
Abstract
Introduction
Venous thromboembolism is a frequently occurring phenomenon with a high risk of acute and chronic complications. To prevent these, subjects are treated with surgical options to restore venous blood flow combined with medical treatment or medical treatment alone. Despite great therapeutic advances considerable morbidity still persists. For example, thrombosis of the leg can result in post-thrombotic syndrome, which has a great impact on quality of life. The best management to prevent the post-thrombotic syndrome is a topic of research and debate. In this study, we searched the literature to identify studies that used oral anticoagulants and evaluated their properties for resolution of thrombus and hence prevention of the post-thrombotic syndrome.
Methods
We searched PubMed, The Cochrane Library, and four international medical journals frequently reporting on venous thromboembolism. Furthermore, we looked at Clinicaltrials.gov for current research on this topic.
Results
Only three suitable articles were identified.
Discussion
We found experimental evidence that direct thrombin inhibitors and factor Xa inhibitors have an influence on clot lysis favoring a quicker recanalization compared to warfarin. Future studies investigating these effects in humans are warranted.
Introduction
Venous thromboembolism affects many people worldwide. A study in the United States showed a lifetime risk of venous thromboembolism ranging from one 1 in 12 in a black and white American population to 1 in 6 in subjects with Factor V Leiden or even 1 in 5 when sickle cell trait or disease was present. 1 If complicated by symptomatic pulmonary embolism, the condition often results in acute cardio-respiratory problems or even death. In the long term, an incidence of 3.8% (95% confidence interval, 1.1 to 6.5) of chronic thromboembolic pulmonary hypertension (CTPH) was shown two years after acute pulmonary embolism. 2 CTPH carries a considerable risk for morbidity and mortality. However, new but invasive strategies have been developed to improve outcome of this condition. 3 Thrombosis of the leg (deep vein thrombosis (DVT)) can present itself without visible abnormalities and rather subtle symptoms or on the other hand phlegmasia cerulea dolens. The latter is usually a consequence of massive thrombosis in the leg. On average, prognosis of DVT is good with current therapies. Nevertheless, a considerable number of patients (25–50%) suffer from the post-thrombotic syndrome (PTS) within the first year after thrombosis. 4 A condition characterized by a range of symptoms varying from mild edema, swelling and pain to severe pain, edema, and leg ulcers. It seriously affects the quality of life of these patients. 5
In a perfect scenario, on the long run venous function of the leg is restored to normal. Luckily 50% of cases that have distal thrombosis with minor symptoms experience recanalization without venous reflux within three months. With more proximal thrombosis however recanalization often requires a longer period and this is more often complicated by disrupted valve integrity and venous reflux. 6 More proximal localization and time to recanalization are associated with PTS as is the balance between pro-thrombotic factors and the fibrinolytic system. 7 Therefore, it seems reasonable to try to achieve recanalization as soon as possible. Treatments, which besides anticoagulant activity, have positive effects on the fibrinolytic system or reduce additional pro-thrombotic factors, could be promising. Currently, most patients are treated with unfractionated heparin or low-molecular weight heparin (LMWH) followed by vitamin K antagonists. More recently, direct thrombin inhibitors (DTI) or oral factor Xa inhibitors (FXI) were introduced as a first line treatment. In addition, compression stockings are advised.8,9 Recently, the effectiveness of compression stockings to prevent PTS was questioned. 10
Treatment of deep venous thrombosis of the leg in the acute setting aims to prevent further growth of the thrombus, new thrombi, thrombus release with consequent pulmonary embolism, and recurrent venous thrombosis. In the past years, several interventions have been developed to improve outcome of the leg. It seems clear that earlier recanalization is beneficial with regard to post-thrombotic symptoms. 6 We can divide interventions in acute and chronic treatments. In the acute setting, there are surgical invasive methods including ultrasound-assisted thrombolysis, suction of the thrombus, and surgical embolectomy mainly applied with iliofemoral thrombosis. Medical options are systemic or local thrombolysis. 11 Chronic treatment involves anticoagulants and compression stockings for three to six months or longer in selected cases. This long term treatment is usually started acutely after diagnosis but does not always result in quick recanalization increasing the risk of a compromised venous return. Treatment with anticoagulants and compression stockings is still advocated in most of the guidelines and an acceptable safety/risk profile has been proven. 12 Whether the more aggressive therapies to resolve thrombus have an acceptable number needed to treat and a low number needed to harm is still a matter of study and debate.13–15 Selecting the right patients for these interventions to maximize a favorable outcome is a challenge. An interesting question is the possibility of differences in chronic treatment concerning the recanalization rates between warfarin and DTI or FXI. The latter two appear to have similar efficacy in the acute management of thrombosis with less bleeding complications. 9 However, whether they are more potent in preventing, PTS has not been evaluated in these studies. 16 In this article, we will search the literature to find evidence for the efficacy of these newer anticoagulants and warfarin with respect to thrombus resolution, recanalization, and hence the prevention of PTS.
Methods
First a PubMed search was performed using the following strategy up to 6 December 2015: deep venous thrombosis AND (doac OR direct oral anticoagulants OR factor Xa OR dabigatran OR apixaban OR rivaroxaban OR edoxaban) AND (warfarin OR vitamin k antagonists OR coumarin OR acenocoumarol OR phenprocoumon) AND (recanalization OR PTS OR venous insufficiency OR venous ulcers OR villalta score OR clot lysis OR fibrinolysis OR pai-1 OR pro-thrombotic) using MeSH terms. Second the Cochrane Library was searched for suitable articles using “thrombosis,” “post thrombotic syndrome,” and “treatment” as search terms. Finally, a search in the index of Phlebology, thrombosis and hemostasis, circulation and blood for additional research on this subject was performed. Here, we used the generic names of DTI and FXI (apixaban, dabigatran, edoxaban and rivaroxaban) and the words clot lysis or PTS as search terms. I read all abstracts to screen the retrieved articles. They were included if they were written in English, Dutch, French, or German. They were excluded if no study results on DTI, FXI, or warfarin were reported. In human studies, follow-up should have been at least one year. Clinicaltrials.gov was searched for upcoming trials on this subject.
Results
Search result on oral anticoagulants clot lysis and post thrombotic syndrome.
Discussion
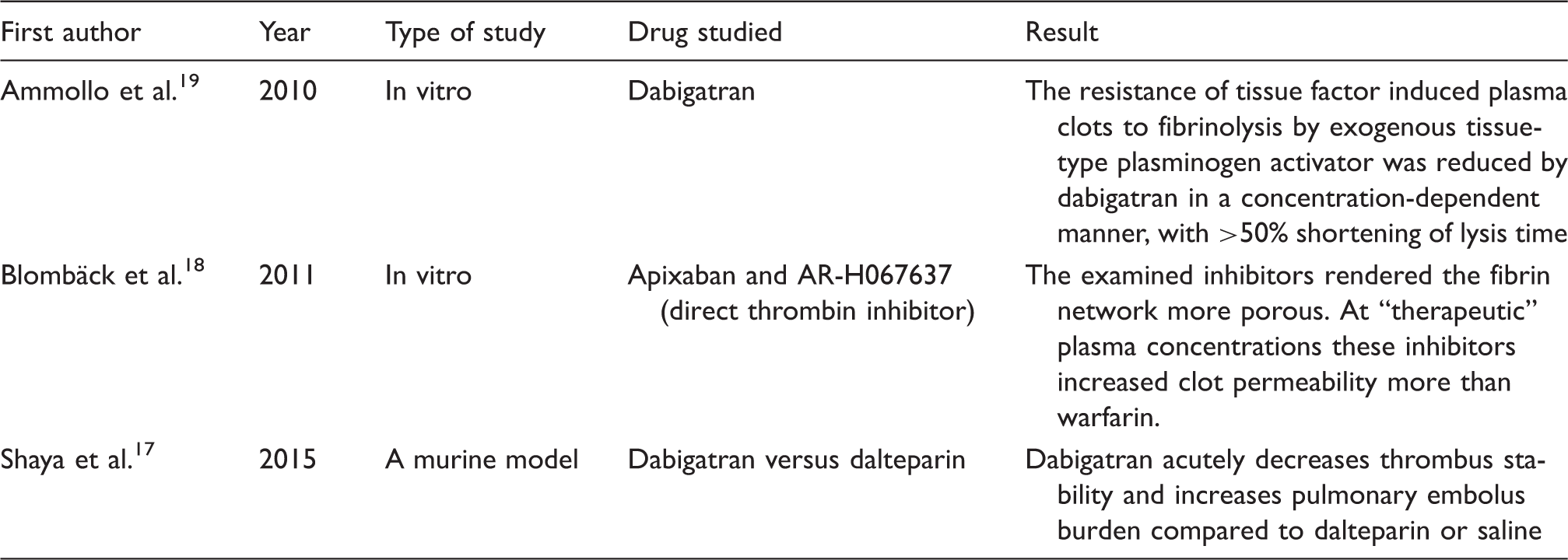
This study shows that no large randomized trials evaluating the effect of warfarin, DTI or FXI on PTS in humans exist. It is a missed opportunity that this was not evaluated properly in the recent intervention trials on treatment of DVT with DTI or FXI. Looking at the in vitro results of the presented studies, it seems that DTI and FXI facilitate clot lysis. The first study investigates the role of dabigatran on fibrinolysis. 19 Fibrinolysis time was cut in half by dabigatran in a concentration-dependent manner after administration of exogenous tissue-type plasminogen activator. This was associated with a reduction in thrombin activatable fibrinolysis inhibitor (TAFI) activation and thrombin generation. They also assessed the viscoelastic properties of clots. Those generated in the presence of dabigatran were more permeable, less rigid, and consisted of thicker fibers. The impact of these physical changes on fibrinolysis was investigated using a model under flow conditions, which demonstrated that dabigatran made the clots more susceptible to flowing tissue plasminogen activator, by a mechanism that was largely TAFI-independent. In contrast to these results, the study published by Blombäck et al. 18 did not show any difference in clot permeability between DTI and FXI. They calculated the permeability constant of fibrin gel in plastic cylinders coated with human fibrinogen and treated with DTI, FXI, Fondaparinux an indirect factor Xa inhibitor, and warfarin. DTI and FXI had a comparable response throughout the experiment but increased permeability more than warfarin. Clot instability with DTI was also shown in a murine model. 17 Intravital videomicroscopy in the femoral vein of mice was used. After thrombus induction saline, dalteparin or dabigatran was given. They showed that thrombus size was similar over time and between treatment groups. However, in the dabigatran group, total and large embolic events and pulmonary emboli were most frequent. They concluded that dabigatran acutely decreases thrombus stability compared to dalteparin or saline. In fact, FXI can safely fully replace the initial treatment with LMWH followed by warfarin, whereas the currently registered DTI was only studied and registered preceded by LMWH in the first days of treatment. A study with Ximelagatran, a DTI, which never reached the market because of unexplained liver damage, showed increased venous thromboembolism recurrence in the beginning of the treatment (THRIVE study). Because of early withdrawal from further studies, it was never tested in higher doses so we cannot be sure this is in fact a property of DTI. The mechanism is complex but an important role for clotting factor XIII is suspected. 17 Activated by thrombin, it stabilizes fibrin and crosslinks alpha2-antiplasmin to fibrin and fibrinogen. The latter effect possibly contributes most to clot stability. Inactivation of thrombin by DTI could prevent this important part of stabilization of the clot and thus make it susceptible to release emboli. The largest trial that compared the safety and efficacy of DTI versus warfarin for the treatment of DVT and pulmonary embolism did not show a statistical significant difference in the rate of pulmonary embolism or related events during treatment. However, three patients died from pulmonary embolism in the DTI group of which one was actually using the DTI (RE-COVER II). FXI do not have this inhibiting effect on clotting factor XIII and the large studies on deep venous thrombosis treated with FXI versus warfarin did not show a difference in pulmonary embolism during treatment. (EINSTEIN DVT, AMPLIFY, and HOKUSAI VTE). The available studies addressing clot lysis with DTI and FXI suggest a possible advantage in clot resolving speed compared to warfarin. Quick clot lysis could be of benefit to the incidence of PTS. 6 However, possible complications of an unstable clot, especially when using DTI, should influence the design of future studies addressing this question in humans.
The overall safety profile of DTI combined with LMWH in the first days of treatment and FXI with comparable effects on thrombosis but lower bleeding complications compared to warfarin justifies new studies evaluating their effect on clot lysis, recanalization, and PTS in vivo. Because the murine model showed increased embolization towards the pulmonary circulation, new human studies should also measure outcomes like CTPH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.