
Abstract
Many female patients are affected by chronic pelvic pain and a significant number of referrals to the gynecology department result in a clinical suspicion of pelvic congestion syndrome. Additionally, patients referred to the vascular surgery department for venous disease can also present with complaints of a persistent dull lower abdominal pain in addition to typically distributed leg varicosities (that extend from the leg through the pelvic floor) which should be evaluated for the presence of pelvic congestion syndrome. In this article, we focus on imaging pelvic vein insufficiency and related (extending) varicosities: how should we evaluate the pelvic veins, what are the signs to look for, and what are the currently established criteria for (pre-interventional) imaging.
Keywords
Introduction
It is commonly accepted that pelvic congestion syndrome (PCS) is caused by the development of varicose veins in the trajectory of the ovarian veins.1,2 A combination of retrograde blood flow and/or dysfunctional venous valves within the ovarian veins increases the pressure within this part of the pelvic venous system which cannot sufficiently compensate and dilates as a result. Literature suggests that not all patients with enlarged pelvic veins are symptomatic, which complicates establishing diagnostic criteria for PCS based on ovarian vein diameter.3,4 Additionally, in some patients the ovarian veins are not or only minimally affected and pelvic varicosities deriving from other parts of the pelvic venous system (e.g. pelvic floor and common or internal iliac veins) cause the symptoms.5–7 This makes accurately identifying and imaging PCS a challenge.
Imaging techniques
It is important to acknowledge that imaging studies are only valuable in patients with a clinical suspicion of PCS.3,8 Imaging cannot diagnose PCS, and it should be used to identify varicosities within the pelvis, identify deep vein obstruction or an alternative diagnosis (that causes chronic pelvic pain).
Ultrasound
Depending on the initial referral, there are different first-line imaging modalities. Patients from the gynecology department usually are screened with trans-vaginal ultrasound. Patients referred from the vascular surgery department have either been screened with trans-abdominal ultrasound or are referred for screening.
The trans-vaginal approach is considered to be the examination of choice since it offers better visualization of the pelvic venous plexus compared to trans-abdominal ultrasound, and is not hampered by patient habitus or undisplaceable bowel gas. On the other hand, more central disease (at the level of the renal veins or common iliac veins) is better appreciated with trans-abdominal ultrasound. Both ultrasound techniques can be performed with patients in a standing/upright position (even though contrary to the leg, for the abdomen this might prove a challenging task to perform). With color Doppler, a dynamic examination of the flow in the (dilated and tortuous) pelvic veins can be performed. An example of dilated and tortuous pelvic veins is shown in Figure 1.
Color Doppler example of tortuous and dilated pelvic veins (arrows) in a patient with pelvic congestion syndrome.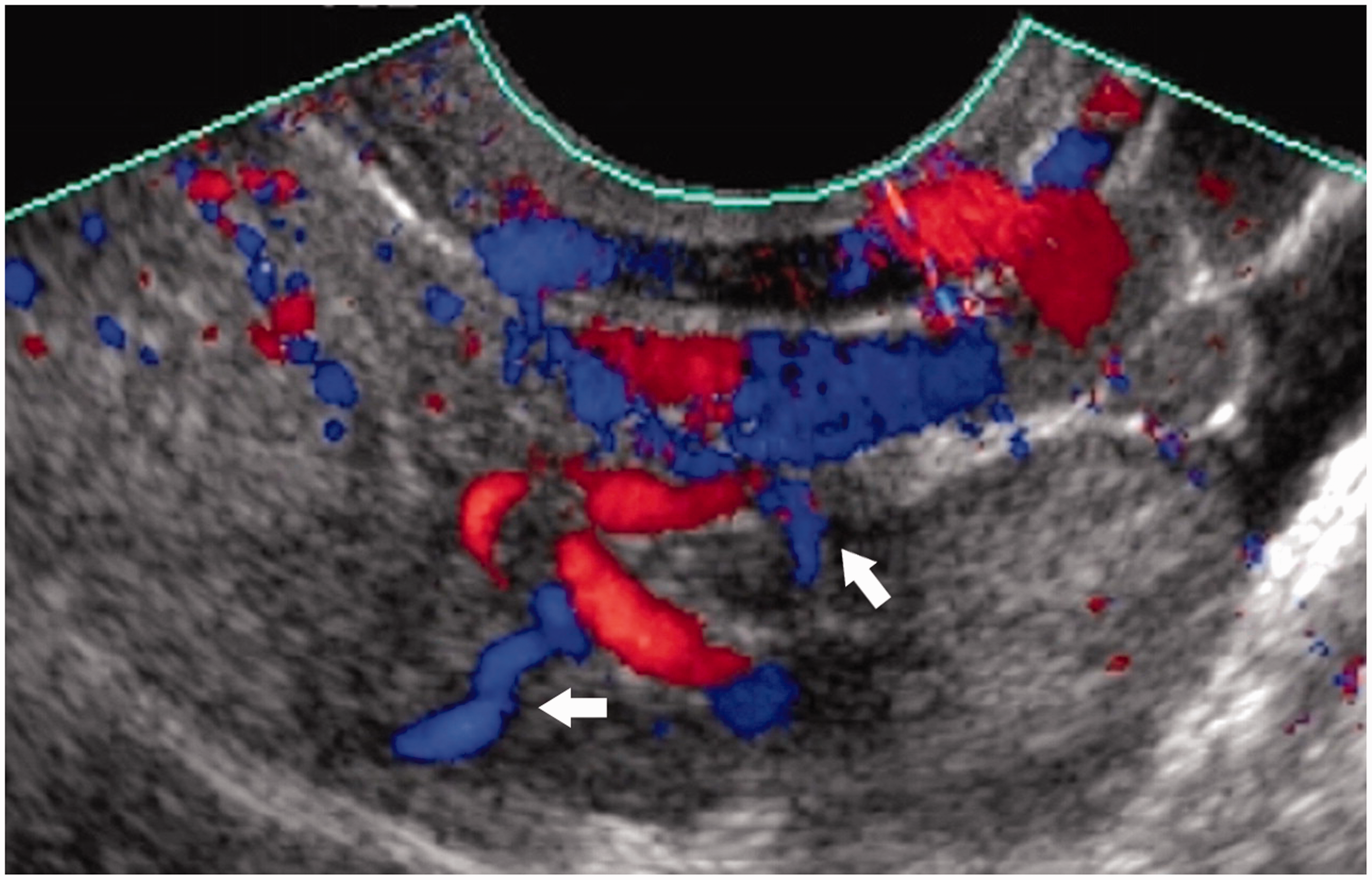
The Valsalva maneuver can be used to increase the venous filling and identify even the less prone pelvic varicosities. One important thing to take into account when evaluating flow using the Valsalva maneuver for pelvic veins, is that it differs from the value for extra-pelvic varicosities such as scrotal varicocele where abrupt flow filling is highly diagnostic. 1 Intraperitoneal variable Doppler waveform appearances are reported, but reversed flow direction and/or abrupt disappearance of flow are highly suggestive of insufficiency.
CT and MR venography
Both CT and MR offer cross-sectional imaging with a detailed anatomical overview of both the pelvic vasculature and the surrounding tissue. Different techniques have been described to identify pelvic varicosities and visualize the abdominal veins.9–12 Contrast-enhanced techniques are superior to non-enhanced techniques and MR has the advantage over CT, as it does not require radiation in this generally pre-menopausal population. An example of contrast-enhanced MR venography is shown in Figure 2.
Multiphase contrast-enhanced magnetic resonance venography showing left ovarian vein insufficiency (arrows).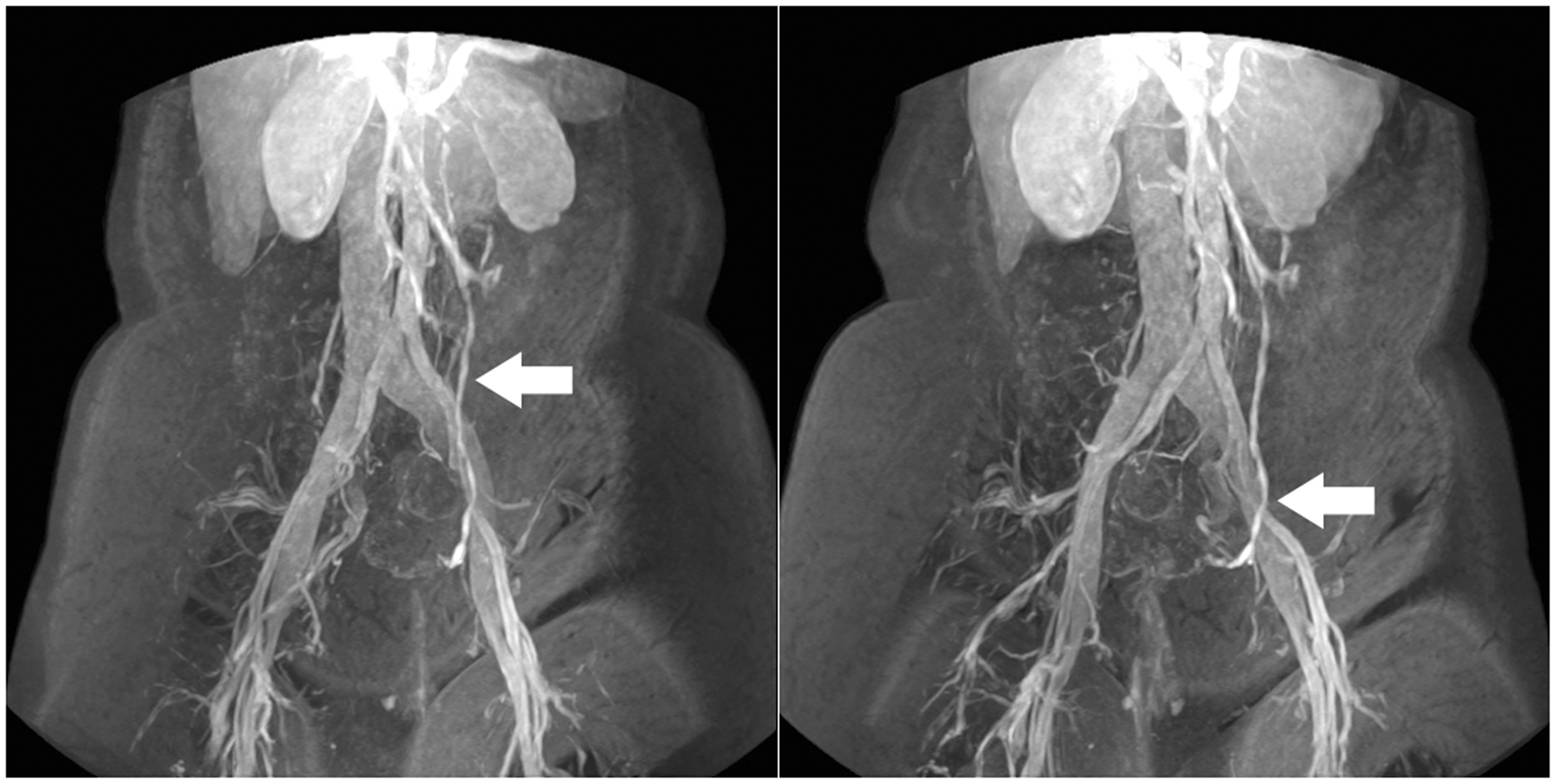
Pelvic varicosities are identified as enlarged (dilated), tortuous tubular structures in the trajectory of the ovarian veins, around the uterus, around the adnexa, and in the pelvic floor. In cases of leg varicosities extension through the pelvic floor into the abdomen, these can be followed from the medial upper leg to their main drainage point/point of origin. This helps in identifying the (main) vein(s) that need to be treated during the intervention. Furthermore, the renal veins can be assessed for signs of compression (Nutcracker syndrome), as well as the common and/or external iliac vein. 13 Compressive tumors, cysts or arterial aneurysms can also be identified if the CT/MR imaging protocol includes scans/sequences to visualize the pelvic anatomy. In our experience, external compression can be an important contributing factor which should be evaluated in the routine imaging work-up. Pelvic inflammatory disease and endometriosis are reported to cause chronic pelvic pain but are not routinely included in the imaging protocols for PCS, as they require different settings (not focused on visualizing vasculature).
Imaging criteria for pelvic varicosities
Established criteria for the (imaging) diagnosis of PCS.

PCS: pelvic congestion syndrome.
As can be seen in Table 1, all imaging techniques can identify patients suspected of pelvic varicosities, even though the criteria are not equal. In particular, the reported cut-off values for ovarian vein diameter differ between the techniques. MRI (and to a lesser extend CT) can then aid in providing a more detailed overview of the disease and the anatomy, defining the location and extent of the insufficiency and corresponding treatment option(s).
Other signs
On ultrasound, polycystic changes of the ovaries can be identified, something that has been shown to be present in up to four times as often in patients with PCS compared to control subjects.
1
On CT and MRI, obstruction of the iliac veins, most commonly the left common iliac vein (May–Thurners syndrome) can be identified, which has been reported to cause varicocele.
17
An example of May–Thurners syndrome is shown in Figure 3.
May-Thurners syndrome as visualized by contrast-enhanced magnetic resonance venography. (a) Compression of the left common iliac vein by the overriding right common iliac artery is seen (arrow). (b) Dilation and collateral formation are seen at the level of the presacral plexus (double arrow). (c) Dilation and collateral formation are seen at the level of the pelvic floor (arrowhead). (d) Coronal reformat of the compressed common iliac vein (double arrowhead).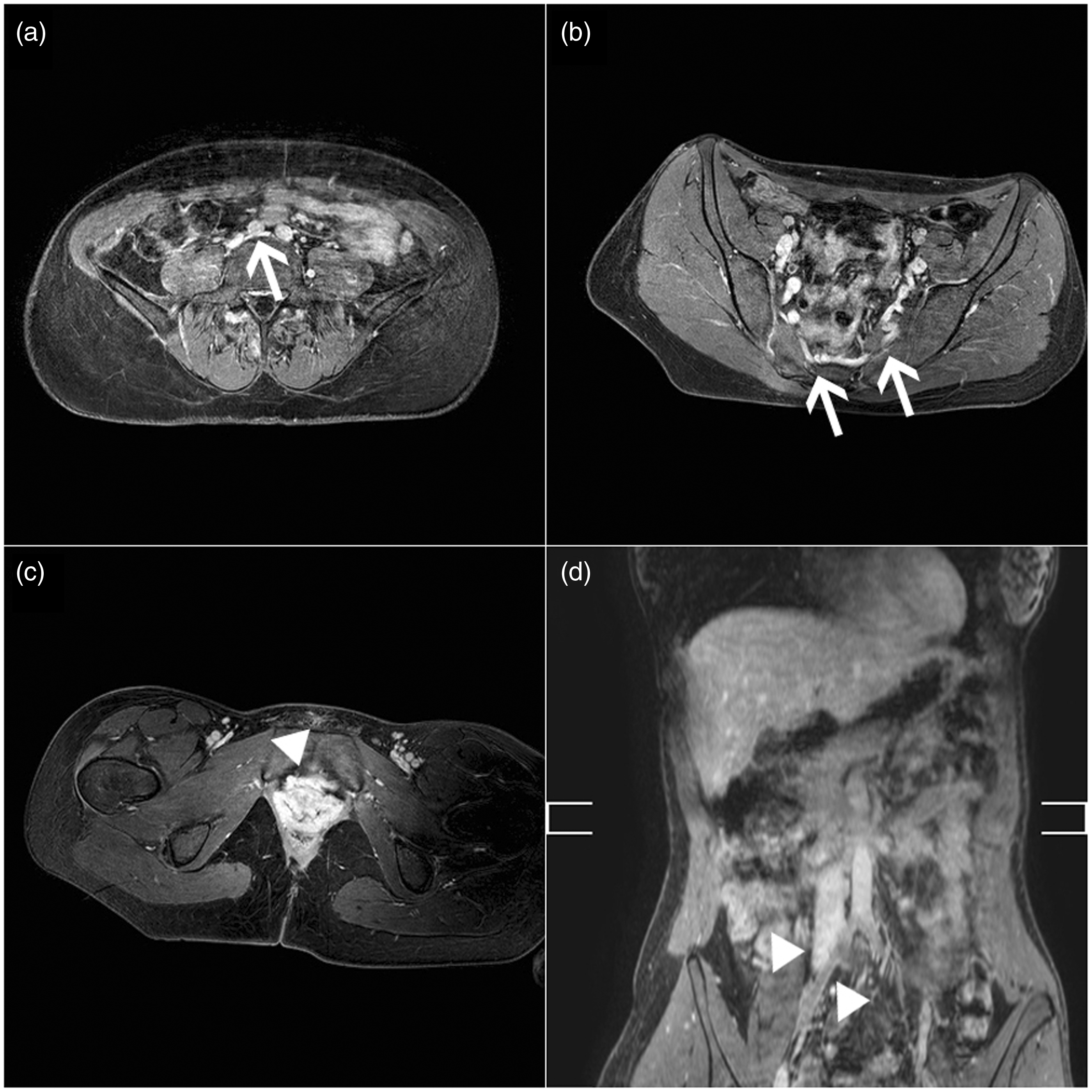
An iliac vein obstruction can be an important cause of pelvic vein insufficiency due to diversion of flow through the pelvic (most commonly left to right).
Items routinely screened in our patients suspected of pelvic congestion syndrome.
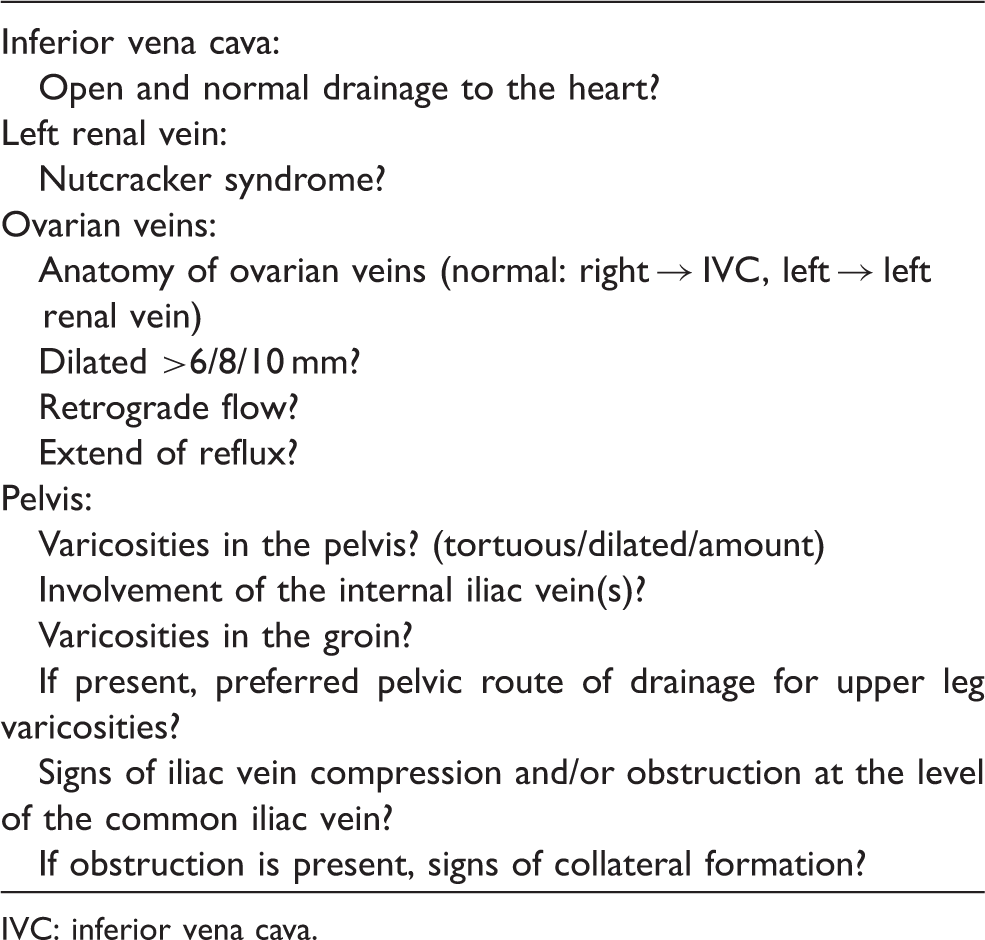
IVC: inferior vena cava.
Importance of correct diagnosis
The first report on treating PCS with embolization of the ovarian veins was published over two decades ago. 21 In the following years, variable success was reported with success rates between 50% and 80%.21,23 In recent years, success is reported between 60% and 100%, which still requires improvement.24–29 Reasons for the variation in success could be caused by variations in the definitions of pelvic insufficiency, variations in embolization technique, variations in outcome measurements but also a still incomplete understanding of the pathophysiological mechanism (or mechanisms) underlying the disease. As can be seen in Table 1, there are different criteria for different imaging modalities and the value of augmentation techniques (such as Valsalva) is unclear. Most commonly coils are used for the embolization of the pelvic veins,27,29 some add a sclerosant to seal the plexus.24,25
In two studies that treated both the ovarian veins and the internal iliac veins, symptom improvement was seen in 93%–96% of patients.25,28 Two studies that treated only the ovarian veins showed symptom improvement in 82%–100% of patients.26,27 Worsening of symptoms was reported in 1%–4% and no changes of symptoms in 7%–13%. The above results suggest that despite the variations in procedural technique (uni- or bilateral embolization of the ovarian veins and/or interna iliac veins) similar results are achieved. There is however still a high number of patients that are diagnosed and treated with limited success. Could it be that we are over treating in some cases or missing a crucial link between the various insufficiencies? Does a more central deep vein obstruction in the (common) iliac or renal vein affect the outcome of ovarian vein embolization? No randomized controlled studies have been performed to date that show a benefit for treating pelvic vein obstruction at the level of the iliacs or renals in patients with PCS. Neither has it been investigated if such obstruction is present in patients that have shown worsened symptoms after embolization, because in fact they embolized the collaterals. In a nutcracker syndrome the outflow of the kidney will be impaired and in a May-Thurners syndrome the venous outflow from the pelvis is further impaired causing a potential increase in venous pressure and symptoms.
Conclusion
For most patients, PCS is a treatable disease if diagnosed and treated correctly. The variations in pelvic vein anatomy and pelvic varicosities mandate accurate pre-interventional imaging to ensure embolization is effective for symptom relief. Future studies need to focus on creating more elaborate but strict criteria for diagnosing PCS to improve patient selection and optimize outcome and prevent obliteration of vital collaterals.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.