
Abstract
Objective
Endovenous techniques are, at present, the recommended choice for truncal vein treatment. However, the thermal techniques require tumescent anaesthesia, which can be uncomfortable during administration. Non-tumescent, non-thermal techniques would, therefore, have potential benefits. This randomised controlled trial is being carried out to compare the degree of pain that patients experience while receiving mechanochemical ablation or radiofrequency ablation. The early results of this randomised controlled trial are reported here.
Methods
Patients attending for the treatment of primary varicose veins were randomised to receive mechanochemical ablation (ClariVein®) or radiofrequency ablation (Covidien® Venefit™). The most symptomatic limb was randomised. The primary outcome measure was intra-procedural pain using a validated visual analogue scale. The secondary outcome measures were change in quality of life and clinical scores, time to return to normal activities and work as well as the occlusion rate.
Results
One-hundred and nineteen patients have been randomised (60 in the mechanochemical ablation group). Baseline characteristics were similar. Maximum pain score was significantly lower in the mechanochemical ablation group (19.3 mm, standard deviation ±19 mm) compared to the radiofrequency ablation group (34.5 mm ± 23 mm; p < 0.001). Average pain score was also significantly lower in the mechanochemical ablation group (13.4 mm ± 16 mm) compared to the radiofrequency ablation group (24.4 mm ± 18 mm; p = 0.001). Sixty-six percent attended follow-up at one month, and the complete or proximal occlusion rates were 92% for both groups. At one month, the clinical and quality of life scores for both groups had similar improvements.
Conclusion
Early results show that the mechanochemical ablation is less painful than the radiofrequency ablation procedure. Clinical and quality of life scores were similarly improved at one month. The long-term data including occlusion rates at six months and quality of life scores are being collected.
Introduction
Varicose veins are a common problem, affecting approximately one-third of the United Kingdom population. 1 Both the National Institute of Health and Clinical Excellence and the Society for Vascular Surgery/American Venous Forum recommend endovenous thermal ablation as first-line treatment for truncal vein incompetence.1,2 However, thermal ablation requires the use of tumescent anaesthesia and is associated with intra-procedural pain and discomfort as well as carrying the risk of skin and nerve damage.3,4 This has, therefore, led to the development of non-thermal, non-tumescent ablative techniques such as mechanochemical ablation (MOCA) and cyanoacrylate glue. 4
Recent studies have shown that Covidien® Venefit™ (Covidien, San Jose, CA, USA) radiofrequency ablation (RFA) and ClariVein® (Vascular Insights LLC., Quincy, MA, USA) MOCA have similar occlusion rates at one year.4,5 Less is known about the comparative intra-procedural patient experiences of pain and return to function.
The Venefit™ versus ClariVein® for Varicose Veins trial study aims to assess this question, and the early intra-operative results of this randomised controlled trial comparing thermal ablation (RFA) with non-thermal, non-tumescent ablation (MOCA) as well as the one-month follow-up data are reported here.
Methods
Recruitment
Patients referred for the treatment of symptomatic varicose veins to the Vascular Department of Charing Cross NHS Hospital (Imperial College NHS Trust) and Northwick Park NHS Hospital (North West London Hospitals NHS Trust) in London were studied. Patients older than 18 years with primary great saphenous vein (GSV) or small saphenous vein (SSV) incompetence were identified at their outpatient visit by a member of the clinical team and were added to the waiting list for endovenous ablation and given information about the trial.
Exclusion criteria.
ABPI: ankle brachial pressure index.
Consenting patients were then subsequently randomised to either MOCA (group A) or RFA (group B) truncal ablation using an online computerised service (Sealed Envelope, London, UK). In patients receiving treatment to both lower limbs, the more symptomatic side was included in the study.
No procedural blinding was possible due to the difference in techniques; however, the investigator at follow-up was blinded as to treatment group.
Clinical severity scoring
At recruitment, all the patients were evaluated by a vascular specialist. Their Venous Clinical Severity Score (VCSS), Venous Disability Score (VDS) and Clinical-Etiological-Anatomical and Pathophysiological (CEAP) classification were assessed. This was repeated at the one-month follow-up.
Quality of life scoring
Patients were also asked to complete the Aberdeen Varicose Vein Questionnaire (AVVQ), a validated disease-specific quality of life (QoL) questionnaire for varicose veins, and the EQ-5D-3 L and EuroQol's visual analogue scale (EQ-VAS) (EuroQol Group), a generic QoL questionnaire, prior to their procedure. They were asked to complete these questionnaires again when they attended follow-up at one month.
Interventions
All varicose vein procedures were carried out under ultrasound guidance and local anaesthetic by vascular surgeons familiar with and approved in both ablative methods. For both techniques, the GSV or SSV was cannulated under ultrasound guidance after injection of local anaesthetic (1% Lidocaine). The catheter tip was positioned 2 cm distal to the sapheno-femoral junction or sapheno-popliteal junction. Cannulation was performed at the most distal point of reflux where cannulation was possible.
The method used for RFA has been described before. 6 MOCA was performed as previously described by van Eekeren et al. 3 except that 2% sodium tetradecyl sulphate (STS) (Fibrovein™, STD Pharmaceutical Products Ltd., Hereford, UK) (made by mixing equal volumes of 1% STS and 3% STS) was used instead of polidocanol. The total volume of liquid sclerosant used was calculated as per the manufacturer’s guidance.
Stockings were worn for two weeks post-procedure, and patients were advised to mobilise for at least 1 h every day and to return to their work and normal activities when they felt able to.
Pain scoring
Immediately after patients have undergone their endovenous procedure, but before concurrent varicosity treatment with phlebectomy was performed (if indicated), patients were asked to record their maximum and average pain score during the procedure using a validated Visual Analogue Scale (VAS) by placing a mark on a 100-mm VAS.3,6 The pain score was also recorded as a number on a scale of 0 to 10. 7
Time to return to normal activities
Before being discharged on the day of their procedure, patients were given a diary to record when they resumed normal activities and, if in employment, went back to work. These were returned at the one-month appointment. No routine discharge medication was provided, but patients were allowed to take non-prescription analgesia as required.
Outcome measured
The primary outcome of the study is the degree of pain during endovenous ablation using a validated patient reported VAS. The secondary outcomes are improvement in the AVVQ scores, EQ-5D-3 L, VCSS, VDS and CEAP at one month and six months and time taken to return to normal activities and work. The occlusion rate at one month was also determined by carrying out a venous Duplex scan. The four possible findings are complete occlusion of the saphenous vein, proximal occlusion, distal occlusion and open.
Power calculations
Power calculations were based on the primary outcome of pain during the procedure. Detection of a 20-mm difference in maximum pain score with a standard deviation (SD) of pain score of 20 mm was considered a significant difference. The minimum target size was calculated to be 94 patients (47 per group) at 90% power and 5% significance. Allowing for loss to follow-up or protocol violations, an overall target recruitment of 170 legs (85 per group) was estimated.
Study registration and ethical arrangements
This study was registered on the Current Controlled Trials website (http://www.controlled-trials.com) (ISRCTN06552809).
The ethical approval for the study was obtained from the National Research Ethics Service Committee London – Chelsea (REC Ref.: 12/LO/0570).
Statistical analysis
All statistical analysis was conducted using the Statistical Package for the Social Sciences (version 21, IBM, Armonk, USA). Significant differences between means were calculated using Student’s t test. A p value of less than 0.05 was considered to be significant.
Results
Early results of this study show that 119 legs (117 patients) have been randomised, with 60 randomised to receive MOCA (group A) and 59 to RFA (group B).
Baseline characteristics
Baseline characteristics and details of veins treated.

MOCA: mechanochemical ablation; RFA: radiofrequency ablation; GSV: great saphenous vein; SSV: small saphenous vein; SD: standard deviation.
Clinical and quality of life scores at baseline and at one-month follow-up.
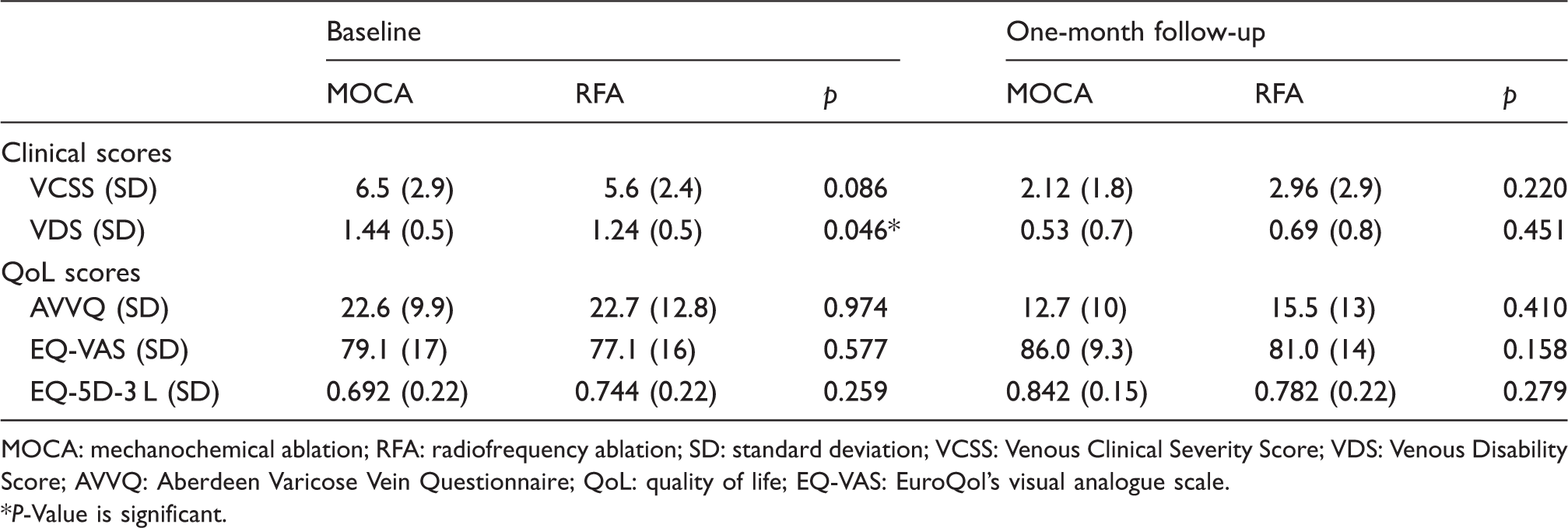
MOCA: mechanochemical ablation; RFA: radiofrequency ablation; SD: standard deviation; VCSS: Venous Clinical Severity Score; VDS: Venous Disability Score; AVVQ: Aberdeen Varicose Vein Questionnaire; QoL: quality of life; EQ-VAS: EuroQol's visual analogue scale. *P-Value is significant.
Intervention
The left leg was treated in 48% of cases and the GSV ablated in 86% of procedures (Table 2). Concurrent phlebectomies were carried out in 68% of patients in the MOCA group and 77% of those in the RFA group (p = 0.30).
Pain score
The mean maximum pain score using the VAS during endovenous ablation was 19.3 mm ( ± 19) for the MOCA group compared to 34.5 mm ( ± 23) for the RFA group (p < 0.001). The corresponding mean maximum pain scores were 2.6 ( ± 2.2) for the MOCA compared to 4.4 ( ± 2.7) for the RFA group (p = 0.001).
The average pain distance was 13.4 mm ( ± 16) for the MOCA group and 24.4 mm ( ± 18) for the RFA group (p = 0.001), while the average pain score was 1.9 ( ± 2.0) and 3.2 ( ± 2.2) (p = 0.002).
The pain score in MOCA included the time from cannulation to vein ablation, while in RFA, it involved the time from cannulation, including infiltration of tumescence to completion of the ablation.
Time to return to normal activities
The mean time to return to normal activities was 3.5 ( ± 3.1) days for group MOCA compared to 4.8 ( ± 4.3) days for RFA (p = 0.235).
The mean time to return to work was 5.3 ( ± 8.7) days for MOCA and 4.9 ( ± 3.6) days for the RFA group (p = 0.887).
Clinical and QoL scores at one month
Both groups showed improvement at one month in all clinical and QoL measures, with no significant differences between the two groups (Table 3).
Occlusion rate
Occlusion rates (%) at one-month follow-up.
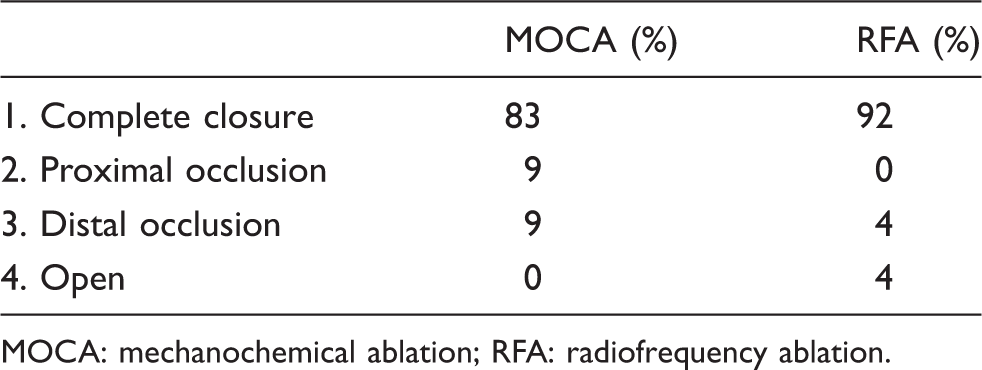
MOCA: mechanochemical ablation; RFA: radiofrequency ablation.
Complications
In the MOCA group, there was no recorded incidence of deep (DVT) or superficial vein thrombosis (SVT) while, in the RFA group, two patients developed thrombophlebitis (3.4%) and one patient developed a non-occlusive popliteal vein DVT (1.7%). The DVT occurred in a patient treated for GSV incompetence only (with no concurrent phlebectomy) and was an extension along the gastrocnemius vein to the popliteal vein.
Discussion
With the efficiency of all the current endovenous techniques, 4 intra-procedural issues with treatment such as pain and patient satisfaction become more important. This is the first randomised controlled study comparing intra-procedural pain scores in patients receiving MOCA or RFA. The early results from this study with one-month follow-up show that intra-procedural pain was significantly lower in patients undergoing MOCA compared to RFA. This difference may be explained by the additional injections required for tumescent infiltration. Patients from the MOCA group also showed a trend of earlier return to their normal activities, but this was not statistically significant. Importantly, early clinical, radiological and QoL outcomes were equivalent between RFA and MOCA.
In a non-randomised observational study of 68 patients, van Eekeren et al. 3 found that post-procedural pain during the first 14 days was significantly lower in the MOCA group compared to patients having RFA (mean VAS over 14 days was 4.8 ± 9.7 mm in MOCA group versus 18.6 ± 17.0 mm; p < 0.001). The difference in pain scores is probably explained by the different methods used to ablate the incompetent veins. The RFA technique (thermal treatment) involves treatment by heat as well as tumescent anaesthesia infiltration to prevent thermal damage to surrounding tissues, both of which can be uncomfortable. 3 In that study, MOCA was also shown to be associated with an earlier return to normal activities. 3
The overall occlusion rates in this small cohort of patients are similar to that seen in other studies,1–6,8 and longer term follow-up is required before any definitive comments can be made on superiority of techniques with respect to patency.
These early results show a decreased pain profile for MOCA compared to RFA and flag up the potential benefits of non-thermal, non-tumescent techniques compared to thermal treatment.
Footnotes
Funding
The research was funded by a research grant from ClariVein® manufacturer, Vascular Insights LLC., and a research grant from the Graham-Dixon Charitable Trust. The research was also supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Imperial College Healthcare NHS Trust and Imperial College London. The views expressed are those of the authors and not necessarily those of the NHS, NIHR or the Department of Health.
Conflict of interest
All study data collection, treatment and analysis were performed independently.