
Abstract
Objectives
Anomalous intraosseous venous drainage is a rare and almost unknown entity; only 14 cases have been reported in the literature and 4 mentioned in textbooks. We report the characteristics of 35 further cases observed in 32 patients.
Method
After the presentation of two cases at the congress of the French Society of Phlebology in Paris (2013), 12 colleagues joined to present a large series of so-called bone perforators observed in their practice, all identified with at least a duplex investigation.
Results
Thirty-two patients suffering from varicose veins and/or skin changes (C2−C6) associated with a bone perforator of the tibia (with bilateral anomalies in three) are reported: 19 females and 13 males, average age 56.9. The majority of the affected legs were symptomatic (30/35). Bone perforator was an isolated finding in 27/35 legs. In three cases, the investigations revealed that the venous reflux in the bone originated from an incompetent posterior tibial vein.
Conclusions
We suggest the name of “bone perforators” for an anomalous tibial intraosseous venous drainage, feeding varicose veins, and in more advanced stages lipodermatosclerosis and leg ulcers. Most of them were successfully treated with surgery or sclerotherapy.
Keywords
Introduction
Determination of the origin of venous reflux in varicose veins and/or skin changes related to chronic venous insufficiency (CVI) is imperative before any treatment. Duplex is presently the standard investigation to establish the venous flux and reflux. Insufficiency from saphenous veins and/or junction, and perforators, is the most frequent finding in chronic venous disorders (CVD). However, non-saphenous veins incompetence may also cause CVD and CVI.
Described in 1962, 1 rediscovered in 1997, anomalous intraosseous venous drainage is a rare and almost unknown cause of venous reflux and varicose veins. 2 We report 35 observations in 32 patients of what we consider to be a “bone perforator.”
The bone perforator may be defined as an abnormally large communicating vein between the superficial veins and the intra-osseous venous network, through a round-shaped bone defect, almost always located on the anterior aspect of the tibia. If the bone perforator is incompetent and feeds varicosities, the venous reflux and the bone defect may easily be detected with duplex ultrasound but also with different radiological investigations.
Patients and methods
Table I. 35 cases of bone perforators.
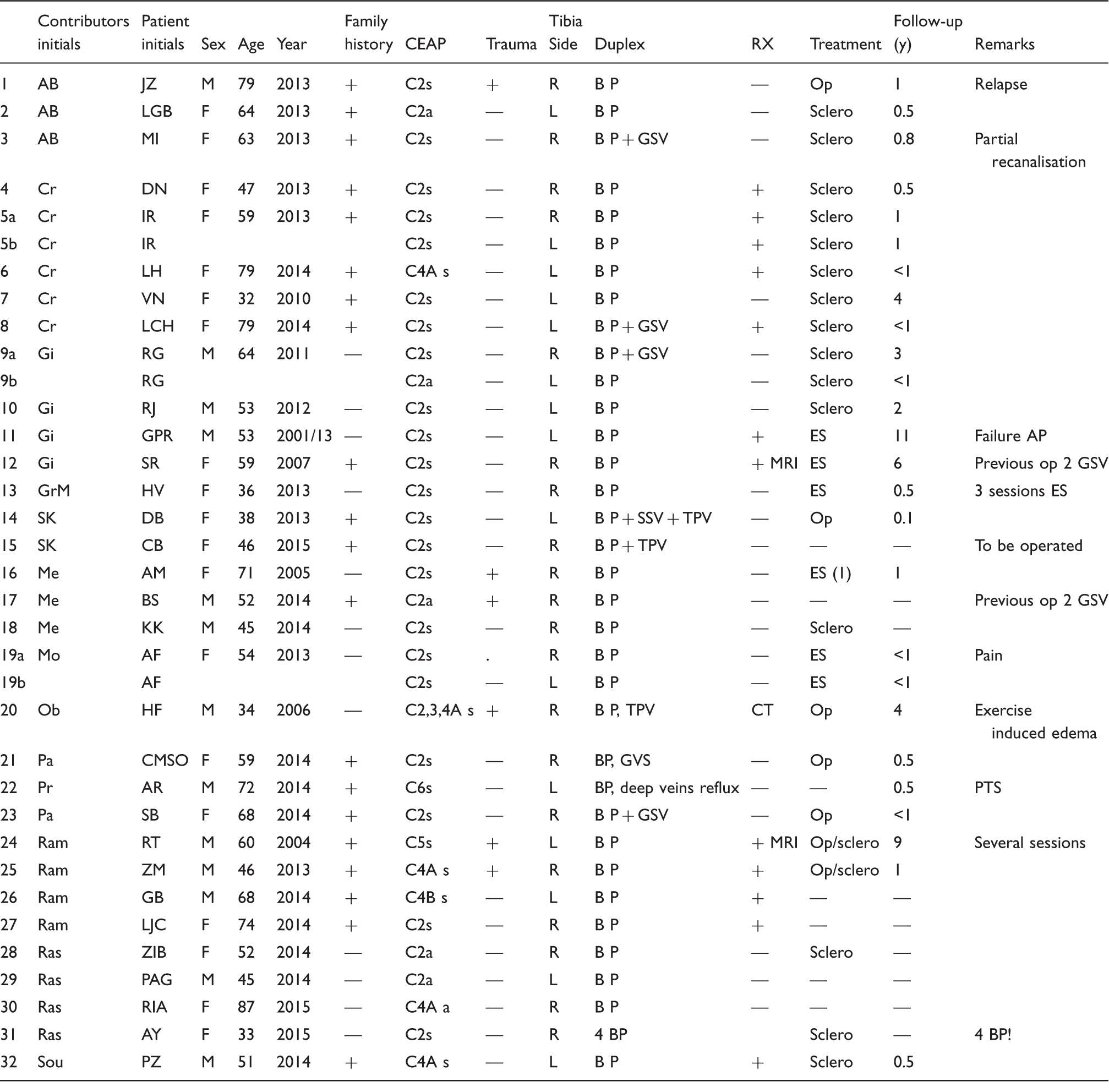
CT: Computed tomography; ES: Echosclerotherapy (Duplex Ultrasound Guided Sclerotherapy); GSV: Great Saphenous Vein; MRI: Magnetic resonance imaging; Op: Operation, including Phlebectomy; PTS: Post-thrombotic syndrome; RX +: Presence of a tibial cortical defect and an enlarged nutrient canal; SSV : Short Saphenous Vein; Tibia R (right side), L (left side); TPV: Tibialis posterior veins and tributaries; Sclero: Sclerotherapy (1 or several sessions)
Results
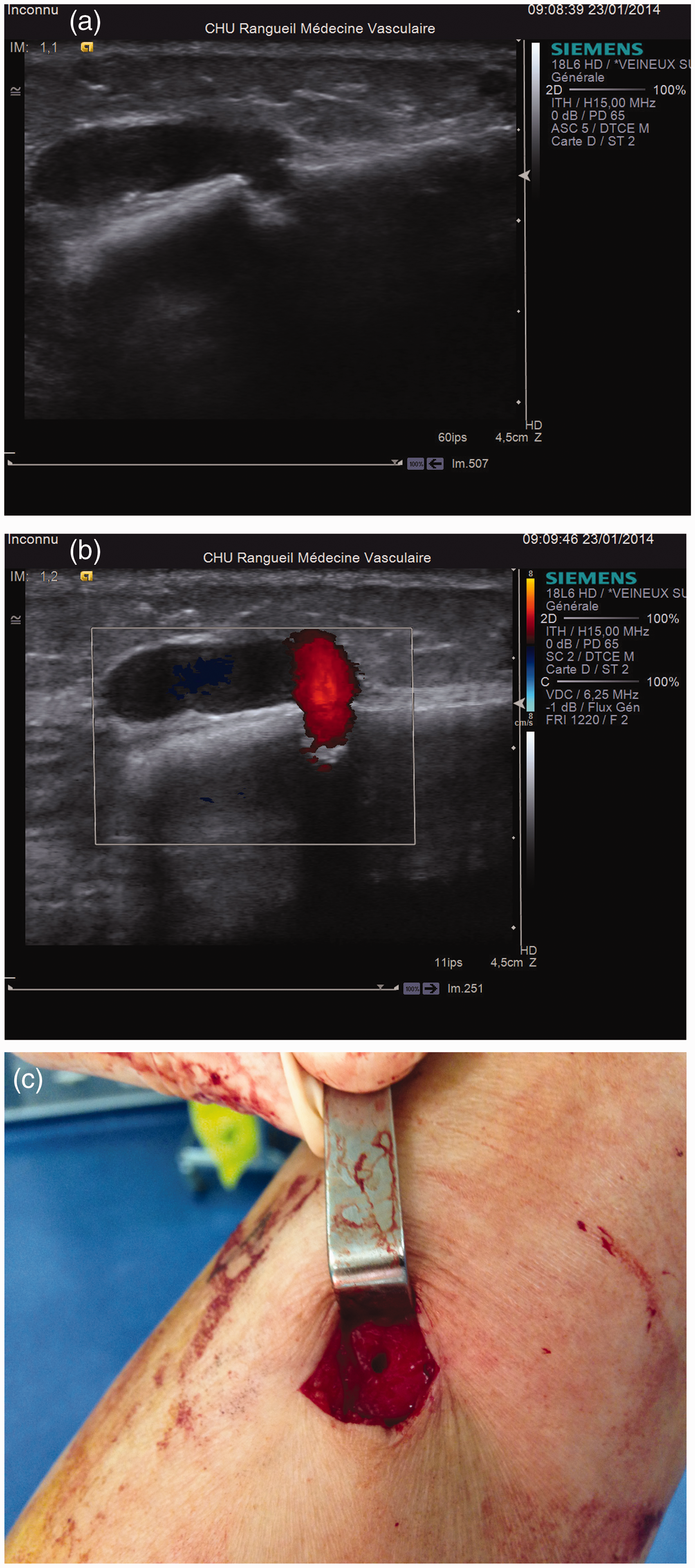
Between 2006 and 2015, 13 office-based phlebologists from six countries identified 32 patients presenting with varicose veins or skin changes consecutive to incompetent bone perforators of the medial aspect of the tibia. Mean age was 56.9 years (range 32−87), including 19 females (mean age 56.2; 32−87) and 13 males (mean age 57.3, 34−79). Bone perforator was located on the right tibia in 20 patients and on the left tibia in 15 patients (three cases with bilateral perforators). Family history of varicosities was positive in 20/32. History of trauma to the concerned leg was reported only in six patients. Thirty legs were symptomatic and five asymptomatic. Varicose veins (class C2 of the CEAP classification) were the single sign of CVD in 26 legs, skin changes (C4A/B) were observed in 6 legs, venous ulcer (C6) in 1 leg, and healed ulcer (C5) in 1 as well (Figures 1 and 2). Venous edema (pitting test positive, C3) was not mentioned in the files, except in one case.


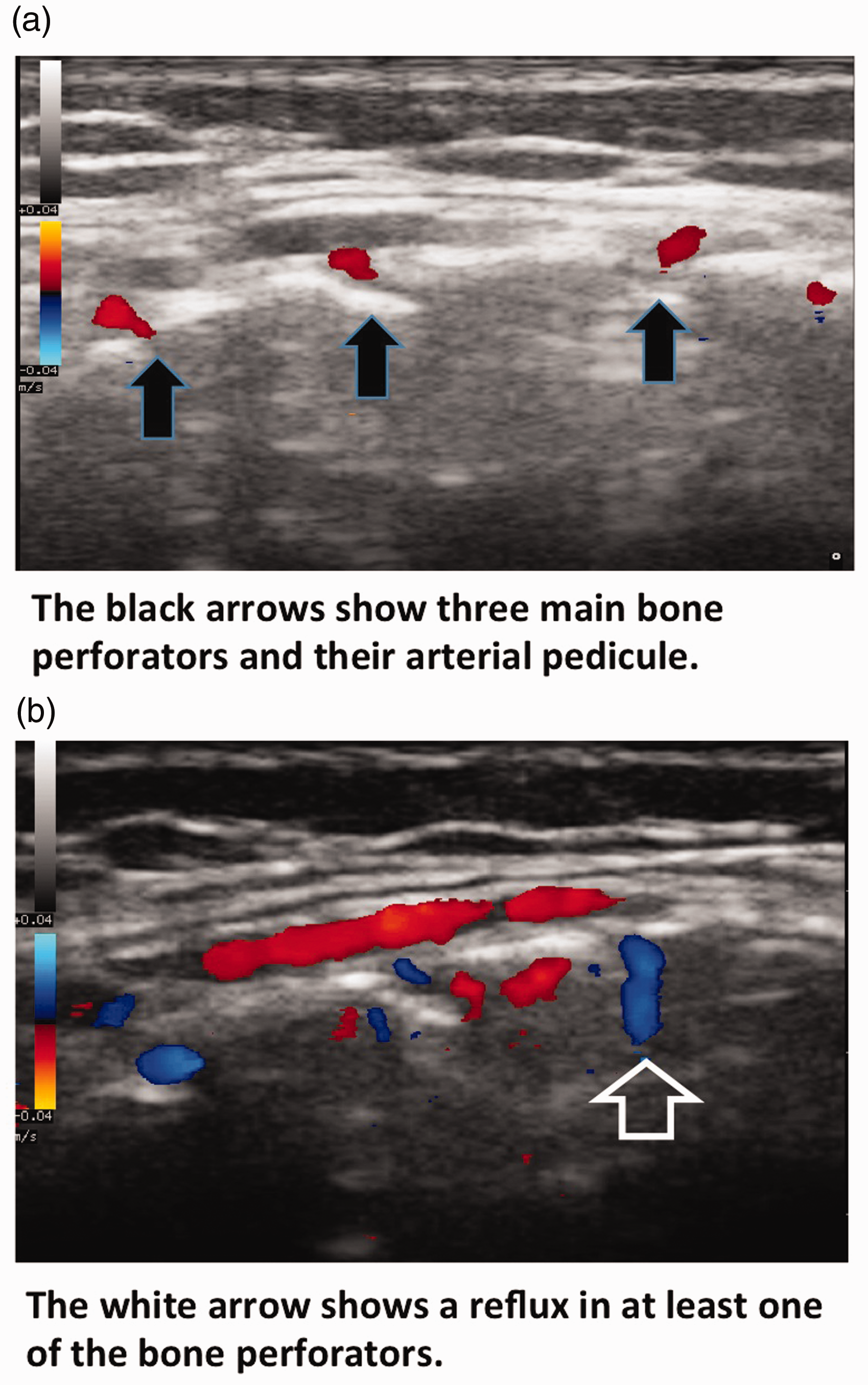
Bone perforator of the tibia was an isolated finding in 25 legs but was associated to great saphenous vein incompetence in 5 legs, short saphenous vein insufficiency in 1 leg, and deep vein reflux in 4 patients. One of these suffered from post-thrombotic syndrome. In the other three patients, a reflux from a tributary of the posterior tibial vein, filling the bone marrow of the tibia in a retrograde fashion, induced a recirculation through the bone perforator. Several bone perforators were observed on the same tibia in patient no. 31.
Conventional radiographies of the tibia were performed in 12 legs. All of them presented the typical image of a small lytic defect on the anterior aspect of the tibia diaphysis, associated to an enlarged longitudinal groove as described by several radiologists.2,4–7
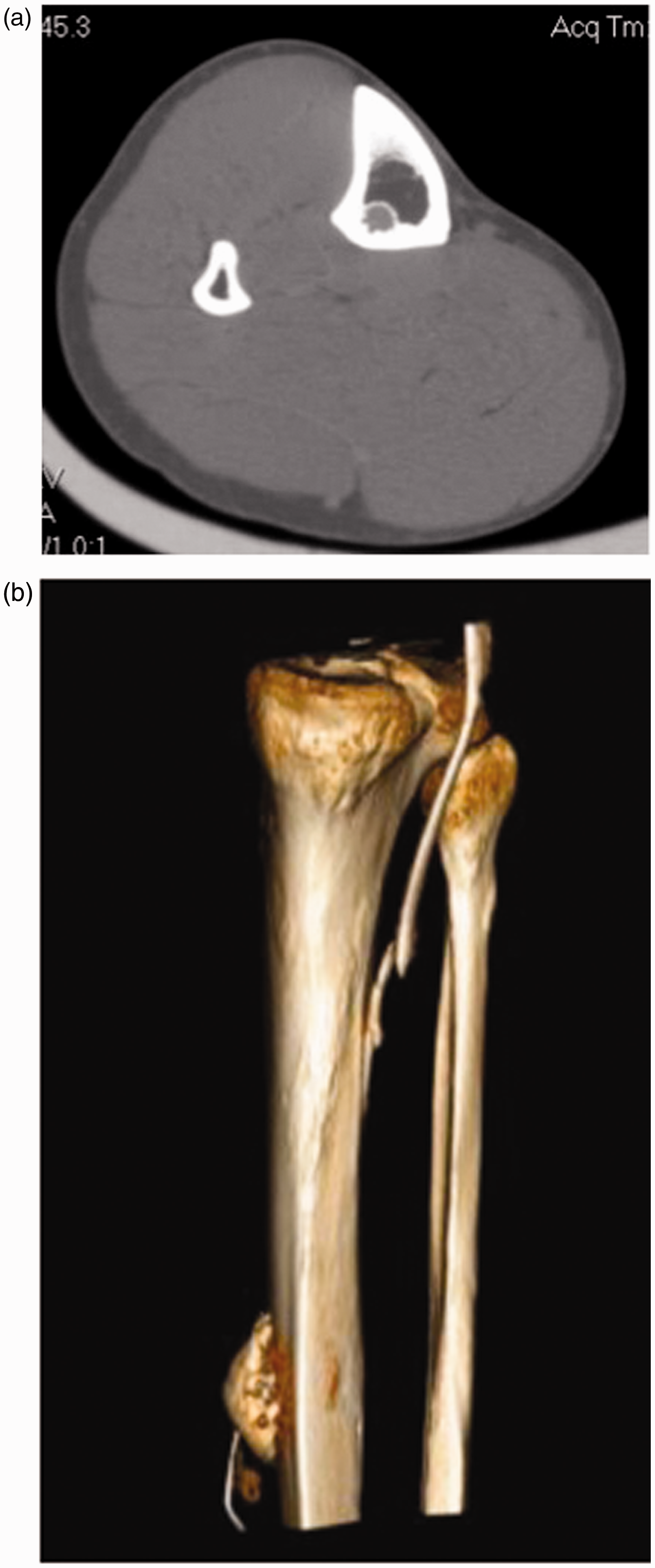
Magnetic resonance imaging (MRI; two legs) and computerized tomography scan with reconstruction (CT; one leg) revealed superficial varicosities, a round-shaped bone defect of the tibia, and an enlarged nutrient canal in the affected tibial diaphysis. A reflux from a branch of the posterior tibial vein, filling the bone marrow of the tibia in a retrograde fashion, inducing a recirculation into the bone perforator was observed in three legs, either by duplex or CT scan. 8
Treatment (one or several sessions) was performed in 26 symptomatic legs, mostly liquid and foam sclerotherapy (13 legs), or echoguided sclerotherapy, 6 or a combination of sclerotherapy and surgery, 2 or surgery. 5
Complications were rarely reported. Severe pain after echosclerotherapy occurred in one 54-year-old female patient. Surgical dissection of the varicose vein down to the bone, at the perforator's emergence, provoked in all cases an important intra-operative or post-operative haemorrhage. Massive bleeding was controlled in one 34-year-old male patient by tamponade of the bone perforator using a previously removed varicose vein. Treatment failure was reported in three patients.
Discussion
In most cases, varicose veins and their complications originate from junction or segmental insufficiency of the saphenous veins or from perforator incompetence. Less frequently, venous reflux takes place in non-saphenous veins, including pudendal varicosities, persistent embryonic veins, veins along the course of the sciatic nerve, among others.
Anomalous intraosseous (or transosseous) venous drainage is a rare and mostly ignored cause of venous reflux and varicose veins, described in one patient in 19621 and in six patients in 1997. 2 Nine cases of chronic venous disorders due to this entity have been published then, all in Radiology Journals, except three.3,9,10 Four further cases are illustrated in textbooks11,12 or reviews. 8 All patients presented with venous reflux originating from the tibia, except one issued from the fibula. 4
According to our 32 patients, clinical presentation depends on the length of evolution and the importance of the reflux. It varies from pretibial varicosities (C2) (Figure 1) to skin changes, including lipodermatosclerosis (C4B) and leg ulcer (C5-6) (Figure 2). Astonishingly, venous edema (C3) was reported in only one observation, probably because this sign is poorly defined and used in practice, except for severe swelling complaints. Swelling was the major complaint in the first published case in the literature. 1
The majority of our patients were symptomatic (30/35 legs) as in other publications. However, this is not conclusive, as asymptomatic patients are less frequently investigated than symptomatic ones.
Duplex is the standard investigation of CVD and demonstrates easily the defect of the anterior shaft of the tibia, with a typical venous reflux through the osteolytic defect of the anterior tibial cortex, feeding subcutaneous varicosities (Figure 3(a) to (c)).3,6,7,9,11,12 In one patient (no. 31), several bone perforators were observed on the same tibia (Figure 4). Duplex may also demonstrate reflux in posterior tibial veins and its tributaries extending into the tibia bone, as observed by one of us (SK) in his two patients.
This reflux has not been mentioned in other files, but it is probable that it was not looked for in most cases.
Plain radiography of the mid tibia is an economic and specific approach to demonstrate a round osteolytic defect (2−4.5 mm diameter), perforating the anterior cortex of the bone. This foramen communicates with a proximal, longitudinal radiolucent groove (“double railway track aspect”) (Figure 6(a)).2,3,5,7,9 This nutrient vascular groove is quite usual and has been observed in 23/25 controls.
2
However, it is enlarged when communicating with incompetent bone perforators.

CT and MRI findings of intraosseous perforating vein incompetence consist of varicose veins in the pretibial soft tissues, a dilated intraosseous nutrient vein, and an enlarged nutrient canal in the affected tibial diaphysis (Figure 6(b)).2,5–7 Multiplanar reconstruction of venous CT scan demonstrates the transtibial route of the venous reflux, originating from the tibial veins, extending through a bony channel to the bone perforator and the varicosities (Figure 7(a) and (b)). CT and MRI may also exclude vascular malformations. In 1962, osteomyelography was used in one case, this tibial intra-osseous venogram demonstrating the drainage of the refluxing vein into the proximal deep vein system.
1
Vascularization of the tibia is mainly supplied by a vascular arterial and venous pedicle, which penetrates into a foramen through the posterior cortex of the diaphysis and joins the vessels of the epiphysis. On the outside of the bone, the periost is richly vascularized. Blood communicate physiologically between the endosteal and periosteal network through tiny transosteal “perforators.”2,9,13 We have no evidence of the presence of valves in these tiny communicating veins, which are normally not involved in the control of venous pressure differences. Only one histopathological study of the perforator vein, including perivenous tissue and bone has been performed, but did not reveal the presence of valves. 1
Anomalous venous drainage of the tibia may correspond to a dilatation of one of these foramina, as suggested by echography and conventional radiographies.
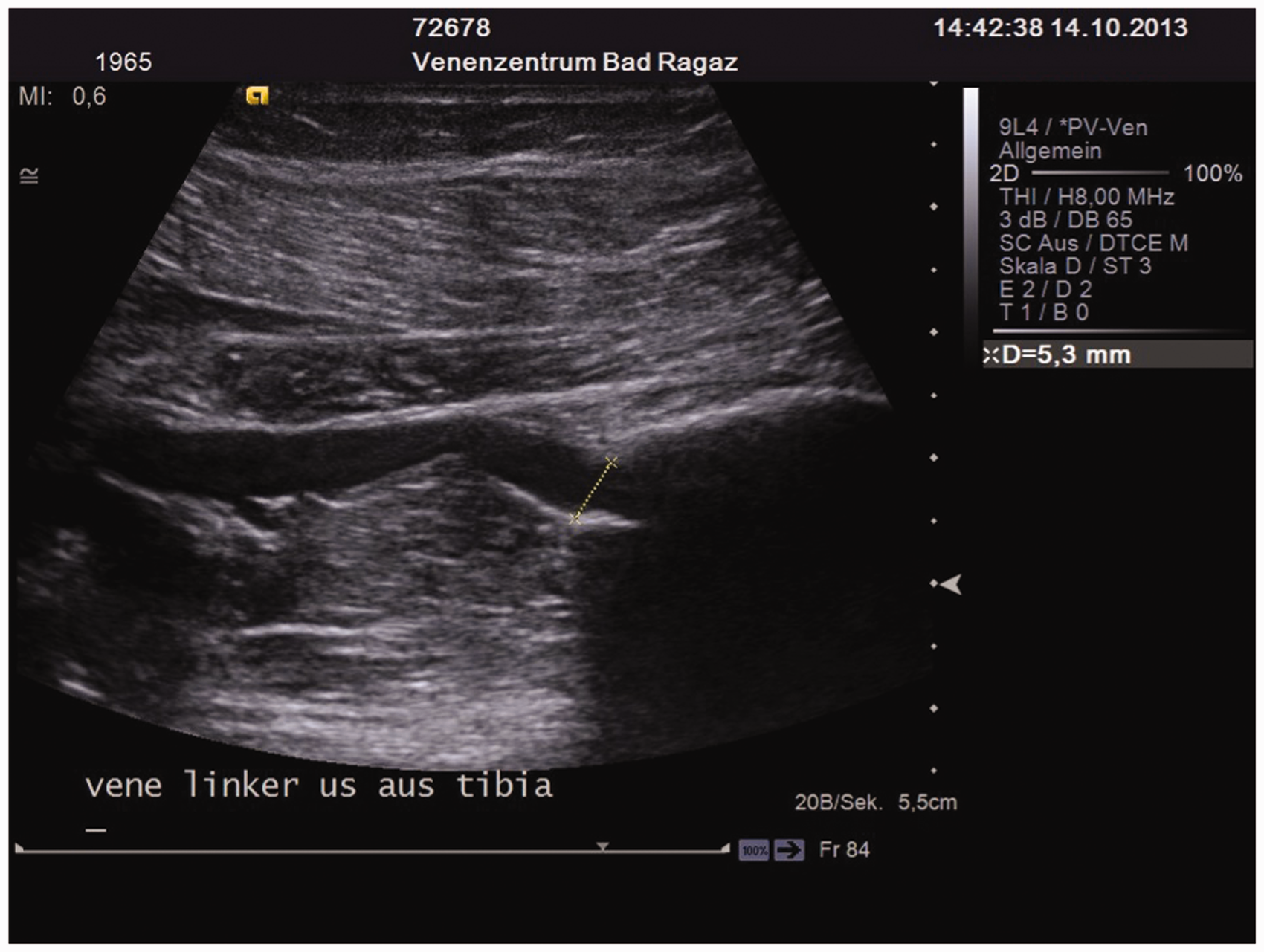
Intraosseous venous hyperpressure may be induced by a reflux in the venous drainage of the tibia, consecutive to a deep vein insufficiency. A reflux of an enlarged tributary (up to 5 mm) of one posterior tibial vein, filling the bone marrow of the tibia in a retrograde fashion, inducing a recirculation into the bone perforator was demonstrated by duplex in two cases of incompetent bone perforators with varicosities (patient nos. 14 and 15, Figure 5). The same anomaly was detected in case no. 20. This patient had a muscular systolic and diastolic blow out through the bone perforator during dorsiflexion of the foot and release. A varicography and a CT with contrast medium and multiplanar reconstruction were performed to detect the origin of this blow out. Venous reflux spread from a branch of the posterior tibial vein, penetrating the posterior cortex of the tibia, descending for 8.5 cm in a bony channel backside in the medullary cavity, escaping to the subcutaneous side varicosities (Figure 7(a) and (b)). Then, the high pressure in the deep tibial compartment escaped from the posterior tibial veins transtibial to the medial located varicose veins. 8 This reflux into the bone has been detected in three patients but was not mentioned or looked after in previous observations. This reflux is impressive in surgery. A massive haemorrhage originates from the bone when the varicosities and the perforator are removed (all three cases treated by surgery, publication by Schobinger. 1 ). This demonstrate a strong intra-osseous venous hyperpressure. It may be a common explanation for varicose veins issued from bone perforators in some patients.
A major traumatism of the concerned extremity occurred in only 6 of 34 legs. In four cases, trauma may be criminated in the incompetence of the bone perforator (patient nos. 16, 17, 20, and 24). 7 Vein lesions consecutive to traumatism may explain intraosseous venous hyperpressure in some cases (demonstrated by CT scan in patient no. 20). There was no history of trauma to the affected leg in other cases of our series. The patient reported by Schobinger suffered from a severe injury of the leg years before. 1 However minor trauma such as contusions have not been reported in the files, although they may induce varicosities, and via a siphon effect an incompetent bone perforator. Banal contusions may also cause some alterations in transosseous communicating veins (post-traumatic veins). In one patient, several bone perforators were observed on the same tibia (Figure 4). This particular aspect may suggest a malformation, as the occurrence of bilateral bone perforators in 3/32 patients.
A bone perforator was associated to saphenous insufficiency (five long saphenous vein and one short saphenous vein) in 6/35 legs. This association may be coincidental.
The presently used appellation “anomalous intraosseous venous drainage” is long and complicated. We suggest the term of “bone perforator.” 3 According to usual definitions, “the perforating veins or perforators are called such as they perforate the aponeurosis” and these “must be distinguished from the communicating veins which anastomose different veins in the same network.” 13 Concerning these transosteal vessels, it is logical to define them as “bone perforator,” as they perforate the cortex.
Bone perforators and pretibial varicose veins should be treated, in particular if they are symptomatic or induce skin changes, with a correction of saphenous insufficiency if present, and removing or obliterating varicosities.
Which treatment may we suggest? Stockings are probably not an appropriate option. Compression therapy reduces trans-mural pressure by means of an additional extravascular pressure. In superficial venous disorders, this treatment at least relieves symptoms. As bone perforators are mostly located in areas where curvature radius is high, compression therapy by stockings is probably not an appropriate treatment option. Consequently, bandages with additional eccentric compression would be haemodynamically better but of course not applicable on a practical point in our patients. Then, other treatments are preferable.
Surgery is effective, with a risk of relapse after several years, as in case 23 (Figure 6). Meticulous dissection of the varicosities may demonstrate the bone perforator (Figures 3(c) and 8). This foramen, with a potential important bleeding, may be occluded by tamponade with a peroperatively removed varicose vein, as performed in patient no. 20 (Figure 8).

Sclerotherapy and ultrasound-guided sclerotherapy, either with liquid or foam, were not performed in the first cases reported in the literature, by fear of a potential risk of deep venous thrombosis, and as compression of a bone perforator cannot be assured after the procedure. However, in our experience, this treatment is quite effective and well tolerated (21/32 of our patients; one case of transitory pain), either with polidocanol or sodium tetradecyl sulfate (STS), as a solution or foam (0.5–1.0% polidocanol). One bone perforator was treated effectively by Peh et al. 5 with ethylic alcohol, with a transitory pain. Sclerotherapy has to be performed at some distance of the perforator and not directly in it, to avoid damaging a satellite artery. In several of our patients, the superficial injection of foam was stopped at the entrance of the geode, to avoid diffusion into the bone. Intraosseous injection of sclerosant agents is, however, well tolerated and considered to be safe: 38 consecutive patients suffering from aneurysmal bone cysts have been successfully treated with percutaneous sclerotherapy with polidocanol. 14
A combination of surgery and sclerotherapy is a reasonable choice in the treatment of varicosities due to bone perforators (two patients of our casuistic).
Treatment results have to be interpreted with caution. Several sessions may be necessary to achieve good results after the different modalities of sclerotherapy and/or surgery. The result of the treatment is considered as good if varicosities and intra-osseous reflux disappear. Follow-up is short in the majority of cases. One of our patients (no. 24) was operated twice, years before developing a leg ulcer, two different surgeons dissecting the perforator down to the bone foramen and occluding the orifice with glue.
Conclusions
Bone perforators are certainly under reported, as duplex investigation is often limited to the saphenous veins and major perforators. Bone perforators should be carefully looked for in all cases of atypical or recurrent pretibial varicose veins of the leg. The origin of the venous intraosseous hyperpressure should be investigated, in particular along the posterior tibial veins and their tributaries.
Treatment is mandatory in presence of symptoms and/or skin changes.
Recognition of this rare and particular entity can prevent misdiagnosis, as arterio-venous malformations, and is essential in performing appropriate treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AAR
Contributorship
AAR conceived the study, performed the review of the literature, and wrote the first draft of the manuscript. All authors made a substantial contribution to the acquisition, analysis and interpretation of data. They reviewed and edited the manuscript and approved the final version.