
Abstract
Venous malformations are the result of an arrested development of the venous system during the embryogenesis. In the treatment of venous malformations the standard of care is a multidisciplinary approach including the use of traditional surgical therapy if applicable and endovascular treatment. Endovascular techniques include embolization therapy for instance with coils but also sclerotherapy with liquid or foamed sclerosants. The aim of this paper is to give an overview of foam sclerotherapy in venous malformations. Sclerotherapy of venous malformations has been performed in superficial and intramuscular malformations. In many cases ethanol has been used for the treatment. Since more than 10 years, less aggressive sclerosants like polidocanol and sodiumtetradecyl sulphate have been used to treat venous malformations. These substances can be used without anaesthesia and the rate of side-effects is much lower. Yamaki and Cabrera are the first who used foam sclerotherapy for the treatment of symptomatic venous malformations. Compared with liquid sclerotherapy foam sclerotherapy has the advantage of a better and longer lasting contact of the sclerosing agent with the vessel wall which leads to a more effective treatment and to a reduction of concentrations needed. In a recent European Guideline on Sclerotherapy foam sclerotherapy is recommended over liquid therapy for the treatment of venous malformations. Foam sclerotherapy is an effective treatment option for low flow extratruncular and truncular venous malformations. Foam is significantly more effective than liquid sclerotherapy and side-effects with polidocanol or sodiumtetradecyl sulphate foam are less compared with sclerotherapy with ethanol. With foam sclerotherapy a significant reduction of pain and volume of the venous malformations can be reached.
Introduction
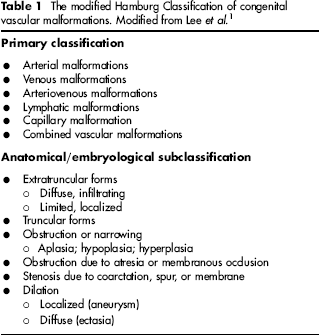
Vascular malformations are congenital anomalies of the vascular system. Venous malformations are the result of an arrested development of the venous system during the embryogenesis. 1 It is recommended to classify vascular malformations according to the modified Hamburg Classification of congenital vascular malformations into: arterial malformations, venous malformations, arteriovenous malformations, lymphatic malformations, capillary malformations and combined vascular malformations (Table 1).
The modified Hamburg Classification of congenital vascular malformations. Modified from Lee et al. 1
Venous malformations are often misdiagnosed as haemangioma. In contrary to venous malformations haemangioma are vascular tumours with a completely different aetiology and treatment.
2
Venous malformations may be extratruncular when they develop before the vascular trunks are developing or truncular if the development occurs during the truncular venous formation (Figure 1). Venous malformations can be located in the superficial and/or the deep venous system. The clinical findings with venous dilation and malformation may occur in a limited area and localized for instance in the skin or the subcutaneous tissue or in intramuscular veins. They can also be infiltrating and diffuse. In truncular venous malformations the clinical findings may show dilation and aneurysmatic malformation of the veins but hypoplasia and hyperplasia of veins are also common, especially in the deep venous system.1,2
Extratruncular venous malformation involving skin, subcutaneous fatty tissue and muscles
A combination with other vascular malformations like lymphatic or arterio-venous malformation is possible. 3
Before treating venous malformations it is always necessary to exclude obstruction of the deep venous system and to exclude arterial venous fistula. 3 It is important to document the extent of the venous malformation and the involvement of different tissues like subcutaneous tissues and muscles. The venous malformation is usually a low flow malformation. In arterio-venous malformations a high flow malformation in the venous system may result.
In the treatment of venous malformations the standard of care is a multidisciplinary approach including the use of traditional surgical therapy if applicable and endovascular treatment. 4
Endovascular techniques include embolization therapy for instance with coils but also sclerotherapy with liquid or foamed sclerosants.4,5
Sclerotherapy of venous malformations
Sclerotherapy of venous malformations has been performed in superficial and intramuscular malformations. In many cases ethanol has been used for the treatment.6–9 However the treatment with ethanol is painful and has a high risk of necrotic side-effects. This kind of treatment has to be performed under anaesthesia. Since more than 10 years, less aggressive sclerosants like polidocanol and sodiumtetradecyl sulphate have also been used to treat venous malformations.10–13 These substances can be used without anaesthesia and the rate of side-effects is much lower. Yamaki and Cabrera are the first who used foam sclerotherapy for the treatment of symptomatic venous malformations.14–16 Compared with liquid sclerotherapy foam sclerotherapy has the advantage of a better and longer lasting contact of the sclerosing agent with the vessel wall which leads to a more effective treatment and to a reduction of concentrations needed.
In a recent European Guideline on Sclerotherapy foam sclerotherapy is recommended over liquid therapy for the treatment of venous malformations.16,17 Recently Blaise et al. 18 demonstrated the effect of ultrasound sclerotherapy with polidocanol foam in the treatment of low-flow venous malformations in 25 patients between seven and 78 years of age. She used 0.25–3% polidocanol-foam. The number of sessions needed was 2.3 ranging between 1 and 16 sessions. After follow-up of five months, 23 of the 25 patients had less pain and 23 of the 25 patients had a size-reduction of the venous malformation. In nine patients the size-reduction was more than 50% and in 14 below 50%. Only in two patients non-severe side-effects occurred. In a prospective randomized study of ultrasound-guided foam sclerotherapy compared with ultrasound-guided liquid-sclerotherapy in the treatment of symptomatic venous malformations Yamaki et al. 19 treated 89 patients with extra truncular symptomatic malformations. The mean age was 14.5 years. For sclerotherapy 1% polidocanol or 10% Ethanolamine mainly in the deep malformations was used. With foam sclerotherapy a complete disappearance of the malformations could be reached in 44.9% compared with liquid-therapy with 25%. A partial disappearance could be reached in 44.9% with foam and 37.5% with liquid sclerotherapy. In one case in each group epidermal necrosis and in one case of the liquid group cutaneous necrosis occurred. Pain and swelling after sclerotherapy was comparable in both groups.
Principles of foam sclerotherapy of venous malformations
Good indications for foam sclerotherapy in venous malformations are low-flow malformations without arteriovenous involvement. The malformation may be extratruncular or truncular preferably in the superficial venous system. A complete diagnostic work-up has to be performed including duplex sonography and if necessary magnetic resonance tomography to document the extension of the malformation. Main goals of the treatment are the reduction of pain and discomfort, the reduction of the volume of the venous malformations and the improvement of the cosmetic aspect. Possible multiple sessions are often necessary. Side-effects are allergic reactions to the sclerosants, neurological symptoms, strong embolic complications, tissue necrosis, pigmentation, induration and pain. For sclerotherapy detergent agents like polidocanol and sodiumtetradecyl sulphate can be used. The recommended concentration ranges between 0.25% and 3% according to the size of the venous malformation. In most of the cases of superficial venous malformation 1% polidocanol or 0.5% sodiumtetradecyl sulphate can be used initially. The recommended relation between liquid and gas is 1 + 4. Room air can be used. As an alternative a 0 + 2 or 3 + 2 mixture can be used. For routine-use a maximum of 10 mL of foam is recommended. There is some evidence that with higher volumes more side-effects like visual disturbances and deep venous thrombosis may occur. For this reason higher volumes of foam can be used but a risk-benefit calculation should be performed. For a puncture of the vein with a short catheter or butterfly needle the patient can be in the upright of 45° position on a tilling table. For the foam injection the patient should always be in the horizontal position. For puncture of non-visible malformations duplex should be used. Again the foam injection should always be performed in the horizontal position. After slow start of the injection and the control of the needle position a quicker injection of the foam volume should be performed to fill the vessel homogeneously with foam. In diffuse venous malformations multiple injections should be performed. With duplex the distribution of the foam can be controlled and followed. In selected cases the injection can also be done under magnetic resonance angiography or angiographic control. After the injection the patient stays in the horizontal position on the table for 5–10 minutes. Afterwards we perform local excentric and concentric compression with cotton wool pads and compression stockings or compression bandages. The patients stay 30 minutes in the waiting room to control any short time side-effects like visible disturbances before he leaves the department. Follow-up visits should be performed.
In venous malformations with a large volume the technique can be modified. After puncturing the venous malformation with a short catheter the malformation is compressed by a compression bandage to reduce the volume. Afterwards the foam is injected.
Summary
Foam sclerotherapy is an effective treatment option for low flow extratruncular and truncular venous malformations. Foam is significantly more effective than liquid sclerotherapy and side-effects with polidocanol or sodiumtetradecyl sulphate foam are less compared with sclerotherapy with ethanol. With foam sclerotherapy a significant reduction of pain and volume of the venous malformations can be reached.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.
Footnotes
The authors have no conflicts of interest to declare.