include a zipper to facilitate the handling. Others use a specially developed rhomboid knit (Bauerfeind Veno Train® ulcertec, Bauerfeind, Zeulenroda-Triebes, Germany) to improve transverse-elasticity which makes it easier to put on the outer stocking. There are also outer compression stockings (e.g. Sigvaris ulcer X), which correlate with one of the manufacturer's MCSs with a generally higher stiffness. This leads to an increased working pressure, while the resting pressure corresponds to the compression class. These stockings can usually be adapted to the patient's size and the shape of the legs (custom-made). The ease of application of four different compression systems for venous ulcers was investigated in an experimental study by means of visual analogue scales. 11 The results showed no significant differences between Veno-Train® Ulcertec, SurePress Comfort® and Sigvaris® ulcer x (St. Gallen, Switzerland). However, all three of these were significantly easier to use than Mediven® Ulcer kit (Bayreuth, Germany) (without the intended stocking aid).
Compression stockings for venous leg ulcer
Combination of compression stockings and compression bandages for venous leg ulcers
The healing rate of venous leg ulcers improves with an increased compression pressure. It is possible to achieve this by applying additional compression bandages over the MCSs. This could be demonstrated in a controlled trial: the healing rate of venous leg ulcers under treatment with Tubulcus alone (compression pressure 43.9 mmHg in an upright position) was compared with Tubulcus plus single-layered long stretch bandage (Niva, 68.2 mmHg in an upright position) and to Tubulcus plus double-layered long stretch bandage (87.4 mmHg in an upright position) within a period of 26 weeks. 12 The results between the compression stocking alone and the compression stocking in combination with single- or double-layered long stretch bandages were significantly different. The healing rate under treatment with the compression stocking alone was 25%. It increased up to 67% in combination with the single-layered bandages and up to 74% in combination with the double-layered bandages.
Intermittent pneumatic compression for venous leg ulcers
The impact of intermittent pneumatic compression (IPC) on venous leg ulcers remains unclear. A systematic Cochrane analysis of intermittent pneumatic compression for treating venous leg ulcers 13 included seven randomized controlled trials. Due to the sparse data, the authors could not draw a final conclusion about the efficacy of intermittent pneumatic compression therapy for venous leg ulcers. They referred to a possibly positive effect of intermittent pneumatic compression when compared with no compression and to a better effect of rapid IPC-cycles. Further investigations are needed to determine whether IPC has advantages in combination with conventional compression therapy or whether IPC can be used instead of them.
The following results were demonstrated in clinical trials:
Intermittent pneumatic compression (4 hours/day) in combination with conventional (30–40 mmHg) showed statistically significant differences in favour of additional IPC when compared with the use of the same type of MCS alone within a study period of 12 weeks. However, the ulcer size at baseline differed considerably between the two study groups; No significant differences of the healing rate were found in four trials investigating the application of conventional compression with additional IPC compared with conventional compression alone. The study group of Kumar et al. used not otherwise specified MCS and a not precisely defined four-layer compression system, Schuler et al. and McCulloch et al. applied Unna boots;
13
A study with only 16 included patients on compression with long stretch bandages compared with IPC showed no significant differences within three months;
13
Rapid IPC-cycles with a seven-chamber system achieved higher healing rates and a shorter time to healing compared with slower cycles with the same compression system.
14
Treatment of venous leg ulcers with compression bandages
Up until the end of the 1990s almost only short stretch bandages were used to treat venous leg ulcers in Europe outside UK. For a long time, the variations of bandages were limited to the mode of how to apply the short stretch bandages. Various application modes by Pütter, Sigg, Altenkämper and others were discussed. While long stretch bandages were used in the UK, they were for instance frowned upon in German-speaking countries. MCSs were considered to be inappropriate when eczema or even active venous ulcers were present. These assessments had to be modified considerably because of newer study results.
The type of bandages has changed as well. Bandages consisting solely of short stretch bandages get continually replaced by multiple component bandages, which apparently increase healing rates and reduce the time to healing. 4 Evidently, the amount of layers is not as essential as the optimal combination of the different materials in a so-called compression system. 15 This was demonstrated in an eight-week crossover clinical trial comparing the two-layer multicomponent compression system Coban 2 with the four-layer Profore (padding bandage, a light conformable bandage, compression bandage and a flexible cohesive bandage), which revealed no significantly different healing rates within eight weeks of treatment. 16
Multicomponent compression systems often combine padding, conformable foams, short stretch and long stretch bandages as wells as cohesive materials. Frequently, the materials are interwoven to composites within one bandage, e.g. padding and short stretch bandage. The importance of formerly often used Unna boots has considerably decreased, not least because of the impaired ankle mobility under these boots. With regard to the healing rate and the time to healing they showed no advantage compared with multicomponent compression systems like the two-layered Coban 2. 15
Commonly, compression bandages are only used during the intensive phase of decongestive therapy within a period of 2–4 weeks and then switched to MCSs as early as possible. The pros for MCSs are shorter time to healing, higher healing rates, more reliable compression pressure over the time and improved patient comfort. In contrast to most compression bandages, patients are able to wear regular shoes.
The most important results concerning compression bandaging are:
4
Single-component compression showed lower healing rates and an increased time to healing compared with multicomponent compression; With two-component systems higher healing rates could be achieved after one year when an elastic component was included; With three-component systems higher healing rates were achieved after three months when an elastic component was included; Four-layer compressions systems led to comparable healing rates as Unna boots after six months; Adjustable medical compression systems (Thera-Boot, CircAid) showed no significantly different healing compared with Unna Boots or four-layer compression systems; Two-component compression systems showed better healing rates compared with short stretch bandages.
Evidently, a high working pressure and stiffness are important factors of compression therapy of venous ulcers, since Unna boots often show good results in comparison with other modes of compression. This is supported by the results of a study, comparing the two-layer compression system Coban 2 with the Unna boot (Zincobend Anelastic without tension, cotton bandage, Zincobend with tension, cohesive bandage Fisioplast), which could not detect significant differences in healing rate or time to healing between the two groups within a period of three months. 15
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Footnotes
The authors have no conflicts of interest to declare.