
Abstract
Objectives
Mechanochemical endovenous ablation is a novel technique for the treatment of great saphenous vein and small saphenous vein incompetence which combines mechanical injury of the endothelium with simultaneous infusion of liquid sclerosant. The main objective of this study was to evaluate early occlusion.
Methods
All consecutive patients who were eligible for the treatment with mechanochemical endovenous ablation were included. Inclusion period was from the introduction of the device in the hospitals (September 2011 and December 2011) until December 2012.
Results
A total of 449 patients were included representing 570 incompetent veins. In 506 treated veins, duplex ultrasonography was performed at follow-up: 457 veins (90%) were occluded at a follow-up of 6 to 12 weeks. In univariate and multivariate analysis, failure of treated great saphenous vein was associated with saphenofemoral junction incompetence (OR 4; 95% CI 1.0–17.1, P = 0.049).
Conclusions
The Clarivein device proves to be safe and had a high short-term technical effectiveness.
Keywords
Introduction
During the last decade, various types of minimally invasive procedures, including endovenous laser ablation (EVLA) and radiofrequency ablation (RFA), have been introduced for the treatment of the great saphenous vein (GSV) and the small saphenous vein (SSV) incompetence.1,2 Most of these techniques show high success rates, even up to 95.4% for EVLA at 5-year follow-up. 3 However, they are based on delivering high doses of thermal energy to the vein wall and require the use of tumescent anesthesia, administered through ultrasound-guided injections in the limb, which is time-consuming and often painful. Even with the tumescent anesthesia, thermal-associated complications, for example pain and skin burn are described. Another complication is injury of the sural nerve, which can be seen in surgical stripping and endovenous thermal ablation of the SSV. 4
Several studies using ultrasound-guided foam sclerotherapy (UGFS) were performed to obviate the need of tumescent anesthesia; however, these studies showed higher complication rates and lower occlusion rates than endothermal ablation.5,6
Recently, a new mechanochemical endovenous ablation (MOCA) method was introduced using the Clarivein device (Vascular Insights, Madison, CT, USA). This technique combines mechanical injury of the endothelium with simultaneous infusion of liquid sclerosant (sodium tetradecyl sulphate). 4 In contrast to RFA and EVLA the MOCA procedure is performed without the use of tumescent anesthesia, resulting in lesser pain and a shorter procedure time. 7 The main objective of our study was to evaluate the early occlusion rate of treated veins. Another aim was to evaluate complications.
Methods
Patients
An observational study was performed in two teaching hospitals in The Netherlands: Onze Lieve Vrouwe Gasthuis (OLVG) and Rode Kruis Ziekenhuis (RKZ). All consecutive patients who were eligible for treatment with MOCA were included. Inclusion period was from the introduction of the device in the hospitals (OLVG September 2011 and RKZ December 2011) until December 2012.
Inclusion criteria were: symptomatic incompetent GSV of more than 30 cm or incompetent SSV of more than 10 cm of the vein, with or without saphenofemoral or -popliteal junction incompetence, patients over 18 years of age. Exclusion criteria were: asymptomatic incompetent GSV or SSV, diameter of the vein <3 mm or >12 mm, pregnancy.
Primary outcome was occlusion of the treated vein at follow-up. Follow-up was at six weeks in OLVG and at three months in RKZ. Secondary outcomes were peri- and postoperative complications.
Data were obtained from operative and outpatient records. The following demographic data were collected: gender, age, co-morbidity (cigarette consumption, hypertension, cardiovascular disease, diabetes mellitus, history of deep venous thrombosis).
Furthermore, Clinical-Etiology-Anatomy-Patho-physiology (CEAP) classification, duplex ultrasonography results and former varicose vein treatment were registered.
Duplex examination
Preoperative
In all patients in upright position inflatable cuffs were attached above both ankles to stimulate anterograde venous flow. With duplex ultrasonography venous flow was evaluated. Incompetence was defined as retrograde flow lasting for more than 0.5 s.
Postoperative
In all patients in upright position the treated veins were evaluated with duplex ultrasonography. Occlusion was defined as 80% or more obliteration of the total length of the treated segment of the vein. The vein had to be incompressible and without flow; if treated areas were patent but not refluxing, this was considered as failure.
Technique
The MOCA technique exists of mechanical agitation of the vessel endothelium by a rotating catheter tip starting 1 cm distal from the saphenofemoral or -popliteal junction. A sclerosant drug is sprayed from the tip of the catheter (0.2 cc/cm) as it is pulled back through the vein at a rate of 1 cm in 7 s. In both hospitals, all consecutive patients who were eligible for treatment with the Clarivein device using polidocanol (2% in the proximal 10 cm of the vein, 1.5% in the distal part of the vein with a maximum of 2 mg/kg) as sclerosans for incompetence of the GSV or SSV were included.
Statistical analysis
A chi-square test was performed to determine any association between occlusion and the other possible predictive variables. A 2-tailed T-test was used with regard to continuous variables. For all variables that were possibly associated with occlusion (significance was set at P ≤ 0.1), a multiple regression analysis was performed with occlusion as dependent variable (significance was set at P ≤ 0.05). For all statistical analyses, IBM SPSS Statistics version 20.0 was used. The GSV and SSV were analysed separately.
Results
Baseline characteristics.
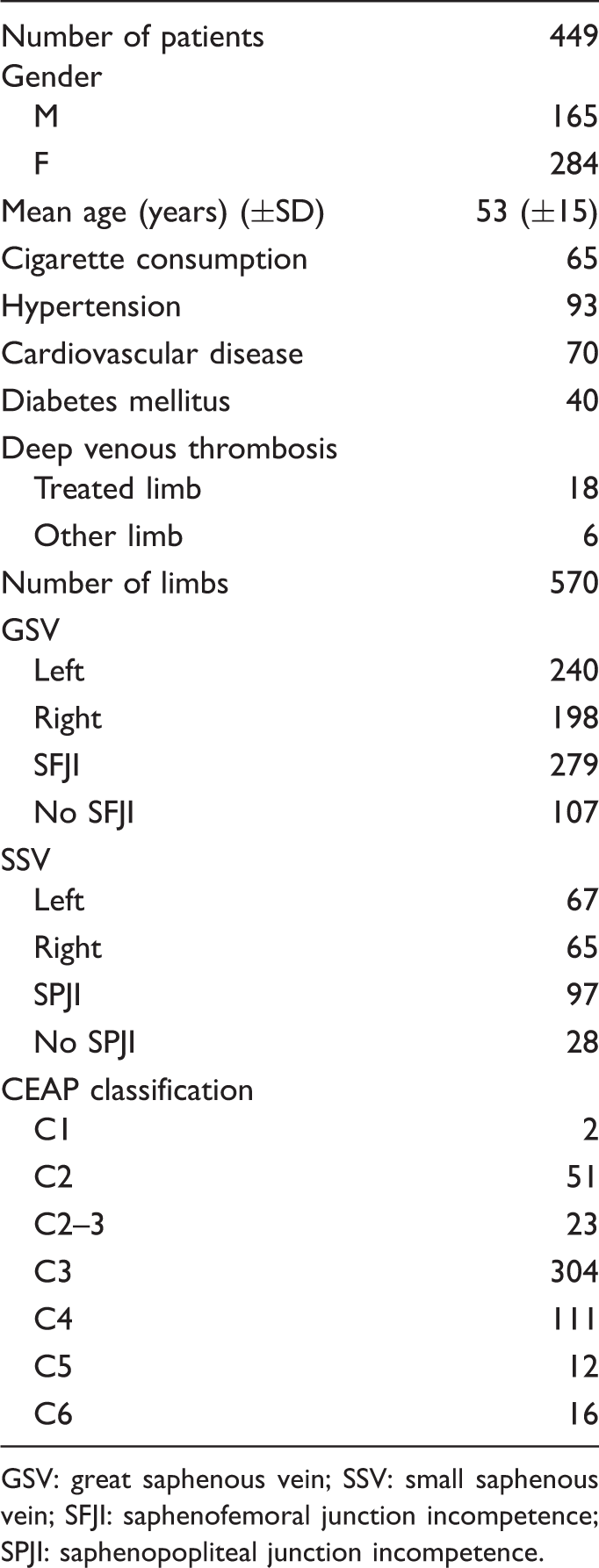
GSV: great saphenous vein; SSV: small saphenous vein; SFJI: saphenofemoral junction incompetence; SPJI: saphenopopliteal junction incompetence.
The procedure could not be performed in 12 cases because the vein was too small to be punctured (7), the vein could not be canalised due to kinking (2) or the vein was already obliterated (2) or no incompetent veins could be identified with duplex ultrasonography (1) contrary to the results of the duplex ultrasonography at the moment of inclusion. In total, 558 limbs were treated. Median follow-up time was 54 days (range 12–266 days) (OLVG 46 days and RKZ 96 days).
Thirty-five patients were lost to follow-up; reasons were unclear. In 17 cases no duplex ultrasonography was performed at follow-up; these patients were unwilling to undergo postoperative duplex ultrasonography as they were satisfied and free of complaints, and based on physical examination the procedure was deemed to be successful.
Occlusion
In 506 treated veins, a duplex ultrasonography was performed at follow-up to determine if occlusion of the treated vein was achieved. In 457 cases (90%) the treated varicose vein was occluded. In 49 cases (10%) no occlusion was accomplished. The occlusion rate for only GSV was 92% versus 84% for SSV. Occlusion rates for the two hospitals separately, i.e. at six weeks follow-up versus three months follow-up, were 92% versus 87% (P = 0.063). Subsequently, for GSV and SSV separately, occlusion rates were: GSV at six weeks 94.5% and at three months 89% (P = 0.047); SSV at six weeks 85% and at three months 80.5% (P = 0.52).
Univariate analysis of variables on occlusion.

GSV: great saphenous vein; SSV: small saphenous vein; SFJI: saphenofemoral junction incompetence; SPJI: saphenopopliteal junction incompetence.
Multivariate analysis of risk factors on treatment failure for great saphenous vein (GSV).
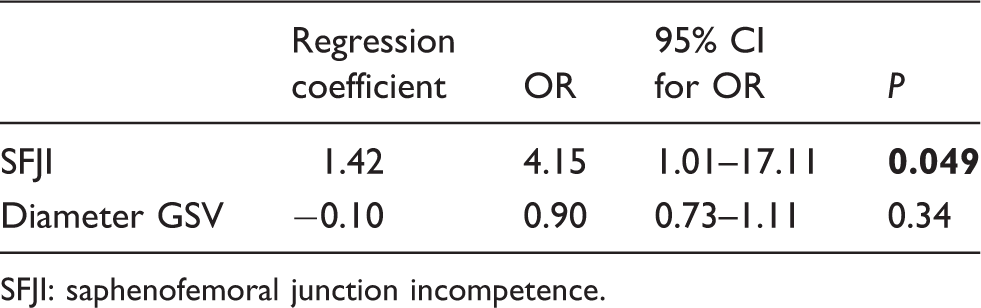
SFJI: saphenofemoral junction incompetence.
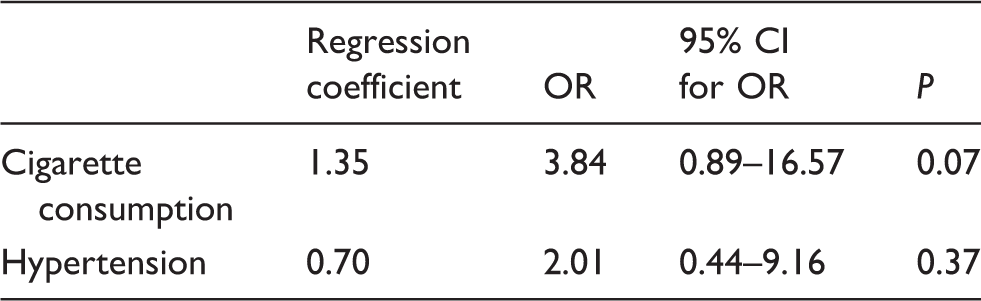
Multivariate analysis of risk factors on treatment failure for small saphenous vein.
Complications
No perioperative complications were reported. The most frequent postoperative complication was thrombophlebitis of the treated limb, which was seen in 12 patients. In most of the cases the thrombophlebitis was located in the varicose tributaries besides and below the treated trunk. In some cases it was only located in the trunk of the GSV or SSV below the treated area. Six patients had complaints of a painful and erythematous extremity. Two patients suffered from pulmonary emboli after the treatment. In both patients no special circumstances were noted that could have contributed to causing the pulmonary emboli. One patient suffered from dyspnea one week after MOCA treatment, and on CT-scan, pulmonary emboli were seen in the right lung. He was admitted for one night and was treated with coumarins. The other patient presented with a painful swollen limb and dyspnea one month after treatment. On CT-scan, pulmonary emboli were found in both lungs and duplex ultrasonography revealed deep venous thrombosis in the popliteal and femoral vein of the treated limb. He received treatment with coumarins as well and was admitted for one night. Both patients did not suffer from any sequelae fortunately. Deep venous thrombosis occurred postoperatively in one other patient as well three weeks after treatment and was located in the popliteal vein. The patient was treated with coumarins for three months, and duplex ultrasonography at six months after MOCA treatment showed that the popliteal vein was no longer occluded and patient had no sequelae. There was one patient with injury of the sural nerve after treatment resulting in transient hyperesthesia. This patient already suffered from sensory sural neuropathy after previous saphenopopliteal junction ligation, which was aggravated by the MOCA treatment. Other postoperative complications were: blister (1), abscess at puncture site (1) and hematoma at puncture site (1).
Discussion
This is one of the largest observational series reporting on early outcomes of treatment with the MOCA technique showing to be effective and feasible. As reported in other studies, endovenous ablation techniques show high closure rates for obliterating incompetent GSV and SSV. With regard to our primary endpoint, the occlusion rate of treatment with the MOCA technique was 90% in this study for GSV and SSV together and 92% versus 84% for GSV and SSV separately.
The occlusion rate of GSV that we found is comparable to a prospective Dutch study with 30 limbs that were treated with the Clarivein device and showed complete occlusion in 87% of the patients at six weeks follow-up. This study only included patients with GSV incompetence. 8 Another prospective Dutch study included 50 patients with SSV incompetence and showed an occlusion rate of 100% at six weeks follow-up and 94% one year after treatment with the Clarivein device. Another study carried out in the USA showed a closure rate of 96.7%. 1 In this study, 1.5% liquid sodium tetradecyl sulphate (Sotradecol) was used as sclerosant, which is not available in the Netherlands. We believe that a higher dose of polidocanol could result in even better occlusion rates. In the ongoing studies in the Netherlands (the ‘Maradona trial’, 9 ‘Dose finding study’ 10 and the ‘Messi trial’ 11 ) a higher dose is used. The answer will come from the ‘Dose finding study’ designed to answer this question. However, based on our results we changed our protocol and now use 3% sclerosant instead of 2% in the proximal segment of the vein.
With regard to follow-up, we found a difference in occlusion rate for GSV of 5.5% in favour of six weeks follow-up compared with three months follow-up. An explanation for this difference could be that in a remarkable number of occluded veins, recanalisation occurs after six weeks. However, long-term results are needed to find out if increased recanalisation occurs over time.
Comparing our results regarding the early occlusion rate with results of other endovenous techniques, we see different results; a randomised controlled trial with 159 patients comparing treatment of incompetent GSV with RFA versus EVLA showed an occlusion rate after treatment with the VNUS closure device of 97% at three months follow-up. For EVLA, the occlusion rate at three months was 96%. 12 A meta-analysis incorporating incompetent GSV and SSV showed occlusion rates of 93% and 89% at three months follow-up for EVLA and RFA, respectively, which are quite similar to our results with the MOCA technique. 3
The only factor that was associated with treatment failure in our series was saphenofemoral junction incompetence. An explanation for this finding could be that the incompetent valve results in higher pressure in the venous system and therefore results in recanalisation. In our series in 64% of the patients with incompetent GSV it was combined with saphenofemoral junction incompetence. One might argue that MOCA should not be performed in these patients based on our results. However, because MOCA is very fast and painless, we think in patients with saphenofemoral junction incompetence the procedure should be performed. It could be that when higher doses of sclerosant are used, this difference in occlusion between saphenofemoral junction incompetence and competence will not be found. We have to wait for the results of the ‘Dose finding study’ to see whether higher doses will result in better occlusion rates in patients with saphenofemoral junction incompetence.
The diameter of the vein was not significantly associated. As we use a vein diameter of more than 12 mm as an exclusion criterion for endovenous treatment, a definitive conclusion cannot be made. However, one can argue that a larger vein, up until 12 mm in diameter, is not a contraindication for treatment with MOCA. As for our secondary outcome, complications occurred in 25 patients (4.5%). In four patients, there were major complications (pulmonary emboli, deep venous thrombosis, sural nerve injury). The studies mentioned above only showed minor complications as superficial phlebitis, ecchymosis and induration at the puncture site (30%, 38% and 10%, respectively). However, all these studies included only a small number of patients.1,4,8 The most frequent complication observed in our study, thrombophlebitis, which was reported in 12 patients (2%), is acceptable when compared to other studies. A systematic review reported thrombophlebitis in 2.8%–12.7% after EVLA and 0%–10.6% after RFA. 13
If our technical results for SSV are consistent, future patients should be informed that the occlusion percentage is not as high as in thermal procedures and has to be balanced against the improved patient’s benefits.
This study has several limitations. First of all, the data were analysed retrospectively. Furthermore, in 52 cases the patient was lost to follow-up or did not have a duplex ultrasonography at follow-up, which accounts for 10% of the total population. Finally, these results only represent the short-term outcomes, and long-term occlusion rates will have to be awaited to gain more information about the efficiency of MOCA in the long-term.
The success of treatment with thermal endovenous modalities remains slightly higher in the short-term. However, the MOCA technique obviates the use of tumescent anesthesia which is of great advantage for the patient in terms of pain. Furthermore, not administering tumescent anesthesia simplifies the procedure and reduces procedure time.
More prospective studies have to be performed, inter alia to determine the optimal dose of sclerosans used for the mechanochemical ablation for even better results of varicose vein treatment and with a prolonged follow-up time to determine efficacy in the long-term.
In conclusion, the MOCA technique shows to be effective and safe for treatment of incompetent GSV and SSV with an occlusion rate of 90%, which is similar to other studies using the MOCA technique, as well as to the results of the meta-analysis of other endovenous modalities. Long-term studies, as well as randomised trials are necessary to provide data on the real value of this technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.