
Abstract
Introduction
Cyanoacrylate ablation is the newest nonthermal vein ablation technique. The one-year results of a prospective comparative study of a new cyanoacrylate glue versus endovenous laser ablation for the treatment of venous insufficiency is presented.
Material and methods
A total of 310 adult subjects were treated with cyanoacrylate ablation or endovenous laser ablation. The primary endpoint of this study was complete occlusion of the great saphenous vein. Secondary endpoints were procedure time, procedural pain, ecchymosis at day 3, adverse events, changes from baseline in Venous Clinical Severity Score, and Aberdeen Varicose Vein Questionnaire.
Results
Operative time was shorter (15 ± 2.5 versus 33.2 ± 5.7, <0.001), and periprocedural pain was less (3.1 ± 1.6 versus 6.5 ± 2.3, <0.001) in cyanoacrylate ablation group compared to the endovenous laser ablation group. Ecchymosis at the third day was also significantly less in cyanoacrylate ablation group (<0.001). Temporary or permanent paresthesia developed in seven patients in endovenous laser ablation group and none in cyanoacrylate ablation group (p = 0.015). One, three, and 12 months closure rates were 87.1, 91.7, and 92.2% for endovenous laser ablation and 96.7, 96.6, and 95.8% for cyanoacrylate ablation groups. Closure rate at first month was significantly better in cyanoacrylate ablation group (<0.001). Although there is a trend of better closure rates in cyanoacrylate ablation patients, this difference did not reach to the statistical difference at sixth and 12th month (p = 0.127 and 0.138, respectively). Both groups had significant improvement in Venous Clinical Severity Score and Aberdeen Varicose Vein Questionnaire postoperatively (<0.001), but there was no significant difference in Venous Clinical Severity Score and Aberdeen Varicose Vein Questionnaire scores between the groups at first, sixth, and 12 months. Only a slightly better well-being trend was noted in cyanoacrylate ablation group in terms of Aberdeen Varicose Vein Questionnaire scores (p = 0.062).
Conclusions
The efficacy and safety analysis shows that cyanoacrylate ablation is a safe, simple method which can be recommended as an effective endovenous ablation technique. The follow-up data more than one year will clarify the future role of cyanoacrylate ablation for the treatment incompetent great saphenous veins.
Keywords
Introduction
Endovenous thermal ablation techniques, such as radiofrequency, laser, and steam were introduced at the beginning of this century which have revolutionized the way varicose veins are treated.1,2 However, these techniques necessitate infiltration of tumescent anesthesia, which can cause severe discomfort for the patient. Bruising along the saphenous vein following thermal ablation, arteriovenous fistula, pseudoaneurysm formation, and neurological complications causing paresthesia are other potential side effects.3,4
Nonthermal techniques, such as foam sclerotherapy, might be the answer to these side effects. In a multicenter randomized trial involving 798 patients with varicose veins, the outcomes of foam, laser, and surgical treatments were compared. The disease-specific quality of life was slightly worse after treatment with foam than after surgery (P = 0.006), but there were no significant differences between surgery, foam, or laser groups in measures of generic quality of life. The successful ablation of the main trunks of the saphenous vein was less common in the foam group than in the surgery group (P < 0.001). 5
Two recent nonthermal, nontumescent methods are mechanochemical ablation and cyanoacrylate glue. These techniques do not use thermal energy therefore obviating tumescent anesthesia. The potential for nerve damage is minimal and midterm results appear superior to some studies of ultrasound guided foam sclerotherapy (UGFS).6,7
Endovenous ablation of both saphenous veins with cyanoacrylate glue for truncal ablation is a recent concept. 8 Cyanoacrylate glue has been used in the treatment of arteriovenous malformations for more than two decades in human without safety concerns. To date, no carcinogenic or mutagenic effect has been reported for cyanoacrylate glue.9,10 It has also been used in endoscopic intravenous injections of peptic varicosities for 20 years. 11 The purpose of this study was to assess the safety and efficacy of the novel VariClose cyanoacrylate ablation (CAA) of the great saphenous vein (GSV).
Materials and methods
Study protocol
In this prospective and independent study, 310 patients with lower limb varicose veins were treated between December 2013 and September 2014 (endovenous laser ablation (EVLA): n: 156, CAA: n: 154) (Figure 1). The inclusion criteria were primary varicosities with C2–C4b patients (clinical, etiological, anatomical and pathophysiological classification (CEAP)) and a sapheno-femoral junction (SFJ) incompetence and GSV reflux lasting longer than 0.5 s on duplex scanning. The exclusion criteria included a history of deep vein thrombosis, reflux of femoral vein going beyond the knee, hemodynamically significant reflux of the short saphenous or great saphenous anterior accessory vein, congenital vasculopathies, thrombophilia, severe systemic disease, pregnancy, breast feeding, as well as noncompliant patients for follow-up. GSV diameter > 15 mm was another exclusion criteria.
Flow chart. CAA: cyanoacrylate ablation; EVLA: endovenous laser ablation.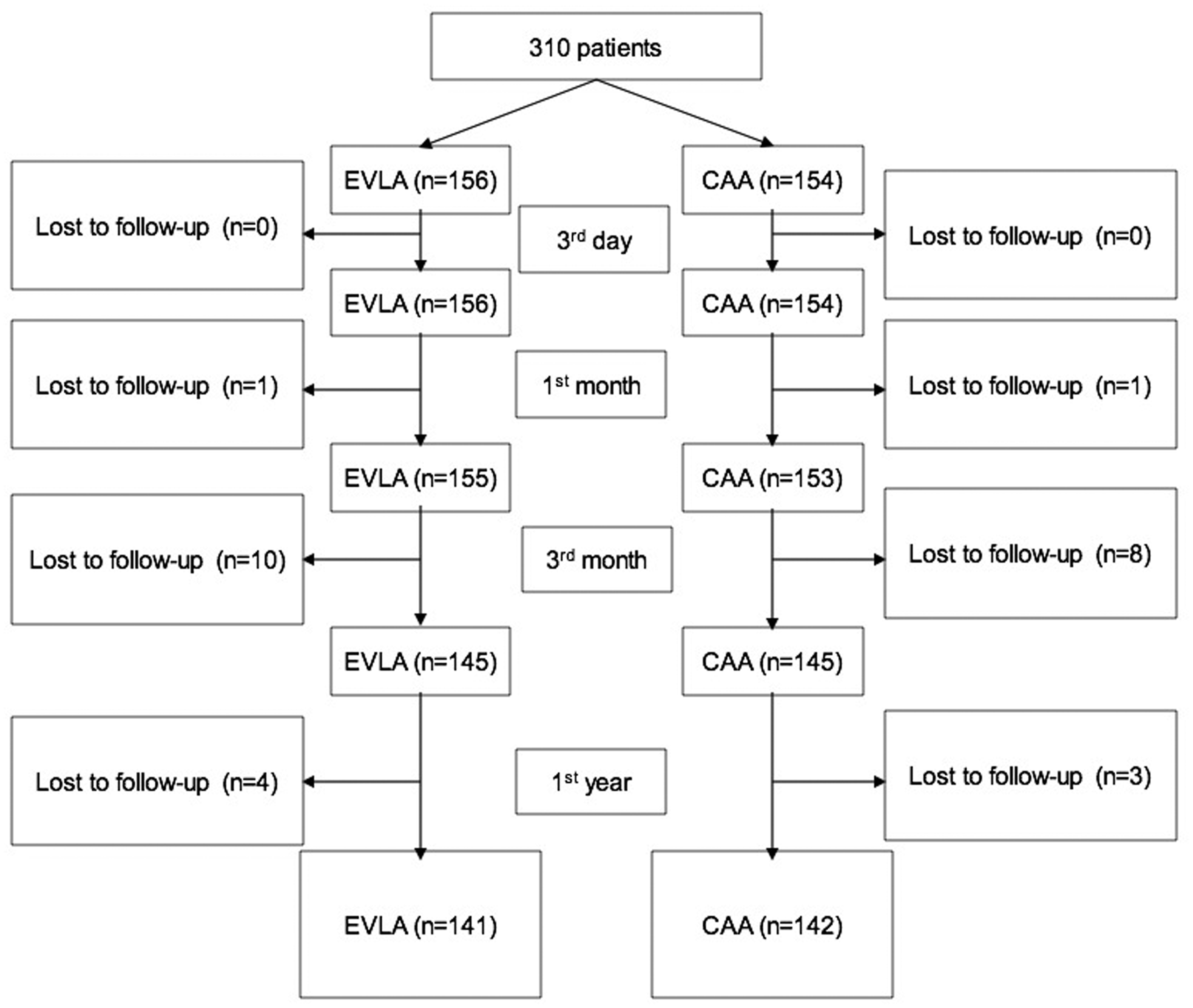
The screened patients were alternatively allocated to EVLA or CAA procedure in two vascular units, and the data collection was performed prospectively. No other concomitant procedures were carried out (i.e. microphlebectomy or perforator ablation) in order to be able to evaluate the safety and efficacy of the ablation method alone. The patients had foam sclerotherapy or microphlebectomy for the residual side branches after three months only if considered necessary. All patients provided written informed consent.
Assessment
Patients underwent clinical and ultrasound examination by a senior surgeon and allocated for endovenous ablation (CAA or EVLA) of the GSV. The assessment included demographic and baseline characteristics as well as the CEAP classification. The Venous Clinical Severity Score (VCSS) was also completed (0 represents no significant venous disease and 30 is the worse score). The diseased relation effect on QoL was determined using the Aberdeen Varicose Vein Questionnaire (AVVQ). The total score for the 13 questions ranges from 0 to 100 points, with 0 point indicating the best possible quality of life. 12
All procedures were carried out under local anesthesia with the use of standard sterile technique. The patients rated the procedural pain on a numeric visual analog scale of 0–10 (0 no pain, 10 extreme pain).
VariClose® procedure
The VariClose® Vein Sealing System (Biolas, Ankara, Turkey) includes 3 ml of VariClose polymer-based cyanoacrylate and a delivery system. The GSV is accessed percutaneously with a micro puncture introducer kit, followed by insertion of a 0.035 in. J guidewire. The lowest insufficient point of the vein was selected for the entry. The 5F introducer sheath was advanced over J guidewire to the SFJ under ultrasound control. The cyanoacrylate is extracted with a 3 ml syringe, which is then attached to the 4F delivery catheter and injection gun. This catheter has a hydrophobic design to help prevent cyanoacrylate-mediated adhesion to the vein wall and has a specific configuration to enhance sonographic visibility. The catheter is filled with cyanoacrylate except the final 3 cm segment. Delivery catheter is inserted into the introducer sheath and secured with a spinlock mechanism. Using direct visualization with a standard linear ultrasound probe in the long axis, 3 cm of the 4F catheter tip is exteriorized from the 5F introducer sheath and positioned 3 cm distal to the SFJ.
Injection technique
Injection gun is set up for continuous delivery. One slow pull of the trigger, while pressing for 5 s, gives 0.3 cc of polymer. Every pull (0.3 cc) should be applied for 10 cm length of the vein. The catheter was pulled back by 2 cm while pushing the trigger of injection gun. In every 5 s or 10 cm, trigger has been pushed again and continuous drawback was applied simultaneously. In this protocol 0.03 cc of polymer was given in every centimeter (Figure 2).
Injection technique suggested by Biolas/VariClose®.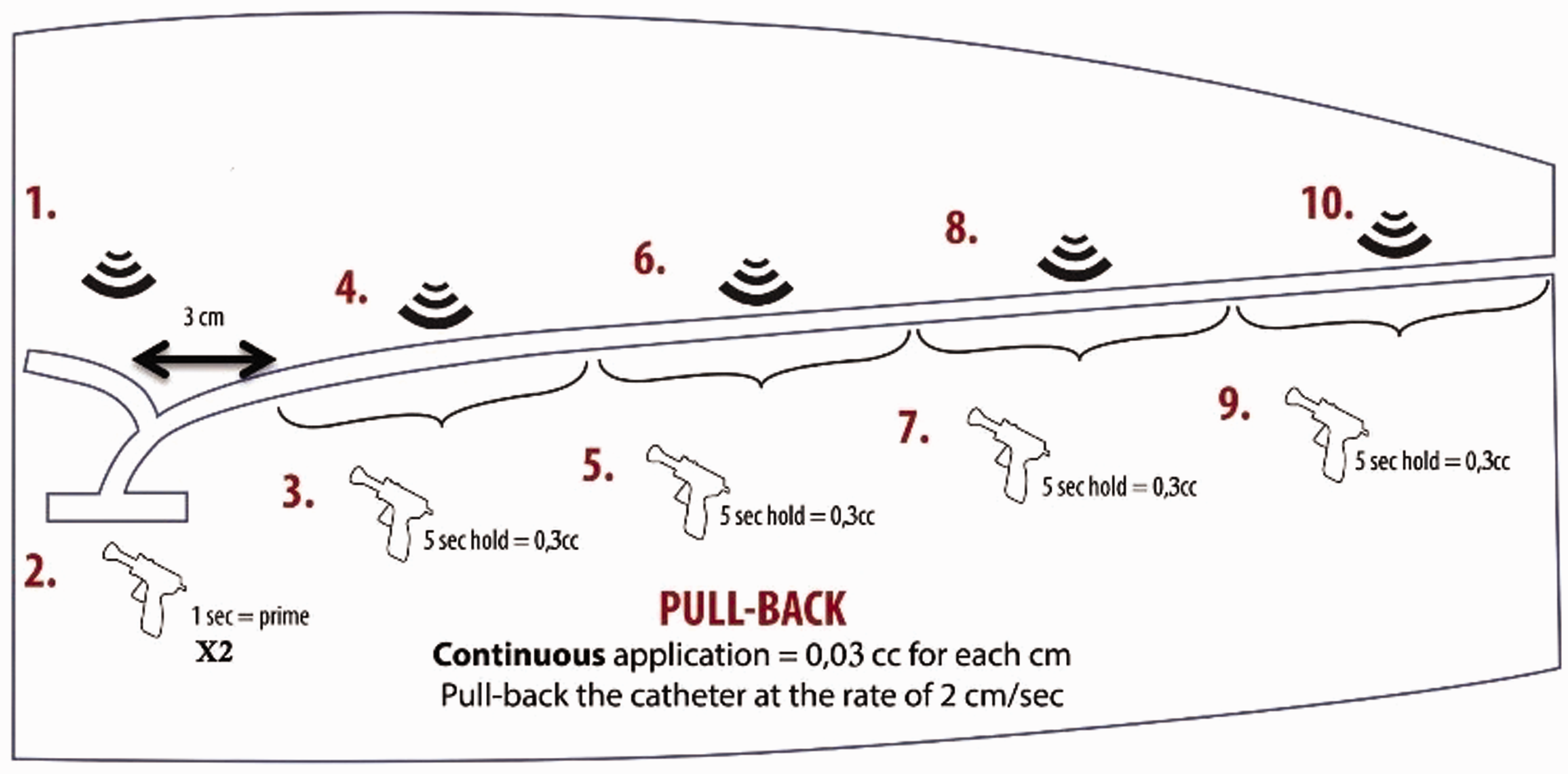
Pressure technique
Before the first injection, pressure was applied with the ultrasound probe over the SFJ in order to prevent migration of first bolus polymer in to the deep venous system. While pressuring SFJ, first injection of polymer was given continuously. Right after first injection pressure must be applied for the first 10 cm of vein for at least 5 s. Afterward, second polymer injection was carried out continuously under compression. Pressure technique was continued until the targeted vein segment fully sealed.
Endovenous laser procedure
The Evlas® Circular Fiber EVLA kit (Biolas, Ankara, Turkey) consisted of 600 µm of radially extending fiber that functioned at a wavelength of 1470 nm with the 6 F introducer kit. The laser fiber was advanced through the sheath and located to 1.5 cm distal to the SFJ. After confirmation, tumescent anesthesia was applied around the tissue surrounding the GSV. Thermal laser energy was applied from the SFJ to the access point at 10 J/cm/mm of the vein diameter.
Postprocedure management
In CAA group a single adhesive bandage is applied to the sheath introduction site; neither compression stockings nor compression bandages are used. Varicose stockings were prescribed for 10 days after EVLA procedure. The activity was not restricted and all forms of reasonable exercise were approved from the first postprocedure day.
Follow-up
Follow-up visits at third day, one month, six months, and 12 months were performed. At each visit an ultrasound study and clinical examination were performed. Ultrasonography criteria for technical success were closed or absent GSV with lack of flow. A recanalized GSV or treatment failure was defined as an open segment of the treated vein segment of >5 cm in length. Ecchymosis was confirmed 72 h after the operation (0, none; 1, involving up to 25% of the treated segment; 2, involving up to 50% of the treated segment; 3, involving up to 75% of the treated segment; and 4, involving all of the treated segment). Clinical assessment included VCSS and quality-of-life evaluation (AVVQ) at first, sixth, and 12th month. Adverse events were recorded at each visit.
Statistical analysis
Values are expressed as mean ± standard deviation or number and percentage (n, %). All comparisons of parametric variables with normally distributed quantitative data among groups were made by using Student’s t-test. Otherwise, the Mann–Whitney U-test and Wilcoxon Rank Sum test were used. Variables with qualitative nonparametric data were made by using X2 test and Fischer’s exact test. All statistical comparisons were made by using SPSS version 21 statistical package.
Results
The primary endpoint of this study was complete occlusion of the target GSV defined as Doppler ultrasound examination and any open segment over 5 cm was considered as failure. Secondary endpoints were procedure time, procedural pain, ecchymosis at day 3, changes from baseline in VCSS and AVVQ scores, and all adverse events.
Demographic and baseline data of the study subjects.
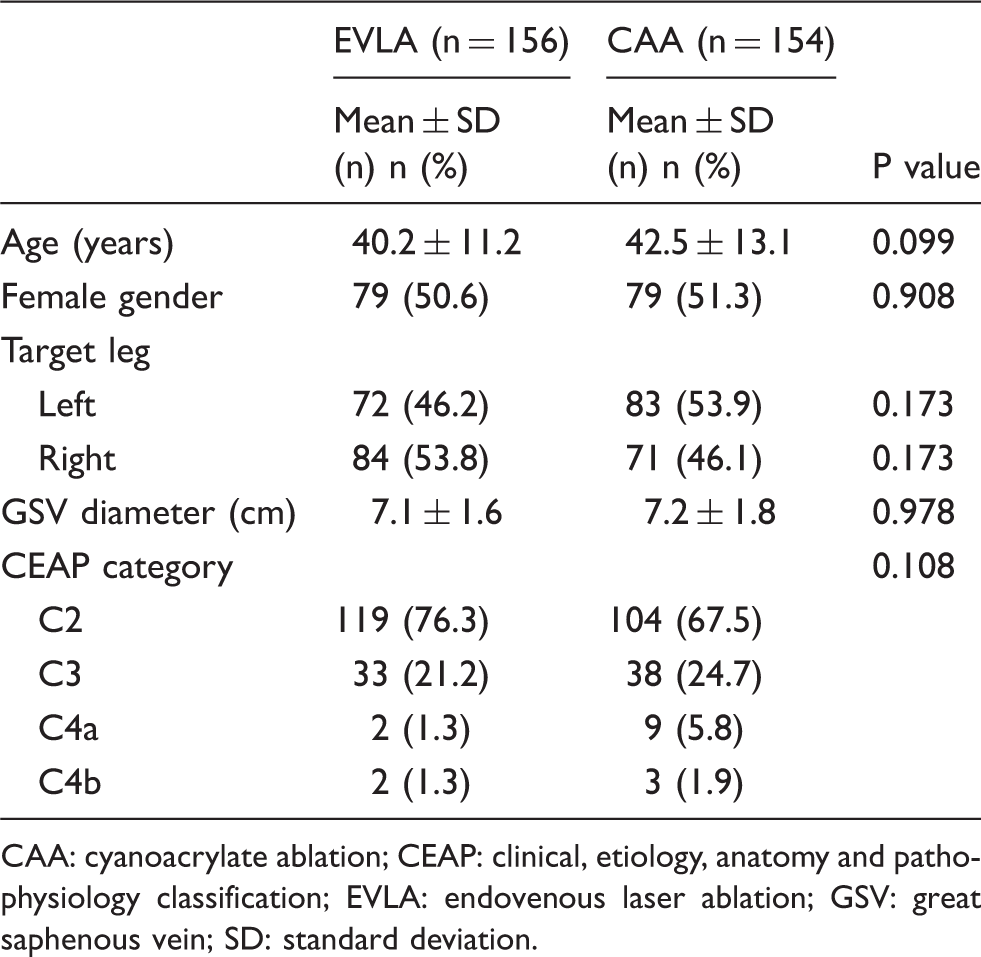
CAA: cyanoacrylate ablation; CEAP: clinical, etiology, anatomy and pathophysiology classification; EVLA: endovenous laser ablation; GSV: great saphenous vein; SD: standard deviation.
In both groups, treatment was successful with 100% ablation rate at the end of the procedure. Procedure time was shorter (15 ± 2.5 versus 33.2 ± 5.7, <0.001), and periprocedural pain was less (3.1 ± 1.6 versus 6.5 ± 2.3, <0.001) in CAA group. Phlebitis was encountered in 12 (7.7%) patients in EVLA group and seven (4.5%) in CAA groups (p = 0.248). Ecchymosis at the third day was significantly less in CAA group (<0.001). Temporary (n: 5) or permanent (n: 2) paresthesia was developed in seven patients in EVLA group and none in CAA group (p = 0.015).
Procedure characteristics and adverse events.
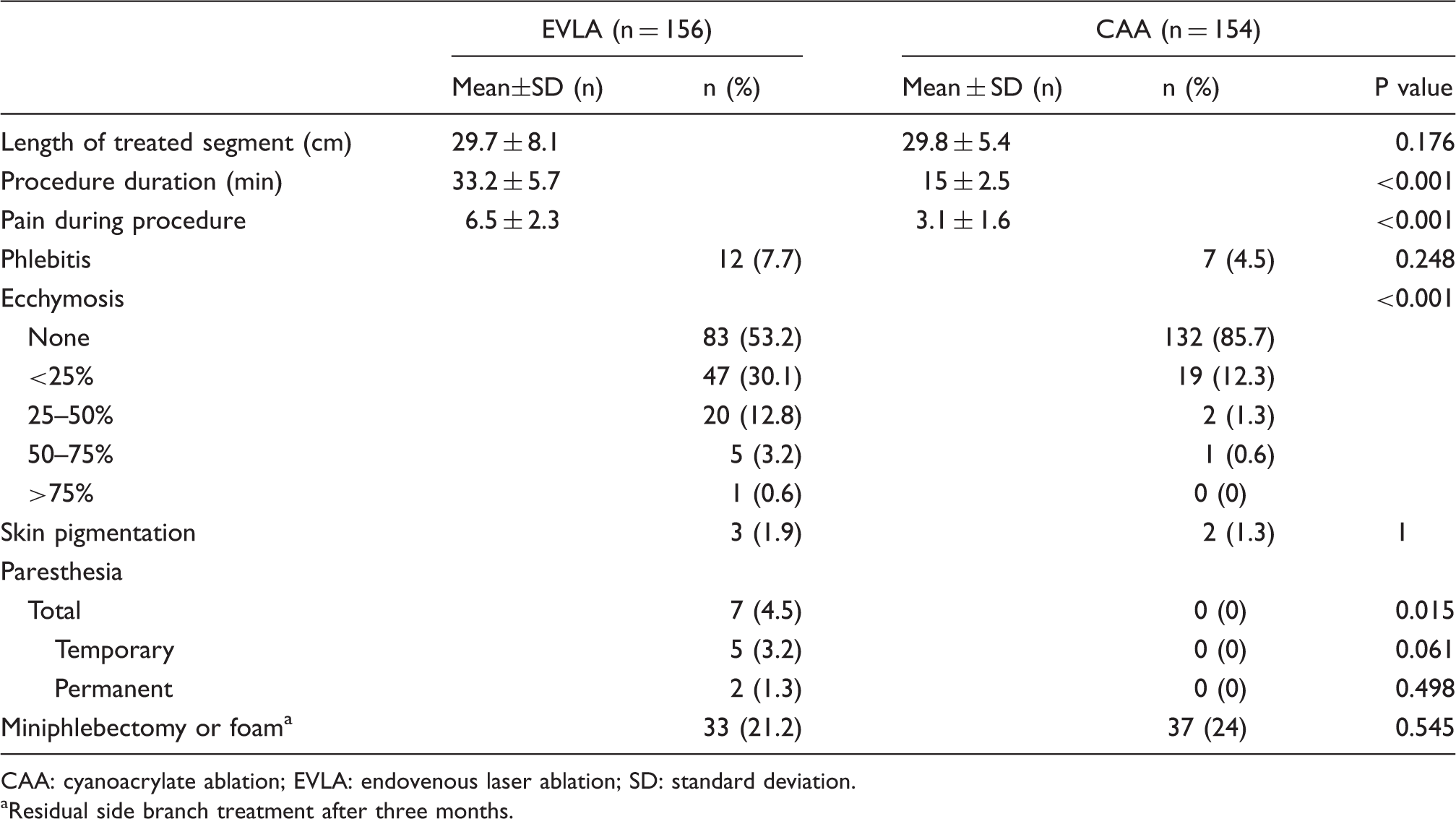
CAA: cyanoacrylate ablation; EVLA: endovenous laser ablation; SD: standard deviation.
Residual side branch treatment after three months.
Closure data
Closure rates.
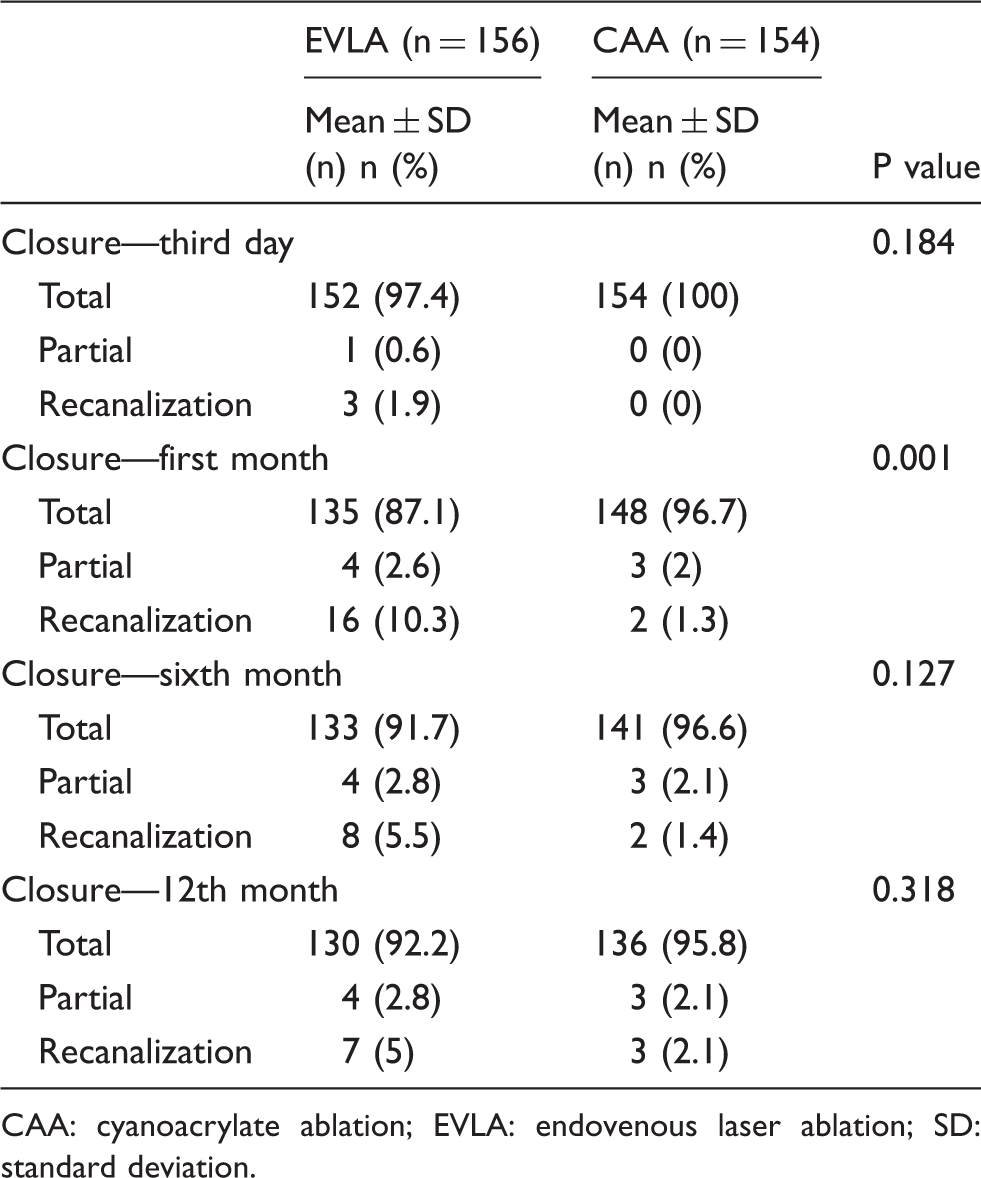
CAA: cyanoacrylate ablation; EVLA: endovenous laser ablation; SD: standard deviation.
QoL assessment
Post procedure clinical assessment.

AVVQ: Aberdeen Varicose Vein Questionnaire; CAA: cyanoacrylate ablation; EVLA: endovenous laser ablation; SD: standard deviation; VCSS: Venous Clinical Severity Score.
p value of repeated measures analysis of variance.
Discussion
One of the disadvantages of thermal endovenous ablation of truncal incompetence for patients with varicose veins is the requirement for tumescence anesthesia which can be a source of procedural discomfort, hematoma, and ecchymosis. Moreover, applying tumescent anesthesia is the most difficult part of the learning curve and requires additional procedural time. Foam ablation is a cheap and effective alternative and gaining popularity especially in Europe. In a study reported by Darvall et al., 391 limbs were followed up at a median of 71 months following first UGFS. Eighty-two percent of the patients were very satisfied with their treatment, 91% would recommend the treatment to others. The retreatment rate was found to be 15.3% by five years. 13 However, foam is still not considered as the first-line treatment for truncal reflux in the current guidelines.1,2
An alternative heatless technique, cyanoacrylate glue, has been introduced recently. The mechanism of cyanoacrylate is simple: plasma and blood stimulate the polymerization and lead to closure of the target vein. Wang et al. demonstrated that when cyanoacrylate mixed with lipiodol was injected into rabbit veins, the vessels were obliterated immediately. 14
Almeida et al. published the results of two-year clinical follow-up on 38 patients who underwent treatment of their symptomatic varicose veins with cyanoacrylate glue. 8 They found the occlusion rate of 92.0% at 24 months follow-up. VCSS improved in all their patients from a mean of 6.1 ± 2.7 at baseline to 2.7 ± 2.5 24 months, respectively (p < .0001). They found no significant side effects or complications. Their patients did not have any deep vein thrombosis or pulmonary embolism. However, Proebstle showed that the first 8 of 38 (21%) patients had postablation thrombus extension through the SFJ. 15 Further modification of their technique with the first cyanoacrylate injection located 5 cm from the SFJ seemed to have eliminated any further postablation thrombus extension.
In eSCOPE trial, 70 GSVs in 70 patients were treated, and follow up to one year was completed in 60 (86%) patients. Life table occlusion rates were 98.6% at two days, 95.7% at three months, and 94.3% at six months. Phlebitis occurred in six cases (8.7%). 16 In a randomized trial of cyanoacrylate embolization (CAE) versus radiofrequency ablation (RFA) conducted by Sapheon, 222 patients with symptomatic GSV incompetence were randomized CAE (n = 108) with the VenaSeal System or RFA (n = 114) with the ClosureFast system. Three-month closure rates were 99% for CAE and 96% for RFA. Pain experienced during the procedure was similar. At day 3, less ecchymosis in the treated region was present after CAE compared with RFA (P < .01). The authors reported that CAE was found to be noninferior to RFA for the treatment of incompetent GSVs at month 3 and is associated with less postprocedure ecchymosis. 17
VariClose received European CE Mark approval for the treatment of varicose veins on 23 December 2013 and had full reimbursement from Turkish National Health System. Thereafter, this study was planned as a totally independent study by two cardiovascular surgeons treating both private (AKB) and National Health Service patients (MFY). Although it is not an official randomized trial because of the cost-related factors, the alternated allocation caused the groups to be perfectly comparable allowing to conclude on the primary and secondary outcome measures. Because no serious adverse events were registered during the 12-month follow-up, our findings suggest that the VariClose procedure is safe.
The VariClose endovenous ablation system differs for several aspects. First, the product that we used in the present study was a low viscosity cyanoacrylate that provided immediate polymerization and a sealing effect in fewer than 5 s. This polymerization enabled very rapid procedures. One slow pull of the trigger, while pressing for 5 s, gives 0.3 cc of polymer. Polymerization is composed of three stages as defined by Kailasnath and Chaloupka in an explanted pig carotid artery model: (1) fast polymerization stage with increasing tensile forces for approximately 10 s, (2) second stage with stable tensile force for up to 1 min, and (3) final polymerization stage with fast and logarithmic expanding of tensile force. 18 Polymerization time may differ according to the CA type, formulization, and intravascular salt and blood levels. Our method is based on low viscosity and faster polymerization time of cyanoacrylate compared to the higher viscosity and slower polymerization in the VenaSeal method.
The second difference of VariClose is continuous delivery application. Following SFJ closure (confirmed by pressing with ultrasonography probe) and placing the catheter 3 cm distal to the SFJ, continuous cyanoacrylate delivery and at a rate of 2 cm/sec pullback was applied. This continuous delivery method and fast polymerization enables to give cyanoacrylate to each centimeter of the vein (0.03 cc/cm). We believe in this technique, development rate of thrombophlebitis is lower, as there is no empty space filled without glue and no residual blood inside the vessel. Besides, and at least theoretically, rapid closure and minimal procedural time may prevent deep vein thrombosis. Because the glue polymerized so quickly, the SFJ portion of the GSV was rapidly closed, and the application of the correct amount of pressure over the SFJ reduced the risk of flow into the deep vein. Alm reported that in his series of 246 CAA patients, the first 41 patients were treated according to the VenaSeal recommendations with the catheter tip placed at 5 cm from the SFJ in order to prevent deep vein thrombosis. Because of the some long stumps up to the 5 cm after the procedure, he changed the protocol and in the subsequent patients, the adhesive catheter was filled completely and placed distally to the epigastric vein at a minimum distance of 15 mm without thromboembolic complications. We suggest to be 3 cm distal to SFJ and fill the catheter until 3 cm from the tip of the catheter. None of the patients in this series, both CAA and EVLA, developed venous thromboembolism. 19
In this this study, 141 of the 156 patients (90.4%) in EVLA group were evaluated at the end of 12th month, and obliteration of the GSV was 92.2%. This closure rate is comparable to the best published results for endovenous laser and radiofrequency at the same follow-up. In CAA group, 142 of the 154 patients (92.2%) had 12th month follow up with 95.8% complete closure. Our assessment suggests that CAA procedure is as efficacious based on 12 months follow-up. During the procedure, few patients complained of pain, and ecchymosis on third postprocedural day was less in CAA patients. These two positive findings can be explained by elimination of heating the perivenous tissue and obviating tumescent anesthesia. Certainly eliminating the most time-consuming part of the procedure is a perfect goal both for the patient and physician. Nerve injury is an important concern for full-length GSV thermal ablation and short saphenous vein ablation. CAA seems to be the solution for these clinical scenarios. Neuropathy manifesting as paresthesia developed in seven (4.9%) patients in the EVLA group in this series. Although in five cases the symptoms resolved completely, has remained persistent in other two subjects. None of the patients in the CAA group experienced paresthesia after the procedure. Finally, in this series, none of the patients used varicose stockings in CAA group with satisfactory follow-up data, and this is an important advantage for the compliance of the patients.
There are two limitations of this study: First, this was not a real randomized and external monitored study, and second, closure of the veins was not confirmed by an independent ultrasound core laboratory. The investigators planned this project as a prospective independent research without financial support from any source, and it was therefore impossible to include an independent ultrasound core laboratory or a monitoring company because of the financial restrictions.
Conclusions
These initial results showed that this novel cyanoacrylate glue appears to be safe and efficacious out to one year. The technique eliminates the need for tumescent anesthesia, improves patient discomfort, shortens the physician learning curve, shortens procedure time and obviates compression stockings. The great majority of incompetent GSVs can be treated with this technique.
Footnotes
Acknowledgements
We would like to thank Ozan Onur Balkanay MD for statistical analysis of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.