
Abstract
Aim
Sclerotherapy is the targeted chemical ablation of varicose veins by intravenous injection of a liquid or foamed sclerosing drug. The treated veins may be intradermal, subcutaneous, and/or transfascial as well as superficial and deep in venous malformations. The aim of this guideline is to give evidence-based recommendations for liquid and foam sclerotherapy.
Methods
This guideline was drafted on behalf of 23 European Phlebological Societies during a Guideline Conference on 7th–10th May 2012 in Mainz. The conference was organized by the German Society of Phlebology.
Results
This guideline focuses on the two sclerosing drugs which are licensed in the majority of the European countries, Polidocanol (POL) and Sodium tetradecyl sulphate (STS). Other sclerosants are not discussed in detail. In this paper the results from recent RCTs in sclerotherapy are reviewed.
Introduction
This guideline was drafted on behalf of 23 European Phlebological Societies during a Guideline Conference on 7th–10th May 2012 in Mainz, organized by the German Society of Phlebology.
These guidelines review the present state of knowledge as reflected in published medical literature. The regulatory situation of sclerosant drugs differs from country to country but this has not been considered in this document.
The recommendations of this guideline are graded according to the American College of Chest Physicians Task Force recommendations on Grading Strength of Recommendations and Quality of Evidence in Clinical Guidelines. 1 This guideline focuses on the two sclerosing drugs which are licensed in the majority of the European countries, Polidocanol (POL) and Sodium tetradecyl sulphate (STS). Other sclerosants are not discussed in detail.
Sclerotherapy is the targeted chemical ablation of varicose veins by intravenous injection of a liquid or foamed sclerosing drug. The sclerosants destroy the venous endothelium and possibly additional regions of the vein wall. After successful sclerotherapy and in the long term, the veins are transformed into a fibrous cord, a process known as sclerosis.2–5
The objectives of sclerotherapy are: ablation of varicose veins, prevention and treatment of complications of chronic venous disorders (CVD), improvement and/or relief of venous symptoms, improvement of quality of life, improvement of venous function, improvement of the aesthetic appearance.
Assessment of the outcome after sclerotherapy
The guideline group recommend clinical outcome evaluation in telangiectasias and reticular varicose veins (C1) and clinical and ultrasound outcome assessment in varicose veins (C2) and venous malformations. (GRADE 1C) to assess the outcome after sclerotherapy.
Clinical outcome includes:
Clinical assessment in everyday practice: varicose vein presence/absence/improvement in the treated area by means of doctor’s and/or patient’s assessment. Evolution of venous ulcers, oedema, haemorrhages, inflammation etc. Symptom assessment. Where appropriate (e.g. during scientific investigations), more sophisticated and standardised symptom-score systems such as the VCSS (Venous Clinical Severity Score) and patient reported outcome scores may be used.
Morphological and hemodynamic outcome include:
Findings included in the duplex-ultrasound investigations after treatment.
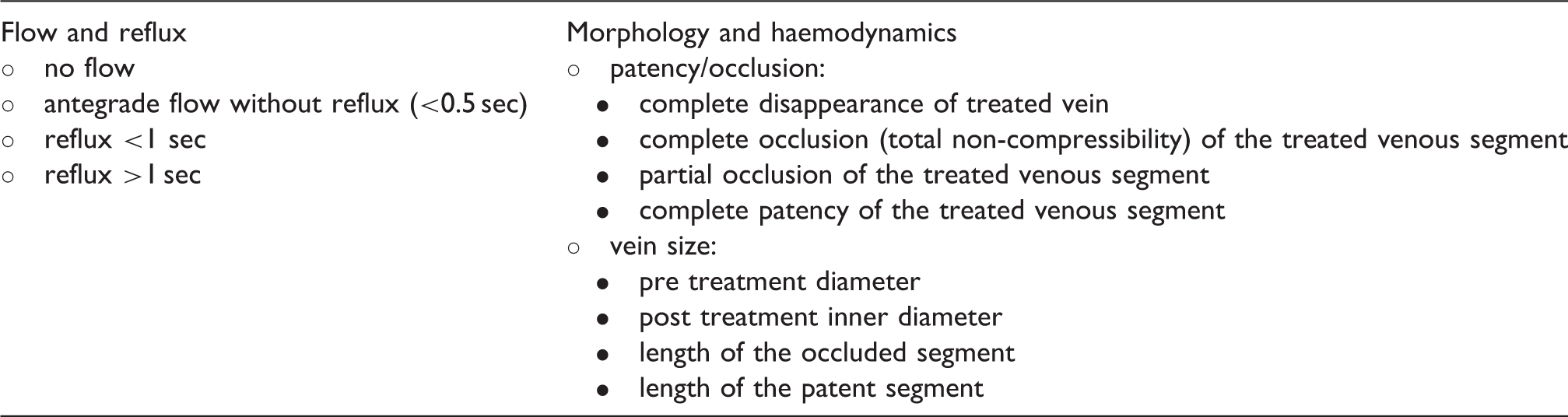
From the clinical point of view a good outcome is the disappearance of the varicose veins and venous symptoms. From the duplex investigation point of view the optimal outcome is the disappearance or total occlusion of the intended vein segments. Clinical improvement of the patient with the occlusion of the treated vein, but with short patent segments with any blood flow may be considered to be a successful outcome, at least in the short (or mid) term.
A wide spectrum of clinical and duplex outcomes is possible after sclerotherapy and these do not necessarily correspond to clinical outcome.
Where applicable, the improvement of venous function can also be demonstrated by pre- and post-treatment functional measurements (e.g. plethysmography, venous pressure measurements).8–10
Efficacy
Based on the available randomised controlled studies sclerotherapy, liquid or foam, is a safe and effective method to treat telangiectasias, reticular varicose veins and subcutaneous varicose veins.4,11–20
The guideline group recommends sclerotherapy as the method of choice for ablation of telangiectasias and reticular varicose veins (C1) (GRADE 1A). Foam sclerotherapy of C1 varicose veins is an alternative method (GRADE 2B).
Liquid sclerotherapy is studied in several big RCTs for ablation of telangiectasias and reticular varicose veins, allowing improvement of more than 90% to be achieved at the end of the treatment.13,14,21–24 Foam sclerotherapy is an alternative method for ablation of telangiectasias and reticular varicose veins, studied only in few small RCTs but with comparable occlusion rates and side effects if a low concentration of more liquid foam is used.11,25
Foam sclerotherapy is recommended over liquid sclerotherapy for the treatment of saphenous veins (GRADE 1A), venous malformations (GRADE 2B) and recurrent varices after previous treatment, accessory saphenous varices, non-saphenous varices and incompetent perforating veins. (GRADE 1C).
Foam sclerotherapy of saphenous varicose veins was studied in several RCTs in comparison to liquid sclerotherapy. In all studies foam sclerotherapy proved to be significantly more effective than liquid sclerotherapy.4,11,12,22,26 However the occlusion rate depends on the diameter of the vein, on the concentration of the sclerosant and on the injected foam volume.22,27
In a recent RCT Shadid and coworkers could demonstrate that large vein diameter and a refluxing distal great saphenous vein at baseline are predictive factors for lower effectivity of foam sclerotherapy. 28
Compared to crossectomy and stripping and to endovenous thermal ablation, foam sclerotherapy shows only a slightly higher mid-term recanalisation/failure rate.29,30 Quality of life and discomfort symptoms improve the same way as after surgery or endovenous thermal treatment. 29 In several studies it could be demonstrated that foam sclerotherapy is effective in the treatment of recurrent varices after previous treatment, accessory saphenous varices, non-saphenous varices and incompetent perforating veins.15,27,31–36
The guideline group does not recommend for mandatory elevation of the leg or compression of the junction for safety reasons during or after treatment. (GRADE 2C). Ceulen could demonstrate that there is no evidence for an improvement of the occlusion rate or reduction of side effects by leg elevation or compression of the junction with the duplex probe. 37
Foam sclerotherapy of incompetent saphenous veins with long catheters is also effective.38–44
Sclerotherapy of varices in the region of venous ulcers improves the healing rate.45–48 (GRADE 1B). Recently catheter-directed foam sclerotherapy for chronic venous leg ulcers showed a good healing rate in a prospective case-control study. 49
Re-treatment by sclerosing partially recanalised vein segments during the follow-up is recommended (GRADE 1B). Re-treatment by sclerosing partially recanalised vein segments during the follow-up improves the mid-term result as could be shown by Blaise and Chapman-Smith.50,51
Foam sclerotherapy is also more effective than liquid sclerotherapy in the treatment of venous malformations (GRADE 1B). This could be demonstrated by Yamaki and Blaise.52–54
Several authors could demonstrate that compression treatment with medical compression stockings or bandages improves the result of sclerotherapy for spider veins.24,55–57 In two small studies the incidence of pigmentation decreased.55,57 Evidence of efficacy for compression after sclerotherapy of saphenous veins is still lacking. Hamel-Desnos could not demonstrate a significant improvement of results and side effects by wearing 15–20 mmHg compression stockings compared to no compression after foam sclerotherapy of GSV. 58 Nevertheless compression may have some influence on efficacy, as the need for an additional sclerosing session seems to be inversely proportional to the pressure exerted by 3 different classes of MCS worn for 3 weeks after sclerotherapy 59 and as selective extrinsic compression may reduce recurrence. 60 Local eccentric compression significantly increases the local pressure in the injection area and may improve the efficacy of sclerotherapy. 61
Footnotes
Conflict of interest
All the authors have no conflict of interest and nothing to disclose.
Funding
This work was sponsored by an unrestricted grant from the German Society of Phlebology.