
Abstract
Deep vein thrombosis, and the resultant development of post-thrombotic syndrome, is a significant health issue. Recent evidence demonstrates that the severity of post-thrombotic syndrome symptoms is directly related to the level of venous thrombosis and following treatment these subsequent symptoms are inversely related to the degree of thrombus removal. If we can improve, and preferably standardise the terminology associated with pre-treatment assessment of thrombus load and post-treatment success of thrombus removal techniques, we should then be able to choose more tailor-made techniques to greater benefit our patients. A number of scoring systems have been devised for the assessment of venous thrombus burden, with a majority impractical for everyday usage. In order to provide a more practical solution, the lower extremity thrombosis classification has been developed, using information on anatomical location for venous thrombus combined with a clinical indicator as to the likely sequelae. Anatomical success following venous thrombolysis can be defined by assessing restoration of anterograde flow in the treated vein or the percentage degree of thrombolysis, using venography. The second option is the method most frequently utilised, with the Venous Registry grading system applied. Data from recent trials have given us conflicting and confusing data mainly because we are not using standardised terminology. We urgently need to agree on a standard method of description of thrombus removal before stent placement which also incorporates the likely clinical impact of the area involved in the thrombosis.
Keywords
Introduction
Deep vein thrombosis (DVT) is a significant health issue. It affects approximately one person per thousand per year in a western, Caucasian population with a mortality rate of 6% one month following diagnosis. 1 Over the longer term, however, quality of life and economic effects become more significant issues. 2 The development of post-thrombotic syndrome (PTS) is seen in 40%–60% of patients with acute DVT who are treated with anticoagulation alone, dropping to 25% if used in conjunction with below knee compression stockings for two years.3,4 The significant decrease in quality of life in patients afflicted with PTS has drawn comparison to that associated with chronic obstructive pulmonary disease, congestive heart failure and angina pectoris. 5 If we can improve, and preferably standardise, the terminology associated with thrombus removal techniques we should then be able to choose those techniques which benefit our patients more.
The open vein hypothesis
There have been multiple trials and registries which have built up a cumulative evidence base which support the following tenets:
The ilio-femoral segment is the critical area in drainage of the lower extremities.6–10 Recanalisation of the ilio-femoral segment occurs in about one-third of patients following an occlusive ilio-femoral venous thrombosis if treated in the standard manner with anticoagulation alone.11,12 The severity of the PTS is related to the level of the venous thrombosis; the more proximal the DVT, the more severe the degree of PTS.
13
Anticoagulation on its own does not remove thrombus. Thrombus removal can be accomplished in a variety of ways, and with the advent of improving endovascular techniques there has been a shift from multi-session catheter-directed thrombolysis towards single session techniques.14–26 The greater the thrombus removal the lesser the subsequent symptoms.
27
Following thrombus removal, patency of the ilio-femoral segment is improved by placement of stents.28,29 Despite the apparent success of many different methods of thrombosis removal/dispersion, there is a lack of clarity in the methods of description of how best to evaluate the outcome of thrombolysis and to correlate this outcome with and without stent placement.30,31
Methods and validity of a scoring system before treatment
A number of scoring systems have been devised for assessment of venous thrombus burden. Every few years a new one is devised, and the fact that there is no one dominant system tells it own tale. Original systems were based on venography32–36 and have been modified so as to use complete compression ultrasound (CCUS)
37
(Figure 1). It was recognised in the late 1990s that venography was not routinely used in the diagnosis of venous disorders, and so two new systems were devised on each side of the Atlantic38,39 which enabled use of computed tomography (CT) and magnetic resonance imaging (MRI).32–41
Modified from Agnelli et al.; method for calculating thrombus burden score.37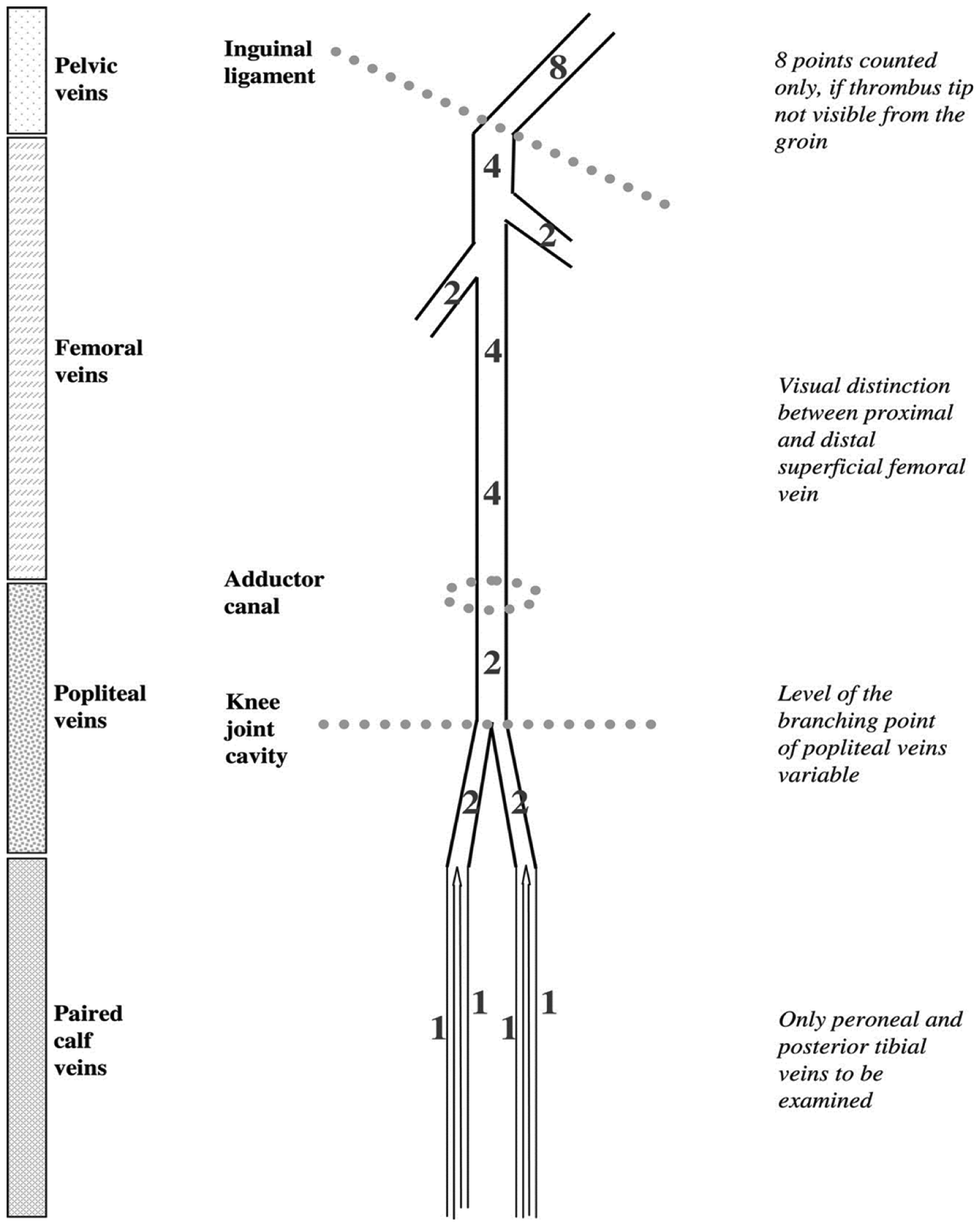
In reality, there are systems which are suitable for trials and those which are more practical for everyday usage. The Length-Adjusted Thrombus Score (LATS) is an example of the former (Figure 2). This is very precise and enables accurate analysis between different techniques for thrombus removal but relies on marker-catheter venography and is clearly not designed for daily use.
Primary EP: percentage reduction in thrombus load by the Length-Adjusted Thrombus Score (LATS). Image courtesy of Professor Nils Kucher, Berne, Ch.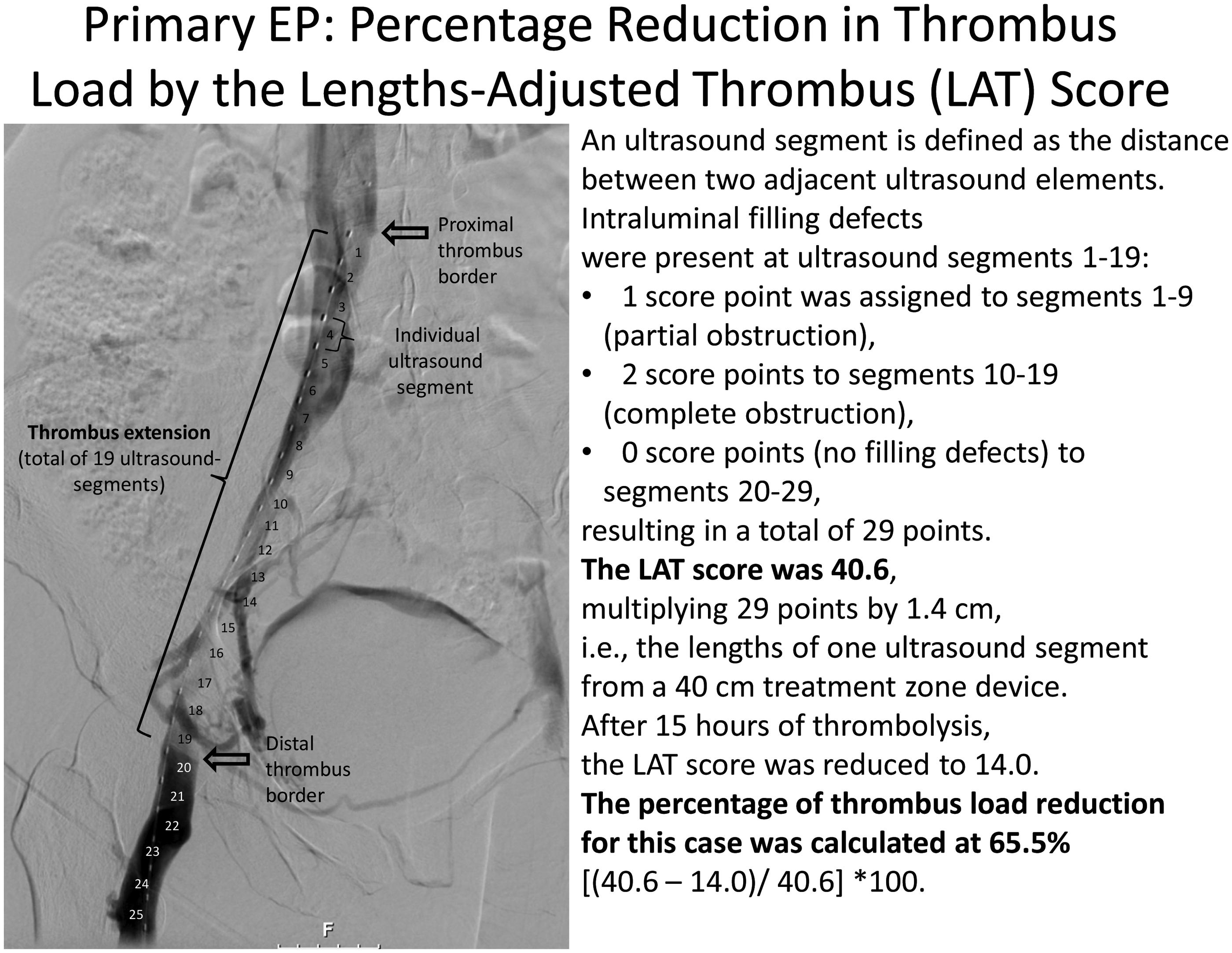
For routine use a system must be simple, practical, user friendly and readily applicable – somewhat comparable to trans Atlantic societal consensus (TASC) for aorto-iliac disease. 42 It must be non-invasive and allow visualisation of the segments above the inguinal ligament where the sensitivity of ultrasound is poor. So in reality this means it must incorporate computed tomographic venography (CTV) and magnetic resonance venography (MRV) for pre-operative diagnosis. Critically, it must separate those DVTs which will do poorly without aggressive treatment from those who should do relatively well with standard anticoagulation. Older terms such as “proximal” and “distal” are not accurate enough. The system must clearly identify those with occlusive ilio-femoral disease – specifically above the common femoral “sump”; the junction point in the common femoral above the inflow of the profunda femoris veins (PFV) and femoral veins (FV) – blockage at this level means the drainage of the entire lower extremity is compromised.
In order to provide a more practical solution, the lower extremity thrombosis (LET) classification has been developed in one of the leading European centres for venous intervention. 43
In essence, this combines an anatomical location for the venous thrombus, with a clinical indicator as to the likely sequelae (Figure 3, Table 2). This is a simple system to identify the level of thrombus. LET I refers to isolated calf vein thrombosis; LET II refers to FV, PFV and above knee popliteal veins; LET III refers to obstruction of the drainage of the entire lower extremity (CFV above inflow of PFV; external iliac veins (EIV), common iliac veins (CIV)) and LET IV refers to the inferior vena cava (IVC).
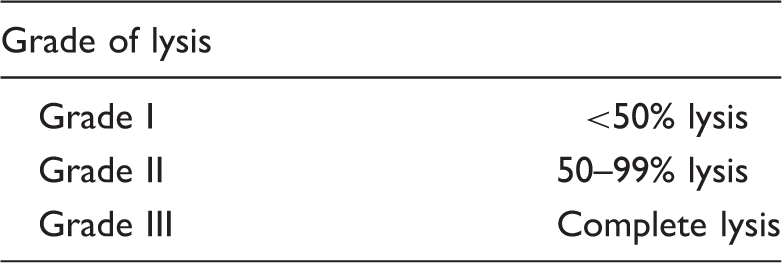
LET score. Critical area- circled-demonstrates importance of occlusion of the entire outflow of the lower extremity. The LET system is the first to focus on this; it deserves on-going validation.46 Grade of lysis following treatment of DVT venous registry.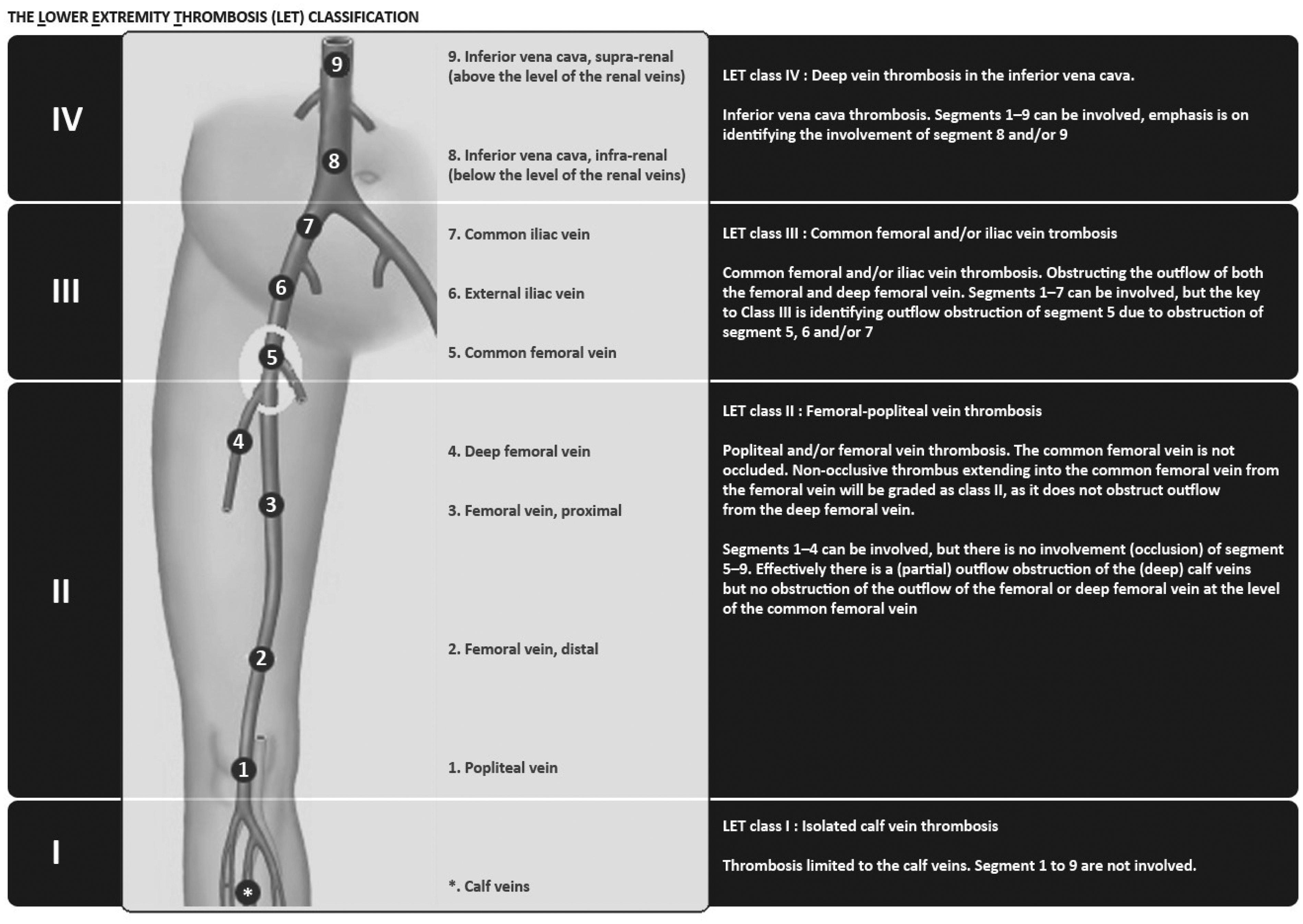
This system is the first to identify the critical nature of complete obstruction to the entire outflow of the lower extremity pinpointing this precisely on the common femoral vein above the inflow of the PFV. So for instance, non occlusive thrombus extending into the CFV from the FV is LET II, whereas complete obstruction of the CFV and above as far as the IVC is LET III. It also does not rely exclusively on Ultrasound for the evaluation of central veins, using MRV for imaging above the inguinal ligament.
Why is this distinction important? Well it is accepted that LET III patients have higher rates of PTS than those with LET II, and this has been validated retrospectively by a survey published recently. 46 This is far more accurate than the previously used terms “proximal vs. distal”, or even “ilio-femoral vs. femoro-popliteal.” A potential disadvantage is the relative scarcity of good MRV, which forms the cornerstone of imaging at the centre which devised this classification but other centres seem to struggle to produce comparable imaging. So if all future DVT lysis trials were graded anatomically according to one system, we would at least have a solid understanding of which techniques remove what percentage of thrombus from each segment. And with so many devices on the market, each with a slightly different mechanism of action, this comparison would be really useful.
Methods and validity of a scoring system after treatment
Anatomical success following venous thrombolysis can be defined in one of two ways
Restoration of antegrade in-line flow in the treated vein with abolition of any underlying obstructive lesion, and reduction or abolition of collateral drainage pathways; Percentage degree of thrombolysis – critically, this should be assessed on the venogram obtained after thrombus removal but before stent placement, as stent placement may well confer a venographically normal appearance even when there is residual thrombus – which obviously will falsely represent the true efficacy of thrombus removal.
Probably the most widely used system is that employed in the Venous Registry. 36
This applies to a single segment; but there are obviously several segments and each can be given separate weighting; some rely on the volume of thrombus removal (Ouriel), etc. Readers are encouraged to read the original references if they are sufficiently interested.
Recent trials and what they have shown us!
The CaVenT (catheter-directed venous thrombolysis in acute ilio-femoral vein thrombosis) trial was a randomised trial involving 209 patients in South East Norway first published in the Lancet in 2012. 44 The study compared standard therapy with anticoagulation in one arm and examined whether additional treatment with catheter-directed thrombolysis (CDT) using tPA reduced the development of post-thrombotic syndrome (PTS) at two years. Patients aged 18–75 years with a first-time ilio-femoral DVT were included within 21 days from symptom onset. Patients were randomly assigned (1:1) and stratified for involvement of the pelvic veins. Two primary outcomes were assessed namely the frequency of PTS as assessed by Villalta score at 24 months and ilio-femoral patency after six months. At completion of 24-months’ follow-up, data for clinical status were available for 189/209 patients (90%; 99 control, 90 CDT). At 24 months, 37 (41.1%) patients allocated to additional CDT presented with PTS compared with 55 (55.6%) in the control group (p = 0.047). The difference in PTS corresponds to an absolute risk reduction of 14.4% and the number needed to treat was seven. Ilio-femoral patency after six months was reported in 58 patients (65.9) on CDT versus 45 (47.4%) on control (p = 0.012).
This trial may be criticised for a variety of reasons including the relatively small numbers, with only 4 of the 20 hospitals actually performing CDT. The time period of 21 days from onset of symptoms is at the maximum most interventionists would consider appropriate for thrombolysis; this widened the inclusion and thereby hastened trial recruitment; but possibly at the expense of sub-optimal lysis as the fibrin receptor sites within the thrombus become depleted and so “fibrinolysis” should occur less frequently. The rate of stent placement was exceptionally low (17%) compared with most recent trials. The size of stents is not indicated nor the degree of dilatation, pressure, or whether both pre- and post-dilatation was performed as opposed to just pre or post. The six-month patency achieved in the ilio-femoral (IF) segment at 6/12 of only 65.9% was lower than comparable work. Thus, in many ways the trial was very “real world”, with some real world sub-optimal aspects. Nonetheless, despite these limitations, patients had a lower rate of PTS at two years with the addition of CDT. Even more telling, however, was the recently presented data (CIRSE 2015) of five-year follow-up which demonstrated an ever-widening gap between the two groups; those treated with additional catheter-based methods demonstrated progressively lower rates of PTS compared with the anticoagulation cohort. This trial, regarded by many as a technical failure, may actually show that even if with sub-optimal results – only about two-thirds of patients had a patent IF segment at 6/12 – (presumably due to the low rates of stent placement), but they still fare much better at five years than those treated by anticoagulation alone.
The second trial of note is the BERNUTIFUL trial involving U.S.-assisted CDT. 45 Ultrasound energy has been shown to cleave open the strands between thrombus and thereby expose the fibrinogen receptor sites to fibrinolysis. This trial randomised patients to either U.S.-assisted CDT vs. standard CDT. Forty-eight patients, mean age 50, 52% female, with symptoms of 14 days or less were treated with the same type of catheters, at the same dose, for the same duration (20 mg tPA over 15 h). In one arm, the ultrasound machine was turned on; in the other it was not. Both received the same dose of thrombolysis. A simple, elegant trial! The trial found that ultrasound assistance did not lead to a significant improvement in thrombus reduction using the LATS scale (Figure 2). The percentage thrombus reduction in both groups was 55% and 54%, respectively. At three-month follow-up, the primary patency was 100% in the U.S.-assisted group and 96% in the CDT group – these are superb results.
This trial is interesting in that the rate of stenting was high (>80%); the percentage thrombus reduction was relatively unimpressive (around 55%); nearly one-third of patients in both groups required further venous thrombectomy (suggesting neither 20 h CDT nor 20 h CDT plus EKOS were adequate in terms of adequate thrombus removal in one-third of patients) and yet the three-month patency was excellent at approximately 98% mean.
So these are two well-designed trials coming from completely different angles, both aiming at thrombus removal/dissolution; yet because the results are reported using completely different methods, it is difficult to draw useful conclusions. For instance, it is difficult to be certain whether the difference in of patency (far superior in Bern; albeit at 3/12 vs. 6/12 in Norway) is due to “better” thrombolysis or more liberal use of stents. It does tend to support the notion that stents are essential to relieve any underlying stenosis following thrombus removal. Which leads us to an interesting issue; could inadequate thrombus removal be masked by increasing usage of stents? Can one “over-stent”? One can certainly “under-stent” – this has to be my main criticism of the Norwegian data.
The CAtheter versus anticoagulation alone for acute primary (Ilio) femoral DVT (CAVA) trial is currently ongoing in the Netherlands; 47 it is designed to assess whether catheter-directed thrombolytic therapy for the treatment of IlioFemoral deep vein thrombosis (IFDVT) can safely and effectively reduce post-thrombotic morbidity after one year. The secondary objective is to study whether catheter-directed thrombolytic intervention has a positive effect on the quality of life of patients with IFDVT and to assess late PTS.
This is a randomized, controlled, multicenter, intervention study for acute (less than 14 days ilio-femoral DVT).
After randomization patients will be allocated to either conservative anticoagulant treatment or to CDT combined with conservative anticoagulant treatment.
Main study parameters/endpoints
The primary efficacy outcome is the incidence of PTS at one year; a decline in PTS incidence from 25% to 8% is anticipated. The secondary outcome is the health-related quality of life and late PTS during follow-up. The principal safety outcome is major bleeding during anticoagulant therapy. Bleeding as well as events of recurrent thrombosis will be monitored. The patency of the venous system of the affected lower limb will be assessed as well as the percentage of clot lysis (LET, The LOwer extremity VEnous pathology scoring system (LOVE)), after thrombolytic intervention. Additionally, measurements of markers of coagulation and inflammation will be performed during follow-up.
The Acute venous Thrombosis: Thrombus Removal with Adjunctive Catheter directed Thrombolysis (ATTRACT) trial 48 assesses PTS at two years and a host of other factors; data should be available early in 2017. It will use the Marder scoring system; but if the data are made open for all to see, it is quite possible that retrospective comparative analysis between the various scoring systems will enable us to evaluate critically which specific thrombolysis/thrombectomy combination technique is superior in thrombus removal PTS. I suspect the subgroup analysis of ATTRACT will run for some time, and the data should be riveting. In addition, the true place of stents should become more apparent.
Conclusion
LOVE score: Relating thrombus location, imaging findings (MRV), and quality of imaging, acute vs. chronic.

IVC: inferior vena cava; CIV: common iliac veins; EIV: external iliac veins; CFV: common femoral vein; PFV: profunda femoral vein; FV: femoral vein; PV: popliteal vein.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.