
Abstract
Purpose
To retrospectively evaluate the feasibility and effectiveness of endovenous laser ablation or ultrasound-guided foam sclerotherapy for Giacomini vein insufficiency. This is the largest cohort of patients treated for Giacomini vein insufficiency with endovenous laser ablation or ultrasound-guided foam sclerotherapy.
Material and methods
Over a three-year period, 23 females and nine males (age range, 19–67 years) treated for Giacomini vein insufficiency with or without saphenous vein insufficiency were retrospectively reviewed. Diagnosis of venous insufficiency was made by color Doppler ultrasonography. Symptomatic insufficiency of the Giacomini vein or the saphenous veins was treated with endovenous laser ablation. Ultrasound-guided foam sclerotherapy was used for tortuous incompetent Giacomini veins. The venous disease was categorized according to the clinical, etiological, anatomical, and pathological classification, and clinical severity was graded with the venous clinical severity score. Follow-up included clinical examination and color Doppler ultrasonography.
Results
Thirty-nine limbs in 32 patients were treated (25 endovenous laser ablation and seven ultrasound-guided foam sclerotherapy). All procedures were technically successful. One patient in the ultrasound-guided foam sclerotherapy group had a recurrence with successful repeated treatment. Recurrence was not seen in the endovenous laser ablation group. No complications were observed. All patients had resolution and improvement in 100% of their symptoms at 12 months of follow-up.
Conclusion
Giacomini vein insufficiency is mostly seen with insufficiency of the great saphenous vein and can be effectively treated with endovenous laser ablation or ultrasound-guided foam sclerotherapy.
Introduction
The Giacomini vein (GV), one of the thigh extensions of the small saphenous vein (SSV) that extends up to the posterior thigh, travels medially and joins the posterior thigh circumflex vein before draining into the great saphenous vein (GSV). It was first described in 1873 by Giacomini and is present in 2.5–86% of the population.1–5 This intersaphenous vein usually lies in a groove between the semitendinosus muscle medially and the long head of the biceps femoris muscle laterally. The thigh extension and GV may transmit reflux from the GSV to the SSV or may transmit an “ascending reflux” from the saphenopopliteal junction superiorly to the GSV. The SSV continues directly as the GV into the GSV in 14% of the population.6–8
Giacomini gave a detailed description of the anatomical variations of the GV, and since then anatomical study of the GV has been supplemented by functional study through the use of ultrasonography. 9 The GV typically presents in three sections: distal and proximal sections that lie in the saphenous compartment and a middle section that is usually subcutaneous. 8 The clinical importance of Giacomini vein insufficiency (GVI) is largely unknown. There are few case series reporting endovenous laser ablation (EVLA) with ultrasound-guided foam sclerotherapy (USGFS) of the GVI. 7 In this retrospective study, we report outcomes of endovenous treatment of patients who had GVI.
Materials and methods
Clinical presentations and characteristics of the patients.
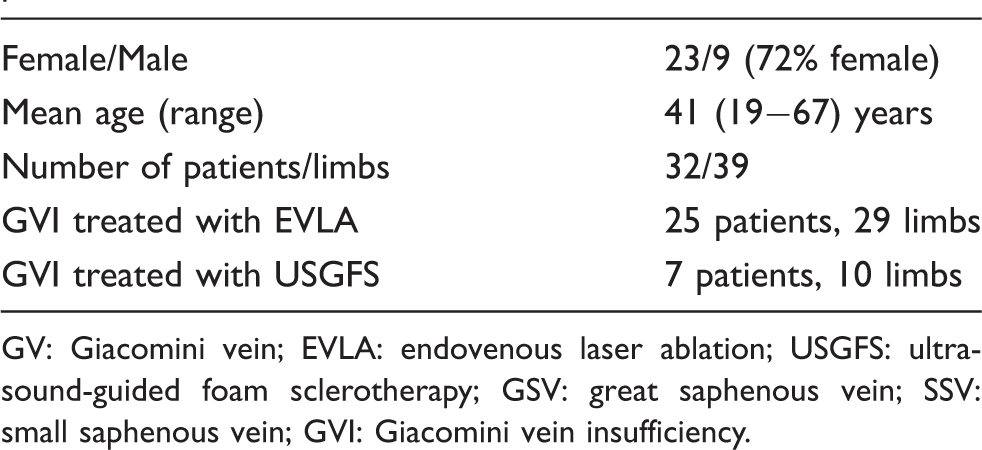
GV: Giacomini vein; EVLA: endovenous laser ablation; USGFS: ultrasound-guided foam sclerotherapy; GSV: great saphenous vein; SSV: small saphenous vein; GVI: Giacomini vein insufficiency.
The venous disease was categorized by clinical, etiological, anatomical and pathological (CEAP) classification, and clinical severity was graded with the venous clinical severity score (VCSS) recommended by the Society of Interventional Radiology. 10 All patients were symptomatic for chronic venous insufficiency and were CEAP Class 2 or greater. GV diameter was measured in all patients. Each patient had a physical examination and color Doppler ultrasonography (CDUS) examination of both lower extremities before and after the treatment by the same physician who also performed the endovenous therapeutic procedures. Diagnosis of insufficiency of the saphenous vein and the GV was made with color Doppler and duplex ultrasonography while the patient was standing. Ultrasonographic examination was performed using 9-MHz or 13-MHz multifrequency transducers (Antares, Siemens, Erlangen, Germany). All patients were examined for superficial as well as deep venous reflux and venous thrombosis. A venous reflux lasting longer than 0.5 s in the saphenous veins or the GV and longer than 1 s in the deep veins with compression and release or Valsalva maneuver was diagnostic for venous insufficiency.11–13
The procedure was carried out under local anesthesia in an outpatient treatment facility. All patients had sedation and analgesia with dormicum and fentanyl just before and during the procedure. Insufficiency of the saphenous veins was treated with EVLA in all cases. GVI was treated with EVLA if the vein had a straight course where placement of a laser fiber was possible. If the course of the insufficient GV was tortuous and placement of a laser fiber was not possible, then USGFS was performed. Insufficiency of other trunkal veins such as anterior thigh circumflex vein was also treated if they caused cosmetic or clinical complaints for the patients. Insufficiency of the GV or the saphenous veins, if present, was treated at the same session. Some patients also underwent sclerotherapy of the large varices during the same session. Ambulatory phlebectomy was not performed in any of the patients, as this was not our routine procedure.
EVLA procedure
The technique for treatment of the saphenous veins has been explained elsewhere.14,15 In brief, the punctures, placement of catheters, and tumescent anesthesia were performed under ultrasonography guidance. The tip of the laser fiber was placed through a long vascular sheath at the target point (saphenofemoral junction, saphenopopliteal junction or proximal GV/posterior thigh circumflex vein). Tumescent anesthesia was applied around the vein. 16 The tip of the laser fiber was placed exposing 1–2 cm of the laser fiber. A 600-micron laser fiber was used at 940-nm (Dornier, MedTech Laser GmbH, Germering, Germany) or 810-nm (Vari-Lase, Vascular solution, USA) wavelength for EVLA. The energy delivered was 120 J/cm for proximal GSV, 60 J/cm for distal GSV and the SSV, and 80 J/cm for the GV. Slow fiber withdrawal was employed in continuous mode to deliver the required energy.11–12
The GV was punctured at its most caudal level under ultrasonographic guidance, usually just above the popliteal fossa for EVLA procedure. If the SSV had associated insufficiency, then the puncture was made at the most caudal part of the SSV insufficiency. 17 If insufficiency of the GV was present along its entire course, the guide wire was advanced as cranially as possible. It was sometimes very hard to direct the guide wire or the laser fiber medially up to the GSV. In such cases, a diagnostic catheter and a hydrophilic guide wire were used to advance the long sheath up to the GSV. In all cases, the tip of the laser fiber was parked at the most cranial part of the GV, if technically possible. If insufficiency of the GV was confined to the posterior thigh, then the tip of the fiber was parked at the most proximal part of insufficient vein.
USGSF
The GV was identified by CDUS. Sclerosing foams were prepared using the technique described by Tessari, applying a sclerosant to air ratio of 1–3. 18 The treatment with USGFS consisted of a single or double injection of 1–3% foam (Aethoxysklerol; Kreussler Pharma, Wiesbaden, Germany) with the patient in the prone position. The operator observing the filling of the GV determined the final volume. A class II compression stocking was applied immediately after the procedure with the patient lying down. Stockings were indicated for use for three weeks. Patients were advised to walk for 15 min immediately after the influence of the sedoanalgesia was over. Patients were sent home with written instructions to take a nonsteroidal anti-inflammatory medication for postprocedural pain, if required.
The primary outcome was successful treatment of the GV vein, which was defined as complete ablation of the treated vein. Recurrences were defined as patency of the vein (3 cm or more in length) with or without reflux by CDUS examination. Secondary outcome measures were improvement of symptoms and VCSS.
Follow-up included physical examination and color Doppler US examination. Physical examination was performed to determine outcomes and side effects, such as induration, ecchymosis, phlebitis, and others. VCSS and CEAP scores were assessed pre-treatment and at each clinical visit. Color Doppler and duplex examinations were performed at three, six, and 12 months after the treatment to demonstrate the patency of the vein and reflux according to SIR reporting standards. 10 The symptoms of each patient were recorded at each follow-up according to a scale of resolution, improvement, no change, and deterioration of symptoms.
Results
CEAP (clinical, etiological, anatomical and pathological).
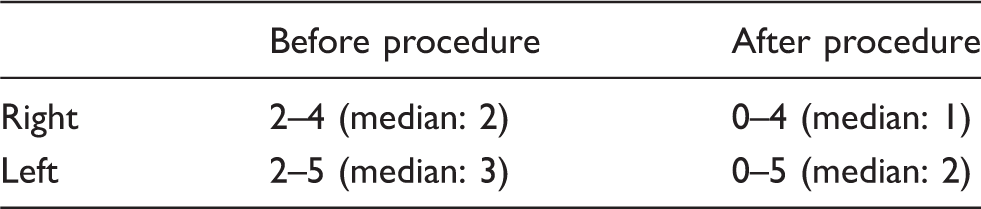
VCSS (venous clinical severity score).

Distribution of truncal venous insufficiencies in the superficial limb veins.

GV: Giacomini vein; GSV: great saphenous vein; SSV: small saphenous vein.
Technical success was achieved in all cases. All patients had resolution and improvement in 100% of their symptoms at 12 months of follow-up. There were no complications other than expected postprocedural complaints of pain, bruising, and cord-like tightening along the course of the treated vein. All patients had clinical and sonographic follow-up at three months; six patients had a six-month follow-up, and six patients had a 12-month follow-up. We did not encounter any recurrences of the GVI in patients who had EVLA. There was one recurrence of the GVI three months after the treatment with USGFS. This patient had a repeated USGFS with successful outcome.
Discussion
This study showed that insufficiency of the GV can be seen in clinical practice and is not very rare. We cannot give the prevalence of GVI in the population, as the total number of patients from which these 32 patients were recruited was not certain. GVI was unilateral in most cases and was more frequently observed in association with saphenous vein insufficiency than without. Isolated GVI was present in only three limbs and caused similar complaints of saphenous vein insufficiency in the affected limb. Patients experienced improvement or resolution of their symptoms after treatment. However, improvements of the symptoms were mostly due to treatment of the GSV. It is hard to draw a conclusion on the improvement of symptoms resulting from treatment of GVI, as only three patients had isolated GVI. Complications were not encountered in any patients with GVI after treatment with EVLA or USGFS. The clinical importance of GVI is largely unknown because most cases had associated GSV or SSV insufficiency and isolated GVI is probably rare. In our series, we identified three isolated GVs in the left limb.
The GV is the best-known cranial extension branch of the SSV. Giacomini, in his original dissection study, described 51 limbs with variation of the cranial extension of the SSV. The SSV emptied into the GSV through the GV in 12% of the cases. However, with new studies using ultrasonography, we know that the incidence of GV is higher; there are other possible variations than the reported dissection findings. Studies in the literature reported a GV prevalence of up to 92%. GVI has a prevalence of 2.5–10%. The cranial extension of the SSV and GV were divided into three categories in a recent study. 6 Group I had a true intersaphenus connection without any significant branching. Group II included the anatomical pattern of a cranial extension branch with connection to the femoral vein by means of a perforating vein. Group III had a cranial extension associated with collaterals from a thigh or pelvic vein.
Endovenous thermal ablation and sclerotherapy are minimally invasive alternatives to high ligation and surgical stripping of the incompetent saphenous vein.11–13 However, studies on the treatment of GVI are very rare in the literature. The first study on the treatment of GVI was reported by Theivacumar et al. 7 on two patients who had GVI with competent proximal GSV and incompetent GSV distal to the draining point of the GV. The SSV was competent but the saphenopopliteal junction and the GVs were incompetent. The authors treated the distal GSV with EVLA and left the GV without treatment. The saphenopopliteal junction became competent with the resolution of symptoms after the treatment of both GSVs in both patients. All the varicose veins disappeared completely, but one patient required an additional sclerotherapy session.
Another study reported treatment of 14 patients with GVI with successful outcomes. 8 The thigh extension branch anatomy was grouped into three categories. In the first group, eight patients were treated. In the second group of four patients, the GV ended in the femoral vein via a perforator. In the third group, GV in two cases ended in the pelvic and thigh veins through collateral connections. In a study by Park et al., 13 18 limbs of 18 patients were treated using EVLA. USGFS was also used in all patients for the treatment of varicosities before the EVLA procedure. The outcome was excellent with ablation of all GVI in the 18 limbs immediately after the operation and during a short-term (12-month) follow-up period. The common outcomes for all studies were excellent. There were no recurrences of the treated GVI after two years of follow-up in any of the patients.
The GV did not always follow a straight course in the posterior thigh, making advancement of a laser fiber difficult, if not impossible. This finding might be due to the duration of insufficiency of the GV where the vein became tortuous as the duration of insufficiency increased. In such cases, we used USGFS, which was found to be very effective at follow-up. We believe the tortuous course of the vein and successful ablation of the GSV or the SSV helped successful ablation of the GVI after USGFS in most cases.
There are some limitations of the study. The retrospective nature of the study is one of the limitations. We did not examine paradoxical reflux in these patients. This may have given additional information regarding the importance of the GVI, especially when present with GSV insufficiency.
Conclusion
GVI is probably not rare and is mostly seen with insufficiency of the GSV and rarely without it. EVLA and USGFS seem promising for treating insufficiency of the GV.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The ethics committee of Baskent University approved this study (REC number: KA12/127).
Guarantor
LO.
Contributorship
LO researched literature and conceived the study; involved in protocol development, gaining ethical approval, patient recruitment and data analysis; and wrote the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.