
Abstract
In the current economic climate, the cost-effectiveness of health-care interventions is under great scrutiny. In this article, the evidence for cost-effectiveness of treatments for varicose veins is summarized. The majority of studies evaluating treatments for varicose veins have not assessed health economic outcomes, but have focused on clinical and anatomical measures. The cost-effectiveness of treating varicose veins (compared with conservative management) was demonstrated in the REACTIV trial. Other in-trial economic analyses suggested that endovenous interventions are likely to be cost-effective and a decision tree analysis demonstrated that the greatest cost-effectiveness may be present for procedures performed under local or tumescent anaesthesia in the office or outpatient setting. However, the treatment modality that offers the greatest cost-effectiveness remains unclear. In conclusion, endovenous treatment performed in the outpatient setting under local anaesthesia is likely to be the most cost-effective treatment strategy for varicose veins. Better quality health economic analyses are needed to refine this conclusion.
Introduction
Those involved in the management of patients with venous disorders are fortunate to have a large and growing range of traditional and minimally invasive endovenous treatments at their disposal. In recent years, the use of traditional varicose vein surgery has declined and largely been replaced by minimally invasive interventions such as ultrasound-guided foam sclerotherapy (UGFS), endovenous laser (EVLA) or radiofrequency ablation (RFA). The use of each modality is supported by numerous prospective and randomized studies. 1 However, while a large choice of treatment options may be considered a luxury, this has also resulted in considerable uncertainty and inconsistency in patient management. 2
In the current challenging economic climate, costs and health economic considerations have become key factors in deciding health policy and which treatments will be reimbursed. The identification and implementation of the most cost-effective treatments is desirable in all areas of health care, but of particular relevance in the management of varicose veins, which is considered a low-priority condition and targeted for rationing in many health-care systems. Although most studies of superficial venous interventions have focused on traditional clinical outcome measures, an increasing number of studies of have evaluated cost-effectiveness. In this chapter, important health economic concepts are introduced and the available evidence for the cost-effectiveness of traditional and endovenous interventions is summarized.
What is cost-effectiveness?
General principles
Assessment of cost-effectiveness is an increasingly important consideration when deciding between different treatments and may be defined as
…the comparative analysis of alternative healthcare strategies in terms of both their costs and outcomes. 3
It is a concept that most people are familiar with in daily life. Just as one would not consider purchasing an item without understanding the precise cost and content, the same principle applies for health-care interventions (either specific treatments or systems of care). A major advantage of assessing health economics is that costs and outcomes of health-care interventions can also be compared with other available treatments in an attempt to identify the best value. The viewpoint of the health economic evaluation has a major influence on the results and conclusions and should therefore be explicitly specified. An analysis from the viewpoint of the health-care provider would not consider the financial implications of time off work or patient travel expenses, whereas these are important costs from the perspective of the patient or society. Numerous types of health economic assessment may be performed, including:
Cost minimization study: These studies assume that all the different treatment strategies assessed have the same clinical success. The evaluation is therefore reduced to a simple comparison of costs. This is not generally considered a full health economic evaluation. Cost benefit study: In a cost-benefit analysis, both the costs and outcomes of different treatment options are expressed purely in monetary terms. Results can be expressed as a ratio of the cost of a treatment to the estimated benefit. Cost-effectiveness study: When the outcome of interest is common to all the different treatment pathways to be compared (such as walking distance and life-years gained), then the costs may be expressed as cost per unit outcome (e.g. cost per life-year gained). Cost utility study: A utility refers to a more generic outcome measure after health-care interventions and is graded between 1 (perfect health) and 0 (dead). The outcome is usually expressed as quality-adjusted life-years (QALYs). QALYs measure health as a combination of duration of life- and health-related quality of life and 1 QALY is defined as one year spent in perfect health. The primary outcome from a cost-utility analysis is cost per QALY, or incremental cost-effectiveness ratio. These outcomes allow meaningful comparison of treatment strategies with different health benefits.
Cost-effectiveness and cost-utility analyses are generally considered to be the most relevant to clinicians as they take important outcome measures into account. The use of cost-utility analyses also allows meaningful health economic comparison of different treatments for different conditions against each other and against centrally determined thresholds. In general, health economic analyses can be performed as ‘in-trial’ evaluations (using actual costs and outcomes for a cohort of patients in a clinical trial) or as modelling studies, using decision tree or Markov models to predict likely average costs for a population.
Is the treatment of varicose veins cost-effective?
Summary of available evidence
Many published clinical studies have reported clinical outcomes after superficial venous interventions in recent years. However, few have included any evaluation of cost or cost-effectiveness as part of the analysis plan. Details of the most relevant published studies are summarized below:
Reactiv trial
A landmark HTA-funded study from the UK, the Randomized and Economic Assessment of Conservative and Therapeutic Interventions for Varicose veins (REACTIV) trial started recruitment in 1999 and was published in full in 2006. 4 The trial comprised of a large observational study, but also a trial of 246 patients randomized to conservative management of varicose veins or superficial venous surgery. The research team deserves particular credit, as, unlike the majority of clinical trials in venous disease, evaluating the cost-effectiveness of venous surgery was a central aim of the study. The researchers used a patient level in-trial economic analysis and decision tree economic modeling.
The analysis of patient-level data to two years clearly demonstrated that surgery was cost-effective in comparison with conservative therapy with an incremental cost-effectiveness ratio (ICER) of £7175 per QALY. Economic modelling suggested that surgery produced an even greater benefit over 10 years with an ICER of £1936 per QALY. In comparison to conservative management, injection sclerotherapy was cost-effective with an ICER of £3500 per QALY. In view of the low cost of injection sclerotherapy, one may expect this to be the most cost-effective, but surgery produced a greater benefit with lower ICER, making it the dominant strategy in this study.
Health economic analyses from other trials
In comparison with the rigorous health economic analyses performed in the REACTIV trial, other studies have significant methodological weaknesses. Other studies evaluating cost-effectiveness are scarce, but a number of researchers have conducted in-trial assessments of treatment costs. In a UK randomized clinical study comparing RFA and surgery, an evaluation of costs (without effectiveness) revealed increased initial costs for RFA, which were partly (but not completely) offset by a quicker return to work. 5 An earlier randomized trial comparing surgical ligation and stripping to RFA using the original VNUS Closure system also drew similar conclusions, suggesting that the societal benefits of a quicker return to work compensated for the higher initial costs. 6 Conversely, a recent retrospective observational study from Texas suggested that the costs of RFA performed in an office-based setting are significantly lower than traditional surgery performed in the operating room ($906 versus $2622, respectively). 7 Some of the differences in treatment costs are likely to represent the varying reimbursement policies in different health-care systems.
The possible economic advantages of UGFS have been highlighted by a number of studies. In a recent publication reporting the results of a randomized study of EVLA + phlebectomy versus UGFS, a microcosting technique was used evaluate the costs of each treatment. 8 The authors reported that the median costs were significantly greater following EVLA (£725) compared with UGFS (£230). They concluded that UGFS was cheaper, with similar effectiveness to EVLA at three months. However, a greater number of re-interventions were required in the UGFS group. In a large randomized study comparing UGFS and traditional surgery for varicose veins, a similar cost analysis was performed. In keeping with other studies, UGFS was cheaper than traditional surgery with two-year mean hospital costs of €774 and €1824, respectively. 9
Although these studies do offer some useful information, isolated cost estimations without evaluations of effectiveness have significant limitations and are not generally favoured by health-care commissioners. Further prospective assessments of cost and effectiveness (with assessment of utilities using generic quality-of-life tools) are essential to fully understand the health economic implications of surgical and endo venous interventions. A large randomized controlled study assessing multiple endovenous interventions would be the ideal vehicle for such a health economic evaluation. A recent randomized study compared EVLA, RFA, UGFS and traditional surgery and successfully recruited 500 patients. Although a cost analysis was included, this was rudimentary and methodologically flawed. Unfortunately, this may represent a missed opportunity for a meaningful cost-effectiveness analysis. 10
Decision tree analysis of traditional and endovenous treatments
As there are a large number of surgical and endovenous treatment options available for varicose veins, comparison between multiple treatment options presents a significant challenge, as randomized trials with multiple treatment arms are difficult and expensive to perform. An alternative strategy commonly utilized by health economists is the decision tree or Markov model. Using this technique, the cost-effectiveness of eight different treatment strategies (Table 1) for patients with symptomatic great saphenous vein reflux was compared. 11 Procedures performed in office-based and operating room settings were included. Costs were obtained from Government health service tariffs and outcomes (QALYs) were estimated from results of published randomized trials including any of the treatment strategies evaluated.
Treatment strategies compared in Markov model
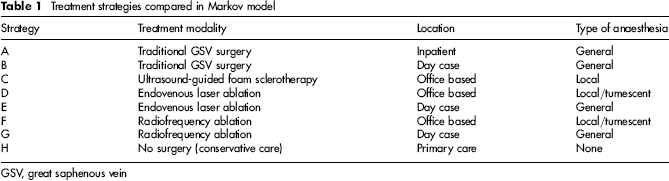
GSV, great saphenous vein
The findings demonstrated that UGFS, EVLA and RFA (performed in an office-based setting with injection sclerotherapy for residual varicosities) and tradition surgery (day case) were all cost-effective treatments in comparison to conservative management using a threshold of £20,000 per QALY. Although UGFS had the lowest absolute cost, the re-intervention rates were significantly higher than the other treatment strategies.
Which are the most cost-effective treatments?
Despite the growing body of health economic evidence for the management of varicose veins, many questions remain unanswered. It has been clearly demonstrated in a number of studies that intervention for varicose veins is cost-effective in comparison with conservative management. In an era where varicose veins are increasingly considered as a cosmetic issue ideal for rationing, this is an important message.
However, the most cost-effective treatment modality remains unclear. While there is strong evidence that UGFS is the cheapest treatment, the re-intervention rate is likely to be higher that other treatment modalities, offsetting some of the cost advantages. Moreover, an increasing number of venous specialists are utilizing a combination of endovenous or open and endovenous treatments to treat individual patients with complex patterns of venous reflux. Assessment of the cost-effectiveness of individual treatment components is extremely difficult in these circumstances.
Discussion
The management of venous disease consumes a significant proportion of the health-care budget in most western countries and identifying the most cost-effective treatments is particularly important in the current economic climate. The available evidence has limitations, but is seems clear that the treatment of varicose veins in general, is cost-effective in comparison with conservative management. This is an important message, particularly as it may seem appropriate to policy-makers to cut funding for ‘benign’ conditions such as venous disorders. Some may argue that patients should pay for venous interventions. However, with the enormous costs associated with the community management of venous ulceration, most clinicians would recognize that the presence of venous skin changes (C4 disease), healed (C5 disease) or open ulceration (C6 disease), indicates severe venous hypertension requiring venous intervention. The treatment of venous reflux to reduce the risk of recurrent venous ulceration has been clearly demonstrated in the ESCHAR trial. 12
There is insufficient, high-quality health economic evidence to clearly identify a single, cost-effective treatment strategy. As the population with venous disease is so heterogeneous, this is unlikely to happen. However, there are strong indications that the most cost-effective way to deliver treatment for varicose veins is using endovenous techniques performed in an outpatient or ‘office-based’ setting. Despite widespread acceptance of the importance of cost-effectiveness, health economic analyses are often poorly performed or omitted from clinical studies. In addition to improving the quality of health economic studies, researchers should also focus on identifying which patients are at greatest risk of progressing to ulceration, in order to best target superficial venous treatments.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Footnotes
The authors have no conflicts of interest to declare.