
Abstract
Objective
To investigate the association of polymorphisms located near the FOXC2 gene with the risk of varicose veins in ethnic Russians.
Methods
Allele, genotype, and haplotype frequencies were determined in the sample of 474 patients with primary varicose veins and in the control group of 478 individuals without a history of chronic venous disease.
Results
Polymorphisms rs7189489, rs4633732, and rs1035550 showed the association with the increased risk of varicose veins, but none of the observed associations remained significant after correction for multiple testing. Haplotype analysis revealed the association of haplotype rs7189489 C–rs4633732 T–rs34221221 C–rs1035550 C–rs34152738 T–rs12711457 G with the increased risk of varicose veins (OR = 2.67, P = 0.01).
Conclusions
Our results provide evidence that the studied polymorphisms do not play a major role in susceptibility to varicose veins development in the Russian population.
Introduction
Varicose veins are one of the clinical manifestations of chronic venous disease and can be described as dilated, palpable, tortuous subcutaneous veins with a diameter more than 3 mm. 1 Prevalence estimates of varicose veins vary from <1 to 73% in females and from <1 to 56% in males that could be due to variations in the use of diagnostic criteria as well as differences in the prevalence of risk factors in the studied groups. Generally, this condition is more common in developed countries than in underdeveloped regions. 2
Factors involved in the pathogenesis of varicose veins include vessel wall alterations, impaired extracellular matrix remodelling, elevated venous pressure, valve failure, ineffective function of calf muscle pump, inflammation, and impaired balance between growth factors or cytokines,1,3 though the priority of these events is still controversial and the precise molecular mechanism underlying the development of varicose veins is still not fully understood. A strong body of evidence indicates a prominent role of heredity in the development of varicose veins.4–11 A twin cohort study showed a linkage between candidate marker D16S520 on chromosome 16q24 and varicose veins in otherwise healthy, unselected sibling pairs. 11 The presence of this marker was also found in nine out of 20 families with affected individuals. 12 D16S520 marker is located in close proximity (80 kb) to the FOXC2 gene, which encodes a forkhead transcription factor involved in the development of the lymphatic and vascular system.13–18 In humans, mutations in this gene cause lymphedema distichiasis, a rare autosomal dominant primary lymphedema of the limbs, associated with an accessary row of aberrant eyelashes present in 94% of the affected individuals.19–23 Other possible complications include congenital heart defects, cleft palate, ptosis, scoliosis, ocular anomalies, photophobia, spinal extradural cysts.21,23–25 Notably, half of affected subjects have varicose veins of early onset, 21 with almost all of patients showing signs of venous insufficiency.26,27 Recent study reported a strong association of FOXC2 mutations with primary venous valve failure in both the superficial and deep veins in the lower limb. 28 These findings provide strong evidence for FOXC2 involvement in the aetiology of varicose veins and make it a good candidate for genetic association studies. To date, one study has been published on association of polymorphisms in the FOXC2 gene with the risk of varicose veins. 29 The study was performed on the Indian population, and three polymorphisms were reported to be associated. Further research is warranted to study whether genetic variants in the FOXC2 gene influence the risk of developing varicose veins in other populations. In our study, we investigated the association of six single nucleotide polymorphisms (SNPs) located in a 30.2 kb region of genome containing the FOXC2 gene with the risk of varicose veins in ethnic Russians.
Methods
Patients
The study was approved by the Ethics Committee of Institute of Chemical Biology and Fundamental Medicine (protocol No. 15, 13 September 2013) and the Ethics Committee of Pirogov Russian National Research Medical University (protocol No.123, 21 January 2013). All the individuals enrolled in this study gave signed informed consent. All clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki.
Descriptive characteristics of patients with varicose veins.
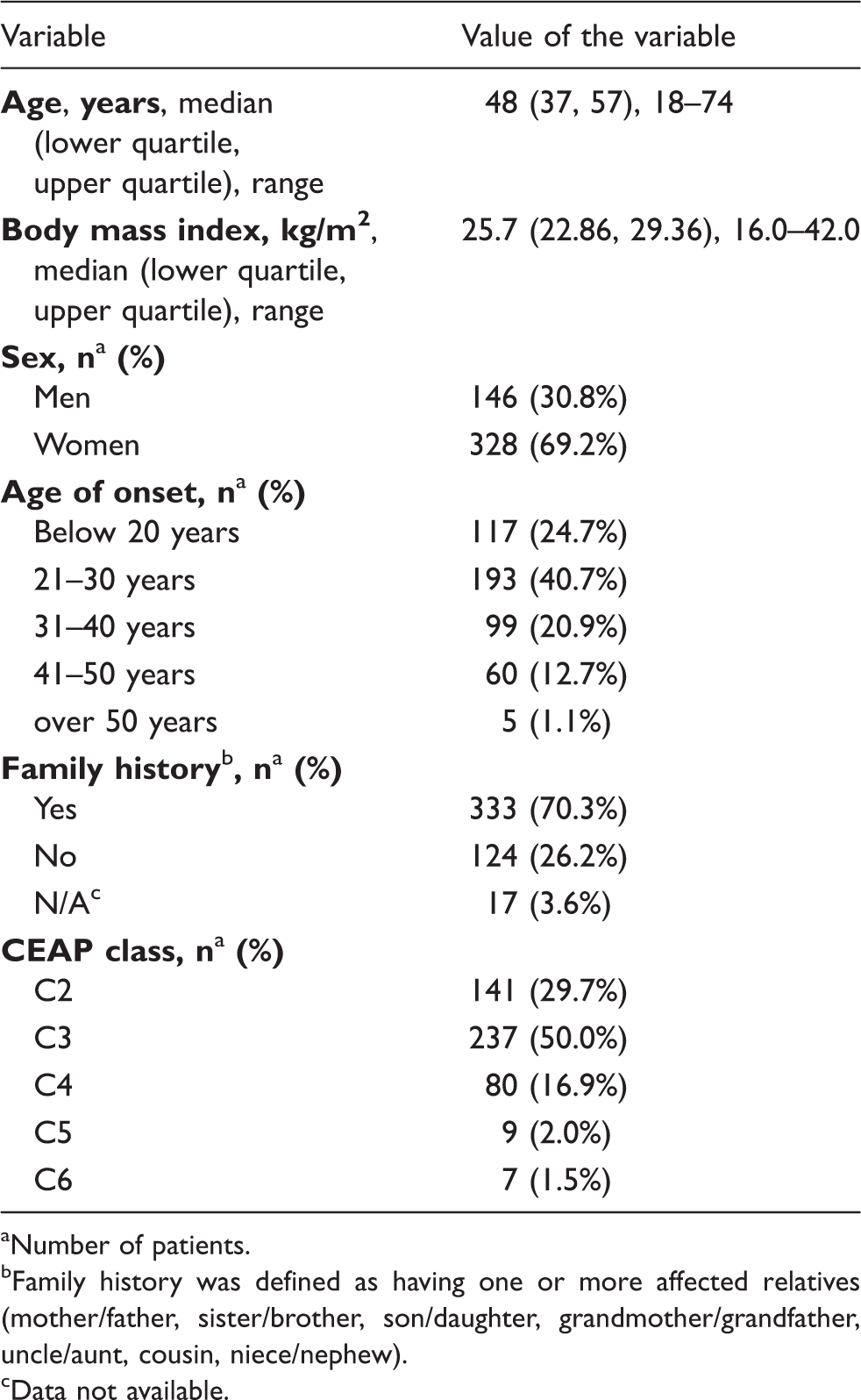
Number of patients.
Family history was defined as having one or more affected relatives (mother/father, sister/brother, son/daughter, grandmother/grandfather, uncle/aunt, cousin, niece/nephew).
Data not available.
The control group comprised 478 patients without a history of chronic venous disease (147 (30.8%) men and 331 (69.2%) women, median age 55 years, lower quartile 44 years, upper quartile 62 years, range 19–84 years).
All cases and controls were ethnic Russians.
Genomic DNA was isolated from leucocytes in venous blood by proteinase K digestion followed by phenol/chloroform extraction and ethanol precipitation. DNA samples were stored at −20℃ in a freezer compartment.
Genotyping
SNPs analysed in our study.

SNP: single nucleotide polymorphism.
Minor allele frequency in European populations according to dbSNP 31 and 1000 Genomes (http://www.1000genomes.org/).
Genotyping of polymorphisms rs7189489, rs4633732, and rs34152738 was carried out by real-time PCR allelic discrimination with TaqMan probes. PCR was performed in 20 μl reaction volume containing 20–100 ng of genomic DNA, 65 mM Tris–HCl (рН 8.9), 24 mM ammonium sulphate, 3.5 mM magnesium chloride, 0.05% Tween 20, 0.2 mM dNTP, 0.3 mM primers, 0.1 mM probes (see Appendix 1), and 1.0 U of Taq polymerase. PCR thermal cycling conditions were as follows: denaturation for 3 min at 96°С followed by 48 cycles of 8 s at 96°С and 40 s at 60°С. Amplification procedure was conducted using CFX96 Thermal Cycler (Bio-Rad, USA).
Genotypes of polymorphisms rs34221221, rs1035550, and rs12711457 were determined by PCR followed by melting analysis of dual-labelled probes (method described by El Housni et al. 32 ). PCR was performed in 20 µl reaction volumes containing 20–100 ng of genomic DNA, 10 mM Tris–HCl (рН 8.9), 55 mM potassium chloride, 2.5 mM magnesium chloride, 0.05% Tween 20, 0.2 mM dNTP, 0.1 mM forward primers, 1 mM reverse primers, 0.1 mM probes (see Appendix 1), and 1.0 U of KlenTaq polymerase. PCR thermal cycling conditions were as follows: denaturation for 3 min at 96°С followed by 55 cycles of 6 s at 96°С, 6 s at 56°С (60°С for rs34221221), and 6 s at 72°С; melting curve 30–70°С, 0.5°С per step. Amplification procedure was conducted using DNA Engine Dyad thermal cycler (Bio-Rad, USA) and melting analysis was performed using CFX96 Thermal Cycler (Bio-Rad, USA).
Primers and probes were designed using sequences obtained from the National Center for Biotechnology Information (http://www.ncbi.nlm.nih.gov/), UGENE software (version 1.14, http://ugene.unipro.ru/), and Oligo Analyzer software (version 1.0.3).
Statistical analysis
To evaluate the effects of the polymorphisms on susceptibility to varicose veins, odds ratio (OR) and 95% CI were calculated by logistic regression analysis adopting co-dominant and additive models of inheritance. All data were adjusted for sex and age. The expected frequencies of genotypes in the control group were tested for accordance with Hardy–Weinberg equilibrium using exact test. Differences were considered statistically significant at P < 0.05. Since overall six SNPs were tested, the significance threshold after implementation of Bonferroni correction for multiple testing was P = 0.008. Statistical analyses were performed using the GenABEL statistical package for the R language (version 3.1.1, http://www.r-project.org; glm function). Haplotype frequencies and the corresponding OR and CI 95% values were calculated using the haplo.stats statistical package for the R language (version 3.1.1; haplo.score and haplo.glm functions). Linkage disequilibrium was analysed based on D′ values calculated using the CubeX program (http://www.oege.org/software/cubex/). To estimate the statistical power of study, genetic power calculator (http://pngu.mgh.harvard.edu/∼purcell/gpc/cc2.html) was used.
Shapiro–Wilk test was used to check whether age and body mass index (BMI) are normally distributed in the analysed groups. Since the distribution was not normal, Mann–Whitney U test was used to evaluate the significance of differences between the groups. P < 0.05 was considered significant. The analysis was performed with STATISTICA 8.0 software.
Results
Allele and genotype frequencies in the case and the control groups. Association of the studied SNPs with the risk of varicose veins.
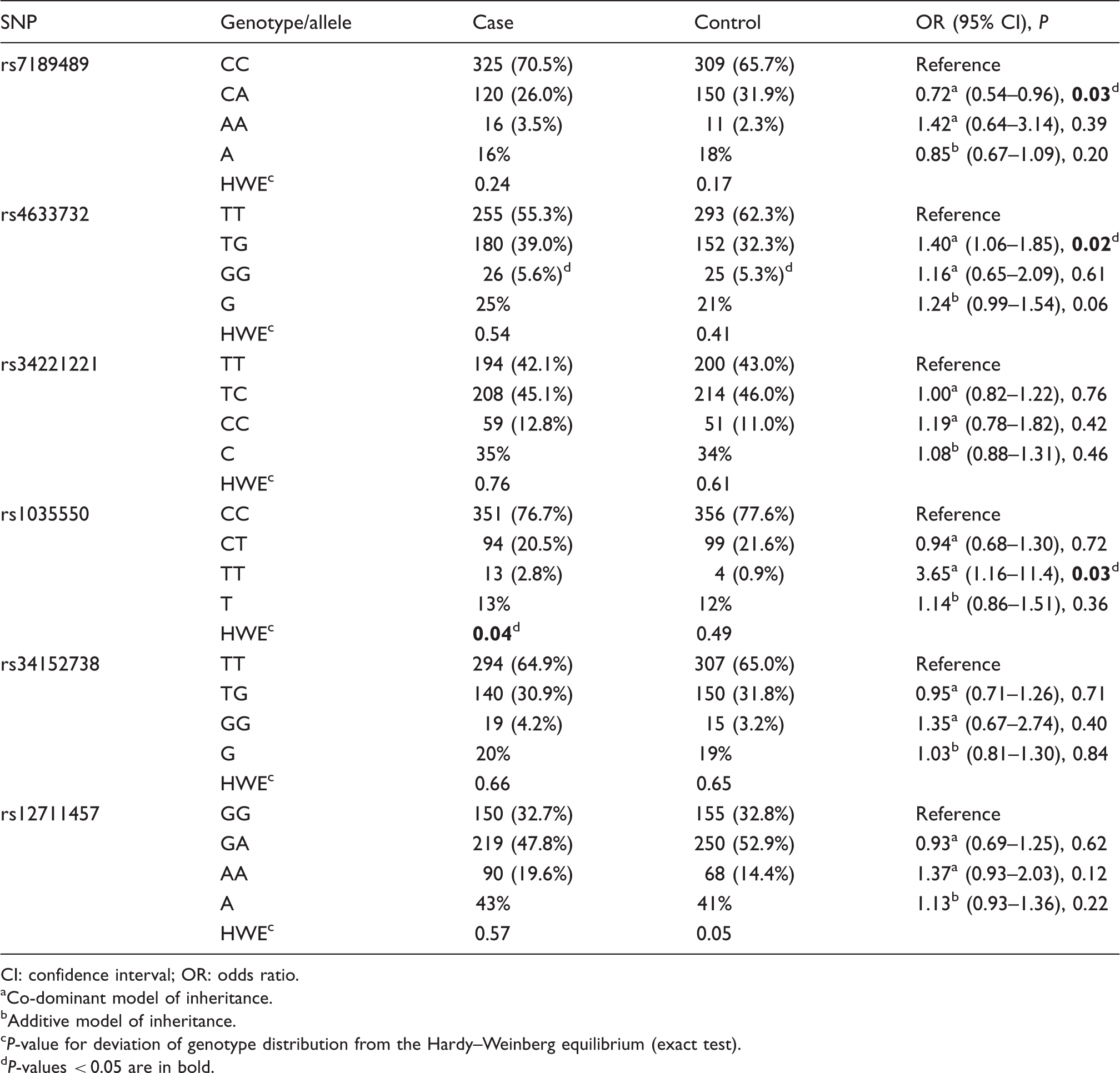
CI: confidence interval; OR: odds ratio.
Co-dominant model of inheritance.
Additive model of inheritance.
P-value for deviation of genotype distribution from the Hardy–Weinberg equilibrium (exact test).
P-values < 0.05 are in bold.
Association of the studied SNPs with the risk of varicose veins.
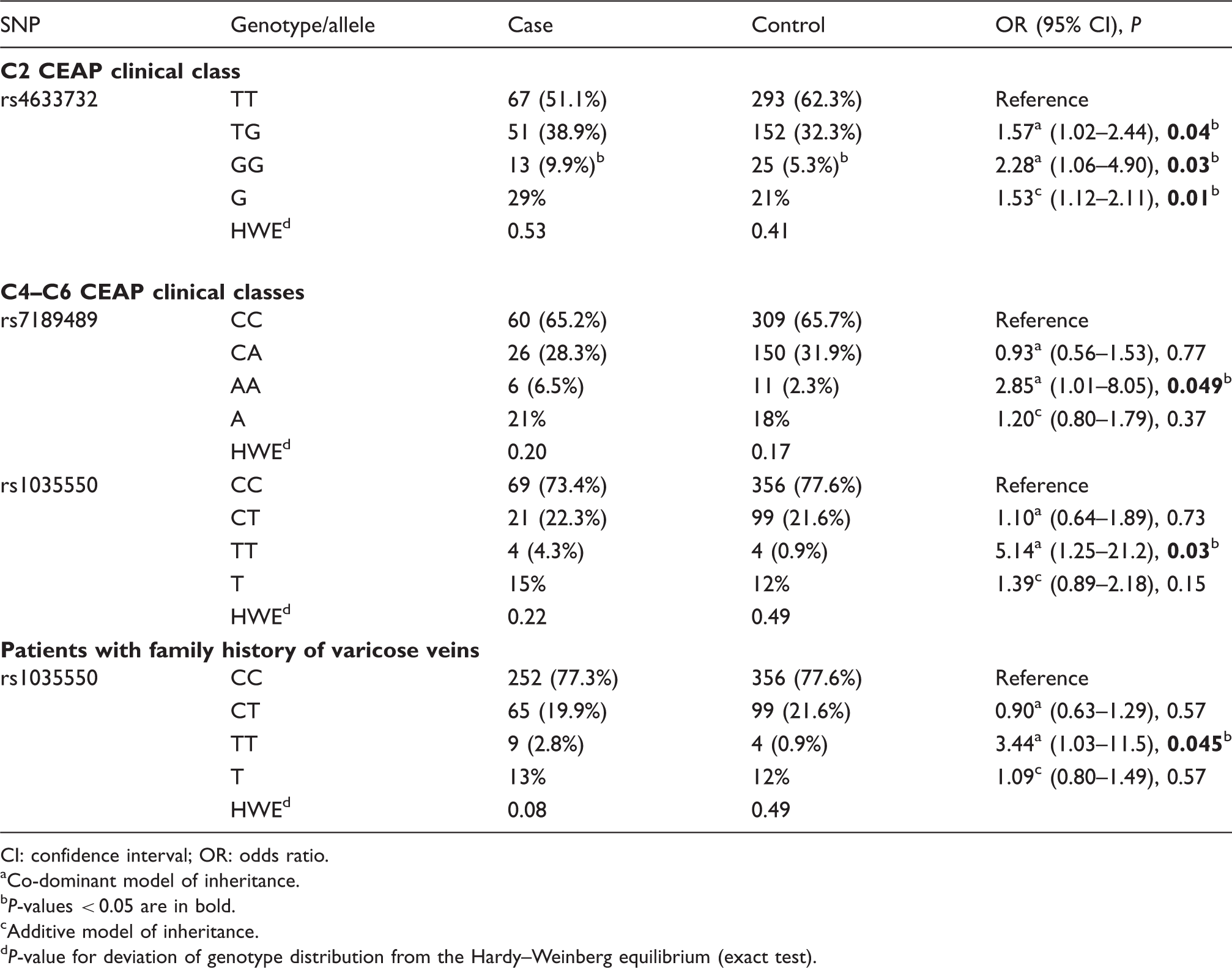
CI: confidence interval; OR: odds ratio.
Co-dominant model of inheritance.
P-values < 0.05 are in bold.
Additive model of inheritance.
P-value for deviation of genotype distribution from the Hardy–Weinberg equilibrium (exact test).
We calculated statistical power of our study. We had 80% statistical power to reveal associations with OR = 1.2 or greater for polymorphisms rs34221221 and rs12711457 and to detect associations with OR = 1.3 or greater for polymorphisms rs7189489, rs4633732, rs1035550, and rs34152738.
Three associations with P < 0.05 were observed in our study: the association of genotype rs7189489 CA with the reduced risk of varicose veins (OR = 0.72, P = 0.03) and the associations of rs4633732 TG and rs1035550 TT genotypes with the increased risk of this pathology (OR = 1.40, P = 0.02 and OR = 3.65, P = 0.03, correspondingly; Table 3). Since the association of heterozygous genotype alone hardly ever has biological sense, we tend to think that these associations are false positive. All the revealed associations turned out to be insignificant after the implementation of Bonferroni correction for multiple testing.
Subgroup analysis was performed for patients having C2, C3, and C4–C6 CEAP clinical classes of chronic venous disease and also for patients with positive/negative family history. The revealed associations are presented in Table 4. Polymorphism rs4633732 showed an association with the increased risk of developing varicose veins in the subgroup of patients with C2 class (TG versus TT: OR = 1.57, P = 0.04; GG versus TT: OR = 2.28, P = 0.03; G versus T: OR = 1.53, P = 0.01). Genotype rs7189489 AA was associated with varicose veins in individuals having C4–C6 classes (OR = 2.85, P = 0.049). Genotype rs1035550 TT showed the association in the subgroup of patients with C4–C6 classes and in the subgroup of individuals having positive family history (OR = 5.14, P = 0.03 and OR = 3.44, P = 0.045, correspondingly). None of the revealed associations remained significant after applying the Bonferroni correction.
We evaluated the linkage disequilibrium between the studied polymorphisms (Figure 1). The majority of neighbouring SNPs were tightly linked with D′ = 0.69–1.00 (except rs4633732 and rs34221221, D′ = 0.25). The frequency of the most common haplotype rs7189489 C–rs4633732 T–rs34221221 T–rs1035550 C–rs34152738 T–rs12711457 G was lower in the case than in the control group (37.0% versus 41.6%, P = 0.049; Appendix 2). To evaluate the effect of this major haplotype, we took the sum total of other haplotypes as reference and calculated OR and 95% CI (0.82 and 0.67–0.999, correspondingly). Other haplotypes had frequencies 0–12%, and most of them were very rare or not seen in our sample (Appendix 2). Haplotype rs7189489 C–rs4633732 T–rs34221221 C–rs1035550 C–rs34152738 T–rs12711457 G was more frequent among patients having varicose veins than in the control group (3.82% versus 1.31%) and was associated with the increased risk of the studied pathology (OR = 2.67, 95% CI 1.14–6.24, P = 0.01).
Linkage disequilibrium between the studied SNPs in the sample of ethnic Russians.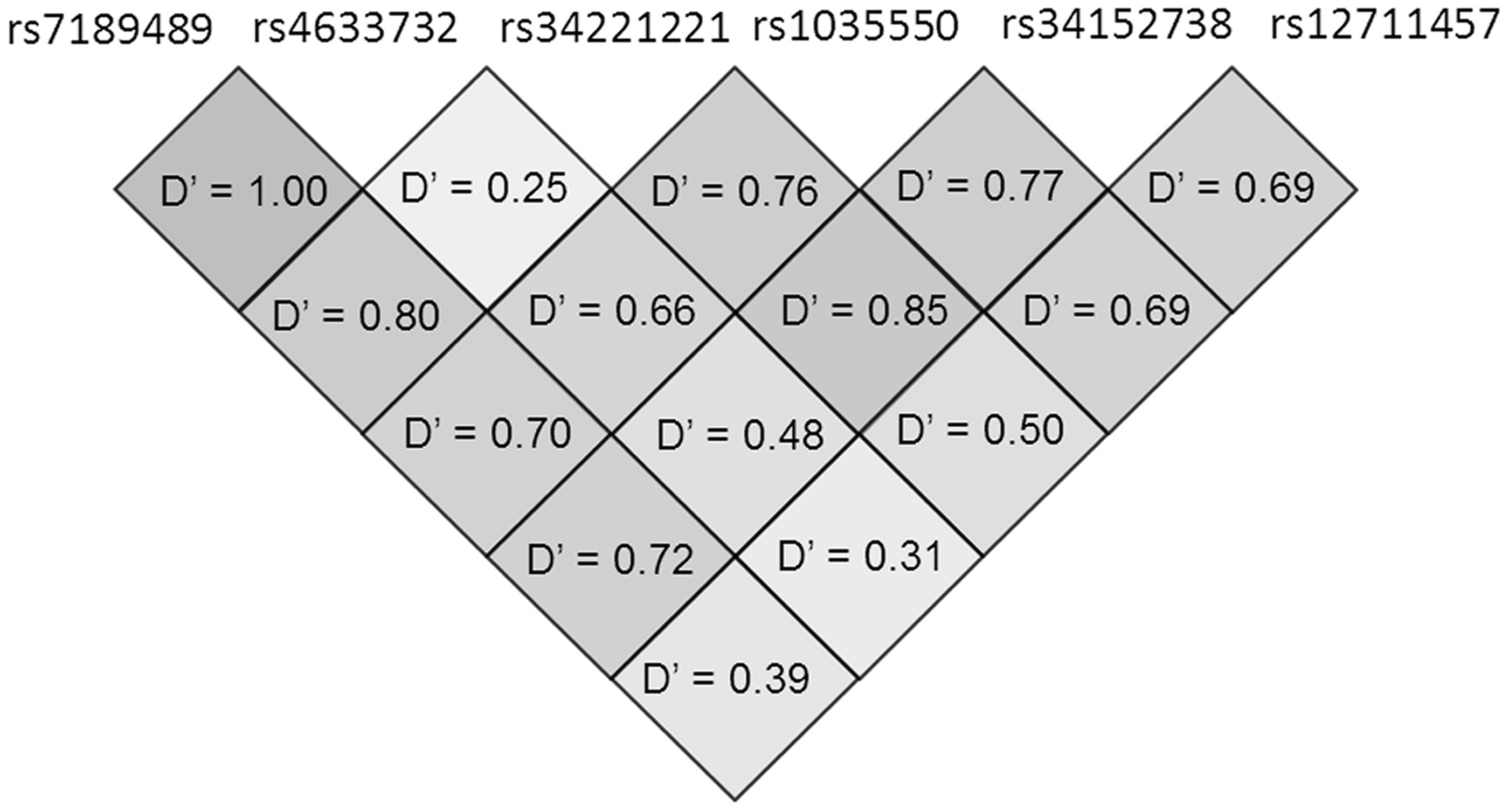
We investigated the influence of SNPs on BMI in patients with varicose veins (Appendix 3). Only polymorphism rs12711457 was significantly associated with BMI. Carriers of rs12711457 A allele had significantly lower BMI (median 25.33 kg/m2, lower quartile 22.53 kg/m2, upper quartile 29.05 kg/m2) than individuals having GG genotype (median 26.40 kg/m2, lower quartile 23.66 kg/m2, upper quartile 30.16 kg/m2, P = 0.03). The association became insignificant after the implementation of Bonferroni correction.
Discussion
FOXC2 is a member of the forkhead family of transcription factors, which bind to DNA via a highly conserved variant of the helix-turn-helix motif. Human FOX gene family consists of at least 43 members. 33 The exact mechanism of FOXC2 action remains largely unknown. Animal studies have shown that FOXC2 plays an important role in embryonic development, including the development of cardiovascular and lymphatic systems as well as angiogenesis and lymphangiogenesis in postnatal life. FOXC2 is required for mesenchymal cell interactions, arterial cell specification, lymphatic and blood vessel formation, valve formation, lymph node formation, cardiac outflow tract morphogenesis, etc.13–18,34 It was demonstrated to regulate the expression of genes encoding Ang2, integrin β3, Delta-like 4, Hey2, CXCR4, and some other proteins important for the control of angiogenesis.35–37 Data obtained from recent studies suggest that FOXC2 could be involved in the aetiology of varicose veins in humans.11,21,26–29 In our study, we tested the hypothesis that SNPs in the genomic region containing FOXC2 could be associated with the risk of developing varicose veins in ethnic Russians. The previously published association study revealed the effect of SNPs in the FOXC2 gene on the risk of chronic venous disease in the group of patients having mostly C4–C6 CEAP clinical classes. 29 Another study demonstrated the presence of the genetic locus related to the FOXC2 gene (D16S520) in families with patients having varicose veins, and all affected individuals, including older patients (with disease duration >20 years), had C2 class. 12 In our study the majority of patients had C2 and C3 classes (Table 1). In order to examine whether potential influence of the studied SNPs is disease subtype specific as well as to be able to compare our results with the results of previous studies, we stratified our sample according to CEAP classes and presence/absence of family history and conducted a subgroup analysis.
We determined allele, genotype, and haplotype frequencies of polymorphisms rs7189489, rs4633732, rs34221221, rs1035550, rs34152738, and rs12711457 in patients having varicose veins and in the control group of individuals without a history of chronic venous disease (Tables 3 and 4, Appendix 2). Allele frequencies in ethnic Russians were generally close to those reported in the SNP database for European populations 31 (Table 2) as well as to allele frequencies previously determined by other research groups (rs34221221 C allele frequency was found to be 35–39% in Scandinavians38,39 and 35% in the Finnish population 40 ).
We did not find strong evidence that the studied polymorphisms have an impact on the risk of varicose veins development in our population. We observed several associations with P < 0.05, but none of them remained statistically significant after the implementation of Bonferroni correction for multiple testing (rs1035550, rs4633732, and rs7189489; Tables 3 and 4). We therefore cannot exclude that our findings are false positive, so the revealed associations should be treated with caution until replicated by independent studies. Nevertheless, we found out that the most common haplotype, containing only major alleles (rs7189489 C–rs4633732 T–rs34221221 T–rs1035550 C–rs34152738 T–rs12711457 G), was less frequent in the case than in the control group (P = 0.049, Appendix 2). Only one of the remaining haplotypes was significantly associated with the increased risk of varicose veins (OR = 2.67, P = 0.01). This haplotype was different from the major haplotype only in the presence of rs34221221 C allele, providing evidence that polymorphism rs34221221 could still be associated with the risk of the studied pathology, but its effect might possibly be masked by joint effects of other polymorphisms. Notably, this polymorphism was shown to be strongly associated with the risk of varicose veins in the Indian population. 29 Functional analysis in that study revealed that TT genotype was associated with FOXC2 overexpression. In contrast to our results, the association with the increased risk was observed for rs34221221 T variant. It is worth noting that rs34221221 T is a minor allele in Asians, while it is a major allele in Caucasians (rs34221221 T frequency is 38–40% in the Chinese population, 31 29–32% in the Japanese population,31,41 45% in the Indian population, 29 and 54–66% in different European populations including our population).31,38–40 It is also interesting to note that varicose veins were found to be less common in Asians than in non-Hispanic Whites. 42 We can speculate that genetic differences between the populations, including differences in gene–gene interaction, could underlie discrepancy in the observed effects. It is possible that Asians could have higher basal level of FOXC2 protein, and excessive FOXC2 amount in individuals with T allele can disrupt the balance and lead to varicose veins formation. On the other hand, if Europeans have low basal FOXC2 level, carriers of rs34221221 C allele may be at risk due to the insufficient amount of this regulatory protein. It would therefore be interesting to examine the influence of this SNP on the risk of varicose veins development in other populations of European and Asian origin.
Furthermore, in our study we failed to replicate the association of rs34221221 with BMI, which was previously revealed in the Finnish population 40 and Pima Indians. 43 Since our sample size was close to those in the above-mentioned studies, this result provides additional evidence that the effect of this SNP could be modulated by ethnic factors.
Finally, the main limitation of our study should be acknowledged. We did not use any sophisticated approaches for SNP selection and investigated only six SNPs in the studied genomic region. Nevertheless, our linkage disequilibrium analysis has shown that the studied SNPs are tightly linked to each other and are therefore likely to cover this region of genome.
Conclusion
We revealed the associations of polymorphisms rs1035550, rs4633732, and rs7189489 with the increased risk of varicose veins in ethnic Russians. Polymorphism rs1035550 showed an association in the whole sample of patients and in the subgroups of patients with C4–C6 CEAP classes and positive family history. Polymorphisms rs4633732 and rs7189489 were associated with the risk of varicose veins only in the subgroups of individuals having C2 and C4–C6 CEAP classes, correspondingly. Since none of the revealed associations reached Bonferroni-corrected significance levels, our findings need further confirmation by independent studies. However, our haplotype analysis indicated that the studied SNPs could mask each other’s effect and suggested an association of polymorphism rs34221221 C with the increased risk of the studied pathology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Russian Science Fund (grant number 14-15-00734, “Searching of genes involved in varicose vein disease pathology”).
Ethical approval
The study was approved by the Ethics Committee of Institute of Chemical Biology and Fundamental Medicine (protocol No. 15, 13 September 2013) and the Ethics Committee of Pirogov Russian National Research Medical University (protocol No. 123, 21 January 2013).
Guarantor
ASS.
Contributorship
ASS performed the research and wrote the paper. EAS and MAS extracted DNA from blood. KSS, AIS, MYD, OAS, and EAI provided blood specimens and clinical data. MLF designed primers and probes. ENV, IAZ, AIK, and MLF supervised the research. All authors reviewed and edited the manuscript and approved the final version of the manuscript.