
Abstract
Objective
To assess the efficacy and safety of a new method of clearing varicose veins in the long term. It consists of applying the long-pulsed Nd:YAG laser following the injection of polidocanol microfoam, in two consecutive sessions, treating both legs in full in each session.
Method
Randomized, Polidocanol-controlled, blind evaluation clinical trial comparing the results between 79 legs treated with Polidocanol and 517 treated with Polidocanol + Laser. Photographs were taken preoperatively and at three months, two years and three years after treatment, as well as patient self-assessments.
Results
Polidocanol + Laser is much more effective than polidocanol microfoam in clearing venulectasias with a diameter under 4 mm (p < 0.001). After three years, clearing percentages of 89% (Class I veins), 94% (Class II veins) and 95% (Class III veins) are observed, in comparison to 15%, 18% and 17%, respectively when only polidocanol was applied. No unexpected adverse effects were found and 86% of patients stated they were Satisfied or Very Satisfied.
Conclusion
The method leads to safe, fast and apparently permanent results. The treatment session lasts less than 1 h, and could become a first-choice treatment for the removal of all types of varicose veins with a diameter under 4 mm.
Introduction
Sclerotherapy continues to be the gold standard treatment for clearing telangiectasias and reticular veins (classes I, II and III), with a diameter of less than 4 mm.1–4 Among the different procedures and materials available, the injection of polidocanol (POL) microfoam most likely achieves the best results. However, when varicose veins are very widespread in both legs, a high number of therapy and maintenance sessions are required.1–4 The 1064 nm Nd:YAG laser is also effective, but the limitation of the caliber of the vessels which can be accessed, the pain at high fluences and the occurrence of relapses have held back its development for this use.5,6
Twelve years ago, at the Instituto Médico Laser (IML, Madrid, Spain), it was observed that, when applying the Nd:YAG laser immediately after the injection of POL microfoam, the abovementioned venous lesions cleared almost completely, and the effects achieved appeared to be permanent. Several trials were performed in order to determine the optimal procedure, which showed that results were very good after a single session, and even better after a second follow-up session three weeks later. Therefore, in 2003, this protocol was added to our daily practice as a recommended initial treatment for large areas of varicose veins. In order to validate this method, a clinical trial was conducted between 2004 and 2008, the results of which are presented in this paper.
Before assessing these results, possible action mechanisms and physical interactions between POL, the Nd:YAG laser and the vessel wall were examined, which would explain the remarkable synergic effect observed on the patients. It was confirmed that the properties of both POL and the Nd:YAG laser could be altered when certain conditions were achieved.7–9 The presence of POL foam bubbles inside the vessel while applying pulse lengths and fluences lower than those used by other authors is required.7–10
Another study assessed the efficacy of this method in the treatment of spider leg veins measuring less than 1.5 mm, on skin type IV patients, comparing the results of the combined therapy (POL + Laser) with those obtained when only POL or the Nd:YAG laser, separately, were applied. The combined treatment produced a considerable improvement in the clearing of veins in the short term (three months after treatment), in comparison to both treatments in isolation, but the results could not be proven to be permanent. 9
The purpose of this paper is to present the clinical evaluation of the treatment of leg telangiectasias and reticular veins (classes I to III) using 1064 nm Nd:YAG laser pulses, following prior injections of POL microfoam in a large series of patients with a long-term control and follow-up.
Material and methods
A randomized, POL-controlled, blind evaluation clinical trial was designed with two objectives: (1) To assess the efficacy and safety of the treatment with Nd:YAG laser after POL microfoam injection in the clearing of venulectasias with a three-year follow-up. (2) To compare the results of the combined treatment (POL + Laser), with those obtained when only POL foam is applied.
Patients were recruited from scheduled visits at the IML (Madrid, Spain), between April and September 2004, to begin the assay as of the month of October. Those who met the inclusion criteria were offered the possibility of taking part in a clinical trial, with a clear explanation of the aims of the study, expected results and potential adverse effects. Prior to inclusion in the trial, all patients were examined by ultrasound (Doppler ultrasound Soniline 050, Siemens, Issaqua, Japan) to rule out deep system reflux at the saphenous junctions and in the perforating veins.
Inclusion criteria were: (1) Age from 18 to 74 years. (2) More than 20% approx. leg’s surface with varicosities, presenting various vein classes. (3) Not having received any previous treatment for varicose veins. Exclusion criteria were: (1) Confirmation of reflux in the deep system by Doppler (2) Organic or psychological conditions which advised against the treatment or which could alter the assessment of results.
The assay was approved by the Antoni de Gimbernat Foundation Ethics Committee and all patients signed a written informed consent form prior to their inclusion in the study. All subjects agreed to the terms and conditions for inclusion in the trial and undertook to appear at the subsequent control and follow-up examinations on set dates, keeping in regular telephone contact with the IML.
A total of 320 patients, all females, aged 19 to 72 years (mean age 46.3 years) and with Fitzpatrick skin types II to IV, were recruited for treatment of both legs in full. The treatments were randomized by sealed envelope, so that 550 legs were assigned the combined treatment (POL + Laser) and 90 legs were allocated to treatment with POL only. Both groups were deemed to be clinically comparable in terms of age and presence of lesions.
For each patient, leg veins were defined as follows: Class I (red vessels of less than 0.5 mm in diameter), Class II (red-blue venulectasias of 0.5 to 1.5 mm in diameter) and Class III (blue reticular veins measuring between 1.5 and 4 mm in diameter). Most patients presented several of these types of lesions.
Each patient received two single treatment sessions, at a three-week interval, with treatment of both legs in full, from groin to ankle, in each session. The second session was considered a reinforcement session of the first. Treatment efficacy was assessed at three months, two years and three years after the second session of treatment. Adverse effects were studied during the procedure, at early post-operative stages and in long-term follow-ups. All treatments were applied by the same physician, trained by the discoverer of the technique. Only the therapist, not the patient or blind evaluators, had knowledge of the treatment applied.
Procedure
Every leg was disinfected for treatment using hydrogen peroxide. The POL microfoam was then injected using a 2 mL Omnifix syringe with a 30 G needle. The sclerosant concentration was 0.3% in all cases and the maximum amount injected was 20 mL in both legs overall, generally less than 10 mL in each leg. Injection caused vessels to blanch, and then a delay time of 1–3 min was necessary for the vessels to recover a soft pink colour. In the following step, the laser was applied along the whole length of the vessel until it was totally covered by laser pulses. After treatment, patients used compression stockings for two weeks, being worn during the day and removed at night.
The procedure is quick, although it depends on the number and type of varicose veins present. A session treating both legs lasts less than 1 h. The treatment of each leg takes 20–25 min, about 10–15 min for the POL injections and around 10 min for the laser application. Working at high frequencies (2–5 Hz) the irradiation time is short.
Treatment with POL
The microfoam was obtained using two 10-mL Omnifix syringes with a Luer-Lock connection, a three-way stopcock to connect the syringes and a 15 G load needle with an air microfilter. Two millilitres of POL (Aethoxysclerol® tamponné/lauromacrogol 400, Kreussler Pharma, Germany) was used at 0.3% and 8 mL of air. POL concentration at 0.3% was obtained by diluting the commercial preparation with a saline solution of 0.5% concentration. Pumping and switching the solution from one syringe to the other 15 times produces a stable microfoam following the Tessari technique.11–13 The resulting foam is rich in nitrogen, a low-solubility gas, presenting an irregular bubble size and high internal cohesion. 14
Treatment with Nd:YAG laser
The laser used was a 1064 nm long pulse Nd:YAG (with long pulse duration of millisecond order), Laserscope Lyra ‘i’™ (Laserscope, San Jose, CA, USA). Laser energy per pulse is delivered at the same time as a constant cooling of the skin surface occurs, due to the glass chamber adapted to the tip of the handpiece nozzle. The coolant is constantly circulated to cool down the skin and, in addition, a continuous air flow produced by a cooling device (Cryo 5, Zimmer Elektromedizin, Neu Ulm, Germany) at a temperature of 4℃ is directed onto the surface where the laser pulses are being applied.
The diameter of the spot used was equal to or slightly larger than the size of the vessel, ranging between 2 and 5 mm. The energy per pulse was similar, regardless of the spot size. For 2 mm spots, the energy per pulse was 9.42 J, whereas, for 5 mm spots, it was 11.77 J/pulse. Pulse width was 30 ms for Classes I and II, and 50 ms for Class III. Pulse repetition rate was 5 Hz for Classes I and II, and 2 Hz for Class III.
Assessment of results
To objectively determine the degree of vessel clearance, the treated areas were analysed by macro-photography using a Canon EOS 400D photo camera (Tokina ATX Pro 100 f 2.8 Macro, Sea & Sea Flash Macro DRF 14, Tokyo, Japan), fitted with a macrolens. The photographs were taken before the first treatment and at three months, two years and three years after the second treatment, respectively. For the purpose of comparison, frontal, dorsal and oblique photographs were taken of both legs, focusing on the areas most affected and covering the entire surface of each leg through various photographs. Some of the most affected areas were also photographed at a constant distance of 18 cm to study the clearing rate, using a previously validated computerized system. 15 The software program produced objective clearing percentages only for the photographed area, which served as a guideline for the evaluators who rated the overall clearing rate achieved for the total surface area of each leg.
A subjective clearing scale was established as follows: 0 points (no changes observed or condition worsened), 1 point (20% clearing), 2 points (40% clearing), 3 points (60% clearing), 4 points (80% clearing) and 5 points (full clearing of veins). Three blinded physician investigators, familiar with leg vein treatment, rated the degree of clearing on the basis of all photographed images. Ratings were established separately for each vein class (I, II and III), observing and comparing the total surface area of each leg in all photographs. The average rating of all three evaluators was used for statistical analysis.
Patients were informed that the objective of the new treatment was to remove the presence of varicose veins in the short and long term. Before the procedure, the patient and the therapist together analysed the varicose veins in detail and agreed on what would be considered a satisfactory or unsatisfactory result. Each patient filled out two questionnaires: the first at the three-month assessment and, the second, upon completion of the study, with separate distinction of the degree of satisfaction with the treatment for each leg (Very Dissatisfied, Dissatisfied, Somewhat Satisfied, Satisfied and Very Satisfied). Other questions relating to the practicability of both techniques and potential adverse effects were also included.
Any possible complications and side effects were recorded during the procedure, at the immediate post-treatment stage and at the long-term follow-ups. On the following day, the seventh day, and the third month, visual signs on inspection and discomfort related by each patient were investigated for each leg separately and recorded in detail in the patients’ medical histories. Enquiries were made as to the pain experienced during the procedure for each treatment, rated as Light, Moderate, Severe or Very Severe.
Statistical analysis
Data was entered and processed using the software program SPSS v.13.0 for Windows. Descriptive statistical data included the average or arithmetic mean (m), standard deviation (SD), median (M), range (r) and percentage (%). The main statistical procedure was the estimation of percentages based on an ordinal semi-quantitative scale. Agreement between the evaluators was assessed using Cohen’s Kappa test (κ). Groups of veins were compared, according to their class and follow-up times, using the Mann–Whitney U test. A p value of <0.05 was considered statistically significant. To determine the effect size of the POL + Laser treatment, Cohen’s d value was calculated as the difference of the means of both treatments divided by the pooled SDs. A large effect was considered when d > 0.8, meaning that the increase in therapeutic effect was greater than 0.8 SDs.
Results
Twenty two of the 320 patients did not complete the study for reasons unrelated to the investigation, or failed to appear at any of the follow-up visits and were thus excluded. Results were analysed for a total of 79 legs treated with POL and 517 legs treated with POL and Nd:YAG laser.
Efficacy results
Intra-group efficacy results. Clearing ratings are specified by groups for each treatment and type of vein, throughout the follow-up period (mean, SD, median and range). The average rating of all three evaluators was used for statistical analysis.

The values indicate the clearing percentage (0 = 0%, 5 = 100%).
The combined treatment proves to be more effective than the treatment with POL alone in the comparisons at three months, two years and three years for all the types of veins (p < 0.001 in all cases). In the short term (three months), the therapeutic effect of the POL + Laser treatment was more than 5 SDs greater when compared to the POL-alone treatment (Cohen’s d values were 7.56, 4.72 and 4.87 for Class I, II and III veins, respectively). In the long term (three years), differences exceeded eight SDs (Cohen’s d values were 8.22, 11.03 and 12.65 for Class I, II and III veins, respectively).
When POL is applied on its own, an average clearing of less than 30–40% is achieved, with maximum results of 2.18 being obtained for Class III veins, equal to 43%, at the third month. Class I vessels fail to reach 20%, and the effects largely disappear within two to three years for all types of veins treated. After three years, the average clearing rates of the group treated with POL alone were lower than 20% and, in some cases, the varicose veins worsened (Table 1). The POL + Laser treatment achieves clearing rates of around 90% or above. By the third year, rates of 89% for Class I veins, 94% for Class II veins, and 95% for Class III veins, can be observed (Table 1).
Degree of satisfaction of patients with legs treated with POL only (n = 79) and POL + Laser (n = 517).

The values indicate the number of self-assessed legs and the percentage of the total assessed, according to the questionnaires completed at three months and three years.
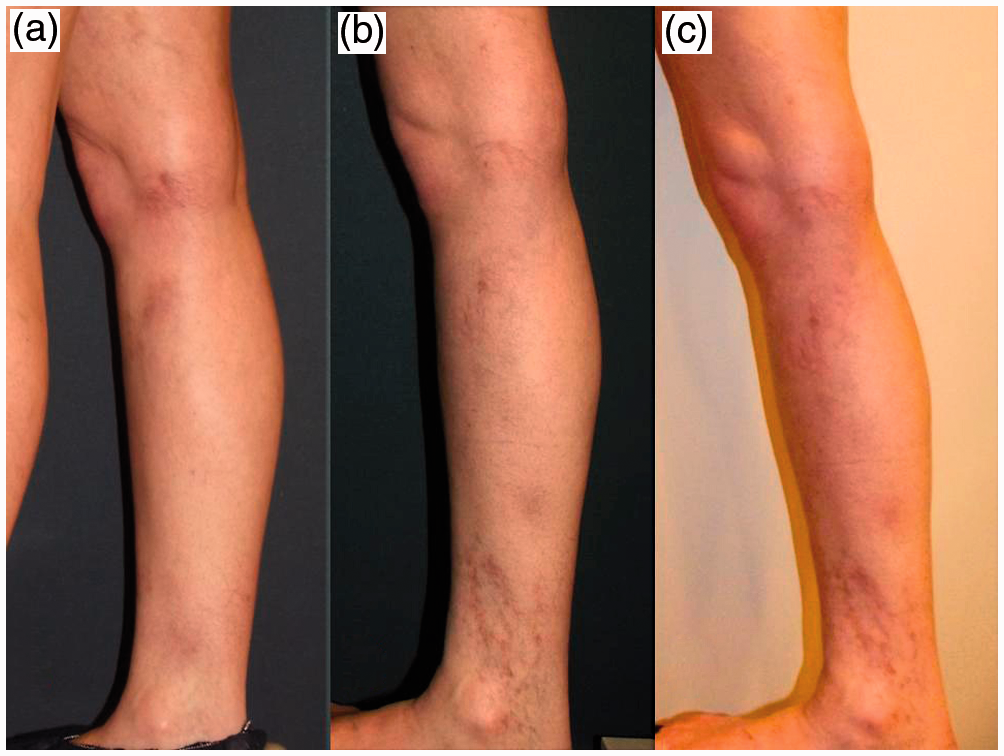
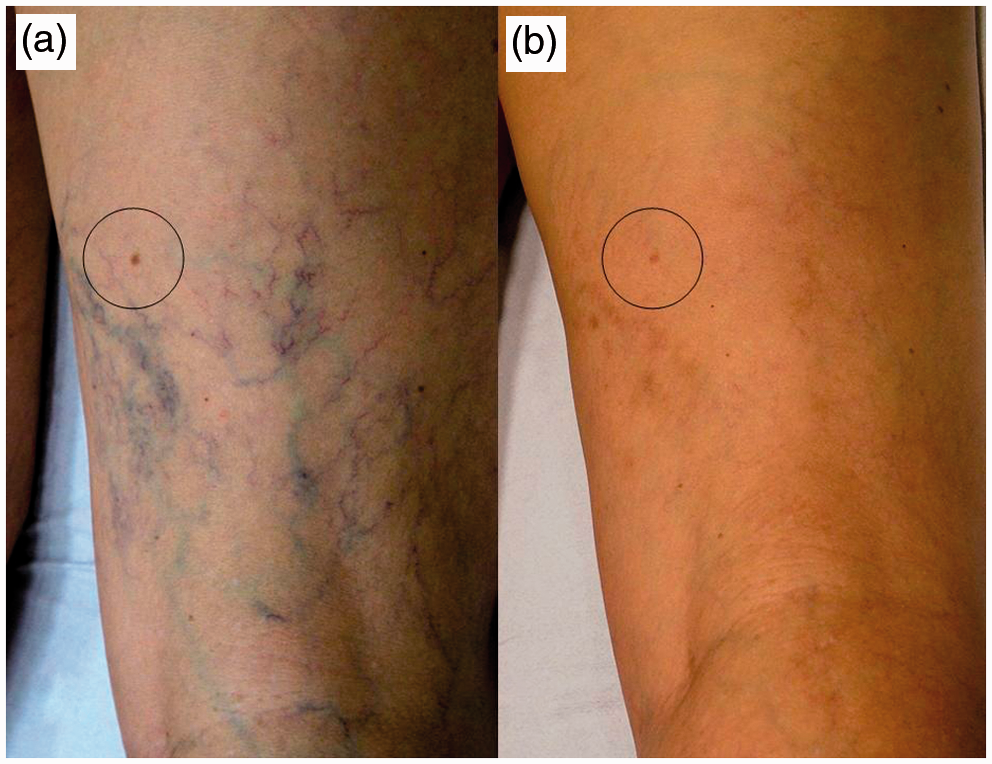
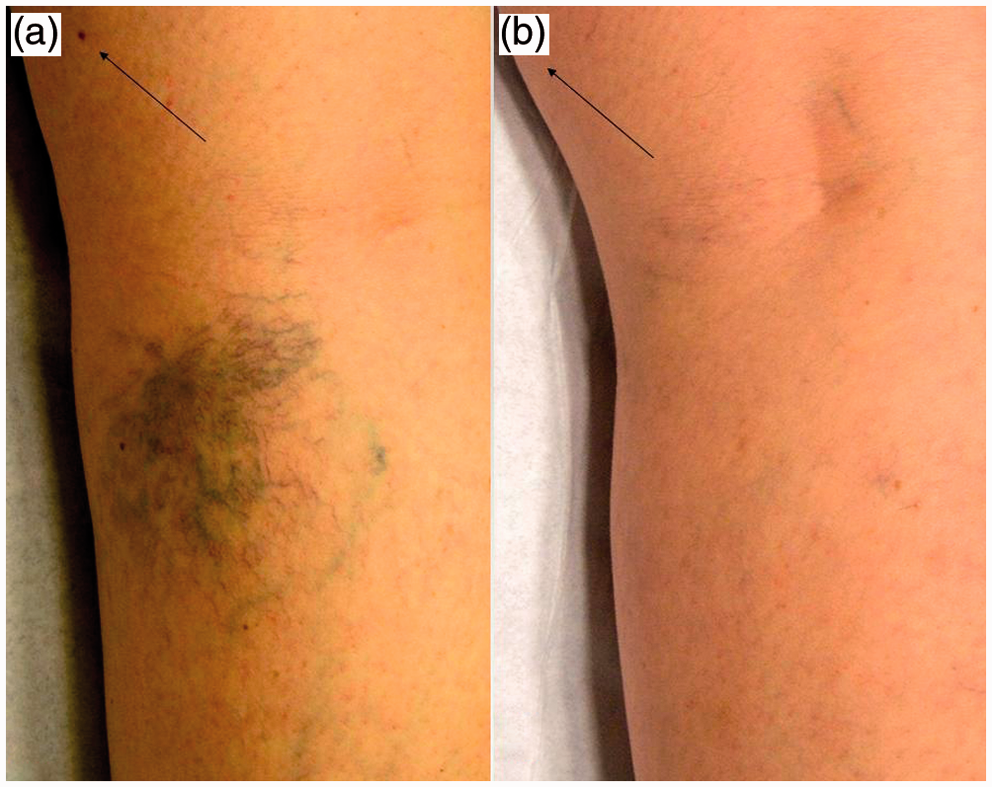
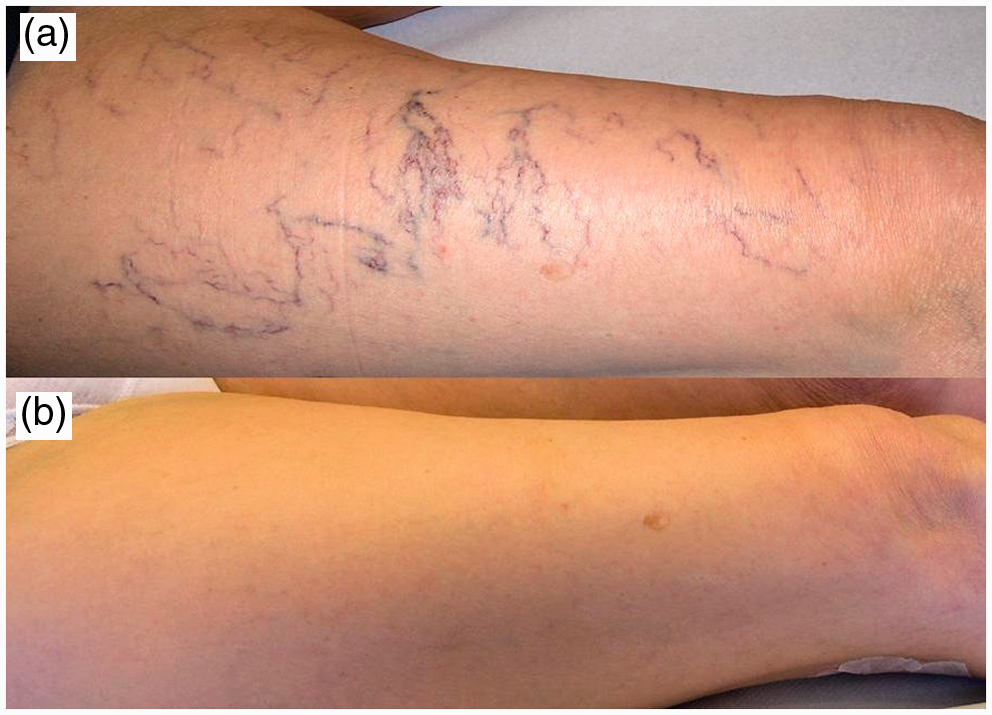
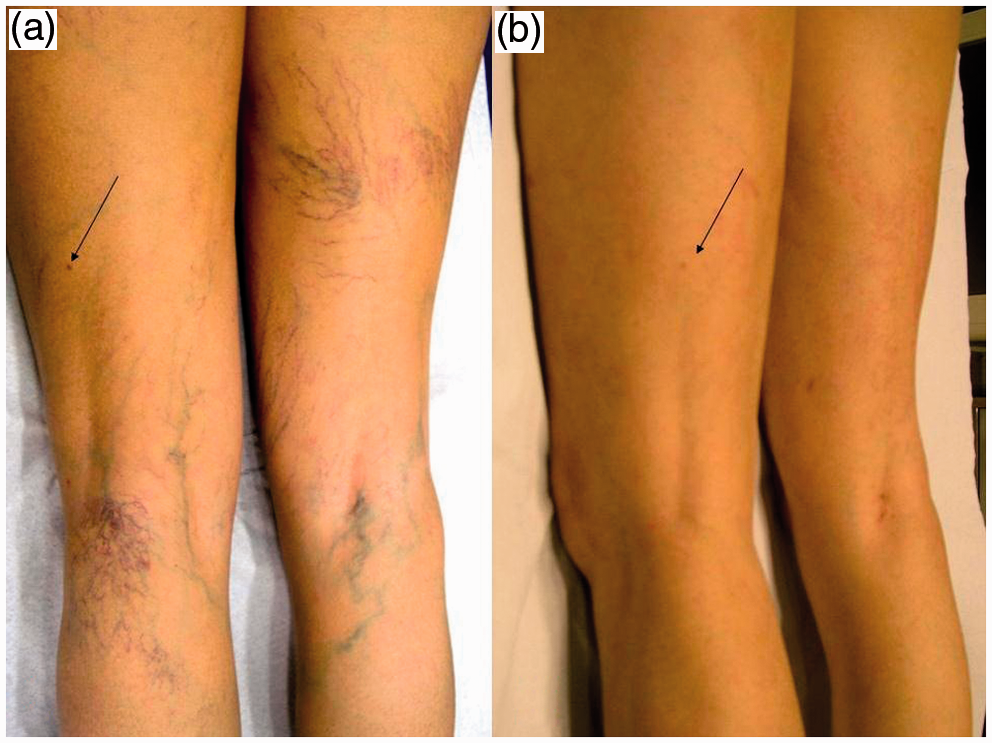
Figures 1 and 2 show the best possible results of the treatment with POL alone at three months, two years and three years. Figures 3 to 9 are photographs of seven different patients treated with POL + Laser. A total clearing of Class I, II and III veins in the areas most affected can be observed. In each of the seven cases, as with the majority of patients, 100% of the visible varicose veins on the limb were cleared, at three months (Figures 3 and 9), and three years (Figures 4 to 8). Varied, illustrative photographs were selected, although the leg position and rotation and/or light and contrast conditions may differ slightly. The position of the varicose veins was marked by arrows against fixed reference points on the skin (freckles) to better display their location.
POL treatment, before (a) and after three months (b). Surface area of the front of the leg showing Class I and Class II veins. The image shows the best possible results of the treatment with POL alone, at three months, with an estimated clearance rate of 2.33 points (46%) in the photographed area. The clearance in the remaining photographs of this leg and for the other patients was significantly poorer. POL treatment, before (a), after two years (b) and after three years (c). Inner side of the right leg showing Class I and II veins, Class I prevalent. At the third year, the clearing rating for the overall surface area of the leg, based on all other photographs, was of 1.66 points for Class I veins and 1.33 points for Class II veins. As an adverse effect, marked hyperpigmentation that persist even after three years are observed in areas treated with higher intensity (ankle). POL + Laser treatment, before (a) and after three months (b). Surface area of the back of the left leg showing Class II and III veins, with prevalence of Class III. Full clearing of lesions is observed, with minimal residual hyperpigmentation. The clearing rating for the overall surface area of the leg, based on all other photographs of this leg, was of five points for each of the three classes of veins. POL + Laser treatment, before (a) and after three years (b). Surface area of the front of the left leg showing Class I and Class II veins, with prevalence of Class II. The full clearing of the lesions can be observed. The clearing rating for the total surface area of the leg, based on all other photographs of this leg, was of five points for each of the three classes of veins. POL + Laser treatment, before (a) and after three years (b). Surface area of the back of the left leg with Class I, II and II veins in a single bunch. Full clearing of the three vein types can be observed. The clearing rating for the overall surface area of the leg, based on all other photographs of this leg, was of five points for each of the three classes of veins. POL + Laser treatment, before (a) and after three years (b). Back of the left knee showing Class III veins. The full clearing of the veins is observed. The clearing rating for the overall surface area of the leg, based on all other photographs, was of five points for each of the three classes of veins. POL + Laser treatment, before (a) and after three years (b). Surface area of the outer right leg showing a high number of Class II veins. Full clearing of lesions is evident. The clearing rating for the overall surface area of the leg, based on all other photographs of this leg, was of five points for Class I and II veins. The presence of Class III veins was not sufficient enough to warrant evaluation. POL + Laser treatment, before (a) and after three years (b). Surface area of the inner right leg showing Class I and II veins, with prevalence of Class II. Full clearing of all veins can be observed. The clearing rating for the overall surface area of the leg, based on all other photographs, was of five points for each of the three classes of veins. POL + Laser treatment, before (a) and after three months (b). Surface area of the back of both legs showing Class I, II and III veins, very widespread. The full clearing of the lesions can be observed. The clearing rating for the total surface area of both legs, based on all other photographs of this patient, was of five points for each of the three classes of veins.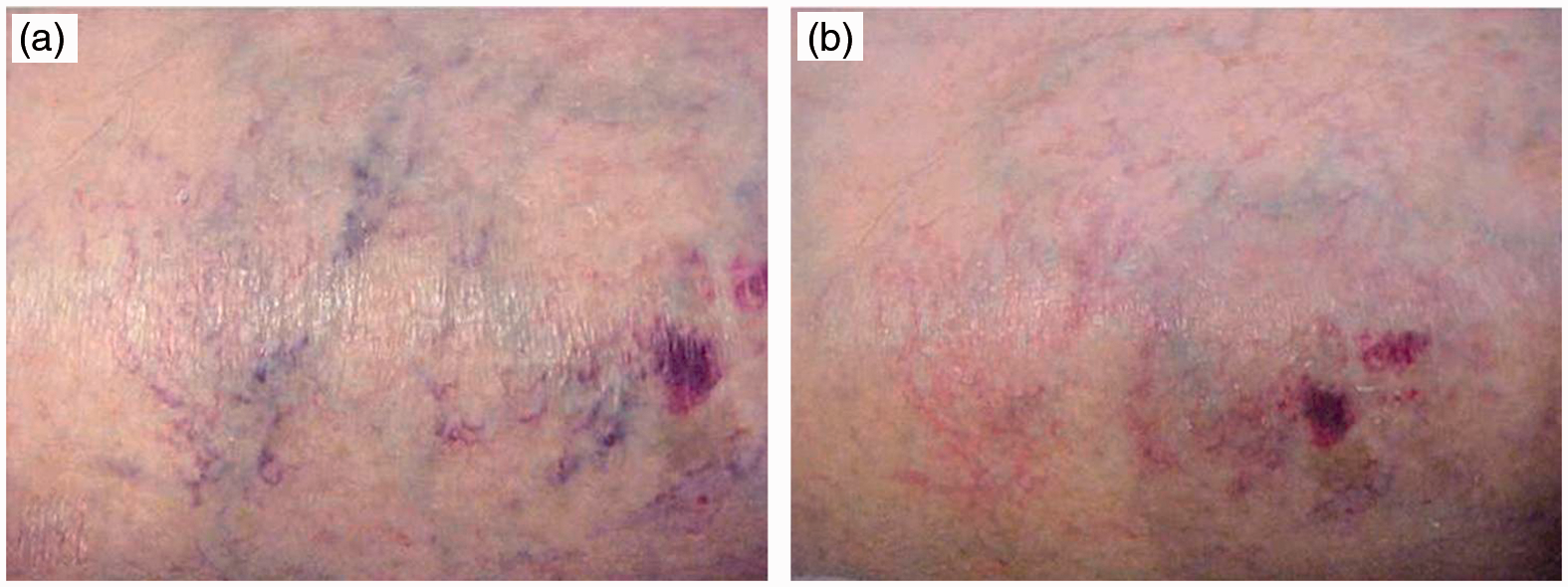



Safety and adverse effects
Both treatments proved to be safe, well tolerated and showed no unexpected side effects. The most frequent adverse effect, in both cases, was a certain degree of pain during the procedure.
In patients treated with POL only (n = 79) hyperpigmentation was observed in 6.3% of cases, and matting in 2.5%, without further findings. After the second and third years, no side effects were recorded. Pain during the procedure was considered to be Light (39.5%), Moderate (34.2%), Severe (20.9%) or Very Severe (5.4%).
Adverse effects during the follow-up of POL + Laser treatment (n = 517).
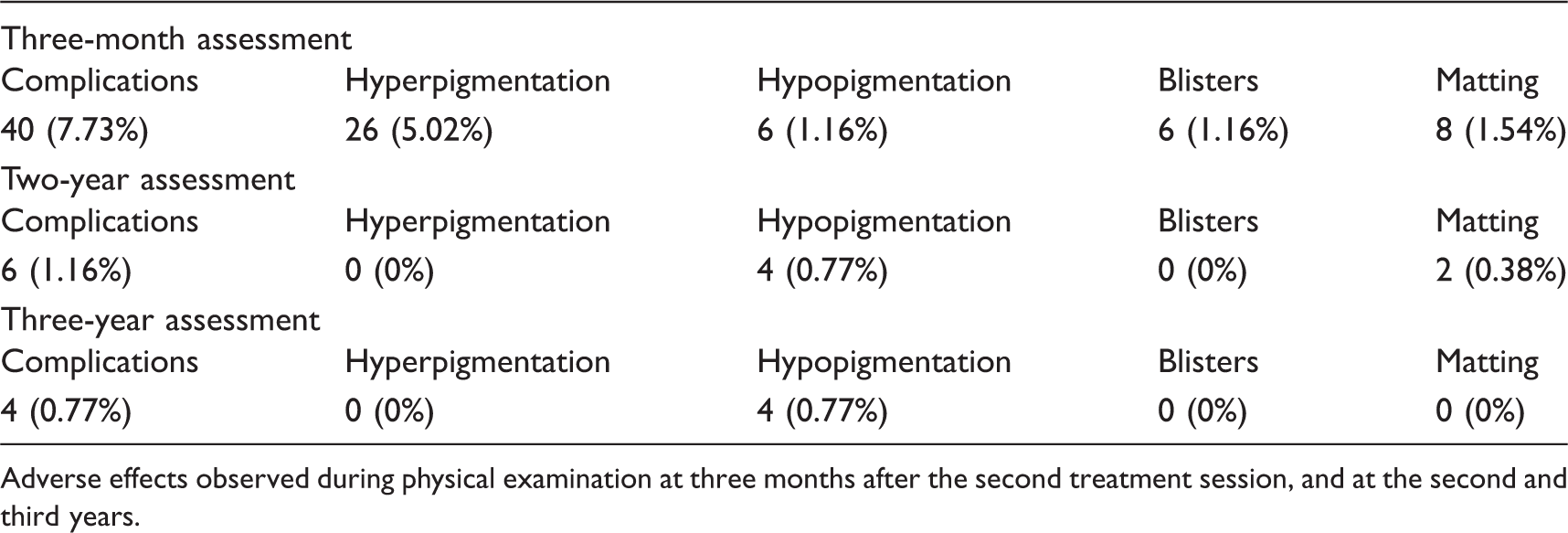
Adverse effects observed during physical examination at three months after the second treatment session, and at the second and third years.
Discussion
The results show a significant difference in efficacy between both treatments, favouring POL + Laser. In our experience, this new procedure offers clearly superior results when compared to any other conventional sclerotherapy technique, and results appear to be permanent on sclerosed vessels.
In patients treated with POL only, a single session is sufficient to treat the full area of the leg with no risk of toxicity. The overall maximum volume of POL injected was 20 mL for both legs, at a concentration of only 0.3%. At such dosages, two sessions are safe but not very effective. In cases of varicose veins covering large areas, sclerotherapy with POL microfoam might achieve similar results to those obtained with the combined method, but would require a much higher number of sessions due to the risk of toxicity at the dosages normally used. Maintenance treatments would also probably be required.1–4
The clearing ratings obtained by the combined method are close to five points at three years. The limitation of the study and the statistics lies in the fact that the clearing ratings do not offer a clear discrimination of the values comprised between four (80% clearing) and five (100% clearing). A rating of five only serves to indicate that the result is closer to 100% than to 80%. Results so close to five are obtained because the three evaluators assigned a rating of five to almost all legs treated with POL + Laser. That is to say the photographs shown here define a subjective result pattern equal to five points, in the opinion of the evaluators. The statistics indicate that the photographs shown do not display the best results, but rather, the results achieved by almost all patients −i.e. the expected results after three years.
A number of authors have researched the effects achieved with the Nd:YAG laser treatment alone for the healing of varicose veins. In all the reports, results refer to the treatment of only selected areas of the lower limbs, and the procedures are not very feasible for treating both legs in a single session.5,6,9,10,16–18 The adverse effects generated and the degree of pain are important limitations.5,6,9,10,16–18 Sadick describes the results obtained after three sessions of Nd:YAG laser for each vein class (I, II and III), using a very similar classification to that applied in this trial. 16 At the third month of the final treatment session, 20% of all vessel types displayed a 50% to 75% improvement. Equal clearing was recorded for blue and red vessels. At the sixth month, 80% of patients displayed a level of clearing greater than 75%, but these results were achieved by using fluences of up to 600 J and pulse lengths of up to 60 ms. 16 Mordon, using fluences of up to 360 J/cm2, with a greater percentage of adverse effects, achieved clearings of up to 98% on 1–2 mm blue leg telangiectasias over a 10-month period. 17 The treatment was limited to 11 patients, only treating an area of 6 × 4 cm. 17 Moreover, many doubts exist as to whether this treatment with Nd:YAG laser is able to produce definite vascular destruction. In histological studies, the presence of recanalized thrombi in some specimens suggests the potential for long-term vessel reappearance. 5 Furthermore, recurrences have been observed at six and 12 months. 6
The mechanisms of interaction between the vein tissues and POL under the influence of laser radiation are not well elucidated.7–9 Ethyl alcohol, one of the substances included in the commercially available POL, has relatively significant absorption peaks at 900 nm, 1000 nm and 1200 nm. At λ = 1064 nm, the absorption may be produced by the ethyl alcohol and the major chromophores such as hemoglobin, especially methemoglobin, and melanin. At λ = 250 nm, the laser radiation may be absorbed by the POL proper. It is possible that nonlinear absorption effects take place in the tissue, such as the absorption of four photons at 1064 nm (which would correspond to a transition at 265 nm), which may be responsible for further effects on the tissue. 7 On the other hand, the effect of the laser light may be expanded if the POL is used as foam, because, then, the light scattering in the tissue becomes more important and the beam absorption becomes larger. The latter effect has been proven through spectroscopy and seems to be important. 8 The fact that the clearings obtained for Class II and Class III veins increase by the third year in comparison with the third month, indicates a probable completive vascular sclerosis.
Pain was tolerated to a higher or lesser extent by all patients without anaesthesia, thanks to the dosage applied, the cooling systems used and a possible anaesthetic-like effect described for POL.19,20 14.5% of women considered the pain to be Very Severe, but no withdrawals occurred as a result of pain. A significant number of women rated the pain as Severe, but tolerated.
Certain discrepancies are observed between the assessments of the evaluators and the satisfaction of the patients, but the results are clearly satisfactory. Such a low rate of withdrawals is due to the good adherence to the trial, with telephone follow-up, and the commitment to offer additional treatment free of charge, if required, at the end of the study. Dissatisfied patients who received therapy with POL only were given a combined treatment session.
The most interesting aspect of this method is that it allows for treatment of the entire surface area of both legs in a single session, with no POL toxicity, and that two sessions allows for removal of almost all of the venulectasias with a diameter of less than 4 mm, at least for three years. It is yet to be determined whether other new venulectasias will form in the long term or whether, on the contrary, this treatment also has a preventive value in regard to the formation of new vessels. In our experience, this is a first choice treatment for a significant number of patients, with numerous and extended varicose veins, who seek fast results, in a few sessions, and as long-lasting as possible.
Footnotes
Acknowledgments
The report given in this study is registered in the academic activities of the Fundación Antoni de Gimbernat, year 2009–2010.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.