
Abstract
Objectives
To conduct economic evaluations of radiofrequency ablation, ultrasound-guided foam sclerotherapy and surgery for great saphenous vein ablation.
Method
A cost-utility and cohort analysis from societal perspective was performed to estimate incremental cost-effectiveness ratio. Transitional probabilities were from meta-analysis. Direct medical, direct non-medical, indirect costs, and utility were from standard Thai costings and cohort. Probabilistic sensitivity analysis was performed to assess parameter uncertainties.
Results
Seventy-seven patients (31 radiofrequency ablation, 19 ultrasound-guided foam sclerotherapy, and 27 surgeries) were enrolled from October 2011 to February 2013. Compared with surgery, radiofrequency ablation costed 12,935 and 20,872 Baht higher, whereas ultrasound-guided foam sclerotherapy costed 6159 lower and 1558 Bath higher for outpatient and inpatient, respectively. At one year, radiofrequency ablation had slightly lower quality-adjusted life-year, whereas ultrasound-guided foam sclerotherapy yielded additional 0.025 quality-adjusted life-year gained. Because of costing lower and greater quality-adjusted life-year than other compared alternatives, outpatient ultrasound-guided foam sclerotherapy was an option being dominant. Probabilistic sensitivity analysis resulted that at the Thai ceiling threshold of 160,000 Baht/quality-adjusted life-year gained, ultrasound-guided foam sclerotherapy had chances of 0.71 to be cost-effective.
Conclusions
Ultrasound-guided foam sclerotherapy seems to be cost-effective for treating great saphenous vein reflux compared to surgery in Thailand at one-year results.
Introduction
Varicose veins (VVs) affect up to 20–30% of adults1,2 in which great saphenous vein (GSV) is the most common site of venous reflux worldwide, including Thailand. 3 Endovenous procedures are emerging which include endovenous laser ablation (EVLA), radiofrequency ablation (RFA), and ultrasound-guided foam sclerotherapy (UGFS). Compared to the standard surgery (i.e. saphenofemoral ligation and GSV stripping), these procedures are associated with less post-operative pain, fewer complications (e.g. wound infection, and hematoma) and shorter times for return to normal activities with similar efficacy for RFA and EVLA but less efficacy for UGFS. 4 However, UGFS has a lower cost, safety and can also be easier to repeat. As a result, these endovenous procedures have become increasingly popular. There has been a threefold increase in patients undergoing sclerotherapy and almost a doubling of endovenous procedures being performed in the United Kingdom (UK). 5
A cost-effectiveness analysis in UK has shown that day case surgery of EVLA and RFA is likely to be cost-effective. 6 However, this conclusion may not be generalisable to other settings, especially in developing countries like Thailand, due to the differences in health and economic infrastructures. Currently, the costs for VV surgery and UGFS are reimbursable by the Thai Universal Health Coverage scheme but not for RFA and EVLA. The latter may be explained by the lack of evidence to justify the increased costs of RFA and EVLA to the Thai health-care system. Therefore, this cost-utility analysis was conducted to assess costs and consequences of RFA, UGFS, and surgery to inform health benefit package development in Thailand.
Methods
Model
The study was conducted according to the Thai Health Technology Assessment Guidelines
7
with ethical approval by research committees of Thammasat University, Ramathibodi, and Chonburi hospitals. A decision tree model was constructed in order to estimate costs and health consequences in terms of quality-adjusted life years (QALYs) of performing three types of interventions (i.e. RFA, UGFS, and standard surgery) (Figure 1). Health consequences included in the model were wound infection and incomplete ablation of GSV (primary treatment failure). This was defined as recanalisation diagnosed by duplex scan for endovenous procedures and incomplete stripping, incomplete removal of an intended vein, or recanalisation for surgery.
4
Other significant different outcomes are post-operative pain, hematoma, and superficial thrombophlebitis were not included in cost estimation because most of them are treated conservatively and already incorporated in the QoL measure.
4
Both outpatient and inpatient management were analysed. Decision to choose inpatient or outpatient management depended on necessary to do concomitant phlebectomy and patient’s preference. Outpatient interventions were done using local tumescent anesthesia with monitored anesthetic care and inpatient interventions used spinal or general anesthesia.
Decision tree analytic model.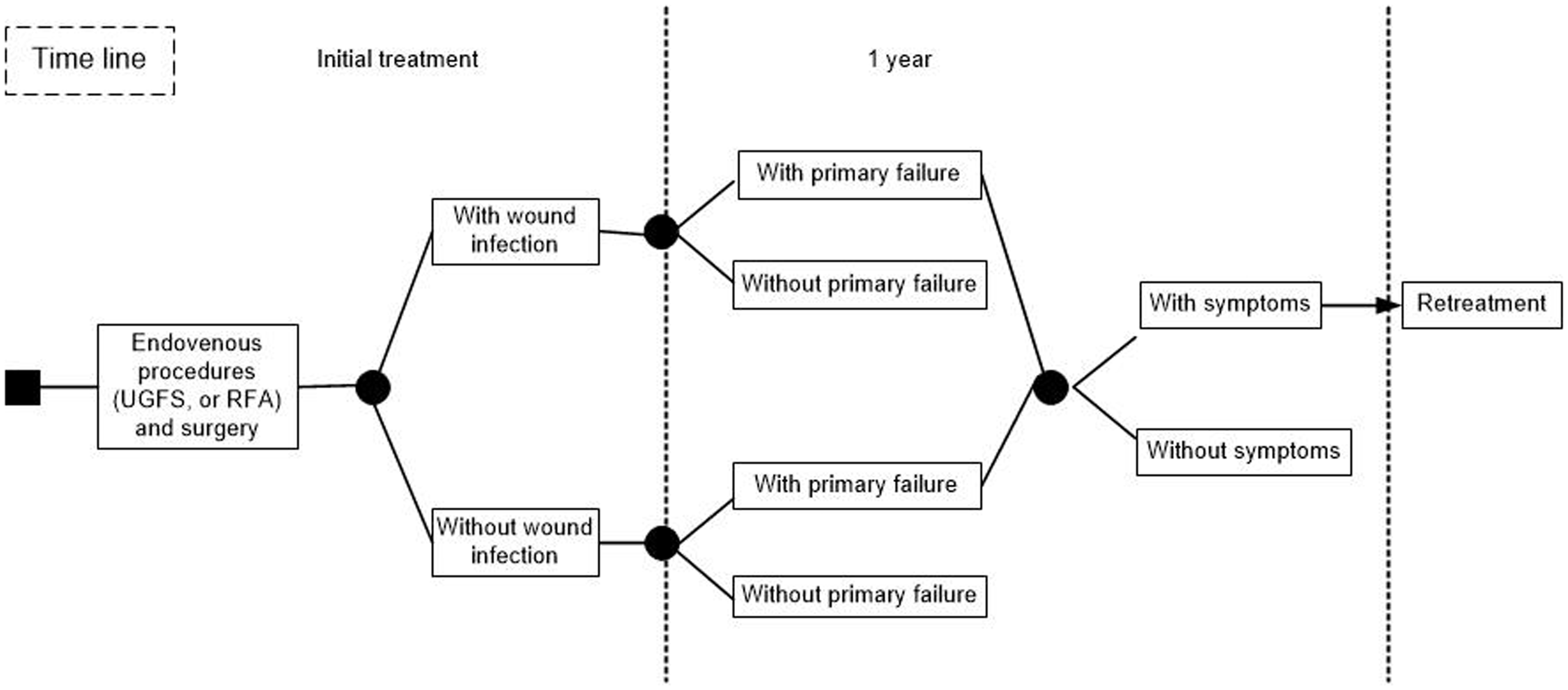
The time horizon was one year due to limited data of long-term outcome in randomized controlled trials (RCTs), which were pooled in the meta-analysis. 4 Primary failure was a surrogate outcome of clinical recurrence 8 and might be symptomatic or asymptomatic. 9 Therefore, it might not be associated with a utility change until there was symptomatic clinical recurrence, when retreatment would be recommended and done by UGFS at one year follow up. 10
Input parameters
Transitional probabilities of wound infection and primary failure
For clinical outcomes, we used results from systematic review and meta-analysis. 4 To prevent biases from different techniques and settings in the pooled studies used in the meta-analysis, 7 the risk ratio was used. The incidence of primary failure and wound infection in the surgery group were taken from data in Thai patients. A transitional probability for each decision tree branch was then calculated by multiplying incidence of events in the surgery group from the cohort with the pooled risk ratio. 4 The proportions of primary failure with symptoms at one year were assumed to be the same as those obtained by Shadid et al. 9
Resources used, costs, and utility
A prospective cohort study was carried out in Thammasat University, Ramathibodi and Chonburi hospitals to collect direct medical costs, non-medical costs (i.e. traveling cost and accommodation for seeking care, and costs of informal care), indirect costs (i.e. productivity loss due to sick leave), and utility data across different types of interventions. Adult patients presenting with VVs with/without ankle edema (Clinical Etiologic Anatomic Pathophysiologic: CEAP class 2, 3) between October 2011 and February 2013 were enrolled if they met all of the following criteria: (i) had isolated unilateral GSV reflux diagnosed by duplex scan, (ii) had no history of deep vein thrombosis or superficial thrombophlebitis, (iii) had no peripheral arterial occlusive disease, and (iv) were not pregnant. Patients with reflux in tributaries were not considered. All patients signed informed consent before receiving intervention. Patients were informed about treatment choices (i.e. RFA, UGFS, and surgery), advantages, disadvantages, and cost of each procedure. Decision in choosing treatment procedure was done by patient under suggestion by physicians.
RFA (Covedien ClosureFAST™, San Jose, California, USA) was performed with tumescent anesthesia begun at 2–3 cm distal to saphenofemoral junction to GSV at knee. One session of UGFS was done with saphenofemoral ligation.11,12 Foam sclerosant (Tessari’s technique; 1 cc of 1% Aethoxysklerol mixed with 3 cc of air) about 6–8 cc was injected to the GSV just below the knee. Surgery was done with saphenofemoral ligation with invagination stripping to GSV just below the knee.
The EuroQol (EQ) 5D™, which has been validated in Thailand, was used to measure health-related QoL and utility score. 13 Utility was measured pre-intervention (U0), at one to two weeks (U1), one month (U2), and six months (U3) post-intervention. Post-intervention utility gained at a given time was calculated by subtracting utility at that time with pre-intervention utility (i.e. utility gain at one to two week = U1–U0). For each individual patient, utility gain at one week, one month, and six months were, respectively, accounted for 0.5 month (1/24 = 4.2%), 0.5 month (4.2%), and 11 months (11/12 = 91.6%) from a one-year time horizon. The utility of wound infection was accounted for within two weeks because wound infections have generally healed within this time. Primary failure without symptoms was not considered to affect to the utility. However, primary failure with symptoms was considered to have utility equal to patients with GSV reflux, which accounted for 11 months in a one-year time horizon.
Statistical analysis
Baseline characteristics, clinical outcomes, and costs for the Thai cohort were described using mean with standard deviation and frequencies. Baseline characteristics and outcomes were compared between intervention groups using Chi-square test for categorical data, and one-way ANOVA (or quantile regression analysis when non-normal distribution was found) for continuous data. A multivariate linear (or quantile where appropriate) regression analysis was applied to assess the relationship between intervention groups and outcomes. Covariables that were significantly associated with the outcomes were also included in the regressive model. Analyses were performed using STATA version 11.0. A p-value of less than 0.05 was considered statistically significant.
Cost-utility analysis was conducted based on a societal perspective by comparing RFA or UGFS to surgery. The incremental cost-effectiveness ratios (ICERs) were estimated to inform additional costs per one QALY gained. One intervention was claimed to be dominant over another intervention if it had lower cost but higher QALY, or it was dominated if it had higher cost but lower QALY. An intervention was cost-effective if its estimated ICER was lower than 160,000 Baht per QALY (a Thai cost-effectiveness threshold). 14 For the reason to inform health benefit package development, the minimum daily wage of 300 Baht per day in Thailand was used.
A probabilistic sensitivity analysis was conducted to examine uncertainty of estimated ICERs using a Monte Carlo simulation with a 1000-replication bootstrap. Probabilistic results were plotted as a cost-effectiveness acceptability curves. The proportion of ICERs that were lower than cost-effectiveness threshold demonstrated probability of that intervention to be cost-effective at that threshold, which would be demonstrated as the cost-effectiveness acceptability curve in which Y axis is the probability of each intervention to be cost-effective and X axis is a value of ceiling ratios. 15 All cost analyses were performed using user-own written commands in Microsoft Excel 2010. 16
Results
Baseline characteristics and outcomes between endovenous and surgery groups.
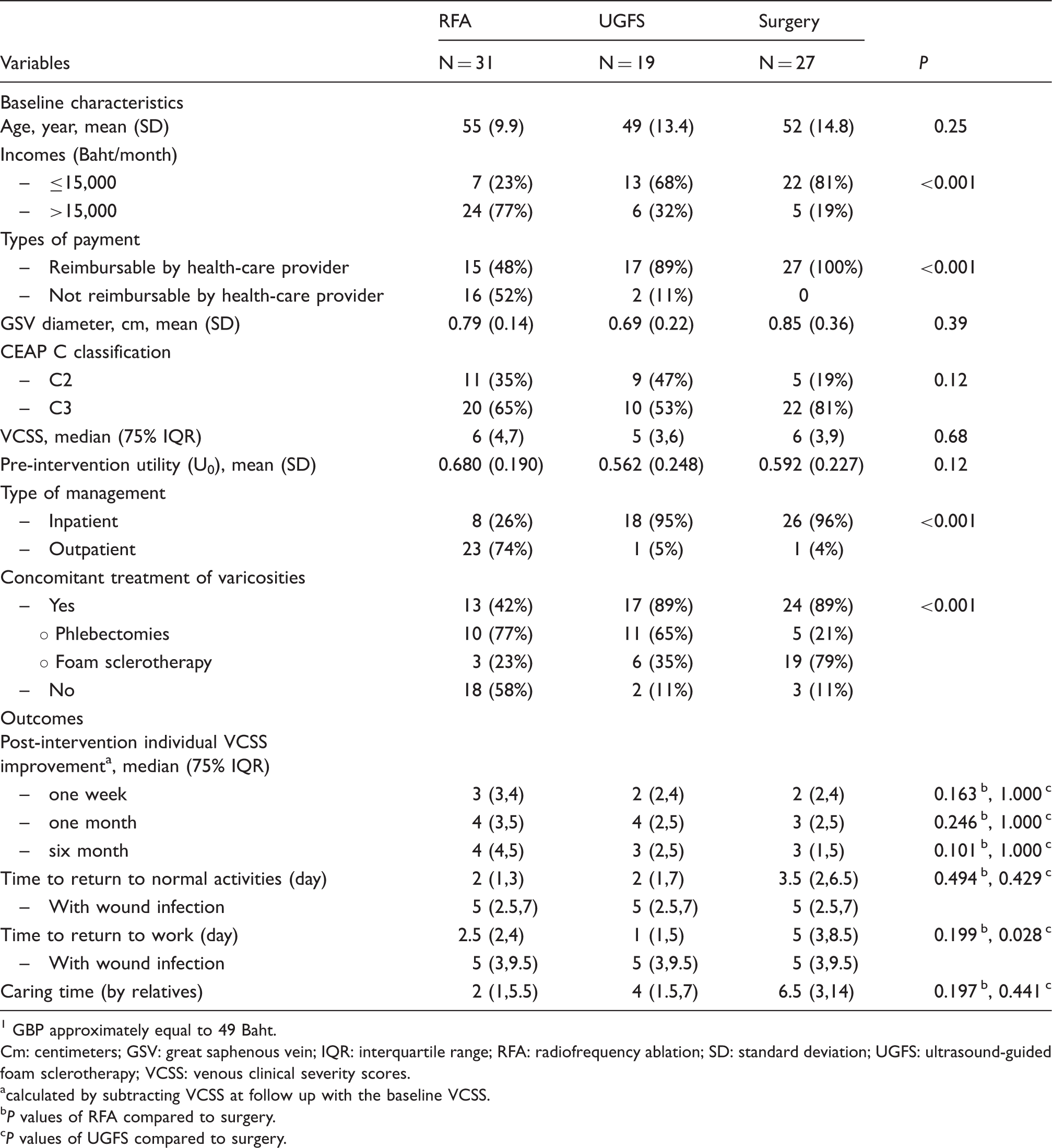
GBP approximately equal to 49 Baht.
Cm: centimeters; GSV: great saphenous vein; IQR: interquartile range; RFA: radiofrequency ablation; SD: standard deviation; UGFS: ultrasound-guided foam sclerotherapy; VCSS: venous clinical severity scores.
calculated by subtracting VCSS at follow up with the baseline VCSS.
P values of RFA compared to surgery.
P values of UGFS compared to surgery.
Input parameters for cost-utility analysis.

IQR: interquartile range; NA: not applied; RFA: radiofrequency ablation; RR: relative risk; SD: standard deviation; UGFS: ultrasound-guided foam sclerotherapy.
GBP approximately equal to 49 Baht.
Health Intervention and Technology Assessment Program (HITAP) (http://www.hitap.net/costingmenu).
P values of RFA compared to surgery.
P values of UGFS compared to surgery.
For direct medical costs, data on resources used was multiplied by unit costs identified from a standard costing menu. 17 Procedural-related costs were significantly higher in: (i) RFA (26,417 Baht) compared to UGFS (5,556 Baht) and (ii) surgery (5096 Baht), (p < 0.001), see Table 2. These included cost of intraoperative ultrasound (1417 Baht 17 ), catheter and generator (21,000 Baht), and operative theater fee (4000 Baht 17 ) for RFA; intraoperative ultrasound (1417 Baht 17 ), Aethoxysklerol (139 Baht), and operative theater fee (4000 Baht 17 ) for UGFS; and standard costs for saphenofemoral ligation with stripping (5096 Baht 17 ) for surgery.
Utility gained for each individual at each time has been shown in Figure 2 and Table 2. At one to two week post-intervention, RFA seemed to have higher utility gained, but it was diluted later and became to be similar to UGFS and surgery at one and six months post-intervention. For those four patients with wound infection, post-operative utility scores at one week, one month, and six months were, respectively, 0.597 (SD = 0.118), 0.905 (SD = 0.191) and 1.000 (SD = 0) with utility gain of 0.047 (SD = 0.430) at one week post-intervention.
Utility gain between procedures.
Probabilistic results of costs, QALYs, incremental cost effectiveness ratios (ICERs) of five options for treating great saphenous reflux in societal perspective.
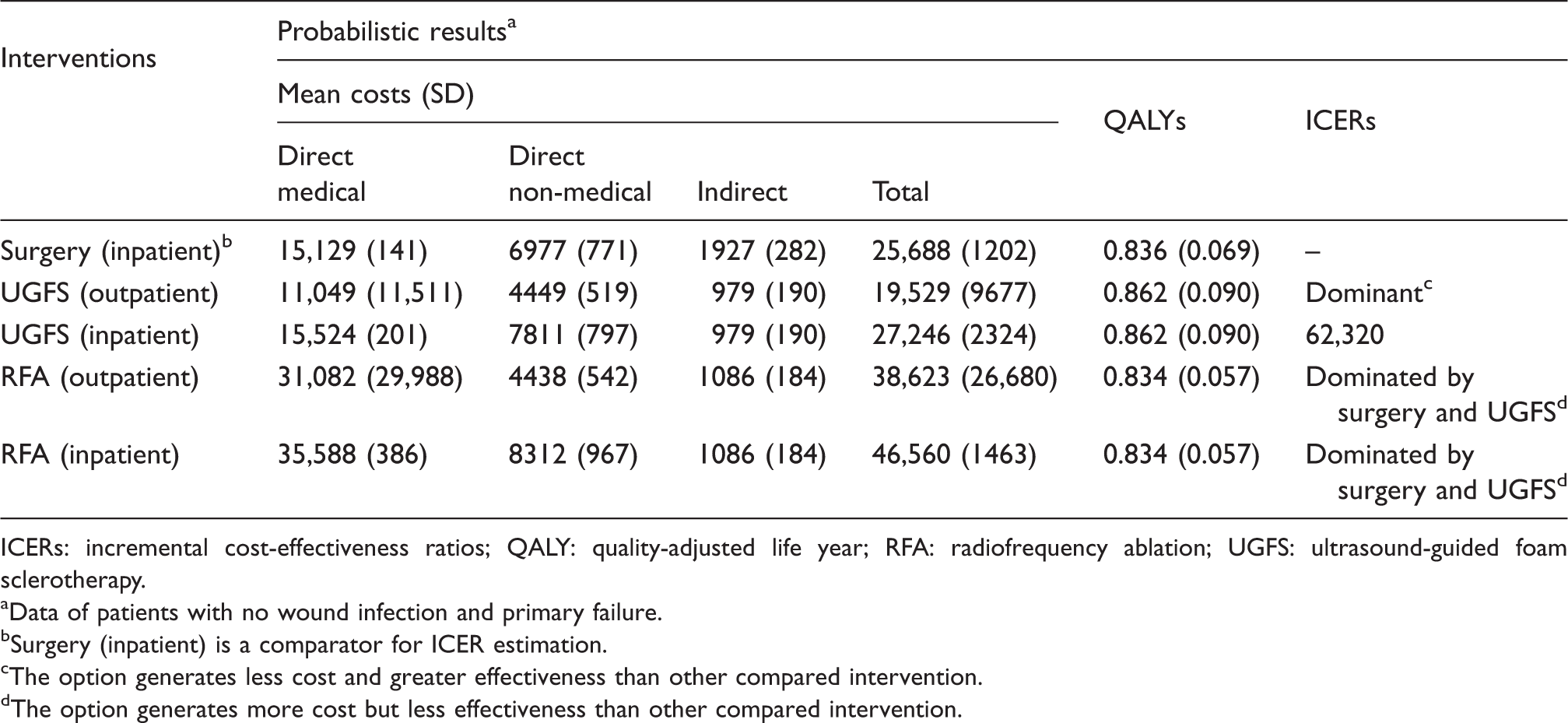
ICERs: incremental cost-effectiveness ratios; QALY: quality-adjusted life year; RFA: radiofrequency ablation; UGFS: ultrasound-guided foam sclerotherapy.
Data of patients with no wound infection and primary failure.
Surgery (inpatient) is a comparator for ICER estimation.
The option generates less cost and greater effectiveness than other compared intervention.
The option generates more cost but less effectiveness than other compared intervention.
The cost-effectiveness acceptability curve has been shown in Figure 3 with demonstrated three options of treatment. At ceiling threshold of 160,000 Baht/QALY gained, RFA and UGFS as outpatient management had the probability of 0.15 and 0.71 to be cost-effective compared to surgery, respectively.
Cost-effectiveness acceptability curves demonstrate the probability that treatment is cost-effective provided at each level of cost-effective threshold (THB/QALY gained) based on societal perspective.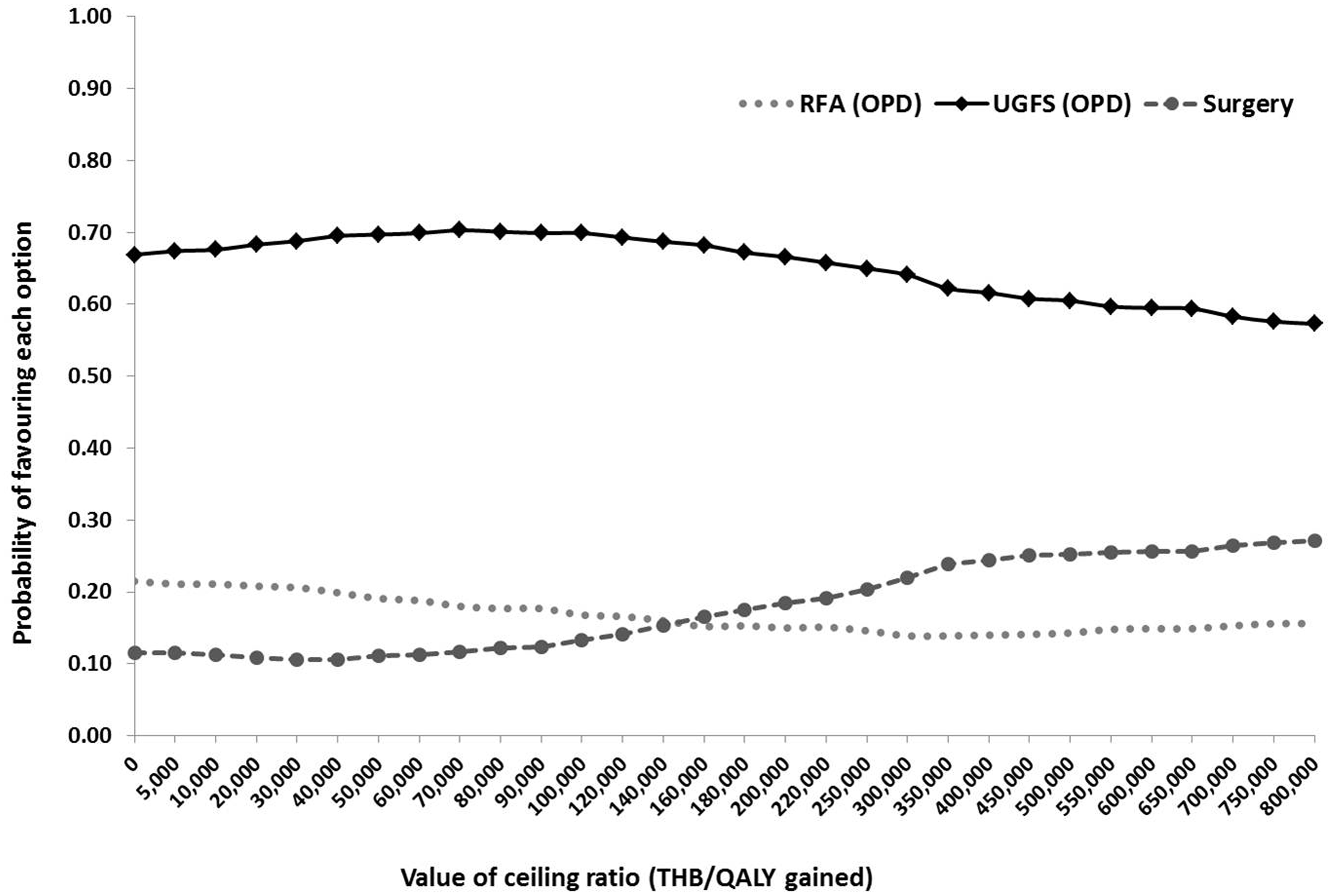
Discussion
To our best knowledge, this is the first economic evaluation of endovenous procedures from a developing country. This study has shown that UGFS was likely to be cost-effective and was dominant to surgery in outpatient setting. RFA was deemed not to be cost-effective for both inpatient and outpatient settings due to its limited time of benefit and much higher direct medical costs.
We used societal perspective which included both direct and indirect costs. Furthermore, the QALY gained was collected from a real clinical setting in Thailand. For treatment efficacy, we used results from most recent meta-analysis of RCTs, 4 which should lead to valid results for the analysis. Disease-specific quality of life measures are more sensitive to the detect changes of outcomes after intervention. To compare interventions between different diseases for informing policymaker, EQ-5D was used to estimate utility for analysis.
RFA had approximately a 21,000 Baht higher procedural cost than surgery but had advantages over surgery by reducing the care time spent by relatives by 4.5 days and reducing productivity loss by 2.5 days. Considering RFA and surgery in condition with similar efficacy, complications, and type of management (outpatient vs. inpatient); RFA would be dominant to surgery if either RFA costed less or Thailand’s minimum wage increased, so the advantages costs from RFA would be more than the difference of procedural cost. UGFS cost approximately 500 Baht more than surgery but was associated with fewer days of post-intervention care by relative (2.5 days) and a gain of four days of productivity. These advantages made UGFS cost-effective (inpatient care) and dominant (outpatient) to surgery.
Utility gained post-intervention was slightly, but not significantly better in the RFA group at one week follow-up and this difference was not seen over one year, consistent with results from recent meta-analysis 4 and two large RCTs.18,19 Furthermore, the overall utility gained after RFA was slightly less than surgery; thus causing RFA to be dominated by surgery. This might have occurred by chance due to the limited number of patients or could be related to the minimal contribution of utility gained at one week post-intervention compared to the overall utility gain. We also found significantly less concomitant treatment of varicosities in RFA. Concomitant treatment of varicosities leads to better gains in QoL in the first three months after treatment compared to delayed treatment with no significant difference in number of further procedures for varicosities. 20 This could influence to the utility gain only in the early period, but not to the cost and should not affect much to the results. Adjusted analysis with concomitant treatment of varicosities also found no significant association of this variable to utility in our study (p = 0.693). A systematic reviews, network meta-analyses and exploratory cost-effectiveness model of randomized trials of minimally invasive techniques vs. surgery for VVs have also demonstrated that cost-effectiveness is largely dependent on the cost of the treatment rather than its efficacy and safety. 21
Our results of RFA contrast to those of Gohel et al. 6 who found that day case surgery of RFA was cost-effective in the UK National Health Service (NHS) which uses a threshold of £20,000 (≈ 1,000,000 Thai Baht) per QALY. In Thailand, RFA costs four times more than surgery whereas in the UK NHS, day case RFA costs less than surgery £776 vs. £980 for surgery, a far better cost ratio than in Thailand. Thus, in Thailand, RFA is not suitable for being reimbursable by the Thai universal health coverage scheme and is only available to those who are willing to pay for it.
Our study was limited by its small size. The limited time horizon of one year could have biased the results in favor of UGFS because symptomatic failure may occur after one year. Therefore, a sensitivity analysis was done assuming all patients had symptomatic primary failure with similar results. These strengthen our conclusion that UGFS is more cost-effective in early term. In addition, our study might be prone to selection biases with more high income patients in the RFA group. However, we adjusted for these in the analysis of the outcomes. These preliminary data are useful for our setting, and we intend to conduct larger prospective cost-effectiveness studies with longer follow-up.
Conclusion
Endovenous procedures are preferred over surgery and UGFS may be the most suitable alternative to surgery in Thai context now for short-term results. RFA also has advantages in terms of cost of care and productivity loss, but its high cost precludes its use in the public health system at this time.
Footnotes
Ethical approval
The Human Research Ethics Committee of Thammasat University (no. 1: Faculty of Medicine) (reference number: MTU-EC-SU-4-095/54).
Contributorship
BY, PN, CW, and PL reviewed literature, conducted study, analysis and writing manuscript, AT involved in protocol development, analysis, and manuscript writing. YT was involved in protocol development, analysis and critical comments
Acknowledgement
We would like to thank Dr. Bob Taylor and Stephen Pinder for helping us editing the manuscript and Ms. Waranya Rattanavipapong for kindly helping us to analyse the data and comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Health Intervention Technology Assessment Program of Thailand (HITAP) through Consortium of Thailand (grant number: HITAF 2554-050) funded this study.