
Abstract
Objective
To highlight current practice patterns in management of superficial vein thrombosis.
Methods
An electronic survey was conducted using the mailing lists of the Mediterranean League of Angiology and Vascular Surgery and European Venous Forum regarding superficial vein thrombosis diagnosis, investigation, and treatment.
Results
The response rate was 41% (175/430) and the majority of the participants were vascular surgeons practicing in a hospital. More experienced physicians considered superficial vein thrombosis as a medical issue of moderate seriousness and performed duplex ultrasound for confirmation of diagnosis. Elastic stockings were recommended by 87% of the physicians, while 57% prescribed nonsteroidal anti-inflammatory drugs. Eighty six percent advised anticoagulation, although a large disparity was shown regarding regime, dose, and duration. Thrombophilia test was regularly suggested by 19% of the physicians. Ligation of the saphenofemoral junction was the treatment of choice by those who suggested intervention in the acute phase of superficial vein thrombosis.
Conclusions
A great disparity exists in the management of superficial vein thrombosis. Current guidelines have not been adopted by physicians; more focused training is needed for those involved in the management of venous diseases.
Introduction
Superficial vein thrombosis (SVT) is a common disease, affecting 3–11% of the general population.1,2 In patients with varicose veins (VVs), the incidence of SVT increases up to 60%.2,3 A recent study has characterized SVT as a superficial form of venous thromboembolism (VTE) sharing the same risk factors. 2 In addition, SVT has been implicated as a risk factor for the development of deep vein thrombosis (DVT) and/or pulmonary embolism (PE).1–4 Despite the potential severity of SVT, this condition has not been studied in a systematic manner.
The management of SVT has been provided by recently published studies.5–8 Duplex ultrasound (DUS) is required to confirm the diagnosis, to estimate the extent of thrombus, to exclude the presence of DVT, and for follow up.2,3,5,9,10 In a large placebo-controlled randomized trial, subcutaneous administration of Fondaparinux 2.5 mg for 45 days was associated with a significant reduction in symptomatic VTE, SVT extension, and recurrence.8,11 Others recommend low-molecular weight heparin (LMWH) in intermediate doses for at least one month.5,12
Nowadays, various specialties including vascular surgery, dermatology, general practice, and general surgery are involved in the management of SVT. Despite current recommendations, the level of compliance shown by physicians is low, probably due to the lack of consistent education and training in venous pathologies.12,13
The objective of this study was to highlight the current practice patterns in diagnosis, investigation, and treatment of SVT. For this purpose, a survey was conducted under the guidance of the Mediterranean League of Angiology and Vascular Surgery (MLAVS) and European Venous Forum (EVF).
Methods
Survey monkey questions.
Invitations to participate to the survey were sent through the EVF and MLAVS mailing lists. The questionnaire was sent to physicians practicing in Central, Northern European, and Mediterranean countries including Egypt, Lebanon, Algeria, Turkey, Israel, and Tunisia. As per the preset protocol, after the initial invitation up to four, more email reminders were sent to those not responding. Data were extracted by the Survey Monkey server and results were analyzed using the SPSS 20 statistical software (IBM, Chicago, IL, USA). A Spearman’s correlation analysis was performed and p < 0.05 was considered significant.
Results
The questionnaire was sent to 430 physicians. There was a 41% (175/430) response rate with the vast majority of the responders being vascular surgeons (80%) (Figure 1). Most of the participants (58%) were practicing in a hospital (regional, general, or tertiary) and the remaining in private practice. Thirty eight percent had more than 25 years of experience in their field, while over 50% of the participants managed less than 50 cases with SVT per year (Figure 2).
What is your specialty? How many patients with SVT do you manage every year?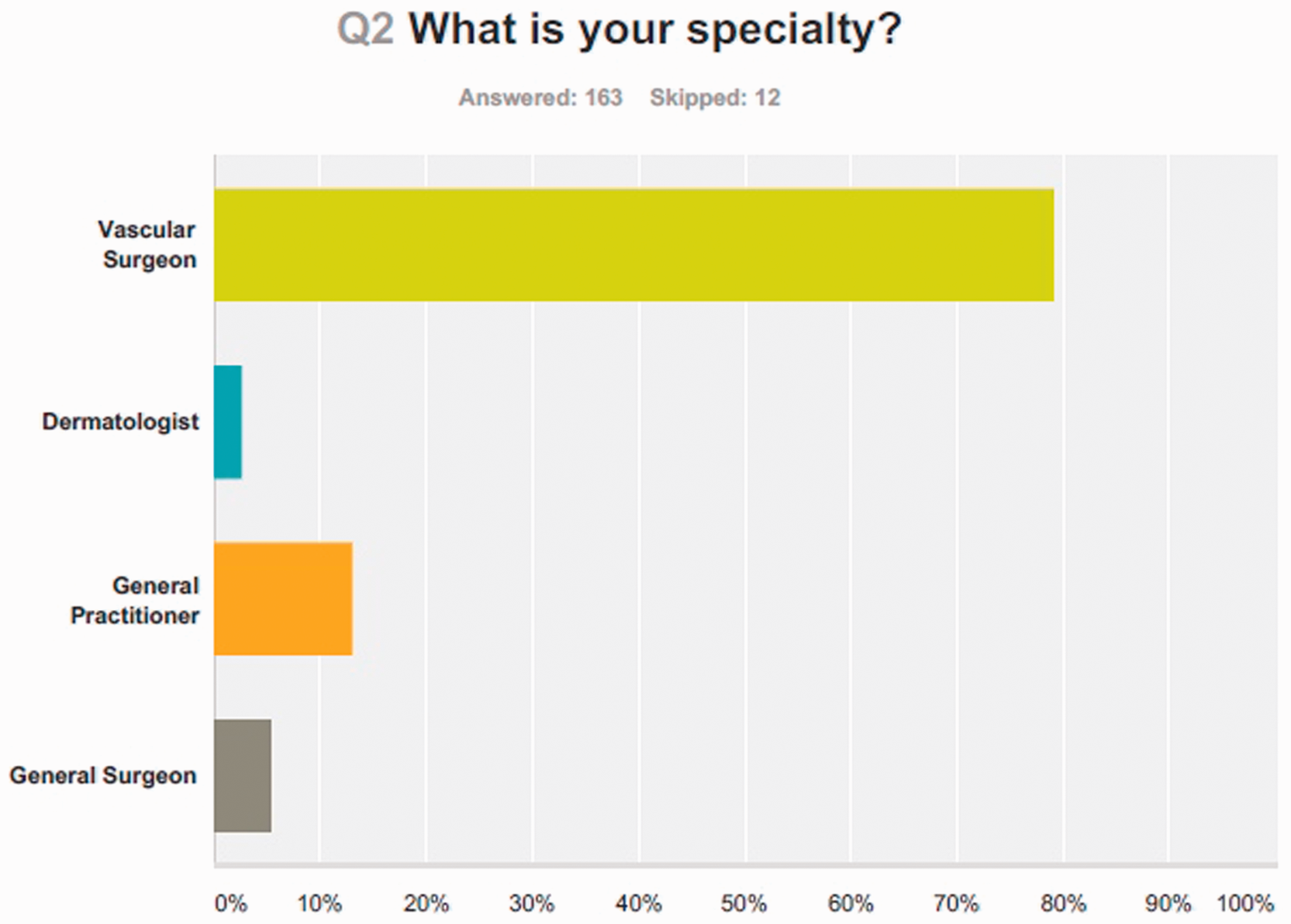

Eighty-three percent of the physicians performed DUS for confirmation of diagnosis, while the remaining ones (17%) did not perform any investigations at all. Spearman’s correlation coefficient rho (rs) showed that physicians with more experience consider an episode of SVT as a medical issue of moderate seriousness (rs = .170, p < 0.05) and perform DUS for confirmation of diagnosis (rs = .158, p < 0.05).
Elastic stockings were recommended by 87% of the physicians; more than half (57%) prescribed nonsteroidal anti-inflammatory drugs (NSAIDS), while 6% prescribed antibiotics. Most of the respondents advised anticoagulation (86%) for the treatment of SVT. Table 2 displays the disparity between treatment options concerning anticoagulation between vascular physicians and not vascular ones. Seventy percent prescribed LMWH, followed by Fondaparinux. The majority of the physicians prescribed anticoagulation regardless of the presence of VVs and location of SVT. Furthermore, 42% of the respondents considered that the administration of Fondaparinux for 45 days is a reasonable treatment for SVT regardless of the thrombosis location. In contrast, 30% of the physicians prescribed anticoagulation only when SVT was confined to an above knee segment. A large disparity was also shown in the dosage and duration of anticoagulation of those prescribed LMWH (Table 2, Figure3(a) and (b)). Most vascular surgeons advised LMWH in therapeutic doses (rs = .197, p < 0.05). More experienced physicians prescribed Fondaparinux as suggested by the CALISTO study (r = .216, p < 0.01).
(a) If you prescribe LMWH, what is the dose?, (b) What is the duration of anticoagulation with LMWH that you advise? Distribution of anticoagulation treatment type among specialties. LMWH: low-molecular weight heparin; VKAs: vitamin K antagonists; NOACs: new oral anticoagulants; SVT: superficial vein thrombosis; VVs: varicose veins; BTK: below the knee; ATK: above the knee.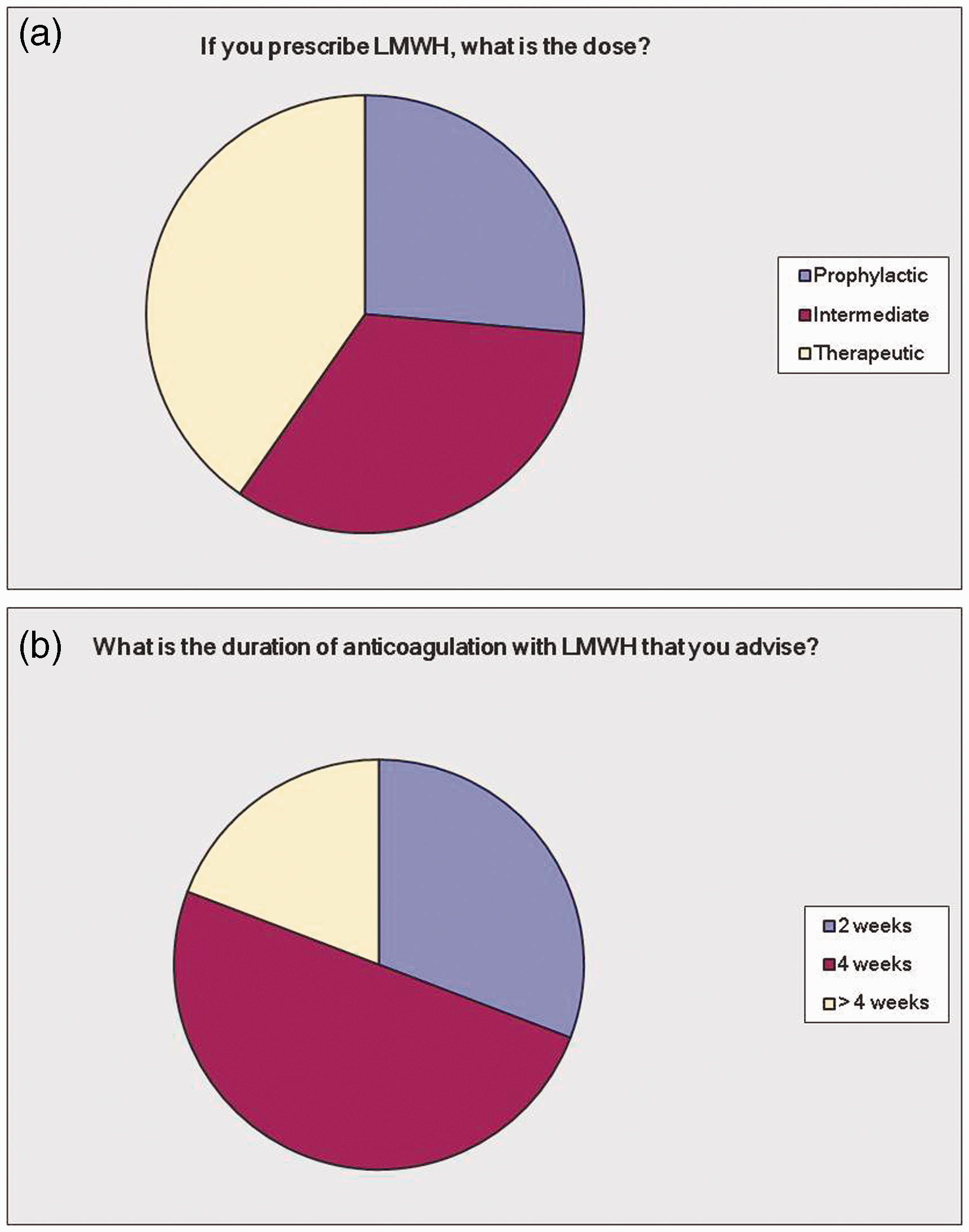

More than half of the physicians (54%) suggested thrombophilia test only when the thrombotic process occurs in the absence of VVs based on the age of the patient and the history of previous episode (rs = .271, p < 0.01), but 30% performed no investigation at all. Physicians practicing in private sector suggested more frequently surgical intervention in patients with SVT and VVs after completion of SVT treatment (rs = .188, p < 0.05), while the more experienced physicians were more conservative (r = .316, p < 0.01). Ninety percent of the participants, when suggesting intervention in the acute phase of SVT, they prefer ligation of the saphenofemoral junction with stripping and phlebectomies and not endovenous ablation or foam sclerotherapy (Figure 4). Finally, physicians that were treating a higher number of patients were not more in compliance with the current recommendations (rs = .098, p > 0.05).
If you suggest intervention in the acute phase of SVT, what kind of intervention do you prefer?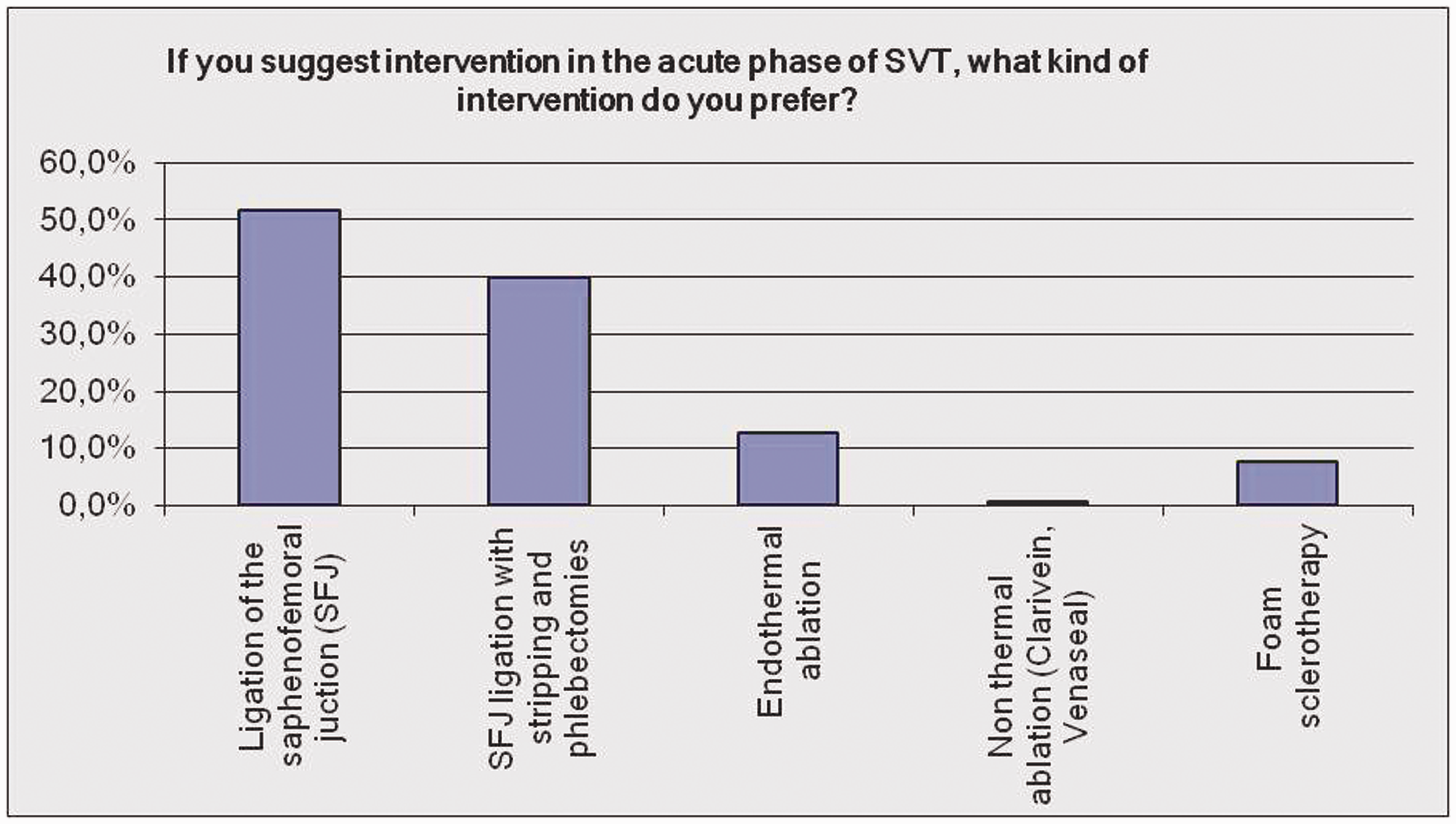
Discussion
Currently, there is still great variability in the management of SVT despite the fact that the relevant guidelines have been published recently.5,6 Furthermore, an updated Cochrane Database review concluded about the optimal treatment for SVT. 8 The main objective of this survey was to highlight the current status in the management of SVT among physicians.
Our study reiterates the great disparity that exists in the management of SVT in the current clinical practice. Physicians of various specialties with different level of experience and training are involved in managing venous diseases. Senior specialists with >25 years’ experience consider an episode of SVT as a moderate issue with potential severity. This is further supported by the fact that they perform DUS for confirmation of diagnosis and for exclusion of DVT. This is in accordance with the results of another survey, which showed that most of the participants believed that there is an association between of SVT and DVT. 15 Decousus et al.2,3 reported that SVT may coexist with DVT in 6–53% of the patients. Almost one-fifth of the participants in our survey, particularly those with less experience, underestimated the risk of DVT and performed no imaging. All patients with SVT should have bilateral DUS to exclude DVT and to estimate the extent of the thrombus. 5
More than half of the participants prescribed NSAIDS in conjunction with other treatment modalities. In a randomized controlled study, administration of dalteparin (LMWH) for 14 days was superior to NSAIDS in preventing thrombus extension. 16 Others reported that, NSAIDS reduce the incidence of SVT extension and local pain in comparison with placebo. 17 Nevertheless, administration of NSAIDS as a sole therapy for the treatment of above knee SVT is not recommended. 5 Another noticeable finding of our survey was that the vast majority of the participants advised compression therapy. Elastic stockings can be used as an adjunctive treatment to anticoagulation or surgery. 18 This combination has been shown to significantly reduce the risk of SVT extension and recurrence and is associated with lower incidence of VTE.10,11,19 However, it is true that most of the patients cannot tolerate the elastic stocking, especially during the first days of SVT development. While for isolated SVT at the below knee segment confined to varicosities, local application of heparinoids, NSAIDs, and elastic stockings has been recognized as an acceptable treatment option, 5 the majority of the participants prescribed anticoagulation in all cases regardless of the location of SVT. Six percent of the participants prescribed antibiotics. In another study, approximately 20% of the clinicians used antibiotics. 15 SVT is characterized by an aseptic inflammatory thrombotic process, and the administration of antibiotics should be avoided. 7
Although the majority of our respondents prescribed anticoagulation, a large disparity was shown regarding the regime, dose, and duration. Most of them prescribed LMWH in therapeutic doses for an interval of four weeks. Anticoagulation aims to prevent extension of the thrombotic process, reduction of SVT recurrence, and prevention of VTE. 8 However, large randomized multicenter trials failed to demonstrate significant differences between different treatments options (placebo, NSAIDS, or different anticoagulants).20,21 LMWH in intermediate doses for at least one month is recommended by the recent Consensus Statement for prevention and treatment of VTE despite the moderate level of evidence to this effect. 5 When thrombus is close to saphenofemoral or saphenopopliteal junctions, LMWH in therapeutic doses is an acceptable option. 5 The CALISTO study demonstrated that administration of Fondaparinux for 45 days was associated with a significant reduction in the thrombotic process.8,11 However, there has been justified criticism that the treatment with Fondaparinux for such a long period is not cost-effective and it should be advised only in patients with high thrombotic risk or for shorter treatment duration. 22 Nevertheless, further research is needed to assess the optimal dose and duration of anticoagulants. In our study, although most of the physicians consider the results of the CALISTO study as a reasonable treatment for SVT, they still prefer LMWH as the treatment of choice.
In our survey, only a minority of physicians prescribed oral anticoagulants for the treatment of SVT. Only one study has evaluated the effect of vitamin K antagonists reporting no significant reduction in VTE events or SVT extension and recurrence. 19 In addition, no data exist about the role of new oral direct thrombin and activated factor X inhibitors in the treatment of SVT. Another finding of our survey was that only 19% of the physicians regularly suggest thrombophilia screening as part of their investigation for the development of SVT. This is in accordance with the results of another survey. 15 Recent studies have demonstrated that protein S deficiency and mutation in prothrombin are associated with the development and recurrence of SVT in patients with VVs, respectively.23,24 Despite this, more than half of our participants performed thrombophilia test only when SVT develops in the absence of VVs. No evidence exists concerning the duration of treatment in patients with thrombophilia defects. In these patients, treatment with Fondaparinux 2.5 mg for 45 days or with intermediate doses of LMWHs for four weeks may be a reasonable and cost- effective treatment as hypercoagulable disorders are associated with an increased risk of DVT and/or PE. 25
Finally, the majority of physicians, when they suggest intervention in the acute phase of SVT, they perform open surgery and not endovenous ablation. Furthermore, senior specialists perform fewer interventions in the acute phase of SVT as they prefer administration of Fondaparinux. Venous stripping in combination with elastic stockings decreased the risk of SVT extension and recurrence compared to elastic stockings alone. 19 A review of studies comparing surgery to anticoagulation showed similar rates of SVT progression, but the incidence of VTE and complications was higher with surgery. 26 Surgery is recommended when thrombus is close to saphenofemoral or saphenopopliteal junctions depending on the patient’s characteristics and the treating physician’s preference. 5
Several questions about the management of SVT remain under investigation. This may explain the disparity in practice as well as the unscientific practice by some of the physicians. The management of SVT is not uniform and should be individualized according to location and etiology. 7 Additional studies are needed to clarify optimal management. However, until such studies are available, physicians should follow the latest guidelines.
This study has some limitations. Most of the physicians included in the study were vascular surgeons. This did not allow us to make comparisons among different specialties. Furthermore, the number of general practitioners was relatively small to allow consistent comparisons in the management of SVT in primary and secondary care services. Also, our results were not analyzed with regard to the national origin of the physicians in order to highlight any differences in the management of SVT among different health care services.
Conclusion
This survey highlights that there is a great disparity in the management of SVT among physicians. To a great extent, the current guidelines have not been adopted by physicians probably because they do not provide solid evidence regarding the regime, dose, and duration of SVT treatment. Further research is needed regarding optimal treatment, while more focused education and training is needed for those physicians involved in the management of venous diseases.
Footnotes
Authors’ contributions
CK, ADG conceived the study. CK, KS, AA collected the data. VL analyzed the data. CK wrote the first draft. CK, KS, VL, AA, ADG reviewed, amended and agreed the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to research, authorship, and/or publications of this article.
Funding
The author(s) received no financial support for the research authorship, and/or publications of this article.