
Abstract
Herpes simplex virus infection following surgery is an unusual postoperative phenomenon. Many mechanisms have been suggested, with the most likely explanation related to latent virus reactivation due to a proinflammatory response in the setting of local trauma. Here, we present a case of herpes simplex virus reactivation in an immunocompetent female following a conventional right lower extremity stab phlebectomy. Salient clinical and physical examination findings are described, and management strategies for herpes simplex virus reactivation are outlined. This is the first known case report of herpes simplex virus reactivation following lower extremity phlebectomy.
Case report
A 42-year-old female presented for management of progressively enlarging right lower extremity varicose veins associated with aching, throbbing, and burning. Her past medical history was significant only for papillary thyroid cancer that was treated with thyroidectomy and radioactive iodine therapy in 2003. Physical exam was remarkable for normal lower extremity arterial pulses with small varicose veins, CEAP Class CII, of the right anterolateral calf. No evidence of advanced venous disease was identified.
A three-month trial of conservative management consisting of compression stockings, lower extremity elevation, and non-steroidal medications was attempted without significant amelioration of her symptoms. A right lower extremity venous reflux examination was performed, which revealed significant focal reflux in the distal small saphenous vein. The varicosities in the right anterolateral aspect of the mid-calf did not communicate with the small saphenous vein. Therefore, the decision was made to proceed with conventional phlebectomy.
A right lower extremity stab phlebectomy was performed with a total of 17 1-mm-long incisions under conscious sedation. Vein diameters were variable and of moderate caliber, predominantly all less than 1 cm. No local anesthesia was used. The extremity was wrapped in a layered compression dressing at the end of the procedure. The patient tolerated the procedure well and was discharged from the surgical center.
On postoperative day 1, the patient developed two erythematous plaques with overlying eschars and few small, slightly fluid-filled vesicles on the skin of her right upper back and underneath the right breast in a non-dermatomal distribution (Figure 1). The rash was preceded by pruritus and pain. She had no fever and otherwise felt well. She was referred for evaluation by a Dermatologist, who made a diagnosis of herpes simplex virus (HSV) on the basis of the patient’s clinical presentation. No laboratory testing was performed. The patient had a remote history of chicken pox, but no history of HSV, herpes zoster, or other skin rashes in the past. She was treated with valacyclovir with complete resolution of her HSV-related symptoms and clinical findings within 14 days of presentation.
On post-operative day 1 following right lower extremity stab phlebectomy, the patient developed a vesicular erythematous rash on the skin of her right upper back (panel a) and underneath the right breast (panel b) in a non-dermatomal distribution, consistent with HSV infection.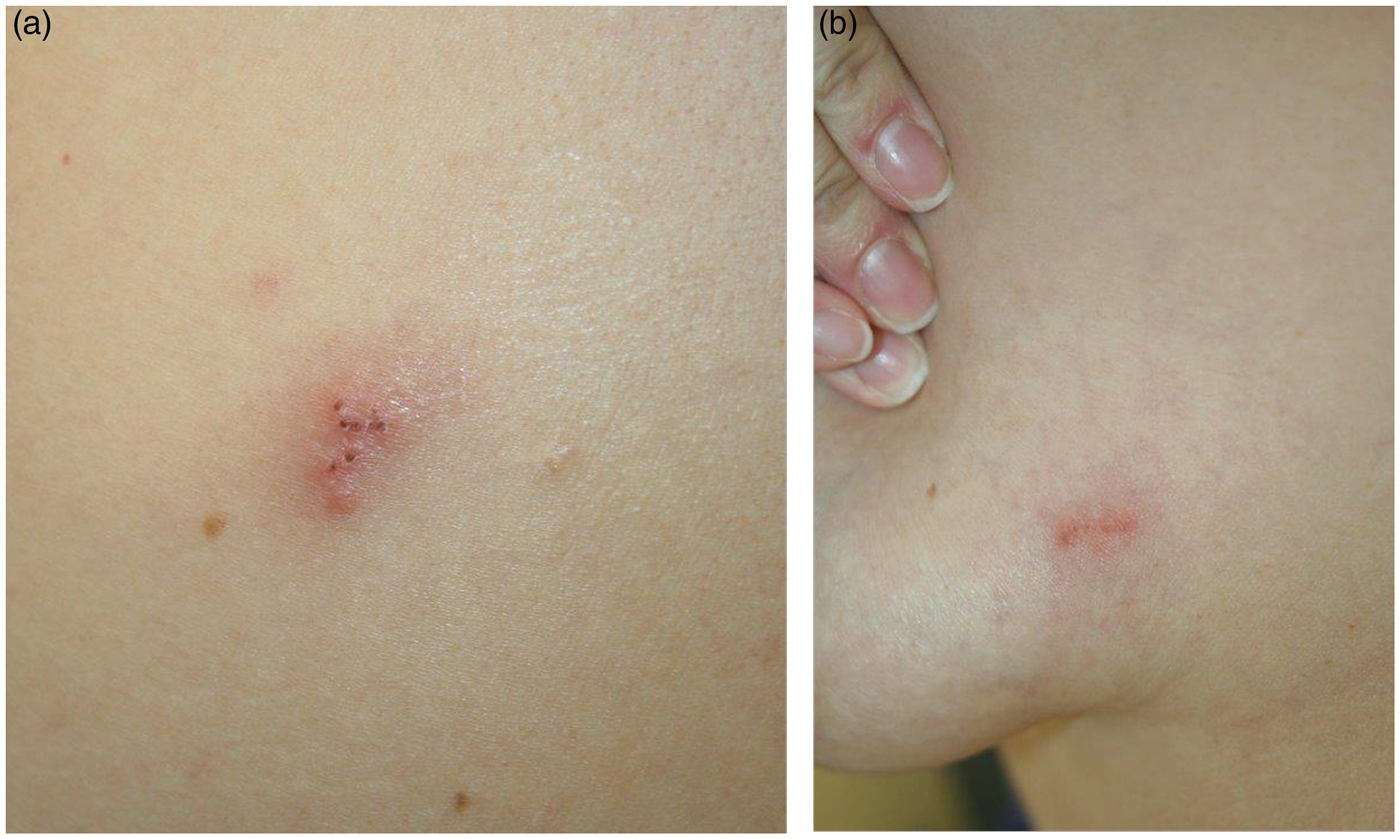
Discussion
HSV is estimated to affect approximately 23.6 million people per year. 1 The number of cases precipitated by surgical trauma is unknown. HSV infections are the result of infection with HSV-1 or HSV-2, which typically causes vesicular lesions of the oral mucosa and genitalia, respectively. Inoculation occurs via mucosal surfaces or the skin, usually at sites with disrupted epithelial integrity, which allows the virus to enter into the epidermis, dermis, and eventually sensory and autonomic nerve endings. Primary infections develop suddenly, and generally begin with a prodrome period characterized by pruritis and pain. This is followed by the development of vesicles on an underlying erythematous base. Affected patients may report fevers, malaise, neuralgia, and/or lymphadenopathy as well, although the majority of primary HSV infections (>70–80%) are asymptomatic.
Once primary HSV infection has occurred, the virus persists in a latent state within skin cells or nerve cell bodies, and thus can reactivate and cause recurrent symptoms. Among immunocompetent patients, commonly reported HSV reactivation triggers include sunlight, fever, menstruation, and emotional stress. In rare cases, surgical procedures have been reported to play a role. 2 There are a few case reports of HSV reactivation following cosmetic procedures, including photoablative therapy, face lift, breast augmentation, and liposuction.2–5 Although the precise mechanism of HSV reactivation in surgical cases is unclear, local trauma and inflammation and/or the generation of heat near a nerve root containing latent virus have been implicated. Consistent with this notion, there are reports of HSV infections adjacent to recent surgical scars, and HSV prophylaxis is now advocated for patients undergoing laser resurfacing to prevent virus reactivation as a result of the mechanical trauma associated with those procedures. 6 HSV reactivation following superficial venous interventions has not previously been reported in the literature, but presumably could present as the result of this same proinflammatory process.
Management strategies for HSV infection among immunocompetent patients include symptomatic treatment only, episodic management, or chronic suppressive treatment with oral antiretroviral agents (i.e. acyclovir, famciclovir, valacyclovir). 7 Although an HSV vaccine is currently in development, clinical trials suggest poor efficacy for preventing HSV disease and the vaccine is not currently recommended. 8 At this time, there are no formal recommendations for the use of HSV prophylaxis among patients undergoing invasive surgical procedures; rather, the indications for treatment are determined based on patient symptoms, risk, and the procedure to be performed.
In the case we report above, the patient underwent a superficial venous procedure with subsequent HSV prodromal symptoms presenting within 24 hours of surgery. Consistent with the natural history of recurrent HSV infections, she presented with pain and pruritus followed by the local eruption of vesicles on an erythematous base on her back and right breast. Although HSV following conventional stab phlebectomy has never been reported previously, reactivation of her HSV infection may have been triggered by the inflammatory response associated with the procedure. It is interesting to note that her rash occurred remote from the phlebectomy site. It is possible that the hook mechanism of the phlebectomy itself caused a proinflammatory cascade sufficient to trigger a latent subcutaneous HSV reactivation, because no injectable anesthesia or other potentially traumatizing agents were used in the area where her HSV erupted. Less likely, the use of conscious sedation may have also played a role. Given the unusual nature of this patient’s presentation, use of prophylactic antiretroviral therapy might be considered for her prior to future invasive procedures in the hope of preventing reactivation.
Footnotes
Patient consent
The patient described herein provided written informed consent for her information and images to be published.
Ethical approval
This manuscript was exempt from Institutional Review Board Approval.
Guarantor
JH.
Contributorship
CH, YL, and JH researched literature, conceived the project, and collected data. JH obtained patient approval. CH and JH drafted the original version of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.