
Abstract
Introduction
The patterns of recurrent varicose veins after endovascular ablation of the saphenous veins are not well described.
Methods
The current study describes the ultrasound defined recurrence patterns seen in 58 patients (79 limbs) who returned for evaluation of recurrent varicose veins from a cohort of 802 patients treated with endovenous laser ablation and subsequent sclerotherapy from March 2000 to March 2007 with clinical follow-up until May 2014.
Findings
The most common ultrasound defined recurrence patterns leading to the varicose veins were new reflux in the anterior accessory saphenous and small saphenous veins as well as recanalization of the treated saphenous segment. Neovascularization at the saphenofemoral junction and incompetent perforating veins as the source of the recurrent veins were not seen.
Conclusions
The patterns of recurrence following thermal ablation of saphenous veins are different to those seen after surgery. Specifically, new reflux in other saphenous veins is responsible for most recurrent varicose veins and neovascularity seems to be unusual following endovenous laser ablation.
Keywords
Introduction
Venous insufficiency and varicose veins are common conditions worldwide affecting up to 23% of adults. 1 Recurrent varicose veins are common following ligation and stripping and the newer ablative procedures with various patterns described. The “recurrent varicose veins after surgery study” reported the outcomes from a large cohort of patients treated with ligation and stripping at a number of international centers and demonstrated that 20% of these recurrences originated from saphenofemoral neovascularization, 19% from incorrect junctional ligation, and 55% from perforator reflux. 2
Endovascular ablation has become the preferred method for treatment of varicose veins and includes endovenous laser ablation (EVLA) and radiofrequency ablation. 3 There are few studies published in vascular literature that detail the recurrence patterns after these thermal ablation techniques. A recently published multi-center study in an open source general science journal evaluated 164 patients in a registry with recurrent varicose veins after great saphenous vein (GSV) radiofrequency (RFA) and laser ablation with or without ambulatory phlebectomy. 4 The patterns of recurrence included partial or total recanalization of the GSV in 29%, new saphenous vein reflux in an untreated segment in 14%, new reflux in the anterior accessory saphenous vein (AASV) in 24%, and new small saphenous vein (SSV) insufficiency in 16%. 4 In a trial performed by Rasmussen et al., 5 137 limbs were randomized to EVLA or ligation and stripping, both done with microphlebectomy, and followed for five years. The authors noted recurrent varicose veins in 47% and 55% in the laser and surgical groups, respectively, a difference that was not statistically significant. The recurrences in the EVLA cohort were noted to be from reflux in the AASV (24%), thigh (20%), and calf (16%) perforating veins, GSV (12%), and neovessels at the saphenofemoral junction (SFJ) (8%). In that study, they also noted open refluxing segments of the GSV greater than 5 cm in 17.9% of patients treated with EVLA. 5 However, the authors used a pulsed laser mode at 12 W and did not report the energy used per centimeter of vein or linear endovenous energy density. We know from other studies that higher rates of recanalization were seen when pulsed mode is used and when less than 70 J/cm are used with a diode laser.6,7
The purpose of the current study is to review the recurrence patterns of those patients who returned for treatment of recurrent varicose veins associated with an ultrasound finding of reflux from a cohort of patients treated with EVLA and followed for up to a 14-year period.
Methods
This retrospective review of patients treated with EVLA from January 2000 to December 2008 received approval from our institutional review board. A physician with extensive experience with venous care selected patients for treatment with EVLA. Ablation was performed using an 810-nm laser in pulsed and continuous mode at 10–14 W targeting approximately 100 J/cm using a bare tip fiber (Diomed/Angiodynamics, Latham, NY). 7 The original ablation targeted the entire length of the refluxing saphenous vein, which if needed included treating below the mid calf for the GSV and below the gastrocnemius muscle for the SSV. These patients include among the first to be treated with endovenous laser with their early outcome reported previously. 7
The retrospective chart review collected the following data: patient age, gender, family history of varicose veins, initial clinical stage and pathophysiology, initial procedure, initial vein treated, start point and endpoint of ablation, length of vein treated, watts used, duration of ablation, continuous/pulsed mode, date of first recurrence, and pattern of recurrence. The routine follow-up for patients treated with EVLA during the treatment period included a one-month follow-up visit with Duplex ultrasound assessment, followed by routine subsequent visits for visual liquid sclerotherapy (sodium tetradecyl sulfate 0.3–3.0%, Angiodynamics, Latham, NY) until desired result was achieved. Patients returned for re-evaluation due to recurrent symptoms or veins at their own discretion and were evaluated at that time with Duplex ultrasound to determine their recurrence patterns. The patients from this cohort that returned to our center up to May 2014 were included in the current study.
The Duplex defined patterns of recurrence were divided into new reflux in an accessory or alternate truncal pathway, segmental recanalization of the originally treated vein beyond one-month following ablation, new reflux in the originally treated vein peripheral to the site of initial ablation, reflux from veins emanating from the SFJ, reflux via an incompetent perforating vein, and technical failure of ablation defined as patency in the treated segment within one month of initial EVLA. Due to the small sample size and large number of patients without follow-up data, only descriptive statistics were performed.
Results
During the study period, there were 1159 veins treated in 802 patients with 58 of these patients (79 treated veins) returning for re-evaluation of “recurrent” varicose veins or symptoms. The mean patient age was 46.6 years including 12 men and 46 women. Nearly, all involved limbs had C2–C4 disease in the Clinical, Etiology, Anatomy, Pathophysiology classification scheme. EVLA was performed in 69 GSVs, 5 AASVs, and 5 SSVs. The mean time until the first recurrence visit was 4.14 years including 2 recurrences between 1 and 6 months, 4 recurrences at 6–12 months, 4 recurrences at 1–2 years, 5 recurrences at 2–3 years, 5 recurrences at 3–4 years, 4 recurrences at 4–5 years, and 11 recurrences greater than five years after EVLA. Thirty-eight of the 58 patients who returned with clinical recurrences had further treatment.
The patterns of recurrence included new reflux in the AASV or SSV in 16 patients, recanalization of a segment of the treated vein with recurrent reflux in 14 patients, and new reflux in the treated vein peripheral to the previously ablated vein segment in five patients. Treatment failure as defined by failure within one month of EVLA occurred in three patients. There were no cases of SFJ neovascularity or primary recurrences related to incompetent perforating veins in any of the patients who returned for evaluation. Figure 1 delineates the Duplex defined recurrence patterns.
Number of recurrences by pattern of recurrence during the entire follow-up period. The patterns of reflux are Recanalized Segment of Previously Treated Vein (RSPTV), New Truncal Reflux (new reflux in the GSV, AAGSV, PAGSV, or SSV not previously treated), reflux peripheral to prior EVLA and early recurrence. EVLA: endovenous laser ablation.
During the study period, the patients were treated at 10 W (n = 1), 12 W (n = 36), or 14 W (n = 42) with pulsed mode laser (n = 41) or continuous mode laser (n = 38). Of the patients treated with our currently used protocol of 14 W using continuous mode and a goal of 100 J/cm, 10.5% (4/38) had recanalization of a segment of the treated vein compared to 21% (8/38) when treated with 12 W using pulsed mode. Of the 11 patients that recurred greater than five years after initial EVLA, eight patients had a new refluxing vein and the majority (n = 5) were due to reflux in the AASV, as shown in Figure 2. The other new reflux involved the posterior accessory saphenous vein, the posterior circumflex vein, and an external pudendal varicose vein tributary leading to reflux in the vein of Giacomini. There was one recanalization of a treated SSV at 2.6 months following treatment in a patient treated at 12 W in pulsed mode.
Number of recurrences by pattern of recurrence for patients that recurred greater than five years after initial treatment. The patterns of reflux are Recanalized Segment of Previously Treated Vein (RSPTV), New Truncal Reflux (new reflux in the GSV, AAGSV, PAGSV, or SSV not previously treated), reflux peripheral to prior EVLA and early recurrence. EVLA: endovenous laser ablation.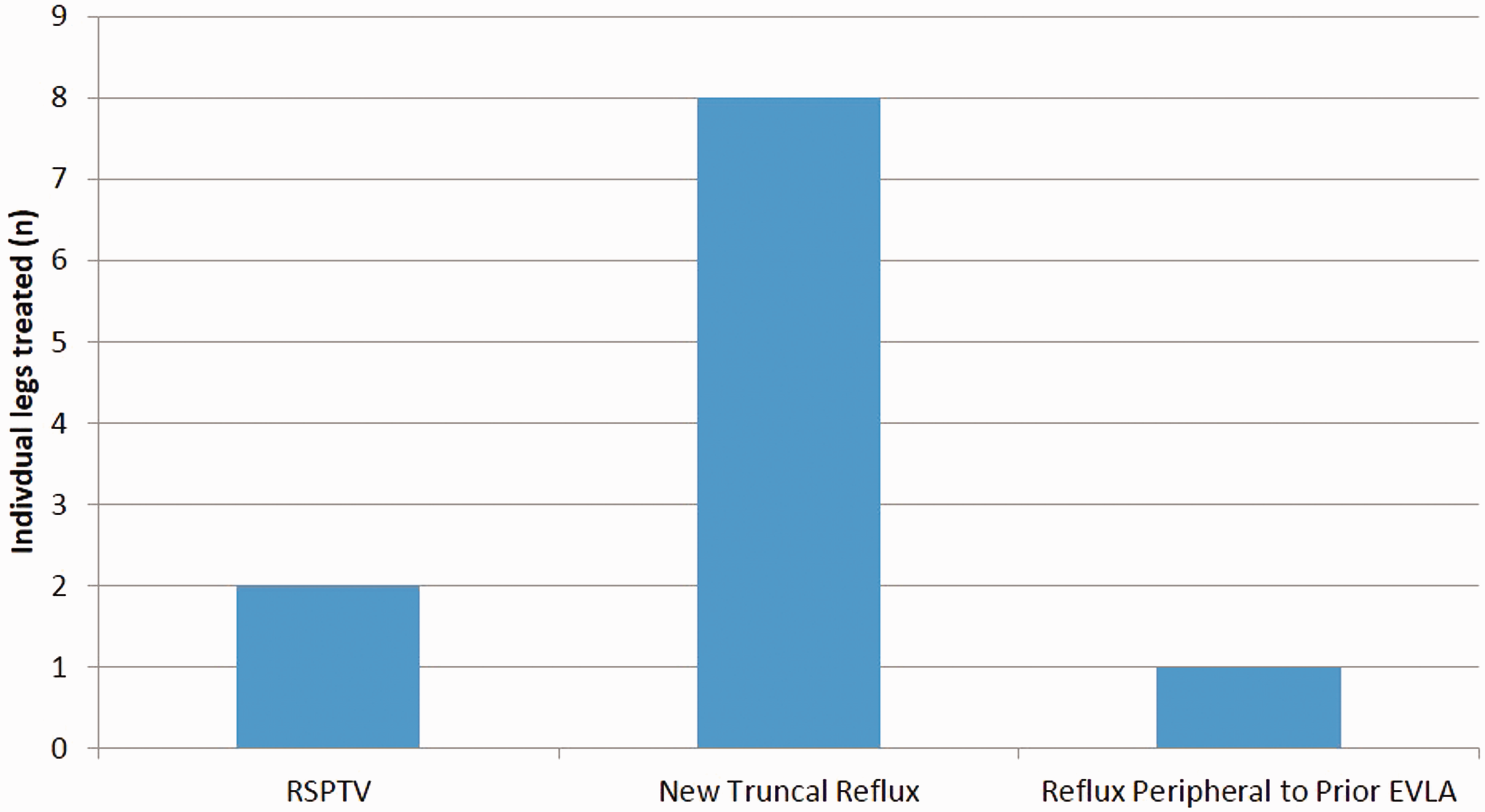
Discussion
The understanding of long-term recurrence rate and patterns of recurrence following EVLA of saphenous veins, introduced 15 years ago, is only now being delineated. In our analysis, the recurrence pattern following endovenous ablation does not involve neovascularization as was seen following ligation and stripping. The majority of cases of recurrence occurred due to recanalization of a segment of a previously treated vein with recurrent reflux or new reflux in an accessory or alternate truncal pathway. This finding is consistent with the findings by Rasmussen et al. 5 showing recurrence following EVLA at five years was predominantly due to recanalization of the previously treated GSV and reflux in the AASV.
Although 14 patients were identified to have recanalization of a segment of the previously treated saphenous vein segment, only 4 of 38 patients who presented for evaluation of recurrent varicose veins were treated with our treatment protocol using 14 W with continuous mode diode laser and 100 J/cm had recanalization. Therefore, the relative incidence of recanalization as a recurrence pattern may be overestimated by our data. This would be due to the predominance of patients in this review being part of the early experience with endovenous ablation when the appropriate energy threshold and delivery mode for reliable venous closure was being determined. The multi-center REVATA study showed that the predominate mechanism of recurrence was ablation failure in their cohort and noted that a disproportionate fraction of these patients treated with laser received less than 60 J/cm, a value known to be less than the threshold for highly successful ablation. 4 Since one- week post-EVLA ultrasounds were not part of the treatment algorithm of the Recurrent Venous disease After Thermal Ablation (REVATA) study, no conclusion can be made regarding the rate of technical failure versus segmental recanalization in patients who had early patency after prior ablation. However, such early recurrence of reflux and patency is nearly all related to inadequate energy delivery regardless if the vein was closed at one week or not.
All visible varicose veins were eliminated prior to conclusion of the “primary treatment” of laser and subsequent sclerotherapy and, therefore, recurrences in our single operator study are new varicose veins. The patients in the multi-institutional REVATA study who presented with recurrent varicose veins had been treated with thermal ablation with some undefined fraction also having microphlebectomy. Other physicians initially treated 18% of patients and the degree to which the original varicose veins were eliminated following the original procedure is not apparent in the report. As such, some of the “recurrences” in REVATA may include untreated or incompletely treated primary varicose veins.
The majority of recurrences in the current study were due to new reflux in an untreated AASV and SSV or segmental recanalization of the treated saphenous segment, which correlates with the findings of the REVATA trial and the five-year follow-up of the trial by Rasmussen et al. 5 Our data found new reflux in the untreated segment below the original ablation in only 6% of the 79 limbs evaluated. This is compared favorably with the 14% found in the REVATA trial. Our low rate may reflect the fact that the entire refluxing segment of saphenous vein was treated during the original ablation, regardless of how low the treatment needed to go. The lowest end of ablation in the REVATA trial was not standardized or reported.
Limitations of our study include the small sample size due to the retrospective nature of the study lending itself to only review the charts of patients who returned to our center for evaluation of reappearing or symptomatic varicose veins. Patients who had recurrences and sought treatment at other facilities or managed them conservatively could not be tracked in the current study. This precludes the ability to determine a true percent recurrence following GSV ablation with endovenous laser. Finally, we report no recurrences primarily caused by an Incompetent Perforator Vein (IPV) identified on Doppler ultrasound in our review. This may in part reflect the fact that small incompetent perforator veins were not aggressively sought for in our Doppler ultrasound evaluation based on our experience that subsequent treatment choices are rarely affected by small IPV presence in C2–C4a patients.
In conclusion, after the initial use of endovascular GSV ablation with an 810-nm diode laser, long-term recurrence is most commonly due to new truncal reflux rather than recanalization of a treated segment or from SFJ neovascularity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.