
Abstract
Objectives: To assess the clinical safety of a new short-stretch 2-layer compression system (3Mtm Cobantm 2 Lite) in patients with peripheral arterial occlusive disease (PAOD). This system combines a low resting pressure with a high working pressure.
Methods: A pilot study was performed in 15 subjects with moderate PAOD, i.e. an ABPI of 0.5-0.8. Co-existing chronic venous insufficiency or leg ulcer was not mandatory. All subjects received the compression system which was reapplied at each study visit (days 1, 2, 3, 4, 7, 10, 14). The safety parameters were: sub-bandage pressure immediately after application, pressure-related skin damage, hypoxia-related pain, and adverse events. A product comfort questionnaire was completed at the last visit.
Results: The average sub-bandage pressure of 30 mmHg defined by the protocol was achieved. No pressure-related skin damage or hypoxia-related pain was found. The reported adverse device effects were as expected for compression therapies, including dry skin and pruritus. The product comfort questionnaire completed by the subjects showed a good tolerability profile.
Conclusion: The short-stretch 2-layer compression system (3Mtm Cobantm 2 Lite) was safe and well tolerated in subjects with moderate PAOD.
Keywords
Introduction
In Western societies, the prevalence of florid or resolved leg ulcer is estimated around 0.7 %. 1
The most frequent aetiologies include venous disease followed by arterial insufficiency, diabetes and rheumatoid arthritis. Chronic venous insufficiency (CVI) is found in about one third of the Western population and its prevalence increases with age. 1 As elderly people often suffer from peripheral arterial occlusive disease (PAOD), a coincidence of both peripheral vascular diseases is a common finding. 3
Compression therapy is the principal mode of treatment for leg ulcer. Numerous benefits of this therapy have been described, including decrease in oedema, acceleration of venous backflow, decrease in venous volume, reduction in venous reflux, and lymph-drainage. 4 Hence, the use of compression therapy is an agreed standard in leg ulcer caused by CVI.
On the other hand, the use of compression therapy in patients with PAOD is still debated in the scientific community, as the application of external compression is assumed to potentially reduce the local perfusion of the leg. To avoid the risk of under-perfusion, a variety of treatment recommendations were offered which mainly referred to the applied level of compression.5,6,7,8,9 In recent studies in patients with moderate PAOD, indicated by an Ankle Brachial Pressure Index (ABPI) between 0.5 and 0.8, an average pressure of 30 to 32 mmHg measured at the B1 location was reported to be safe and well tolerated.10,11
Regarding the effectiveness of compression therapy, it was shown in a recent clinical study that the stiffness of the compression system plays a central role. The ejection volume and ejection fraction from the peripheral venous system following muscle activity were much higher if inelastic systems were used. 12 The authors assumed that inelastic compression systems lead to pressure peaks during walking, comparable to a pneumatic pressure pump. Moreover, the muscle systoles during walking with an inelastic compression system in situ may block venous reflux intermittently and thus imitate competent venous valves.
To differentiate between elastic and inelastic systems, the static stiffness index (SSI) is used. The SSI is determined by the difference in pressure under the compression system when comparing supine position to standing position. A difference of more than 10 mmHg classifies a compression system as stiff bandage. 13
Because of a significant correlation between the quotient working pressure to resting pressure, compression bandages with a higher quotient improve venous drainage best. 14
In the present article, we are reporting about a pilot study that was conducted with a new inelastic, short-stretch system, 3M™ Coban™ Lite Compression System (hereafter Coban 2 Lite), which was developed for the use in leg ulcer and concomitant PAOD. This safety trial was performed to gain data about the tolerance with regard to clinical symptoms and acral arterial perfusion in patients with impaired peripheral arterial blood supply. The new bandage provides a thin, conforming inelastic sleeve, which combines a reduced resting pressure with the required stiffness in standing position. This combination was expected to be associated with a high rate of tolerability, which is mainly dependent on the reduced resting pressure. 15
Methods
This open-label, single-centre, prospective pilot study was conducted at the UNIVERSITY HOSPITAL in Greifswald, Germany. Prior to study start, nurses at the study site in Greifswald were trained to apply compression, providing sub-bandage pressure values around 30 mmHg at the B1 position.
The protocol was approved by the Ethics Committee of the Ernst-Moritz-Arndt-University. Study participants granted written informed consent prior to inclusion into the study.
Subjects were included to the study if they were 18 years or older, suffering from PAOD with an ABPI at the investigational leg between 0.5 and 0.8, able to walk and being co-operative, willing to give written informed consent prior to study entry and willing to comply with the study protocol.
Exclusion criteria were: general conditions which in the opinion of the investigator did not allow for compression therapy, paralysis of the study leg, mood altering substances if started or significantly changed within two weeks prior to enrolment, significant unstable coagulopathy, participation in any other prospective clinical study that could potentially interfere with this study, and known allergies against Coban 2 Lite.
The study started with visit 0 (screening and treatment initiation) on day 0 and ended with visit 7 on day 14.
All subjects received treatment with Coban 2 Lite which includes a comfort layer bandage and a compression layer bandage. The protocol contained detailed instructions on how to apply the 2 bandages. For the compression layer, the instructions asked for ‘full stretch’ to be reached by maintaining consistent full stretch throughout the wrapping process and by winding with 50% overlap. Wounds were to be covered with a primary dressing before applying the comfort layer. For precautions, the protocol specified that the compression system should be changed when the wrap was not conforming to the leg circumference. Subjects were advised to notify the study site if they experienced severe pain, numbness, tingling and swelling or blue/pale colour of toes.
The system stayed in place for 1 up to 4 days according to scheduled study visits. The system was reapplied by the study personnel at 6 interval treatment visits (days 1, 2, 3, 4, 7, and 10). On study day 14, the study was finished with an end of study visit. At each clinical visit safety assessments were performed. Parameters to evaluate safety included: 1. clinical signs of early skin damage, eventually substantiated by measuring the transepidermal water loss (TEWL); 2. photodocumentation in case of skin damage; 3. documentation of painful sensations as potential signs of tissue under perfusion; 4. Sub-bandage pressure measurements and 5. collection of adverse events. In addition volume evaluations of the lower legs were performed at the first and last study visit and a product comfort questionnaire was completed at the end of the study.
TEWL as an early symptom of skin damage was to be measured with the Tewameter (Courage & Khazaka, Cologne, Germany) only if skin damage was clinically visible. The TEWL was to serve as a diagnostic tool to substantiate these potential early clinical signs. Typically, TEWL is increased in areas of irritated skin. Digital photodocumentation was planned in case of clinically visible skin damage.
Immediately after each bandage application the sub-bandage pressure was measured at B1 which is the proximal end of the tendon of the calf muscle where the muscle interlocks with the Achilles tendon 13 with the PicoPress Compression Measurement System (Microlab Elettronica, Ponte S Nicolò, Italy).
The circumferences and the volume of the leg were determined by Image 3D (Bauerfeind Phlebologie, Zeulenroda, Germany).
The statistical method was defined as follows: Aggregate data were collected using an Access database. This included all measurements and the product comfort questionnaire with 8 criteria. The product comfort questionnaire data was evaluated using a frequency table. Statistical calculations and graphic generation were done with Excel using Access queries. Exploratory testing for difference was done at a 5% level of significance. All adverse events were summarised according to severity and relation to study.
Results
15 subjects with PAOD were included in the study of which 7 were female and 8 were male. At the time of inclusion into the study, women had a mean age of 74.1 ± 10.1 (average ± standard deviation) years while men were 71.4 ± 10.5 years old.
6 of the 15 enrolled subjects suffered from coincident chronic venous insufficiency. Among these 6 subjects, 2 were female and 4 were male.
3 subjects had an active leg ulcer at the study start. However, this study with a maximum observation period of 14 days was not expected to provide relevant information about the clinical course of these ulcers.
The ABPI was ≥0.5 and <0.6 in 5 subjects, ≥0.6 and <0.7 in 4 subjects and ≥0.7 and ≤0.81 in 6 subjects.
Immediately after the bandage application, the average sub-bandage pressure in standing position at the B1 location varied between 31.20 ± 7.85 mmHg at visit 0 and 29.54 ± 6.96 mmHg at visit 6. Figure 1 shows the average sub-bandage pressure by subject. The figure shows the sub-bandage pressure immediately after application and in the standing position. With reference to literature, a sub-bandage pressure of 30 mmHg was intended. Referring to studies that revealed a 10 mmHg difference between two applications by well trained and experienced nurses, the pressure results were expected to range from 20 mmHg to 40 mmHg. The actual results were in line with these conditions. Sub-bandage pressure values of 43 mmHg and more in the standing position were found in 4 subjects. None of them reported adverse events that started during or shortly after this bandage was in place.
Sub-bandage Pressure in Standing Position Immediately after Application, Average and Standard Deviation by Subject.
The leg volume assessment with the Image 3D technique revealed an average volume reduction of 7.3 ± 7.9% (p = 0.03) at the end of the study. Only one subject had an increase of volume of 0.7% in the lower leg.
All 15 subjects enrolled were included in the safety evaluation: 12 of 15 subjects (80%) reported adverse events. In total, 22 episodes of adverse events were reported from these 12 subjects. One adverse event, i.e. cardiac arrhythmia, was classified as serious because it led to hospitalisation. This event was assessed as not related to the study device, i.e. the compression system. All other adverse events were classified as probably or possibly related to the device.
Adverse Events.
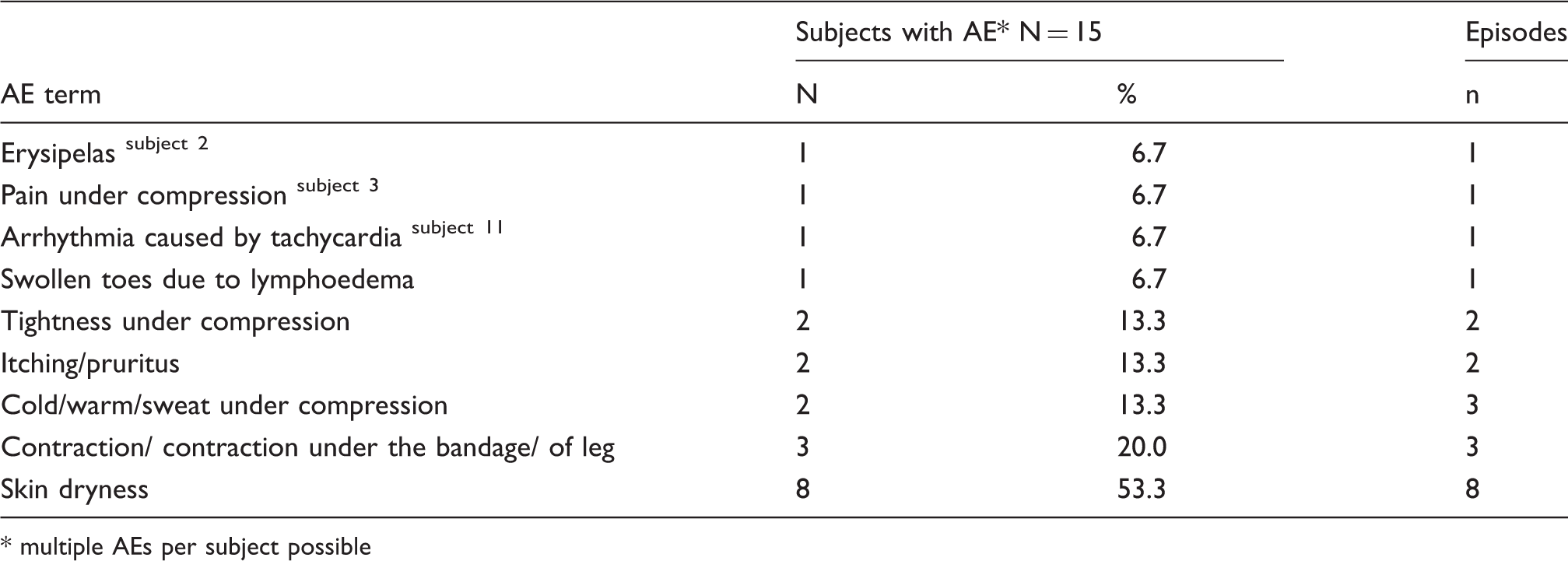
* multiple AEs per subject possible
Subject no. 2 had 6 episodes of leg erysipelas in his medical history. Over the conduct of the study a further episode developed on the investigational leg. The event was moderate in intensity and rated as possibly related to the compression system. The subject was withdrawn from the study and the event resolved 5 days after its onset.
Subject no. 3 completed visit no. 5 on study day 7 without complication. Two days later he was submitted to an angiology department for elective angiography at the study leg. During this hospital stay, moderate pain was reported which started after the bandage had been removed and stopped on the same day. For reasons of safety and completeness, the event was reported as mild in intensity and possibly related to study procedures. The study was discontinued in this subject. However, according to the study staff this event was most likely related to the invasive diagnostic procedure.
Subject no. 11 developed severe cardiac arrhythmia and tachycardia one day after study visit 6 and was hospitalised for further diagnostic and therapeutic interventions. Due to the need for hospitalisation, this event had to be classified as serious. The subject was withdrawn from the study. The event was assessed as not related to the compression system.
In summary, the reasons for premature withdrawal did not indicate any specific risk caused by the compression system.
All study subjects were closely monitored for any skin alterations over the conduct of this study. No clinical signs of any skin damage occurred under Coban 2 Lite therapy in any of the subjects. Hence, TEWL and photodocumentation did not become necessary.
No study subject reported painful sensations as possible signs of underperfusion or hypoxia.
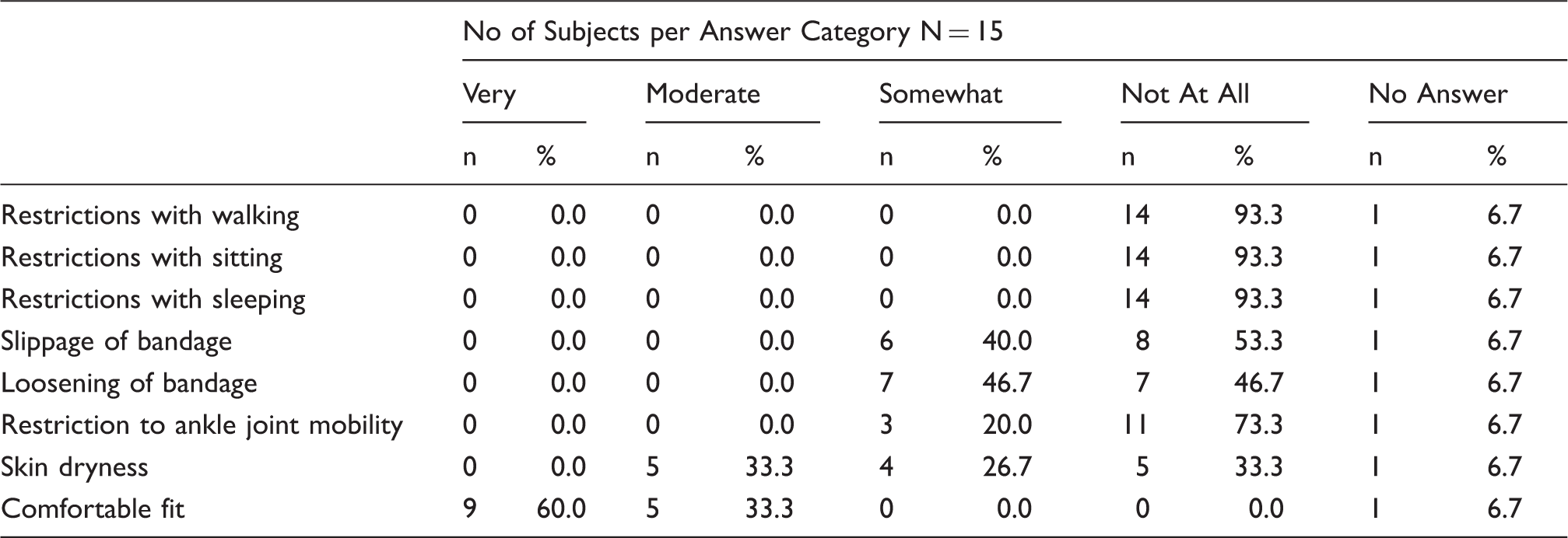
Product Comfort Questionnaire.
Discussion
The most frequent aetiology of leg ulcer is chronic venous insufficiency. Mixed arterio-venous disease is present in about 20% of patients with ulcerated legs. 10
The treatment of leg ulcer with compression systems is a widely accepted standard. However, for patients suffering from leg ulcer and PAOD, the standard compression systems are regarded as not suitable because of their potential to further decrease skin perfusion. This potential may result mainly from a high resting pressure. 15
The compression system investigated in this pilot study, Coban 2 Lite, was particularly adapted to the needs of patients with leg ulcer and PAOD, because it combines low resting pressure with an effective working pressure. The system is a short-stretch bandaging system consisting of two layers: a comfort layer and a compression layer to be applied with full stretch giving a thin, inelastic sleeve with an anatomical fit.
15 subjects with moderate peripheral arterial disease, defined as an ABPI between 0.5 and 0.8, wore the Coban 2 Lite compression system for a maximum of 14 days with 6 visits to renew the bandages after 1 to 4 days. 3 of these subjects had an active leg ulcer at study start.
An average sub-bandage pressure of approximately 30 mmHg in the standing position was established by measuring at the B1 location with an electronic compression measurement system.
The study comprised an observation period of 14 days which was regarded as sufficient for potential clinical signs of compression related arterial under perfusion.
The absence of any pressure related skin damage in subjects with reduced arterial perfusion was the most relevant finding of this clinical study. Likewise, hypoxia-related pain was not reported which also indicated that the system was safe to use in patients with moderate PAOD. These data confirm previous reports where patients with moderate PAOD were safely treated with reduced resting pressures of 32 mmHg in average in standing position). 11
Regarding the active leg ulcers that were present at study start, the observation period of 14 days was judged as not being sufficient to study their clinical course. However, the leg volume measured with the image 3D technique decreased in all but one subjects over the course of the study.
The list of actually observed adverse device effects, as dry skin or local skin constrictions, mainly contained symptoms, expected during any compression therapy regardless whether applied to patients with or without PAOD. However although most subjects used compression therapy the first time, the subject rated comfort questionnaires revealed a high grade of tolerance of this new product.
In summary, the compression system Coban 2 Lite was safe and well tolerated by patients with moderate peripheral arterial occlusive disease.
Footnotes
Author contributions
Data collection and statistical analysis was conducted by Andrea Ladwig and Hermann Haase
Conflict of interest
MJ, AL, HH and LS have no conflicts of interest to declare. JB and JS are employed by 3M Deutschland GmbH.
Funding
This study was sponsored with an educational gift by 3M Deutschland GmbH to the Ernst-Moritz-Arndt-University in Greifswald, Germany.