
Abstract
Objective:
To assess whether re-do varicose vein surgery as a day case is feasible and safe.
Methods:
Data were collected retrospectively on 70 consecutive patients (77 legs) undergoing re-do sapheno-femoral or sapheno-popliteal ligation by consultant surgeons as day cases. Follow-up was by structured telephone interview.
Results:
The 70 patients comprised 53 females and 17 males. Median age and body mass index were 47.5 years and 27, respectively. All patients were ASA Grade I or II. Median operating time was 75 min (range 25–140). Of the 70 patients intended to be treated as day cases, four (5.7%) were admitted overnight. There were no were re-admissions nor did any patient develop deep vein thrombosis. Eleven per cent developed wound infection and 4% transient lymphatic leakage. Overall, 91% of patients were pleased with the initial surgical result but this decreased to 81% in the longer term. Eighty-nine per cent would have their surgery performed again as a day case.
Conclusion:
Re-do sapheno-femoral or sapheno-popliteal can be performed safely as a day case.
Introduction
Increasing pressure on in-patient beds and recommendations from the Royal Colleges of Surgeons has led to an increase in the number of patients undergoing day surgery. Primary varicose vein surgery is well established as a day procedure in the UK. However, re-do sapheno-femoral ligation (SFL) and sapheno-popliteal ligation (SPL) are often performed as in-patient procedures because the surgery can be technically demanding and of long duration. As re-do varicose vein surgery can comprise up to 25% of varicose vein procedures, significant efficiency could be achieved and waiting lists reduced if these operations were performed as day cases. This study evaluates the feasibility and safety of day re-do varicose vein surgery.
Methods
The study was conducted in two parts. Data were collected retrospectively on all patients who underwent surgery for recurrent varicose veins during a 44-month period (June 2002 to February 2006). Patients who had re-do SFL and/or SPL as part of their operation were included in the study. Patients who had phlebectomies only, without re-do junctional ligation for recurrent varicose veins were excluded. Demographic profile, body mass index (BMI), operation details, immediate post-operative complications, unexpected overnight stay and re-admission were recorded on a pre-designed proforma.
The second part of the study was conducted by telephone using a structured questionnaire to assess intermediate outcome and patient satisfaction 1 following operation. The time interval from operation to interview ranged from nine to 54 months. Two patients who could not be contacted were excluded from the study.
There are dedicated day surgery units on all Doncaster & Bassetlaw Hospitals NHS Foundation Trust sites. Strict criteria were already in place to assess the suitability of patients for day surgery including medical, anaesthetic and social assessments. All patients underwent pre-operative duplex assessment of the affected limb in our vascular laboratory by a dedicated vascular technician. All patients were ASA I or II and attended a nurse-led pre-assessment clinic where they were provided with relevant leaflets and advice.
Operating lists were scheduled as morning sessions to allow patients sufficient time for recovery. A senior anaesthetist saw patients on the morning of surgery. Low-molecular-weight heparin was administered to patients considered at high risk of developing deep vein thrombosis (DVT; patients with previous history of DVT/pulmonary embolism). Operations were performed under general anaesthesia either by a consultant vascular surgeon or by a registrar under supervision. Following surgery, patients were discharged to the care of their primary care physician.
Results
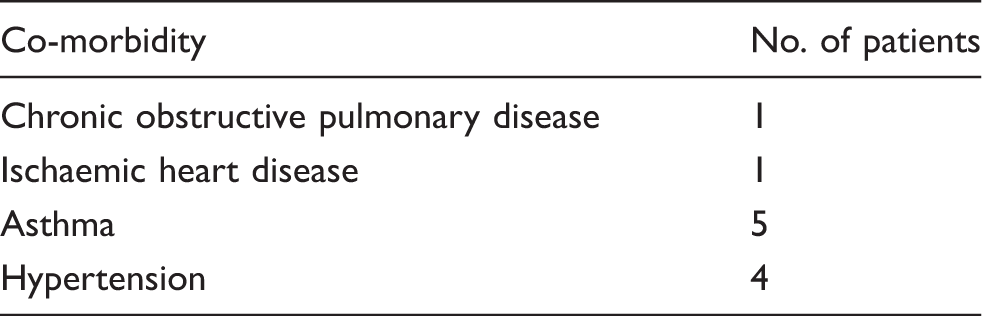
During the period of the study, 70 patients (77 legs) underwent re-do main trunk varicose vein surgery and were included in the study. There were 53 females and 17 males, with a median age of 47.5 years (Figure 1). Fifty-six patients (80%) had a BMI less than 30 with a median of 27 (Figure 2). Fifty-nine patients (84%) were categorised ASA I and 11 patients (16%) were ASA II with associated co-morbidity (Table 1).
Age distribution. BMI. Co-morbidities.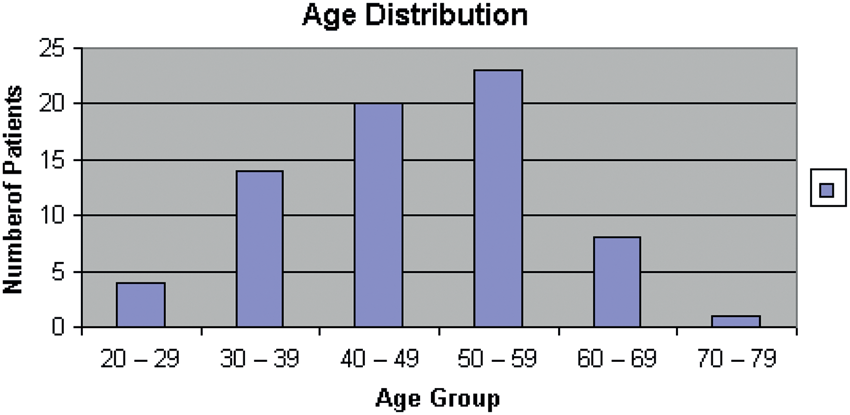

Of 77 operated legs, 70 were re-do SFL and seven re-do SPL (right = 50, left = 27). Seven patients had surgery performed on both lower limbs, four at the same sitting. Operation time ranged from 25 to 140 min (median = 75). Sixty-six patients (94.3%) went home on the day of operation, whilst four (5.7%) required overnight admission. Reasons for overnight admission were post-operative nausea and vomiting (n = 1), delayed recovery (n = 1), post-operative hypoxia requiring oxygen (n = 1), and social reasons (n = 1). There were no re-admissions following discharge.
Indications for re-do surgery.

Patient satisfaction following surgery.

Post-operative wound infection occurred in nine legs (11.8%) and lymph leak in three legs (3.9%). There were seven reported cases of vein recurrence (bad as before, n = 6; worse than before, n = 1). Two patients required further intervention (sclerotherapy, n = 1; surgery, n = 1). There were also reports of minor patches of numbness related to scars (n = 11), thread veins (n = 4) and ankle swelling (n = 1), following surgery. There were no reported cases of DVT.
Four patients not requiring overnight stay said that they would have preferred to be inpatients.
Discussion
The high prevalence of varicose veins 2 as well as the low priority afforded to them 3 ensures that there is a waiting list for the treatment. Several reports have confirmed the safety and acceptability of day surgery for primary varicose veins.4,5 There is scant information regarding objective measurements of the outcome of surgery for recurrent veins. To date, studies performed are small and not comparable to ours, due to differences in methodology, duration of follow-up 6 and the fact that they examine recurrence from a surgeon’s perspective. Our study assessed the quality of surgical outcome from the patients’ perspective.
Edwards et al. 7 described a 35% recurrence rate after re-do varicose vein surgery from a patient perspective. Only 10% of our patients reported recurrence at the time of interview. The incidence of complications following recurrent varicose vein surgery varies in the literature (20–57%). 8 In our series, 15.7% developed complications, mainly wound infection (11.8%) and lymphatic leak (3.9%). There was no clinically apparent DVT. Ninety-four per cent of our patients were discharged on the same day. Most patients (91%) were pleased with the initial results of re-do surgery but this decreased to 81% in the longer term. The main reasons for dissatisfaction were recurrent/residual veins and wound complications. Eighty-nine per cent of our patients stated that they would opt for day surgery if they were to have their operations again.
The fact that the patients were not examined following surgery is a limitation of our study. The patients’ satisfaction may have been confounded by the memory bias as patients may have forgotten about the surgery. In addition, two patients were lost to follow-up. Despite these weaknesses, our results are favourable and suggest that with proper organisation, day-case re-do varicose vein surgery is feasible and relatively safe.
The introduction of newer techniques 9 such as endovenous laser, radiofrequency and sclerotherapy facilitates a greater proportion of patients with recurrent veins to be treated as day cases. However, there will remain some patients who require surgery. We recommend that re-do SFL/SPL be performed as day cases by default unless anaesthetically unfit. Social circumstances should be fully addressed before scheduling patients for day surgery. Few patients will require overnight admission for delayed recovery from anaesthetic. This should not be regarded as a failure of day care service but a necessary contingency if good results are to be achieved.
Footnotes
Declaration of interest
All the authors have no conflict of interest and nothing to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.