
Abstract
Aim
To investigate the potential role of a novel electrostimulation device in augmenting the femoral vein venous blood flow following total knee replacement surgery.
Material and methods
A total of 30 consecutive patients undergoing total knee replacement were allocated to receive either peroneal nerve electrostimulation plus low molecular weight heparin and below-knee compression stockings (Group 1, electrostimulation group, n = 15, mean age: 63.40 ± 5.91 years, male: female ratio 9:6) or low molecular weight heparin and below-knee compression stockings alone (Group 2, control group, n = 15, mean age: 63.86 ± 7.47 years, male: female ratio 8:7). Electrostimulation was performed for 1 h in every 4 h after the operation. Peak blood velocity in the femoral vein was evaluated with Duplex ultrasonongraphy in supine position. Presence of leg edema and calf diameter was also taken into consideration as outcome measures, which were recorded both before surgery and at the time of discharge from hospital.
Results
Postoperative peak blood flow velocity in the femoral vein was significantly higher in electrostimulation group compared to control group (17.46 ± 2.86 cm/s vs. 13.84 ± 3.58 cm/s, p < 0.02). Electrostimulation group achieved a significant increase in peak blood flow velocity in the femoral vein after the operation (mean increase 67.48 ± 17.38%, p < 0.001).
Conclusion
Electrostimulation of the common peroneal nerve enhanced venous flow in the lower limb and may potentially be of use as a supplementary technique in deep venous prophylaxis following lower limb orthopedic operations.
Introduction
Venous thromboembolism (VTE) has been of major concern following total knee replacement (TKR) since its occurrence increases cost, readmission rates, and mortality. 1 The prevalence of positive venographic findings of VTE was reported to be as high as 57.6% in patients undergoing TKR who did not receive chemical prophylaxis. 2 Moreover, symptomatic VTE is quite more infrequent in this population with the incidence being ranged from 0.44% to 2.6% depending on the specific characteristics of the population.3,4 These highlight the importance of using a standardized prophylaxis regimen against VTE that will outweigh the costs of treatment since most patients with thrombosed lower extremity veins remain asymptomatic without any chemical prophylaxis within 1 year after surgery.2,5
Based on recent randomized trials, current practice guidelines recommend anticoagulation agents including low-molecular weight heparin (LMWH), fondaparinux, and vitamin K antagonist for patients undergoing TKR (Grade 1A recommendation). 6 The concept of the well-known multifactorial pathogenesis of VTE including hypercoagulability, venous stasis and endothelial damage, or the so-called Virchow's triad, can be well translated to the setting of orthopedic surgery 7 where release of thromboplastins from reamed bones and incised tissue may add to the diminished venous blood flow due to postoperative immobilization. 8 This insight supports the use of additional measures including early mobilization after surgery and use of intermittent pneumatic compression (IPC).9,10 However, early mobilization may be unachievable in some patients with comorbidities and IPC has certain limitations regarding its use including poor compliance, patient intolerance and inappropriateness for use at home.
The Geko (FirstKind Ltd, High Wycombe, UK) is a novel device, producing rhythmic electrostimulation to the common peroneal nerve of the leg and thus triggering contraction of the muscles responsible for dorsal flexion of the foot. The device was demonstrated in healthy volunteers to augmentate venous, arterial, and microvascular blood supply in the leg,11,12 suggesting a novel means of preventing stasis and thus contributing to existing prophylaxis regimen against VTE. We conducted a pilot study to evaluate its potential role in augmenting venous flow in patients undergoing TKR surgery.
Material and methods
From September through October 2014, a prospective randomized investigator-blinded pilot study was carried out in a university hospital setting and the study group was made up of patients who were scheduled to undergo TKR for severe knee osteoarthritis. The study was approved by local ethics committee and all participants signed procedure oriented informed consents. Participants were also informed about the context of the study and they signed informed consent forms which include a detailed description of the study procedure. All patients <75 years of age with a clear indication for knee replacement were considered eligible. Patients with polytrauma and thigh or leg fractures, varicose veins, previous knee arthroplasty, severe obesity, congestive heart failure, history or family history of venous thromboembolism, and severe motor disability were excluded. Using a computerized randomization, a total of 30 consecutive patients were allocated to receive either a standardized protocol of peroneal nerve electrostimulation plus LMWH and below-knee compression stockings (Group 1, electrostimulation group; standardized protocol of peroneal nerve electrostimulation plus LMWH and below-knee compression stockings, n = 15, mean age: 63.40 ± 5.91 years, male: female ratio 9:6) or LMWH and below-knee compression stockings alone (Group 2, control group; LMWH and below-knee compression stockings alone, n = 15, mean age: 63.86 ± 7.47 years, male: female ratio 8:7). Randomization was performed using blocks in two methods to ensure equal numbers of patients in each group. A blocked design overcomes a possible imbalance in the number of patients assigned into two groups by simply clustering the numbers into two sets containing assignment numbers (i.e. 1 or 2) from both groups. All of the operations were performed by one of two orthopedic surgeons who had adequate experience in knee surgery. Operations were performed under spinal/epidural anesthesia and patients were taken to post-surgical ward soon after the operation. Calf diameters of patients were measured at the largest below-knee diameters of the both legs and the measurements were performed both before and after the operation (immediately before discharge). Presence of leg edema was defined as >10% increase in calf diameter at the involved leg compared to the uninvolved leg. Peak blood flow velocity in the femoral vein was measured using color Duplex ultrasonography. Ultrasonography examination was performed both before and after surgery with the compression stockings being removed in both sessions. In Turkey, the Geko device used in the present study costs approximately US$125 per patient.
Compression stockings were applied soon after the patients arrived on the ward and all patients were initiated on LMWH (subcutaneous injection of enoxaparin sodium, 1 mg/kg, twice daily) about 6 h after the operation. In electrostimulation group, Geko device was applied by a vascular surgeon to the skin over the common peroneal vein, just above the crease of the knee on the involved leg, according to the manufacturer's instructions. Electrostimulation was delivered with a repetition rate of 1 Hz and a current of 27 mA, with the pulse width was set individually around 200 µs (adjusted by pressing the on-button several times) until obtaining a visible twitch on the foot. When a patient complained of discomfort, the level of stimulation was decreased to lower level to enhance patient compliance. A nurse was assigned to check for the device was well-functioning for one hour in every 4 h during the ward stay. The patients were allowed to mobilize out of bed on the day after the operation and encouraged to walk during their hospital stay. The device was operated only while the patients were resting in bed lying in supine position. They were referred to ultrasound scanning the day before discharge to home. In both groups, peak blood flow velocity in the femoral vein was measured using a 7.5 MHz linear array probe with the patient being in supine position. In both groups, femoral vein blood flow velocity was measured without compression stockings. In electrostimulation group, the Geko device was removed before transferring the patient to ultrasonongraphy unit in order to ensure blinding of the radiologist involved in the study.
Statistical analysis
All statistical analyses were performed using SPSS (SPSS version 19.0 Inc. Chicago, IL. USA) packaged software. Visual histograms and analytical methods (Kolmogorov–Simirnov/Shapiro–Wilk's test) were used for determination of normal distribution. Continuous variables were defined by the mean ± standard deviations. Parametric data were compared using independent sample t-test and nonparametric data were compared using Mann–Whitney test. Intragroup comparisons were performed using paired samples t-test. Categorical variables were compared using chi-square test or Fisher's exact test where appropriate. A p-value of less than 0.05 was considered to be statistically significant.
Results
Baseline characteristics.

Changes in study parameters between before and after the operation.
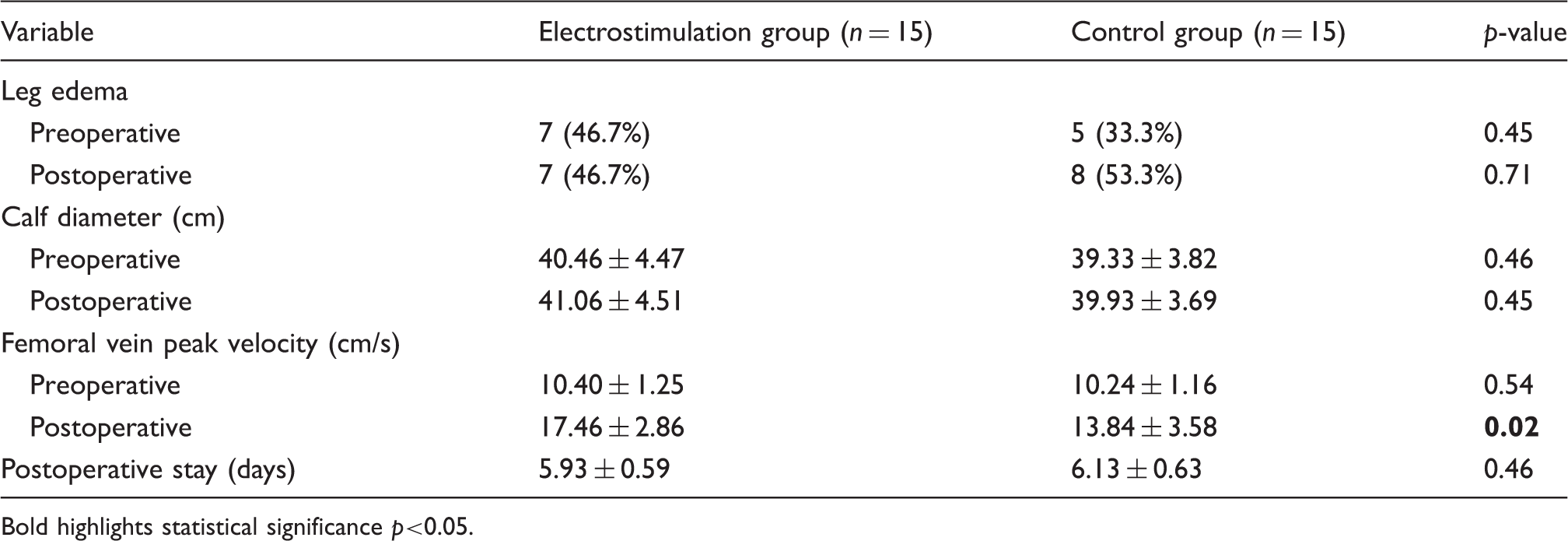
Bold highlights statistical significance p<0.05.
Individual adjustment of device parameters and patient experience in electrostimulation group (electrostimulation was delivered with a constant pulse current of 27 mA and repetition rate of 1 Hz).
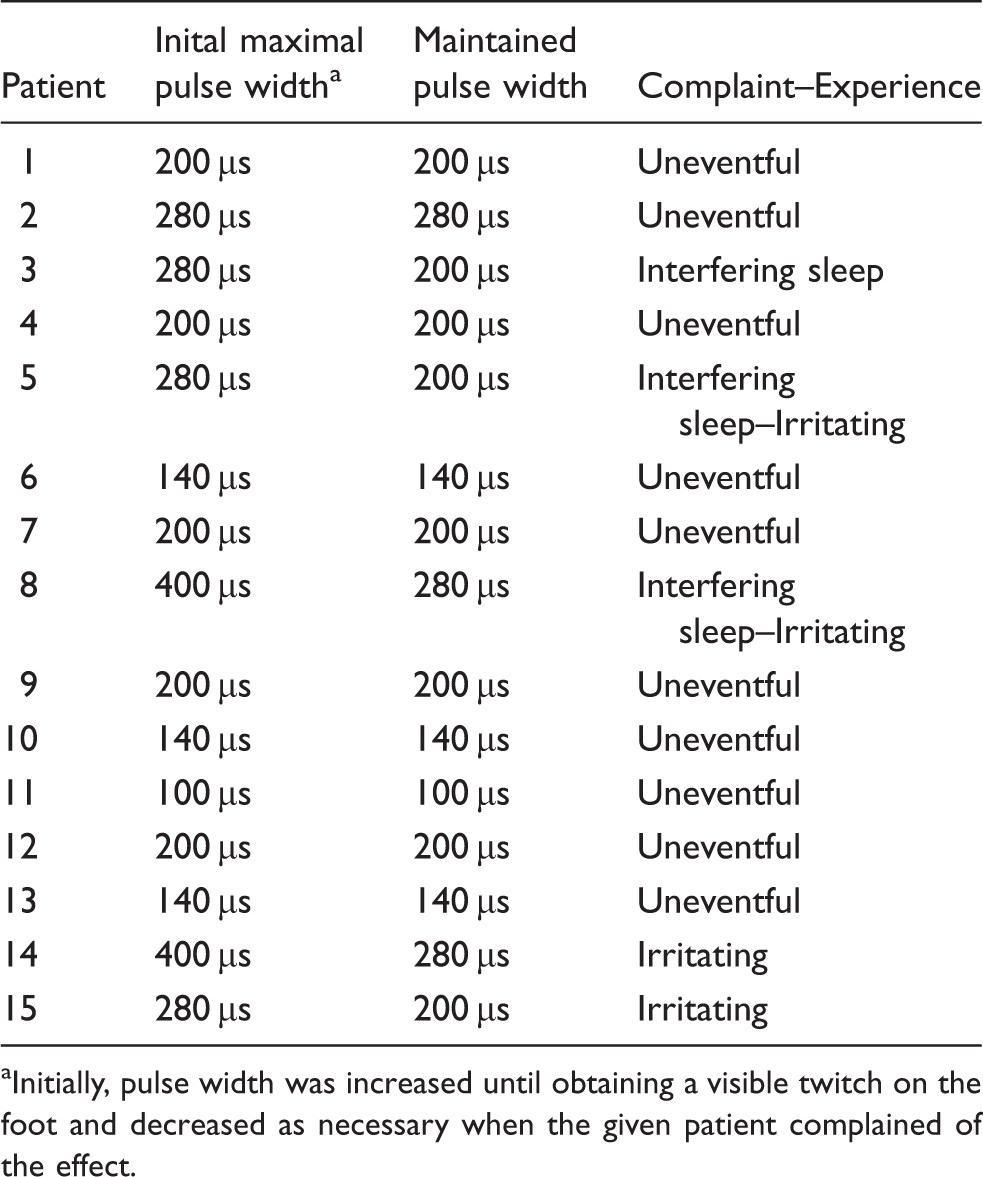
Initially, pulse width was increased until obtaining a visible twitch on the foot and decreased as necessary when the given patient complained of the effect.
None of the patients had clinical symptoms or ultrasound findings of VTE postoperatively. Overall, time of hospital stay did not differ between two groups.
Based on the significant difference we found in mean and standard deviations of peak blood flow velocity in the femoral vein between two groups (17.46 ± 2.86 vs. 13.84 ± 3.58, p = 0.02 for electrostimulation and control group, respectively), we estimate that any further study should include a total of 22 patients in each group to reach 0.95 power level (1-beta) and 31 patients in each group to reach 0.99 power level (1-beta) with an alpha error level of 0.05.
Discussion
Using a novel electrostimulation device producing pulsed muscle contractions in the leg, our pilot study on a selected group patients undergoing TKR provided that the device (i) could easily be applied to the postoperative patient, (ii) was safe as to be left on patient throughout the ward stay, (iii) was not causing serious discomfort, should its intensity level be adjusted as tolerated, (iv) allowed patients to mobilize effectively when stopped and finally (v) caused measurable increase in peak blood flow velocity in the femoral vein compared to controls. Establishing its availability on orthopedic surgery patients and its potential to decrease venous stasis as well, our study seems to produce a favorable insight to test its effectiveness in future studies, especially in patients with specific risks for developing VTE following orthopedic surgery.
Our study took inspiration from a recent one by Warwick et al. 11 where Geko electrostimulation device was applied to healthy volunteers to test for its potential effect on increasing venous flow. In this study, electrostimulation with the device was performed in an identical way to that we performed and produced a mean increase of 11.5 cm/s and 7.7 cm/s in peak blood flow velocity in the femoral vein blood flow velocity in all postural positions when the lower limb was placed or not placed in a plaster cast, respectively. Although the effect was more profound when the extremity was placed in a cast, the increase noted without casts was also significant to some degree and, to us, deserved attention for potential use in clinical setting.
Similar to ours, there have been several studies using electrical stimulation with different devices in order to improve venous blood flow in the lower limb. Izumi et al. 13 compared transcutaneous electrical nerve stimulation with other ways of mechanical compression including electrical muscle stimulation, IPC, active ankle motion and calf squeeze and found that this technique was as effective as the others in achieving acceleration of venous flow in the lower limb. Hou et al. 14 performed electrostimulation on certain acupuncture points on lower limb and found that venous blood flow increased when Zusanli (ST36) and Taichong (LR3) points were stimulated together. It is interesting that the so-called Zusanli (ST36) acupuncture point just corresponds to the below-knee skin landmark of common peroneal nerve where Geko device is applied.
VTE remains as one of the most important causes of hospital readmission and death after orthopedic surgery. Patient with older age, family history, varicose veins and ischemic heart disease were reported to be at high risk for its occurrence after orthopedic surgery. 4 There have been several studies demonstrating benefit of LMWH regarding effectiveness and safety in prophylaxis. Until 2008, practice recommendations were against the use of additional measures including intermittent compression devices and foot pumps whereas their use was first recommended in 2008, 6 especially in patients with certain comorbidities precluding the prolonged use (at least until discharge to home) of chemical venous thromboembolism prophylaxis. 15
Since in the past, graduated compression stockings have commonly been used in prevention of VTE basically for reducing cross-sectional area of the limb, increase venous blood flow, reduce venous wall distension, and improve valvular function. 16 However, whether these effects can be translated into clinical outcomes in terms of VTE prophylaxis is controversial. Munk et al. 17 reported no clinically relevant effect of using compression stockings in relieving pain and swelling after knee surgery. It is also controversial whether venous blood flow increase with use of compression stockings; Jamieson et al. 18 reported that rate of venous blood velocity increased from 10 cm/s to 13.9 cm/s 30 min after application of stockings in postnatal women whereas Stein et al. 19 found no significant change in common femoral vein blood flow but pointed out a slight increase in popliteal vein flow.
Moreover an earlier study reported that graded compression stockings produced a “reversed gradient” in at least one occasion in 54% of patients, which was also associated with a high rate of occurrence of VTE. 20 In our study, a 35% increase in peak blood flow velocity in the femoral vein was noted in controls. This increase did not reach statistical significance but together with those above, this finding suggests that elastic compression stockings are of use but insufficient in enhancing venous blood flow. The possible explanations of this slight increase we observed in venous blood flow are as follows: (i) external compression might have decreased capillary leak and augmented intravenous volume, (ii) increased emptying of the blood from superficial to deep venous system by circumferential compression of the thigh and leg, (iii) improved patient mobilization after surgery. However, in electrostimulation group, cyclic muscle contractions produced by electrostimulation of the common peroneal nerve might have provided a more effective resistance against capillary leak and further augmented emptying of the superficial blood flow through common femoral vein. Nevertheless, in both groups, use of low molecular heparin is likely to be another important factor improving the venous blood flow in the postoperative period.
It has increasingly been recognized that more than one components of Virchow's triad are simultaneously responsible for development of VTE. Blood rheology is considered as an integral part of the thrombosis pathogenesis and amount of blood flow is known to be a key factor in platelet degranulation and formation of surface active enzyme complexes to initiate and stabilize thrombus.21,22 One study showed that peak blood flow velocity in femoral vein was higher in re-canalized deep venous thrombus than that in healthy subjects and emphasized the eddy blood flow as a risk factor for VTE. 23 These highlight the importance of implementing supplementary means of enhancing blood flow in situations where prophylaxis against venous thromboembolism is necessary. Our study showed that electrostimulation seems to improve venous flow as effectively as external compression stockings or devices but without compromising arterial blood run-off to the distal lower extremity.
Determination of VTE incidence and whether the technique we used provide prevention against its development was not, as an outcome measure, among the objectives of this pilot study. Besides this, in order to ensure investigator blinding, Geko device was stopped and even removed from the leg just before the patients were taken to the ultrasound scanning. Because femoral vein blood flow would be higher while the device is activated, the present study might have underestimated the increase in femoral vein blood flow velocity.
As a conclusion, electrostimulation of the common peroneal using a compact, battery-powered device provided enhanced venous flow in the lower limb and may potentially be of use as a supplementary technique in deep venous prophylaxis following lower limb orthopedic operations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.