
Abstract
Objective
To evaluate the results of radiofrequency ablation (RFA) of the great saphenous vein (GSV) using one versus two 20 s energy cycle treatment in the proximal 7 cm segment of the GSV.
Methods
All patients who underwent RFA of the GSV from 1 May 2013 to 30 September 2013 in eight of our vein centers were included. Duplex ultrasound scans (DUSs) were performed prior to treatment on all patients and 2–3 days, and 1 month after procedure. Demographic data, GSV diameters, and other relevant data were recorded. Clinical, Etiologic, Anatomic, Pathologic (CEAP) classification and Venous Clinical Severity Scores (VCSSs) were determined prior to ablation and one month later. Patients who developed endovenous heat induced thrombosis (EHIT) were followed till resolution.
Results
A total of 205 patients had one cycle treatment (group A) and 204 had two cycle treatment (group B). The two groups were comparable in their demography, CEAP classification, and VCSS scores. The rate of failure of ablation and incidence of EHIT were also not significantly different. The incidence of complications was low, <5% in both groups and all were minor.
Conclusion
Two cycle treatment of the proximal GSV for vein ablation does not improve the success rate of vein closure in the short term, compared to one cycle treatment. It also does not increase the risks of DVT, EHIT, major bleeding, and other complications. However, we do not know at what diameter two cycles may be superior to one cycle.
Introduction
Catheter based endovenous thermal ablation using either radiofrequency ablation (RFA) or laser ablation (EVLA) is currently the procedure most often used for the treatment of varicose veins and symptomatic superficial venous diseases of the saphenous veins. It has received wide acceptance because it is a minimally invasive, office based outpatient treatment with good outcomes. Its advantages over the standard surgical management of high ligation and stripping of the great saphenous vein (GSV) include: minimal post-operative pain, 1 faster recovery, 2 and lower recurrence from reduced neovascularity. 3
RFA is currently performed using the ClosureFAST (CF) technique (VNUS Closure Fast: Covidien) which was introduced in 2006. This system uses a 7 cm coil at the distal end of the catheter which operates at a treatment temperature of 120℃ and allows segmental ablation staying stationary every 7 cm during its 20 s energy cycle.4,5
It is recommended by the manufacturer that the proximal 7 cm segment of the GSV where the vein diameter is widest is treated with two 20 s energy cycles. The expected advantage for double treatment is to reduce the risk of failure of ablation, but the possible disadvantage is that it may increase the risk of pain, ecchymosis, deep venous thrombosis (DVT), superficial venous thrombosis (SVT), and endovenous heat induced thrombosis (EHIT). It has also been suggested that only large diameter GSV should be treated with two cycles to reduce the risk of failure of ablation. However, there is no published data to show the advantages and disadvantages of using double versus single treatment cycles.
The purpose of this prospective study is to evaluate the result of RFA of the GSV using one versus two 20 s energy cycle treatment in the proximal 7 cm segment of the GSV and determine if there is any benefit and/or risk of one technique over the other.
Methods
Patients
All patients who were scheduled to undergo RFA of the GSV in eight of our centers by four of our physicians from 1 May 2013 to 30 September 2013 were included in this study. No cases were excluded. Each physician was randomly assigned to do one cycle treatment in one center and two cycle treatment in another center. The study was approved by our research committee and patients provided written informed consent. All of our centers follow the same protocols and use a centralized system of data collection. As there is no data in the literature for the one versus the two cycles treatment, we assumed a 5% failure rate for the one cycle and 1% failure for the two cycles. At a power of 90% and 95% confidence interval (CI) a total of 378 patients in both groups were necessary. Therefore, in our study just over 400 patients were included to allow for technical problems and patients who may not return for their follow-up. All patients had duplex ultrasound scan (DUS) prior to GSV ablation and 3–5 days post procedure. A follow-up scan was done after one month following the procedure. Evaluation of the lower limb veins was performed by qualified technologists in our Intersocietal Commission for the Accreditation of Vascular Laboratories (ICAVL) accredited laboratories using color flow Ge Logic (General Electric, Wauwatsu, WI, USA) with 5- to 8-MHz linear transducers. Saphenous reflux was defined as retrograde flow >0.5 s. 6 In order to eliminate any bias from the treating physicians, all reports and images were reviewed by an experienced surgeon who did not participate in any of the procedures. The clinician providing follow-up was not blinded to the treatment protocol.
Demographic data and clinical information such as age, sex, height, weight; symptoms of chronic venous disease (CVD), and past history of DVT were recorded. No patient was given DVT prophylactic. The body mass index (BMI) was calculated (kg/m2). GSV diameter and reflux times were measured at the SFJ and at the proximal thigh (PT), 10 cm distal to the SFJ prior to ablation. The catheter tip position (CTP) from the SFJ was measured and recorded at the time of ablation. The length of the ablated vein was also recorded. Patients who had stab phlebectomies were identified and the number of phlebectomies performed at the time of GSV ablation was noted.
The patients’ symptoms and signs were recorded using the Clinical, Etiologic, Anatomic, Pathologic (CEAP) clinical classification system 7 and the Venous Clinical Severity Score (VCSS) 8 preoperatively and at one month follow-up. The primary end points were failure of ablation defined as a patent segment >5 cm of the ablated vein with or without residual reflux and development of DVT or EHIT. Patients who were found to have EHIT in the 3–7 day post-operative duplex U/S were classified according to method by Kabnick et al. 9 and were followed weekly till the resolution of EHIT. Secondary end points were development of other complications such as bleeding, skin necrosis, ecchymosis, hematoma, and paresthesia. Post-operative pain scale and return to work time were not evaluated.
Technique
Ablation of the GSV was done using the CF technique (VNUS Closure Fast: Covidien). All the procedures were performed in an outpatient office setting. Our technique for mapping and marking of the superficial vein to be ablated, vein access, and catheter tip positioning 2.5–3.0 cm from the sapheno-femoral junction and tumescent anesthesia has previously been reported. 10 In the four centers that were randomized for single treatment, the proximal 7 cm segment of the GSV was treated with one 20 s energy cycle (group A). In the other four centers two 20 s energy cycles were used for the same GSV segment (group B). Post-operatively the limb was wrapped with elastic bandage from the ankle to the thigh for 24 h.
Data were collected in Excel (Microsoft, Redmond, WA, USA) and converted to SPSS (IBM Corp., Armonk, NY, USA) for statistical analysis. Categorical data were compared by a two-tailed Fisher exact test. Continuous variables such as age and BMI were assessed with a two tailed t test. p values of <0.05 were considered significant.
Results
Demographics and other parameters.
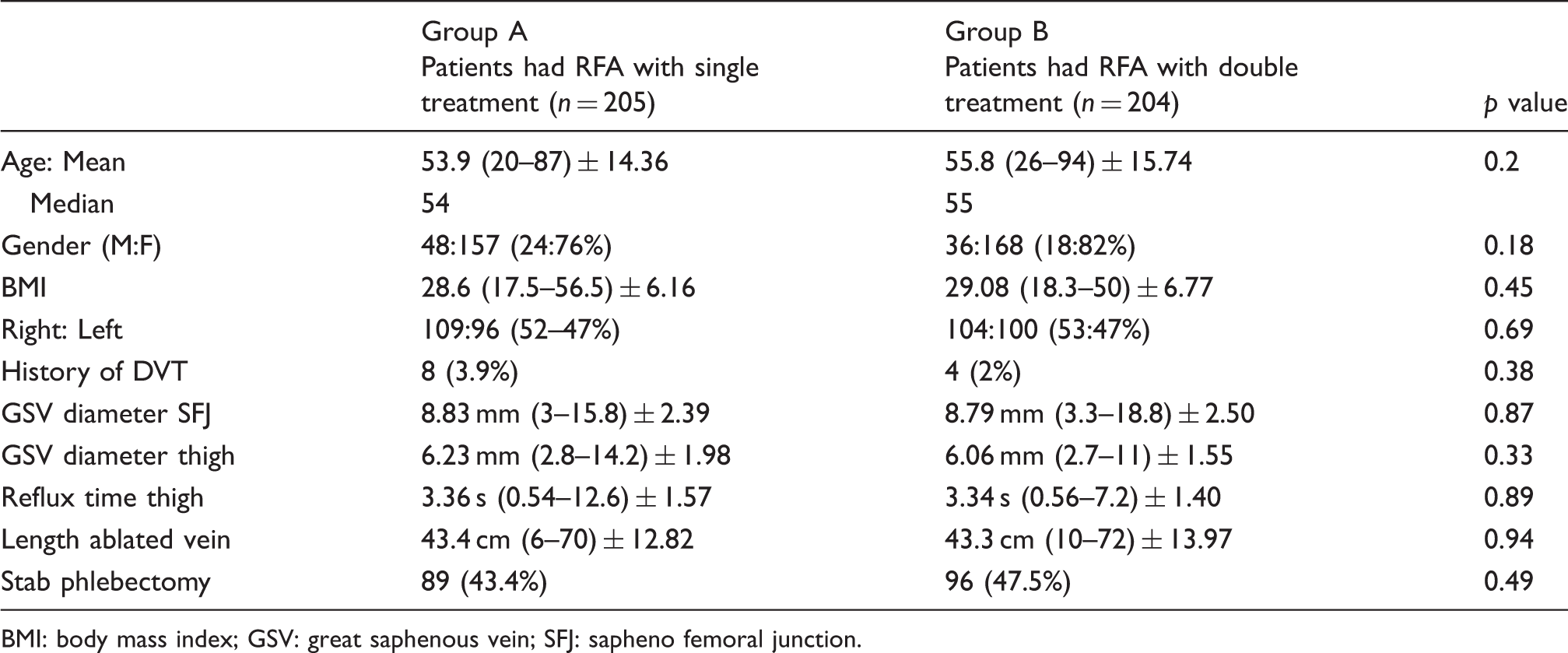
BMI: body mass index; GSV: great saphenous vein; SFJ: sapheno femoral junction.
There was no difference in the CEAP class (mean 2.59 vs. 2.61) or the VCSS score (mean 4.98 vs. 5.71) prior to the RFA ablation in the two groups. Likewise the one month post-operative improvements in CEAP class (mean 1.79 vs. 1.81) and the VCSS score (mean 2.13 vs. 2.48) were similar in both groups.
Incidence of EHIT.

EHIT: endovenous heat induced thrombosis.
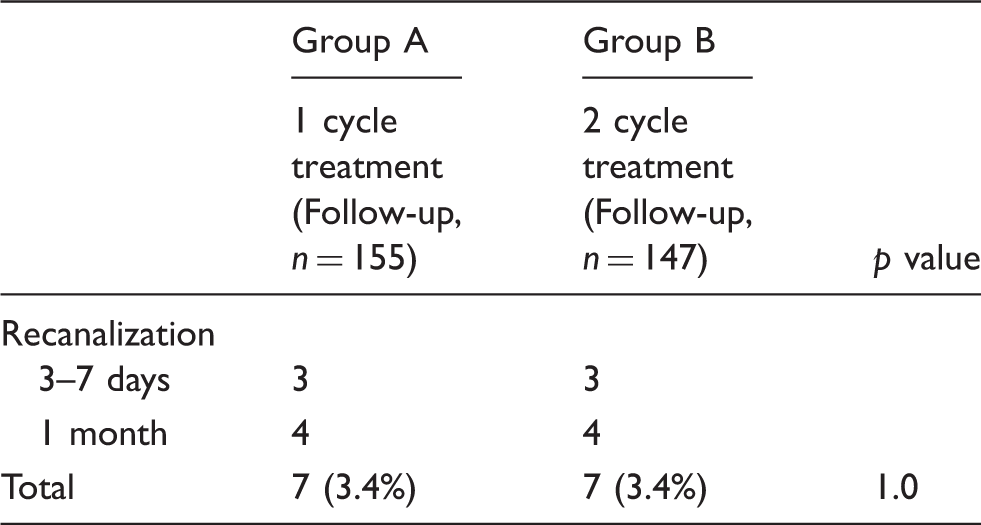
Recanalization rates after one month.
No cases of skin necrosis, major bleeding, or pulmonary embolism were identified in either group. Mild hematoma occurred in two cases in group A and three cases in group B. No paresthesia occurred in either group.
Discussion
The PT segment of the GSV most often has the largest diameter. Therefore it is expected that increased energy delivery will improve the occlusion rate. Consequently, the manufacturer has recommended that this GSV segment should be treated with two energy cycles.
Proebstle et al. 4 reported delivering an average linear endovenous energy density (LEED) of 116.2 ± 11.6 J/cm along the first 7 cm of GSV. This was to ensure good vein closure to what they referred to as “critical location”, compared to 68.2 ± 17.5 J/cm along the rest of the vein. Their mean GSV diameter at the thigh was 5.7 mm and the occlusion rate was 99.6% at six months. Similarly high rates of occlusion were reported by others using the same technique.11,12 Another study demonstrated 98% occlusion rate at short term when using three cycles in each of the 7 cm cycles. 13 However, there is no published data to show the benefits and or risks of two cycle treatment over one cycle treatment. In our study, 96.6% occlusion rate was achieved at one month. The number of cycles did not affect the occlusion rate.
We have previously reported our experience with 201 EHIT cases out of a cohort of 6707 patients where the incidence of EHIT was 2.99%, but if only those who developed significant EHIT, i.e. >class 2, the incidence was 1.25. 10 In our present study, the incidence of EHIT for group A was 3.41% versus 1.96% for group B. However, if only those with >class 2 are considered the incidence rates were 1.95 versus 1.47 which is not significantly different. There was no difference in the early clinical outcome as measured by the VCSS in the two groups.
Our study shows no significant benefit or risk of using double cycle treatment in the proximal GSV over single cycle treatment. This suggests that the LEED delivered with single treatment may be adequate when CF technique is used. In addition to the amount of thermal energy delivered, another factor such as proper tumescent infiltration to cause compression and spasm of the GSV may be important for successful ablation.
It has also been suggested that only large diameter GSV should be treated with two cycles to reduce the risk of failure of ablation. In our published data, we found out that mean diameter of the GSV in symptomatic patients with GSV reflux was 7.9 ± 3.8 mm compared to those that developed EHIT which was 10.2 ± 2.7 (p < 0.001). 10 In our current study, the mean diameter of the GSV at the SFJ was 8.83 mm ± 2.39 and at the PT (10 cm from the SFJ) it was 6.23 ± 1.98 for those treated with one cycle and for those with double cycle it was 8.79 ± 2.50 mm at the SFJ and 6.06 ± 1.55. This correlates well with the recent study by Mendoza et al. 14 who reported that the diameter of the GSV at the SFJ in patients with reflux has a mean diameter of 10.9 mm (±3.9) compared to 6.3 mm (±1.9) at the PT. They note that the GSV diameter measurement at the PT (15 cm from the SFJ) has a better correlation with clinical class and is more sensitive and more specific than measurement at the SFJ.
Our study has several limitations. Although the sample size in each group was large, there were not enough patients with large vein diameter (>10 mm) at the PT in order to perform a meaningful analysis. In a recent presentation at the European venous forum it was demonstrated that a single cycle had a higher recanalization rate for GSV >10 mm diameter. 15 When three cycles were used in the PT segment there was only one recanalization out of 174 GSV treated. Interestingly, the only patient who had complete recanalization in our study had GSV diameter of 12 mm. Two cycle treatment may be useful to treat GSV with >10 mm diameter, but further study will be required to determine its advantage. Another limitation was the short follow-up and 25% lost to follow-up. According to our power calculations, we needed 378 patients and in the follow-up we were short by 76. However, it is very clear that the difference we assumed is not there and practically there is no difference for the two methods for the diameters we treated. Typically the failure rates increase somewhat over time but usually the difference is not statistically different in the next three years. Finally, although our patients were consecutive the individual patients were not randomized, but the surgeons were assigned to perform one cycle or two cycles to the proximal GSV at sites that were randomly assigned.
Conclusion
Our study shows that two cycle treatment of the proximal GSV for vein ablation does not improve the success rate of vein closure in the short term, compared to one cycle treatment. It also does not increase the risks of DVT, EHIT, major bleeding and other complications. However, we do not know at what diameter two cycles may be superior to one cycle.
Footnotes
Acknowledgments
We are grateful to Ms Marsha Withers and Mr Rohan Vanjara of Center for Vein Restoration for their invaluable help with data collection.
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.