
Abstract
Background
The “Adductor canal syndrome” has been described as an unusual cause of acute arterial occlusion inside the Hunter’s canal in young sportsmen. It may also produce a compressive neuropathy of the saphenous nerve. To our knowledge, femoral vein compression in the canal has never been reported.
Objective
To describe the anatomy, to propose a physiology of this canal, and to show that the femoral vein is much more exposed than the artery to compression inside this adductor hiatus, particularly at the outlet.
Material and methods
The whole adductor canal was exposed in 100 limbs for anatomical study following latex injection. A series of 200 phlebographies and 100 CT venograms were also analyzed.
Results
Anatomically, we found a musculotendinous band called the “vastoadductor membrane,” which jointed the adductor tendon to the vastus medialis in all the cases. The femoral vein, located more posteriorly, was frequently narrowed at this level. This band can create a notch with a venous stenosis at the outlet of the Hunter’s canal, usually located 12–14 cm above the femoral condyle. Two femoral valves constitute the landmark of the canal on the venograms: the lower is just below the outlet, 9 cm above the condyle. The second valve is 3 cm higher inside the canal.
Functionally, the cadaveric simulations showed that the contraction of the adductor longus closes the hiatus, while the adductor magnus opens it. Our hypothesis is that Hunter’s canal prevents femoropopliteal axis reflux by synchronizing with calf pump ejection during ambulation.
Conclusion
Compression of the femoral vein inside the adductor’s canal is an underestimated and misdiagnosed cause of postural stenosis of the femoral vein. Ultrasound investigation of both limbs in patients with chronic venous disease (CVD) should be systematically carried out at this precise level in order to prevent future occlusion and onset of acute deep vein thrombosis.
Keywords
Introduction
History of Hunter’s canal
John Hunter (1728–1793) was a Scottish surgeon from Glasgow. 1 In 1785, he created a new operation to treat popliteal artery aneurysm instead of amputation: a ligation of the femoral vessels in the lower part of its course at the thigh, in the fibrous sheath enclosing the space now known as “Hunter’s canal.”
This has the advantage that the artery at this site is healthy and will not tear when tied, as may happen if ligation is attempted immediately above the aneurysm.
During his fourth operation for popliteal aneurysm, Hunter did not include the vein in the ligature. The patient lived for 50 years afterward. 2
The adductor canal syndrome
“Adductor canal syndrome,” also called “Jogger’s syndrome” has been described as an unusual cause of acute arterial occlusion in younger men.3–9
The adductor canal syndrome has also been identified as a cause of compressive neuropathy of the saphenous nerve.10–13
Surprisingly, to our knowledge, femoral vein compression in the canal has never been described.
Objectives
To describe the anatomy and attempt to explain the physiology of Hunter’s canal. To show that the femoral vein is much more susceptible to compression than the artery. To describe the different mechanisms of venous compression inside the canal, particularly in the outlet.
Material and methods
This was a study of 100 limbs of 50 nonembalmed cadaveric subjects (mean age of 82). All cadavers were obtained from the Division of the “Don des Corps” in the Department of Anatomy, University Paris Descartes, bequeathed by informed consent.
The technique of injection of the venous system of the lower limbs with green neoprene latex has been described previously: 14 After exposing the adductor hiatus area, a colored segmentation was achieved by painting the veins in order to obtain a more comprehensive identification of the anatomical elements.
In addition, we used a series of 200 phlebographies and 100 CT venograms (CTV) to study the 3D morphology of the femoral vein across the adductor hiatus.
The technique of direct CTV used to investigate the venous system has been described previously.15–17 This made it possible to obtain realistic 3D reconstructions of the whole venous network with an accurate morphological description.
A quantification of the venous volume and diameter can be used to assess the degree of compression of the femoral vein. We used Osirix® software (http://www.osirix-viewer.com) in volume rendering (VRT) and multi planer reconstruction (MPR) modes to obtain these quantifications and display the 3D reconstructions.
Results
Anatomical description of Hunter’s canal
The adductor’s canal described by John Hunter is located at the medial aspect of the lower thigh. The roof of the canal is made by the vastus medialis muscle, the floor by the adductors, and it is closed medially by the sartorius muscle (Figure 1).
Anatomy of Hunter’s canal. (a) Medial view of the right thigh. (b) Slice at mid thigh at the level of the black arrow. The roof is made by the sartorius muscle (S). Medially, we find the huge vastus medialis muscle (VM). The floor consists of the two muscles adductor longus (AL) and adductor magnus (AM). The outlet is occupied by the vastoadductor membrane (*). (b) A transverse slice is made at the outlet level (black arrow). Inside the canal, we find the femoral vein (1), a collateral canal (2), the femoral artery (3), and femoral nerve (7). 4=veins of the semimembranosus muscle, 5=great saphenous vein, 6=axial venous arcade, 8=sciatic nerve.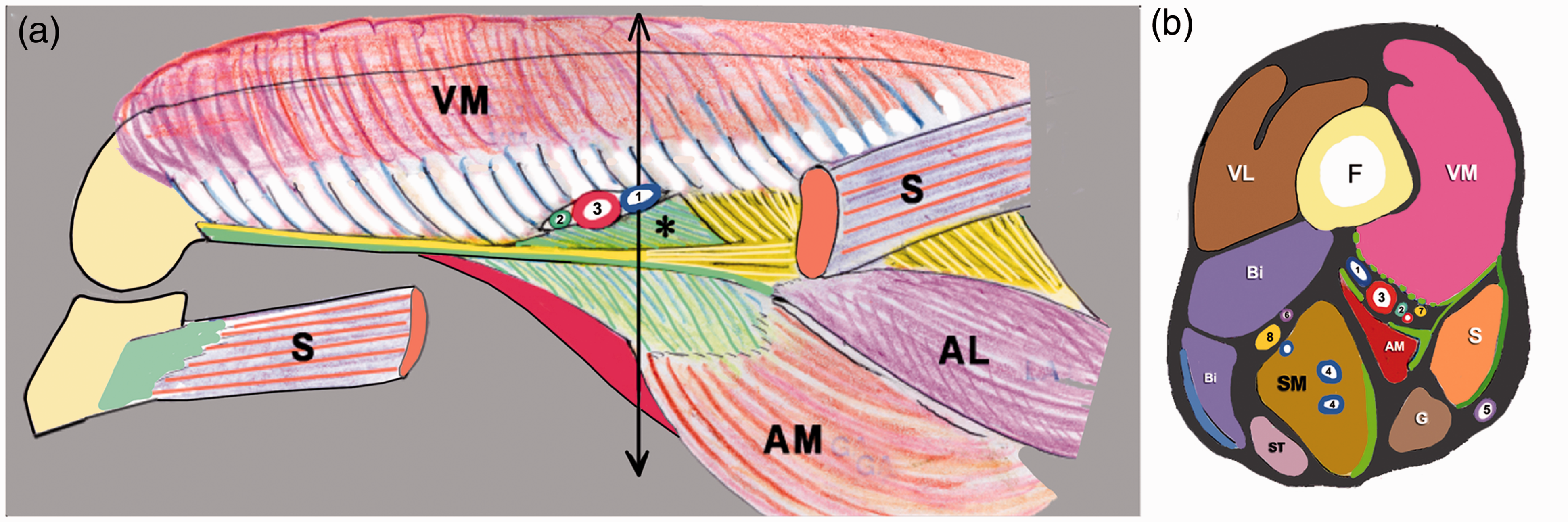
Anatomically, in all cases, we found that a musculotendinous band arose from the adductor magnus muscle, joining the adductor tendon to the vastus medialis (Figures 1 and 2). This band is called the vastoadductor membrane.
18
Hunter’s canal and its outlet (shown by an arrow). (a) Drawing of the Hunter’s canal. (b) Anatomical dissection (medial view). The edge of the vastoadductor membrane is shown by a dotted line.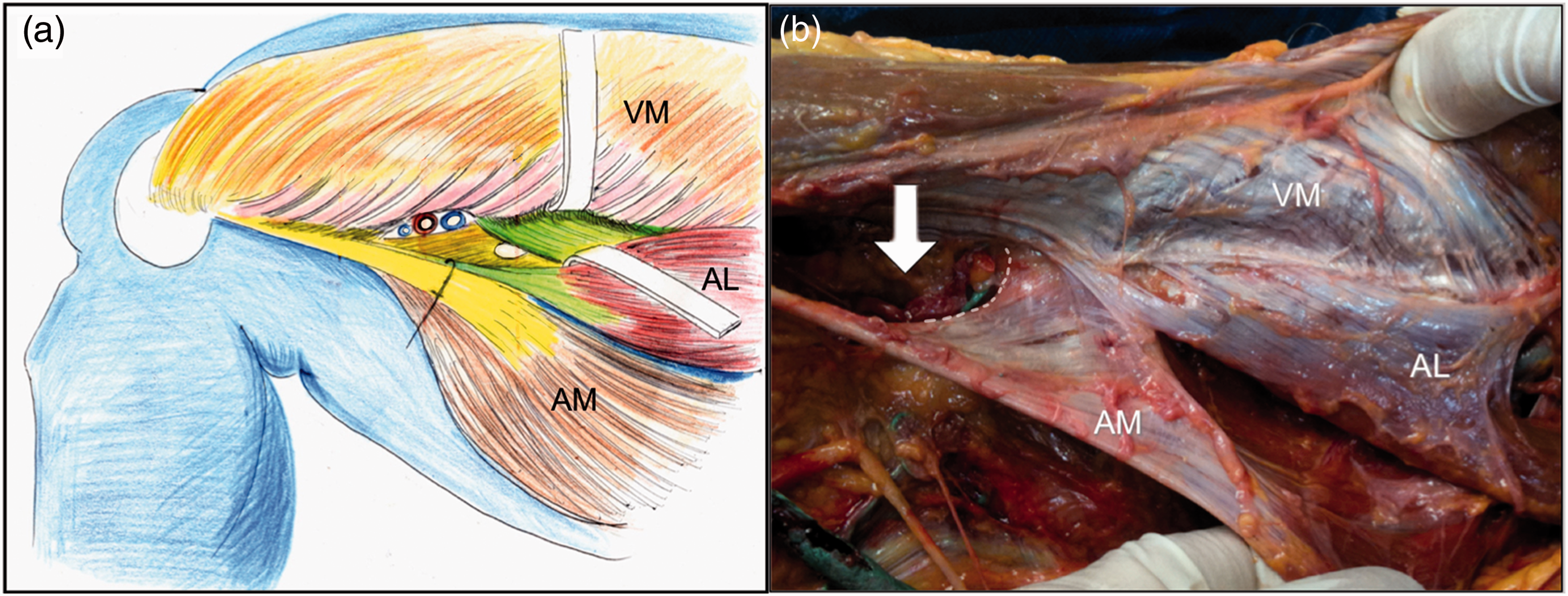
Thus, there is a ring marked by this fibrous membrane that indicates the precise location of the Hunter’s canal outlet (Figure 3). The vascular pedicle being tightened inside this small fibrous space changes its direction to go from the thigh to the popliteal fossa: this explains the frequent kink or plication of the vein, compressed at the posterior aspect of the canal.
Anatomical limits of the outlet of Hunter’s canal. Limits of the outlet: anteriorly, the vastus medialis muscle (VM) and posteriorly, the vastoadductor membrane (yellow*). The femoral vein is located at the posterior part of the outlet, compressed by the artery.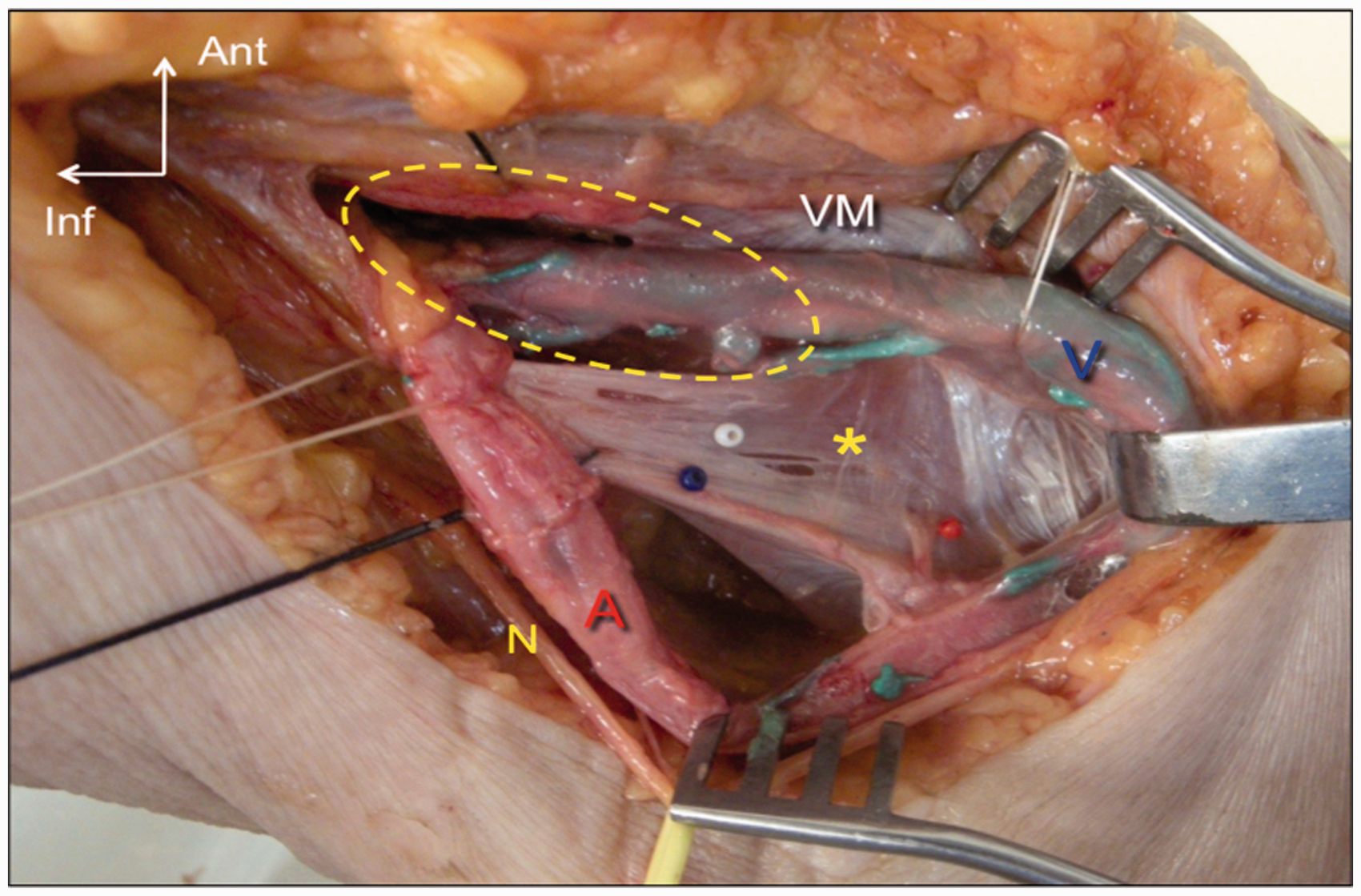
The contents of Hunter’s canal
The artery is located at the anterior aspect of the canal (as shown in Figure 1(b)).
The saphenous nerve is located deeply next to the collateral canal and perforates the muscular fascia at the lower third of the thigh. It runs subcutaneously parallel to the tendon of the adductor longus (Figure 4).
Anatomical dissection of the superficial anatomy of the Adductor’s canal: the perforation of the saphenous nerve (right limb). 1 = Nerve and vessels of the sartorius muscle; 2 = saphenous nerve in the canal above the perforation; 3 = vastoadductor membrane and perforation of the saphenous nerve.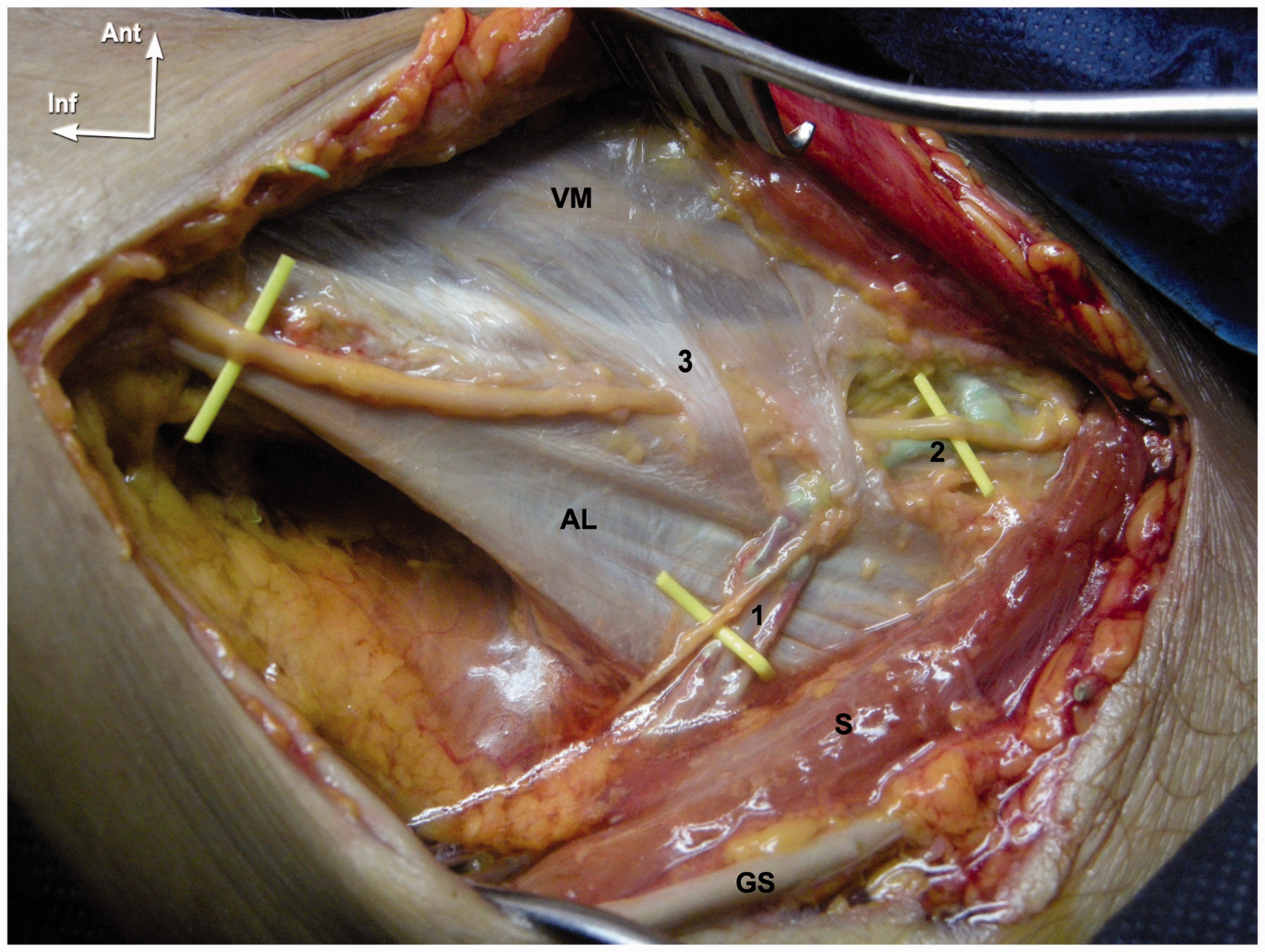
The femoral vein is located more posteriorly and is frequently narrowed at this level by the edge of the vastoadductor membrane (Figure 3). This is particularly true when the artery is calcified, with an imprint on the femoral vein.
The reason for venous compression is the reduced width and stiffness of this part of the canal, surrounded by fibrous structures, while more medially the anatomical elements, including the collateral canal and the nerve, are surrounded by loose adipose tissue and thus have more available space (Figure 1(b)).
Anatomical landmarks of the Hunter’s canal and location of the femoral valves in the vicinity
Summary of the main anatomical landmarks of Hunter’s canal (for an average femur length of 43 cm).
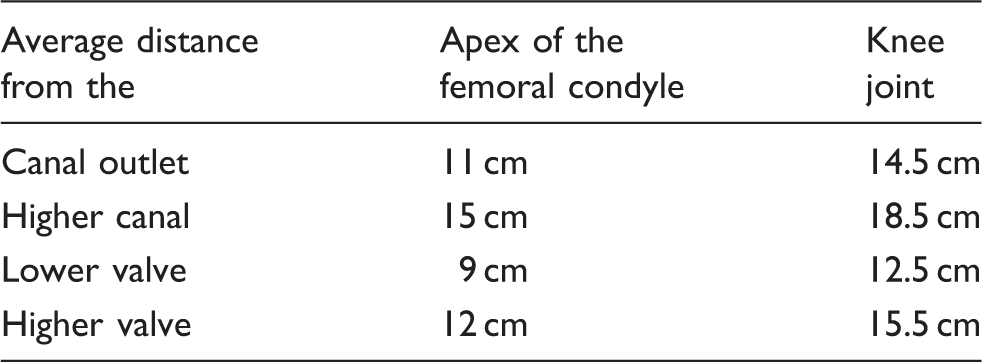
A femoral valve was commonly found just below the canal outlet, located an average of 9 cm above the tubercle of the medial condyle, and another 3 cm above that (12 cm above the condyle).
Three different mechanisms of femoral vein compression in the Hunter’s canal are described in Figure 5
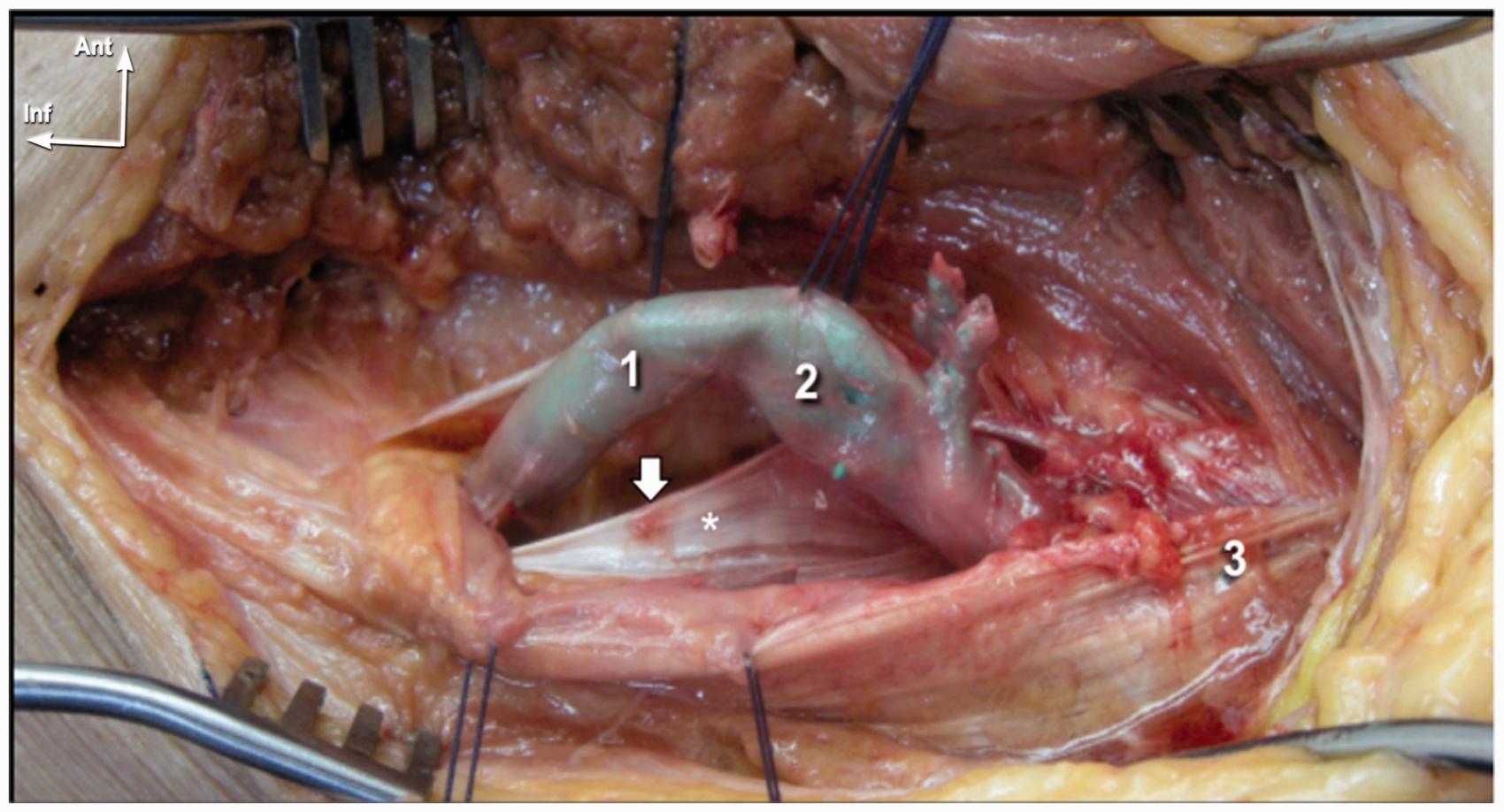
The three types of compression of the femoral vein in the Hunter’s canal: The white arrow shows the edge of the vastoadductor membrane, marked by *. (1) Edge of the vastoadductor membrane responsible for a notch in the canal’s outlet. (2) Compression by a calcified artery in the lower part of the canal. (3) Stenosis higher inside the femoral canal.
The edge of the vastoadductor membrane creates a notch on the vein at the level of the canal’s outlet. In the lower part of the canal, a calcified artery can compress the vein due to the narrowness and stiffness of the canal. Higher inside the femoral canal, compression could cause a longitudinal stenosis with an imprint along the vein.
But the most understandable mechanism of compression is in the canal outlet, due to the edge of the vastoadductor membrane: this stiff anatomical structure creates a notch with venous stenosis occurring at the lower part of the hiatus, which is well analyzed with a cast of a femoral vein injected with latex (Figure 6) on phlebography (Figure 7) and on the 3D reconstructions from CT venography (Figure 8).
Latex cast of the femoral vein with a notch found at the precise location of the edge of the vastoadductor membrane. Also note the venous valve location (V). The transverse section of the vein is shown below to better illustrate the reduction of caliber. Venograms showing two cases of femoral vein stenosis in the outlet. (a) Notch and twist of the vein (arrow). (b) Notch due to the ridge of the vastoadductor membrane (arrow). VenoCT of the lower limbs with 3D reconstruction. (a) Posterior view of a right limb showing a notch just below the valve (v, gray arrow) and an arterial imprint (white arrow) in the lower part of the fibrous canal. (b) Antero medial view with resection of the femur bone showing deep compression of the femoral vein in the outlet of the Hunter’s canal: Notch (gray arrow) and twist (white arrow) of the vein in the outlet. Also note the derivation route in the venous arcades of the semimembranosus muscle (S) joining the popliteal vein to the deep femoral vein above, shunting the femoral compression. (c) Posterior view of a left limb showing longitudinal compression of the artery (white arrows) and compression higher inside the canal (gray arrows).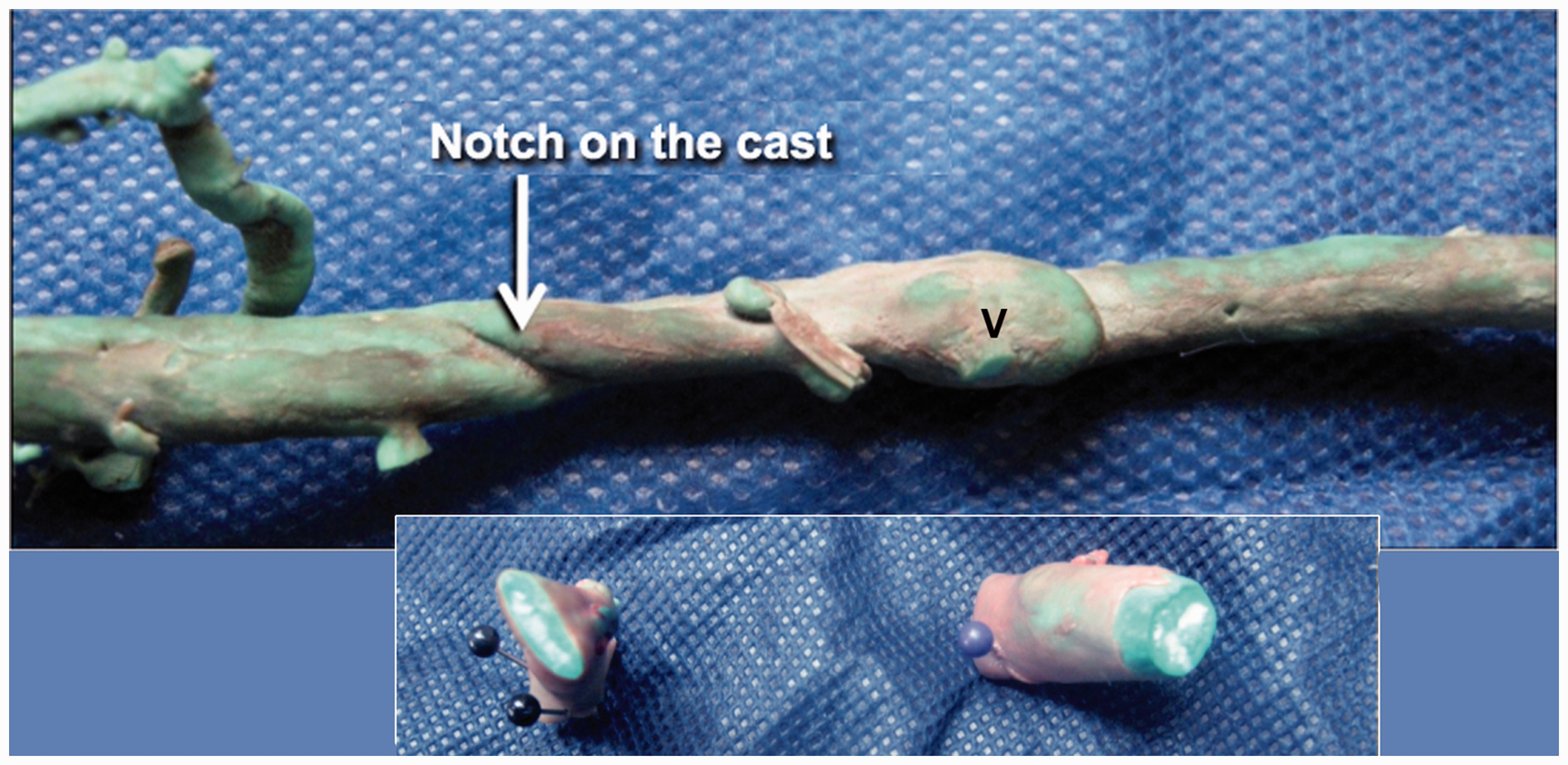


When this type of stenosis was found, it was typically at the lower part of the canal, 12–14 cm above the femoral condyle.
Compression by the artery or higher inside the canal (Figure 8(c)) can also be seen, but they are often missed by the investigations.
Discussion
Discussion about anatomy18–22
The vastoadductor membrane was also described by Tubbs et al. 18 in the Hunter’s canal outlet. Kale et al. 19 tried to classify the hiatus and found the apex located an average of 12 cm from the condyle line. De Souza et al. 20 described the limits of the canal.
Other authors studied the connective tissues inside the canal in order to understand the reasons of early degenerative arteriopathy at that level.21,22
But nobody has described venous compression in the outlet or proposed a physiology of the adductors hiatus.
Proposal for the physiology of the Hunter’s canal
Physiological hypothesis: The cadaveric simulations demonstrated that contraction of the adductor longus closes the hiatus, and contraction of the adductor magnus opens it.
Our hypothesis is that Hunter’s canal prevents femoropopliteal axial reflux by synchronizing with the calf pump ejection during ambulation (Figure 9): During the impulsion phase of the step (extension of the thigh), the systole of the calf muscle pump pushes the blood up into the femoral vein. At this time, the adductor longus is relaxed and the adductor magnus contracts, which opens the Hunter’s hiatus. During thigh flexion, at the beginning of the step (suspension phase), the calf is relaxed and the adductor longus is in tension, which closes the Hunter’s hiatus. This, together with the closure of the Hunter’s femoral valves, avoids downward reflux into the femoropopliteal axis secondary to gravity.
The role of the adductor muscles in regulating flow in Hunter’s canal: On the left side: the adductor longus (AL) opens the canal during extension of the thigh, while the calf pump systole ejects the blood upward into the femoropopliteal axis. On the right side: the adductor magnus (AM) closes the canal during the flexion, while the calf is relaxing (see yellow arrows also in the corresponding anatomical dissection). The roof of the canal is limited by the vastus medialis muscle (VM).
In summary, these anatomical features suggest that the role of the adductor muscles is mainly to regulate the venous outlet of the Hunter’s canal. This is another mechanism preventing reflux along the femoropopliteal axis.
Consequences in clinical practice
Ultrasound investigation of Hunter’s canal for saphenous nerve blocks25–27 is commonly used in locoregional anesthesia of the lower limb. The main advantage of this technique is related to the challenge of providing sensory anesthesia of the lower limb without impairing disposition (quadriceps muscle weakness) of the ambulatory surgery patient.
But the main goal of investigation of the Hunter’s canal is related to the prevention of venous thrombosis of the femoropopliteal axis.
This is particularly true during long-distance flights in immobile sitting position, also called “economy class syndrome.” Of course, the risk of DVT is mostly related to venous stasis by calf pump impairment due to immobility, but the postural compression of the femoral vein in long-lasting sitting position has never be highlighted.
In the sitting position, as previously shown in Figure 9 during walk, the adductor longus muscle relaxes and the adductor magnus is shortened, which closes the outlet of the Hunter’s canal, leading to venous compression.
This could explain that the occlusion site of the femoral vein is commonly the Hunter’s canal outlet, but no clinical studies can confirm this.
Differential diagnosis
The diagnosis of Hunter’s outlet syndrome has to be differentiate from the postural obstruction of the popliteal vein known as “popliteal entrapment syndrome” 28 also playing an underestimated role in the economy class syndrome. But here, the compression is located at the knee level or below knee, related to the position of the knee joint (flexion or hyperextension).
In clinical vascular practice, an duplex ultrasound (USD) investigation at the precise level of the outlet (11–13 cm from the condyle) should be routine, checking for:
An extrinsic compression of the venous axis. A dilatation of the derivative routes (Figure 10), particularly the venous arcades inside the semimembranosus muscle. Derivative routes in cases of stenosis of the Hunter’s canal: The axial vein (8, in red) along the ischiatic nerve (5, in yellow), the deep femoral vein with a low popliteal communicating branch (7), the venous arcades of the vastus medialis (6, in pink), and principally the dilated arcades (9, in blue) of the semimembranosus muscle (SM). These arcades act like a safety valve, derivating blood from the popliteal vein (1) to the deep femoral (10) and thus bypassing Hunter’s canal (white arrow). Black arrows show the way of the blood. White double arrow show the narrowed part of the Hunter’s canal. 2: femoral vein. – the axial vein located along the ischiatic nerve, – the deep femoral vein with a low popliteal communicating branch, – the venous arcades of the vastus medialis, – and especially the dilated arcades of the semimembranosus muscle. These act like a safety valve, derivating the blood of the popliteal vein to the deep femoral vein, bypassing the Hunter’s canal stenosis.

In clinical practice, a venous examination should systematically include an evaluation below the semimembranosus muscle at the posteromedial aspect of the thigh, 10 cm up to the knee joint, close to the midline: the presence of dilated arcades is a sign of stasis, and probably of femoral compression of the Hunter’s outlet.
A prevention should systematically be proposed to those patients before a long-lasting flight.
In some cases, in particular recurrent DVTs, a surgical enlargement of the outlet has to be considered, especially the resection of the vastoadductor membrane that could be performed under endoscopy.
Conclusion
The outlet of the Hunter’s canal is narrowed by a tendinous band, the vastoadductor membrane, joining the vastus medialis to the adductor longus. The vein at this level could be easily compressed in the posterior angle of the hiatus, commonly tightened by a calcified artery.
Compression of the femoral vein in the canal is an underestimated cause of venous obstruction and deep vein thrombosis and explains the high rate of femoral obstruction at that particular level. This is especially true in sitting position during the long-lasting flights called “economy class syndrome,” and we should keep in mind that the Hunter’s canal is in this context an underrated risk factor.
Ultrasound investigation of both limbs should be systematically carried out at this precise level of the venous axis for all CVD patients in order to detect stenosis and prevent future venous obstruction.
Footnotes
Acknowledgements
Thanks to Celine Fortin MD for her participation on this work during the master of phlebology (Paris, France).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.